Literature Review on Obesity: Causes, Treatment and Correlation with Pandemic COVID-19
Obesity is one of the most public health problems that face the health care practitioners and the whole mankind as well. Over the last 30 years, many countries have witnessed the prevalence of obesity in its citizen’s double, and even quadruple. As such, in this literature review, we are introducing most updated information about obesity in terms of its definition, complications, causes, effect of lifestyle on obesity, discovery and development of anti-obesity drugs, challenge in obesity treatment in addition to its relationship with pandemic COVID-19.
Introduction
Obesity and overweight are both described as abnormal or excessive fat buildup that poses a health concern. The body mass index (BMI) is a simple weight-for-height index that is often used to categorize humans as underweight, overweight, or obese. It’s calculated by multiplying the weight in kilograms by the square of the height in meters (kg/m2).WHO considers someone overweight if their BMI is 25 or higher, and obese if their BMI is 30 or higher. Obesity is a major cause of premature death as it is associated with metabolic disorders, including cardiovascular diseases and type 2 diabetes. Obese adults in the Eastern Mediterranean Region have these metabolic diseases at an alarming rate. According to data from 16 countries for adults aged 15 and older, Egypt, Bahrain, Jordan, Kuwait, Saudi Arabia and United Arab Emirates. Egypt, Bahrain, Jordan, Kuwait, Saudi Arabia, and the United Arab Emirates had the highest rates of overweight and obesity. The prevalence of overweight and obesity in these countries ranges from 74% to 86% in women and 69% to 77% in men. These data show a much higher prevalence of obesity among adult women, while overweight is more common among adult men. Recent data linking childhood and adolescent obesity to higher risk of obesity and morbidity in adulthood raises specific concerns about rising levels of overweight and obesity among children and adults [1].
Childhood Obesity
Obesity in children is a major public health issue in the United States and around the world. Obesity in children has become more common in recent years. It is produced by a discrepancy between the number of calories consumed and the number of calories expended. Obesity in children is caused by one or more variables (genetic, behavioural, and environmental). Childhood obesity leads to physical, psychological, and social health issues.Hence, effective intervention strategies are being used to prevent and control obesity in children [2].
Obesity and Diabetes
Much co-morbidity are associated with obesity, but it is type 2 diabetes that is most closely linked with increasing adiposity and even within the normal weight range diabetes prevalence begins to rise with increasing On a global scale, there are around 110 million diabetic patients, with this figure expected to rise to 180 million by 2010. This will clearly have major economic implications with diabetes consuming ever higher proportions of healthcare budgets. 80–90% of type 2 diabetes patients are overweight or obese, with an abdominal fat distribution [3].
Obesity and Cardiovascular Disorders
Obesity raises the risk of heart disease and death. Adipose tissue produces a large number of bioactive mediators that affect not only body weight homeostasis but also insulin resistance (a key feature of type 2 diabetes), lipids, blood pressure, coagulation, fibrinolysis, and inflammation, all of which contribute to endothelial dysfunction and atherosclerosis [4].
Obesity and Its Complications
Obesity can be defined as a condition of abnormal fat accumulation in adipose tissue to the extent that it is adversely affecting the function of all body systems and worsening many coexisting morbidity [5, 6]. Obesity occurs with increased adipose tissue formation. This originates from increased adipocyte number growth and the hypertrophy of adipocytes. A recruitment of new adipocytes from mesenchymal stem cell sources is one of the main causes of adipocyte number growth and thus in obesity, the fat mass exceeds 22 and 32 % of the total body weight in males and females. Respectively, but it can reach as much as 60–70 % of the bodyweight in massively obese individuals. Adipose tissue grows by hypertrophy of adipocytes, which is often followed by hyperplasia, as obesity progresses. Excess triglyceride accumulation in adipocytes causes hypertrophy, which causes the swollen cells to release proliferative paracrine factors (e.g. TNFa and IGF1), which are internal regulators of preadipocyte proliferation [7].
The increased mass of adipose tissues causes hypoxia in the tissues, resulting in cell death, increased chemokine secretion, and fatty acid flux dysregulation in advanced obesity. The dead cells stimulate infiltration of macrophages into the adipose- tissues which fuse to phagocytose the residual Lds forming large lipid-laden multinucleated syncytia, a stage that characterizes chronic inflammation and this accompanied with elimination of collagen type VI which result in adipose tissue fibrosis thus reduce plasticity as a result of fat expansion. Infiltrating macrophages are a major source of inflammatory mediators, especially TNFa, which interfere with adipocyte differentiation, promote lipolysis and free fatty acid secretion, and contribute to insulin resistance Similar to TNFa, other adipocytes with pro-inflammatory activity (e.g. IL-6 and monocyte chemoattractant protein-1) or adipocytes that are involved in thrombosis and hypertension (e,g. Plasminogen activator inhibitor-1 (PAI-1) and angiotensinogen) are also overproduced with increasing adiposity. On the contrary, secretion of some adipocytes with anti-inflammatory and anti-oxidant properties (e.g. adiponectin) is decreased [7].
The low-grade chronic inflammation in dysfunctional adipose tissues characterizing obesity is associated with the “metabolic syndrome “which clusters several metabolic abnormalities, including hypertension, dyslipidemia, glucose intolerance and Insulin resistance, malfunctions that increase the risk of developing type-2 diabetes and related cardiovascular disease [7]. Obesity is caused by a long-term energy imbalance between intake and output. Humans who are prone to obesity have hyperphagia, a slow metabolic rate, low fat oxidation rates, and reduced sympathetic nervous system activity [8]. Obesity isn’t included in the current classification of mental disorders and isn’t considered as an eating disorder. Obesity pathogenesis comprises a complex range of pathogenetic conditions, such as environmental, genetic, and epigenetic factors, all of which contribute to the disease setting in different ways Obesity pathogenesis is complicated by a number of pathogenetic factors, including environmental, genetic, and epigenetic factors, all of which play a role in the disease setting in different ways [6].
Obesity, and central (abdominal) obesity in particular, are known to be associated with comorbidities in various systems and high prevalence of dyslipidemia, insulin resistance and hypertension than in peripheral obesity [5] as the visceral fat tissues secrete higher levels of pro-inflammatory factors. In obesity, the appearance of dysfunctional adipose tissues is also associated with accumulation of ectopic fat in other tissues eg skeletal muscle and viscera, which eventually impairs systemic processes in the liver, pancreas, heart, and brain [7] and mediates lipotoxic effects on target cells such as dysfunction and cell death [6].
Obesity-Induced Liver Disease (Nonalcoholic Fatty Liver Disease)
High concentrations of diet and adipose tissue-derived free fatty acids, as well as proinflammatory adipocytokines, are the key contributors to NAFLD development and progression. Reactive oxygen species and other species that mediate liver damage, inflammation, and apoptosis are overproduced when mitochondrial oxidation levels are increased. In addition to storage of circulating FFAs, the liver becomes insulin resistant, secretes proinflammatory cytokines. NAFLD is also defined as hepatic fat content over 5% of total liver volume or weight. In NAFLD, liver increases gluconeogenesis, despite the high glucose plasma levels, releases more VLDL produced from FFAs contributing to hypertriglyceridemia, increases hepatic cytokines but also thrombotic factors secretion [6].
The uncontrolled release of FFAs from the adipose cell, caused by impaired hypertrophic growth and the local proinflammatory environment, is the first step in the development of dyslipidemia in which FFA and tri-glyceride levels in the blood are high, HDL levels are low, and LDL levels are altered. FFAs enter the liver via the portal vein and promote the development of VLDL, which inhibits the lipolysis of chylomicrons and causes hypertriglyceridemia. The triglycerides-cholesterol esters exchange seen between VLDL, which is high in triglycerides, and LDL/HDL, which is high in cholesterol esters, is caused by hypertriglyceridemia. This leads to a decrease in HLD-cholesterol levels and to the formation of small, dense LDL, a relevant risk factor for cardiovascular disease [6].
Obesity and Hypertension
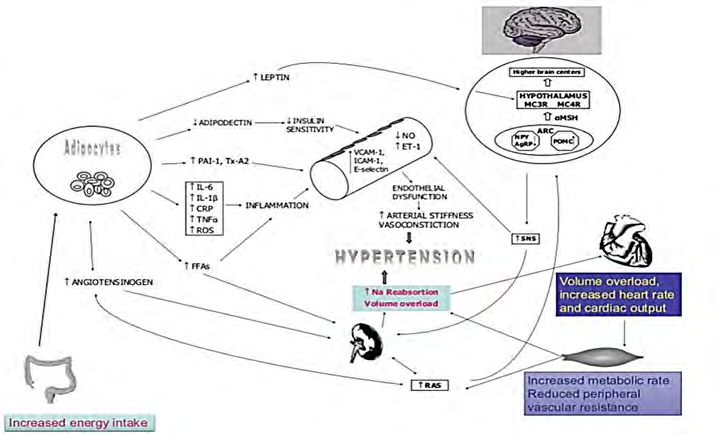
Obesity is consistently associated with hypertension. Obesity and hypertension have a clinical relationship since weight loss can result in a considerable drop in systemic blood pressure. There may be racial disparities within the impact of obesity because it is evaluated that weight control would dispose of hypertension in 28% of the Black population. This can be nearly multiplied to an assessed 48% within the White population. The mechanism by which obesity increases blood pressure is unknown. One assumption is that hyperinsulinemia is the cornerstone of this relationship, and many mechanisms have been proposed to explain the resultant increase in BP [9] as seen in Figure 1.
Obesity and Osteoarthritis
An obesity increase the risk of OA at both weight bearing (e.g., knee) and non-weight bearing (e.g., hand) joints in men and women but it is more common in women due to hormonal, productive, genetic factors [7]. Obesity raises diurnal cartilage tissue strain and knee adduction moments. This alteration isn’t well understood one reason for this uncertainty is because cartilage is a mechano sensitive tissue and under increased loading conditions, cartilage may up-regulate anabolic pathways to increase proteoglycan content and thickness. By altering cartilage susceptibility to inflammation and oxidative stress-mediated catabolic pathways, biomechanical stimulation associated with obesity and ageing can increase the risk of OA. Enhanced inflammation by pro-inflammatory cytokines TNFa and IL-1b, associated with obesity may contribute to OA pathogenesis by increasing mitochondrial ROS generation. Chronic inflammation-induced ROS generation without a compensating increase in mitochondrial antioxidants leads to oxidative stress pathology which results in damage in tissues of obese patients [7].
Obesity and Sleep Apnea
Obesity is the most documented risk factor for obstructive sleep apnea. OSA is a condition marked by episodes of hypopnea or apnea caused by repeated partial or total obstruction of the upper airway during sleep. Obesity is associated with significant sleep apnea in around 40% of obese people, and the incidence of OSA increases as the BMI rises. Obesity hypoventilation syndrome is often coexisting with OSA, and OSA may be one of the causes (OHS) [9].
Obesity and Cancer
Obesity is thought to be responsible for 20% of all cancers as a single risk factor. Obesity and excess weight are linked to an increased risk of cancers such as colorectal, postmenopausal breast, endometrial, renal, and esophageal cancer.
Weight gain itself is also associated with cancer risk. For example, in a Canadian report, men who gained ≥21 kg after age 20 had a 60% higher risk of colorectal cancer than men who gained only 1–5 kg. In another study, women who lost≥10 kg after menopause and kept it off saw a 50% reduction in breast cancer risk. Specific mechanism behind the link between obesity and cancer development is unknown; however it is likely to be many. The enhanced aromatization that occurs in adipose tissue, resulting in higher estrogen levels, is suggested to be one contributing reason. This could play a role in the development of endometrial cancer and breast cancer. Other mechanisms suggested include the impact of obesity and weight gain on insulin resistance and the resulting effects on inflammation. The latter may be particularly significant in cases of colon cancer [9].
Causes of Obesity
The balance between calorie intake and energy expenditure determines a person’s weight. A person gains weight if he or she consumes more calories than they burn (metabolise) (the body will store the excess energy as fat). A person will lose weight if he or she consumes fewer calories than he or she metabolises. As a result, overeating and physical inactivity are the most common causes of obesity. Ultimately, body weight is the result of genetics, metabolism, environment, behavior, and culture [10].
Diet
Overeating leads to weight gain, especially if the diet is high in fat. Food high in fat or sugar (for example, fast food, fried food, and sweets) has high energy density (foods that have a lot of calories in a small amount of food). Diets high in fat have been linked to weight growth in epidemiological research [11]. Obesity does not develop overnight, but rather over time as a result of poor dietary and lifestyle choices.
Lack of Physical Activity
Another important factor in obesity is a lack of physical activity. Many people work jobs that require them to sit at a desk for the majority of the day. They also drive rather than walk or ride their bikes. If you are not physically active enough, you will not utilize the energy provided by the food you eat, and the excess energy will be stored as fat by your body. Adults should engage in at least 150 minutes of moderate-intensity aerobic activity per week, such as cycling or fast walking, according to the Department of Health and Social Care. This does not have to be completed in one sitting, but can be done in smaller increments. You could, for example, exercise for 30 minutes five days a week. If you’re overweight and attempting to reduce weight, you might need to undertake more exercise. It may help to start off slowly and gradually increase the amount of exercise you do each week [11].
Genetic Reasons
A small proportion of cases of obesity arise from genetic factors, leading to specific clinical syndromes. Monogenic causes of obesity include mutations in the leptin gene and its receptor, or the melanocortin system. If one or both parents are obese; a child is more prone to develop obesity. Hormones involved in fat management are also affected by genetics. Leptin deficiency is one hereditary cause of obesity. Leptin is generated treatment in fat cells and the placenta. When body fat storage is too high, leptin sends a signal to the brain telling it to eat less. If the body is unable to create enough leptin or leptin is unable to signal the brain to eat less, this control is lost, and obesity develops. The use of leptin replacement therapy as a for obesity is being investigated [12].
Medications
Medications associated with weight gain include certain antidepressants, anticonvulsants such as carbamazepine and valproate, some diabetes medications such as insulin, sulfonylureas, and thiazolidinedione, certain hormones such as oral contraceptives, and most corticosteroids such as prednisone. Weight gain is a side effect of some blood pressure medicines and antihistamines. The reason for weight gain with drugs varies depending on the prescription. If this is a concern for you, you should discuss your medications with your physician rather than discontinuing the medication, as this could have serious effects [13].
Diseases
Hypothyroidism
Hypothyroidism report weight gain as opposed to 13.8% in controls. Undiagnosed hypothyroidism may go unnoticed for sometimes due to insidious onset of symptoms including weight gain. There is a slow progression of thyroid under activity and development of clinical symptoms. Hypothyroidism causes a mild weight increase in most people. As early symptoms are variable and non-specific, there should be allow threshold for screening patients for primary hypothyroidism with a serum thyrotropin- stimulating hormone (TSH) determination.
The weight gain in hypothyroidism is related to several factors:
- Hyaluronic acid builds up in the dermis and other tissues as a result of hypothyroidism.. As this material is hygroscopic, it produces mucinous edema responsible for thickened structures and puffy appearance [14].
- Due to reduced bowel peristalsis and deposition of glycoproteins in the bowel wall, patients invariably complain of constipation which may lead to fecal impaction, myxedema, mega -colon and myxedema ileus.
- The effects of thyroid hormone have also been reported in the myocardium and vasculature. T3 enhances cardiac output and reduced systemic vascular resistance in normal adult males within 3 min [15], and cell culture studies suggest that thyroid hormones rapidly, and non- genomically, regulate the Ca2 ATPase enzyme, the Na channel via PKC, the K channel via PI3-kinase, the Na/H anti-porter via PKC and MAPK and the inward rectifying potassium channel.
T3 also increases sarcoplasmic reticulum Ca2, cell shortening, contractility and calcium mediated arrhythmic activity, suggesting that T3 has a non-genomic, positive ionotropic and arrhythmogenic effect. Thus, lack of thyroid hormones leads to a reduced inotropic and chronotropic effect on the cardiac output.
Patients with severe hypothyroidism may develop pericardial and pleural effusions. Protein and glycosaminoglycan are abundant in the exudates. Renal blood flow, glomerular filtration rate, tubular reabsorption, and secretion are all impaired in this condition. This leads to a decrease in water clearance due to hydrophilic deposits in the tissues and leads to an increase of total body water content [14, 15].
Environment
Obesity is not just a concern for individuals. Increase in obesity connected to economic development show that obesity is a hidden risk factor. There are groups all over the world who live traditional lives but gain weight and get diabetes after being exposed to 21st century Western society. Obesity runs in families closer to home, owing to common genes as well as a shared family lifestyle. Changes in society have resulted in a larger reliance on convenience foods and a higher consumption of food cooked outside the home, which tends to be higher in fat and sugar than food prepared at home. People are becoming increasingly reliant on time- saving devices that reduce effort, and then rewarding themselves with hours in front of the TV or computer after a long day at work [12].
Anti-Obesity Drugs Discovery and Development
In the past: Centrally acting sympathomimetic, such as the amphetamine derivatives desoxyephedrine, phentermine and diethylpropion, were among the earliest pharmacological agents used for weight loss. They were popular in the 1950s and 1960s, but growing worries about cardiovascular risk and misuse potential led to a significant drop in use by the early 1970s, despite the fact that they were still available in many countries. Phentermine and diethylpropion were replaced by the serotonin (5-HT)- releasing agents fenfluramine and dexfenfluramine in the 1970s and 1980s. In the early 1990s, United States used combination of phentermine and fenfluramine to reach superior efficacy over either compound given alone, but after a few years the manufacturers withdraw fenfluramine and dexfenfluramine from the market due to reports of cardiac valvopathy specially when these agents were combined with phentermine [16, 17].
In Europe, three agents were approved for the long- term clinical management of obesity and related metabolic syndrome:
• Sibutramine [17, 18] (trade names Meridia® and Reductil®) A dual monoamine reuptake inhibitor (noradrenaline and serotonin) was introduced in the late1990s to clinical practice, but in January 2010clinical trial led to withdraw from marketing authorizations by the EMA.
• Rimonabant (Acomplia®) [17, 18] In the mid-1990s, a cannabinoid CB1 receptor antagonist/ inverse agonist was discovered. It has ability to suppress appetite and weight gain in experimental animals and, in four major clinical trials, although that not approved in the United States. In Europe was licensed as an anti-obesity agent by the EMA in June 2006, but in October 2008 has been suspended marketing authorizations by the EMA.
• Orlistat (Xenical® and Alli®) [17, 18] FDA approved orlistat for the treatment of obesity in 1998 other than other agent above, at the time of writing, orlistat is the only weight loss agent approved for long-term clinical use in Europe.
Leptin, Leptin Analogues and Leptin Sensitizers
White adipose tissue secretes leptin, a protein (WAT). In the ARC of the hypothalamus, it activates anorexigenic POMC neurons while inhibiting orexigenic NPY neurons, encouraging satiety, increased energy expenditure, and weight reduction. Leptin levels in the bloodstream rise with obesity and fall with weight loss, suggesting that the latter is involved in the decrease in total and resting energy expenditure seen after weight loss. In the field of obesity research, the discovery of leptin in 1994 was a game- changer It contributed to the understanding that obesity is a disease with a solid biological foundation, rather than just the product of bad lifestyle choices. Physiological amounts of leptin were shown to reduce food intake and body weight in very obese congenitally leptin-deficient subjects. Obese people, on the other hand, are leptin-resistant and have elevated circulating leptin levels. In a placebo-controlled study, 47 obese men and women were given varying doses of recombinant human leptin (0.03 mg/kg and 0.30 mg/ kg, respectively) for 24 weeks and told to eat 500 kcal less per day than their body requirements. Reports were similar from animal studies testing the effect of leptin sensitizers targeting the protein tyrosine phosphatase-1B (PTP1B) or the chemical chaperones that repair ER stress4-phenyl butyric acid (PBA) and tauroursodeoxycholic acid (TUDCA) are two examples [19].
Melanocortin-4 Receptor Agonists
The hypothalamic control of body weight and energy expenditure is heavily influenced by the melanocortin system. Through the production of CART and melanocyte- stimulating hormone (-MSH), leptin suppresses the orexigenic neuropeptides orexin and melanocortin- concentrating hormone (MCH) in the lateral hypothalamic Area (LHA). The latter is produced by prohormone convertase-1 cleavage of POMC and works by activating the melanocortin-3 and -4 receptors (MC3R, MC4R).-MSH has emerged as a potential new anti-obesity medication, with normal-weight participants receiving intranasal injection of the melanocortin sequence MSH/ACTH4-10, which was found to enhance subcutaneous WAT lipolysis and reduce body fat by 1.7 kg after six weeks. In a 12-week trial of 23 overweight men, it failed to cause any substantial reduction in body weight or body fat when compared to placebo [19, 20, 21].
Lorcaserin:
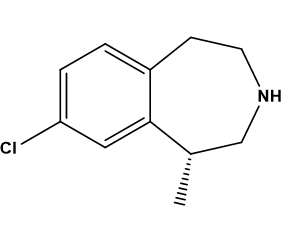
As activation of the 5-HT1B receptor has been implicated in both primary pulmonary hypertension and valvopathy, the 5-HT2C receptor subtype has been proposed as a target for therapeutic intervention to allow weight loss. Several potent and selective 5-HT2C receptor agonists proved to be effective in suppressing food intake and inducing weight loss in rodents, including WAY-163909, CP-809101, and vabicaserin. However, only lorcaserin (Figure 2) moved into clinical testingLorcaserin (Belviq) is a selective 5-HT2c receptor agonist that belongs to the third generation of anti-obesity medicines based on 5-HT. It increases satiety and decreases food intake by activating hypothalamic POMC neurons, but has little effect on energy expenditure. It has been found to inhibit binge eating habits by acting on midbrain dopaminergic tone. Its role in addictive disorders is currently being researched. Based on the outcome of the BLOOM and BLOSSOM trials, in 2012 the FDA approved lorcaserin as an addition to a reduced-calorie diet and exercise for eligible patients. The effectiveness of lorcaserin appears to be equivalent to that of orlistat (about 3 to 4 kg difference in weight reduction between active and placebo treated groups) and maybe somewhat better. Less than that of phentermine-topiramate. The BLOOM-DM trial looked at the impact of lorcaserin in patients with T2DM and a BMI of 27-45kg/m2, and found that it reduced body weight by about 5kg compared to 1.6kg in the placebo group, as well as significant reductions in heart rate, HDL levels, and waist circumference. Valvopathy did not appear to be increased as a result of therapy, and lorcaserin was usually well accepted, with few side effects such as headache, dizziness, tiredness, and nausea. After the results of BLOOM-DM trial, a potential combination of GLP-1RA and 5-HT2A/C is now under investigation [22, 23, 24].
Glucagon-Like Peptide 1/Glucagon
As mentioned before, GLP-1 analogues are effective anti-obesity medications and improve glucose intolerance. Glucagon stimulates gluconeogenesis and glycogenolysis in the liver directly. Hyperglycemia and T2DM are possible outcomes. It’s worth noting that T2DM patients have a problem with glucagon secretion. Glucagon, on the other hand, reduces food intake, increases energy expenditure via brown fat thermogenesis, reduces fat storage by lipolysis and lipid synthesis inhibition, improves cardiac function, and slows stomach motility in the CNS., and stimulates autophagy.
The first human research published in 2009 found that low-dose co-infusions of GLP-1 and glucagon reduced food intake while increasing energy expenditure. When the amino acids 17, 18, 20, 21, 23 of glucagon were replaced by the corresponding GLP-1 residues in the glucagon molecule, therapy with a GLP-1/glucagon multi-agonist was produced. The alanine at position 2 of the peptide was substituted with Amino iso butyric acid (Aib) to protect the molecule from DDP- IV inactivation, and a lactam bridge was introduced between to guarantee glucagon receptor efficacy, amino acids 16 and 20 stabilise the secondary structure. In diet-induced obesity in mice, once weekly treatment of this pharmacological drug for four weeks improved obesity, hepatic steatosis, glycemic control, and lipid profile. Only the multi-agonist treatment, not the glucagon monotherapy, resulted in an increase in energy expenditure. Furthermore, treatment with the multi- agonist enhanced DIO mice’s leptin sensitivity. Different GLP- 1/glucagon multi-agonists are currently under investigation. Interestingly, an oxyntomodulin multi-agonist was under investigation concurrently with the GLP1/glucagon multi- agonist [25, 26].
Current Anti-Obesity Drugs
Phentermine
Phentermine (Figure 3), which was approved in 1959 for those aged > 16 years, is still the most commonly prescribed anti-obesity medication in the USA and in other countries, with the exception of the European Union due to its potential side effects [27, 28].
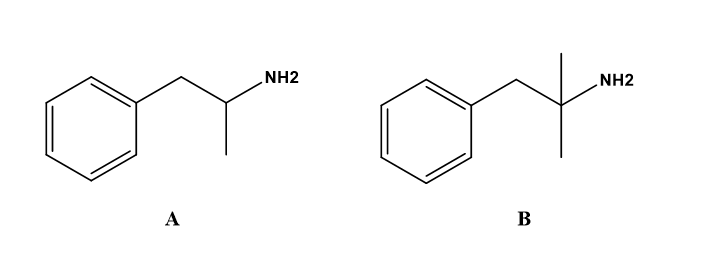
Phentermine is a synthetic counterpart of amphetamine that has an extra methyl group on the carbon next to the amine moiety.However, this small structural change results in a significant difference in potency and selectivity on the release and reuptake of monoamine neurotransmitters [28, 29].
Although the exact mechanism of action is unknown, weight loss might be mediated through the release of catecholamine in the hypothalamus, which lead to reduced appetite and decreased food consumption [28, 29, 30].
Orlistat
Orlistat (Figure 4) was first approved by the FDA in 1999. Today, it remains the longest licensed anti-obesity drug for long-term use [28, 29, 30, 31].
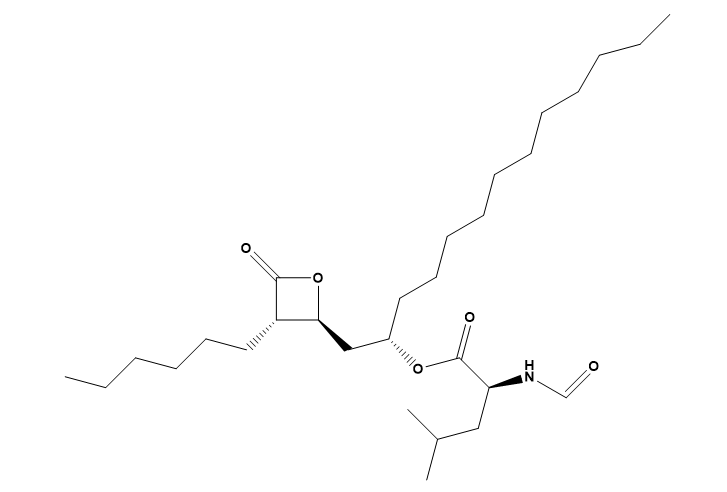
Orlistat is a potent and reversible gastrointestinal lipase inhibition for preventing dietary fat absorption by 30% by inhibiting pancreatic and gastric lipase [27, 28, 29, 30].
Naltrexone SR/Bupropion SR
The naltrexone /bupropion (NB) combination (Figure 5) was demonstrated in preclinical animal models to function in a synergistic manner, augmenting POMC activity to cumulatively reduce food intake and satiety [27, 28, 29, 30]. Naltrexone / bupropion are drugging Combination for the long-term management of weight loss. In combination was approved the FDA [31].
Bupropion has been used for the treatment of depression and smoking addiction, while naltrexone has been independently used to treat opium addiction withdrawal. It was stated that the combination of these two medications, naltrexone and bupropion, stimulates neuronal activation and lowers food intake by stimulating the satiety center [30].
Naltrexone blocks opioid receptor-mediated POMC auto inhibition and bupropion selectively inhibit reuptake of dopamine and noradrenaline. The combination has an effect on CNS reward pathway food intake and satiety through antagonistic feedback inhibition [28, 32].
Liraglutide
Liraglutide is a glucagon-like peptide 1 (GLP1) receptor agonist of an incretin-derived hormone that affects glucose homeostasis, food intake, and satiety through both peripheral and central receptor pathways. Because of its incretin properties, this compound is an attractive drug for patients with T2DM and obesity [27, 28, 32].
After meals, GLP-1 is secreted from the distal ileum proximal colon, and the vagal nucleus of the solitary tract and exhibits multiple effects as an incretin hormone GLP-1 mainly regulates blood glucose by enhancing insulin secretion from the pancreatic beta-cells and inhibits glucagon secretion in a glucose-dependent manner [31]. Liraglutide functions at the pancreas to enhance glucose-stimulate insulin secretion and reduce inappropriately elevated levels of glucagon. It also delays gastric emptying and increases satiety by central effects on the hypothalamus [27, 28, 32].
The Challenge with Anti-Obesity Drugs
Obesity is a serious and growing health problem around the world. To address this issue, efforts in schools, communities, and the food business will be required, as well as broader measures to increase diet and physical activity among the general population. In clinical care, a focus on life change in patients who are willing and motivated to make changes is the most practical treatment strategy. Now there are several anti-obesity medications that have been thoroughly studied by regulatory organizations and found to be safe and effective; nevertheless, these medications are not commonly administered [33].
It’s possible that this is due to a long history of side effects associated with older medications, as well as many doctors’ hesitancy to think of obesity as a biological illness for which pharmacotherapy is an appropriate therapeutic option. However, existing information contradicts this viewpoint, which clearly demonstrates the biological underpinnings of obesity in animals and humans, as well as the critical physiological processes that encourage weight rebound after a person has lost weight. Admittedly, available anti-obesity drugs are not as effective as we would like and they do have side effects. However, it is still troubling that only 1–2% of patients in the USA who are eligible get a prescription (international information is unavailable). These medications are supported by authoritative guidelines produced by numerous expert panels, and extensive safety and efficacy data exist for the newer drugs. If adherence to pharmacotherapy guidelines for diabetes, hypertension, or hyper-lipidaemia were this low, serious action would be undertaken to address the issue [33].
Drug Mechanism of action, Effect on weight and Side effect: phentermine reducing food intake: sympathomimetic amine, 3.6 kg at 6 months while its side effects: Headache, insomnia, irritability, palpitations and nervousness. diethylpropion as above 3.0 kg at 6 months, as above. Fluoxetine Reducing food intake: selective serotonin reuptake inhibitor 4.74 kg at 6 months, and 3.15 kg At 1 year, its side effects: Agitation and nervousness. Sibutramine Reducing food intake: combined Norepinephrine and serotonin reuptake Inhibitor, 4.45 kg at 1 year, side effects: Headache, insomnia, dry mouth and constipation. Long term Treatment increases the risk of major adverse cardiovascular Events Orlistat Reducing fat absorption: lipase inhibitor 2.59 kg at 6 months and 2.89
kg At 1 year, diarrhea, flatulence, bloating, abdominal pain and dyspepsia Rimonabant Reducing food intake: selective CB1 Receptor blocker 5.1 kg at 1 year Nausea, dizziness, arthralgia and diarrhea [33].
Other Anti Obesitic Drugs
Three more medications show potential but have not yet been approved for use in the treatment of obesity. Metformin has been used for many years in patients with type 2 diabetes mellitus. It is the only anti-diabetic drug that has been shown, in long term clinical trials, to reduce mortality and to prevent the development of diabetes. It does not cause weight gain unlike sulphonylureas and insulin. Weight loss has been observed among non-diabetic individuals in some studies. Metformin is not currently licensed for the treatment of obesity, but it is a first line treatment in diabetes [34].
Topiramate which is an anti-epileptic drug blocks voltage-dependent sodium channels, glutamate receptors, and carbonic anhydrase, and increases the activity of GABA. It remains unlicensed for the treatment of obesity because diarrhea and leakage were observed in early clinical studies. Qnexa is a combination of topiramate and phentermine [34].
Liraglutide is a glucagon-like peptide-1 analogue which was firstly used for the treatment of type 2 diabetes mellitus. As GLP-1 suppresses appetite and delays gastric emptying, liraglutide reduces body weight even in non-diabetic individual [34].
Despite promising outcomes in body weight loss and some cardiovascular risk factors, most anti-obesity medications have yet to be licensed or have had to be pulled from the market due to negative side effects. Orlistat is the only anti-obesity medicine licensed for long-term usage now that sibutramine is no longer available. There is an urgent need for the development of new anti-obesity drugs. The long-term safety and efficacy of newly developed drugs should be carefully evaluated [34].
Effects of COVID-19 and Quarantine on Lifestyle
COVID-19 is a highly pathogenic virus that is causing a global pandemic with a high number of deaths and infected people. To prevent the spread of infection, numerous governments have imposed limits on outdoor activities or even imposed a population-wide quarantine. Quarantine is linked to stress and despair, which leads to a poor diet and lack of physical activity. The main effect of quarantine-related stress is a change in lifestyle and eating habits. Changes in dietary habits can be because of:
- Reduced availability of goods
- Limited access to food caused by restricted store opening hours.
- Switch to unhealthy food. Diet takes a step back from being a healthy diet rich in fresh food to one containing foods with a long shelf-life during quarantine. In addition, for many people, the typical response to chronic stressful situations is not to avoid food but possibly to seek out and consume energy-dense foods [35].
Anxiety, depression, uneasiness, and anger are emotions that commonly accompany chronic stress [36]. The responses to acute or chronic stress also include several modifying behaviors such as smoking, and eating [36, 37].
Impact of Quarantine on People with Obesity
Obese patients were exposed to a great deal of stress throughout the quarantine, which made them more sensitive to overeating and a sedentary lifestyle, predisposing them to gain even more weight. Furthermore, as a result of the impending economic crisis, people will consume more unhealthy foods because they are less expensive. This will lead to further increase in obesity prevalence especially in weaker sections of the society [38].
Effects of COVID-19 Restrictions, Social Distancing, and Quarantine on Skeletal Muscle Mass
Prior to this pandemic, World Health Organization recommendations for PA (physical activity) (150 min/week of moderate intensity aerobic PA with muscle strengthening exercises 2 day/week, etc.) were not being met, particularly in older populations [39]. COVID-19 presents several risks for further reductions in activity levels for the general population. Gyms and recreation centres are closed, and group exercise and rehabilitation programs have been suspended, as a result of quarantine, self-isolation, social distancing, and other government actions. It has never been easier to live a sedentary lifestyle. In addition to and independently of reduced PA, increased sitting time and sedentary behavior, which have been reported to increase during COVID-19 quarantine [40], are also associated with multiple adverse health outcomes (Figure 6) [41].
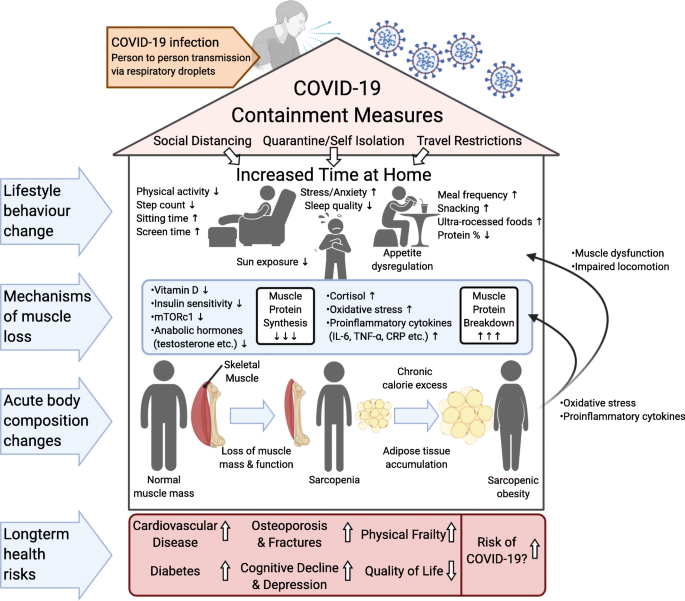
Behaviors and the mechanisms by which it can lead to reduced muscle protein synthesis and increased muscle protein breakdown resulting in muscle loss. Sarcopenia, or sarcopenic obesity in the context of caloric excess, is linked to an elevated risk of a variety of comorbidities, some of which may also raise the risk of COVID-19 infection and severity (Figure 7) [42].
![Figure 7: A summary of physical activity, nutritional, and supplement countermeasures that may be useful in avoiding muscle loss in both younger and older persons. The inclusion of telehealth services offering regular contact, guidance, and support to such counter-measures may result in greater adherence and positive outcomes [42].](/fulltextimages/7902/fig_7.png)
Conclusion
Over the last 30 years, obesity cases have risen dramatically due to economic expansion, industrialization, mechanized transportation, urbanization, an increasingly sedentary lifestyle, and a dietary shift to processed foods and high-calorie diets. This literature review describes all required information about obesity in terms of its complications, causes, effect of life style on obesity, treatment using drugs with different mode of actions, challenge in obesity treatment in addition to its relation with COVID-19.
References
-
Deurenberg P, Yap M, van Staveren WA (1998) Body mass index and percent body fat: a meta-analysis among different ethnic groups. Int J Obesity Rel Metabol Dis 22 (12): 1164-1171.
-
Ramachandran A, Snehalatha C, Viswanathan V, Viswanathan M, Haffner SM (1997) Risk of noninsulin dependent diabetes mellitus conferred by obesity and central adiposity in different ethnic groups: a comparative analysis between Asian Indians. Mexican Americans and Whites. Diabetes Res Clin Prac 36(2): 121-125.
-
McKeigue PM, Marmot MG, Adelstein AM, Hunt SP, Shipley MJ, et al. (1985) Diet and risk factors for coronary heart disease in Asians in northwest London. Lancet 2(8464): 1086-1090.
-
Björntorp P (2001) International textbook of obesity. Björntorp P (Ed.), Chichester, UK: Wiley.
-
Sbraccia P, Finer N (2019) Obesity: Pathogenesis, Diagnosis, and Treatment. Sbraccia P, Finer N (Eds.), Springer International Publishing.
-
Gefen A, Benayahu D (2014) The Mechanobiology of Obesity and Related Diseases. Gefen A, Benayahu D (Eds.), Cham: Springer.
-
Wadden TA, Bray GA (2018) Handbook of obesity treatment, 2nd (Edn.), The Guilford Press.
-
Youdim A (2015) The clinician’s guide to the treatment of obesity, Springer.
-
Aronne LJ, Nelinson DS, Lillo JL (2009) Obesity as a disease state: a new paradigm for diagnosis and treatment. Clin Cornerstone 9(4): 9-25.
-
Wilding J PH (2001) Causes of obesity. Prac Diabetes Int 18(8): 288-292.
-
Jebb S (2004) Obesity: causes and consequences. Women’s health medicine 1(1): 38-41.
-
Schwartz TL, Nihalani N, Jindal S, Virk S, Jones N (2004) Psychiatric medication‐induced obesity: a review. Obesity Rev 5(2): 115-121.
-
Smith TJ, Bahn RS, Gorman CA (1989) Connective tissue, glycosaminoglycans, and diseases of the thyroid. Endocr Rev 10: 366-391.
-
Schmidt BM, Martin N, Georgens AC, Tillmann HC, Feuring M, et al. (2002) Nongenomic cardiovascular effects of triiodothyronine euthyroid male volunteers. J Clin Endocrinol Metabol 87(4): 1681-1686.
-
Weaver JU (2008) Classical endocrine diseases causing obesity. Obesity and Metabolism 36: 212-228.
-
Rodgers RJ, Tschöp MH, Wilding JP (2012) Anti-obesity drugs: past, present and future. Disease models & mechanisms 5(5): 621-626.
-
van der Meer L, Costafreda S, Aleman A, David AS (2010) Self-reflection and the brain: a theoretical review and meta-analysis of neuroimaging studies with implications for schizophrenia. Neurosci Biobehav Rev 34(6): 935- 946.
-
Rahman AU, Choudhary MI (2017) Anti-obesity drug discovery and development, Bentham Science Publishers, 3.
-
(2011) Amylin and Takeda Discontinue Development of Pramlintide/Metreleptin Combination Treatment for Obesity Following Commercial Reassessment of the Program.
-
Wellhoner P, Horster R, Jacobs F, Sayk F, Lehnert H, et al. (2012) Intranasal application of the melanocortin 4 receptor agonist MSH/ ACTH (4-10) in humans causes lipolysis in white adipose tissue. Int J Obes (Lond) 36(5): 703-708.
-
Fehm HL, Smolnik R, Kern W, McGregor GP, Bickel U, et al. (2001) The melanocortin melanocyte-stimulating hormone/adreno corticotropin (4-10) decreases body fat in humans. J Clin Endocrinol Metab 86(3): 1144- 1148.
-
Launay JM, Herve P, Peoc K, Tournois C, Callebert J, et al. (2002) Function of the serotonin 5-hydroxytryptamine 2B receptor in pulmonary hypertension 8(10): 1129- 1135.
-
Fitzgerald LW, Burn TC, Brown BS, Patterson JP, Corjay MH, et al. (2000) Possible role of valvular serotonin 5-HT (2B) receptors in the cardiopathy associated with fenfluramine. Mol Pharmacol 57(1): 75-81.
-
Dunlop J, Sabb AL, Mazandarani H, Zhang J, Kalgaonker S, et al. (2005) WAY-163909 [(7bR, 10aR)-1,2,3,4,8,9,10,10a- octahydro-7bH-cyclopenta-[b] [1,4] diazepino [6,7,1hi] indol e], a novel 5-hydroxytryptamine 2C receptor- selective agonist with anorectic activity. J Pharmacol Exp Ther 313(2): 862-869.
-
Cegla J, Troke RC, Jones B, Tharakan G, Kenkre J, et al. (2014) Coinfusion of low-dose GLP-1 and glucagon in man results in a reduction in food intake. Diabetes 63(11): 3711–3720.
-
Day JW, Ottaway N, Patterson JT, Gelfanov V, Smiley D, et al. (2009) A new glucagon and GLP-1 co-agonist eliminate obesity in rodents. Nat Chem Biol 5(10): 749- 757.
-
Srivastava G and Apovian C M (2018) Current pharmacotherapy for obesity. Nature Rev. Endocrinol, 14(1): 12-24
-
Kang J G and Park C Y (2012) Anti-obesity drugs: a review about their effects and safety. Diabetes & metabol J 36(1): 13-25.
-
Mayer M A, Hocht C, Puyó A, and Taira C A (2009) Recent advances in obesity pharmacotherapy. Curr Clin Pharmacol 4(1): 53-61.
-
Mayer MA, Hocht C, Puyó A, Taira CA (2009) Recent advances in obesity pharmacotherapy. Curr Clin. Pharmacol 4(1): 53-61
-
Tak Y J and Lee S Y (2021) Anti-obesity drugs: long-term efficacy and safety: an updated review. World J of mens health 39(2): 208-221.
-
Nuffer W A and Trujillo JM (2015) Liraglutide: a new option for the treatment of obesity. Pharmacotherapy: J. Human Pharmacol. Drug Ther. 35(10): 926-934.
-
Bessesen, D H, and Van Gaal L F (2018) Progress and challenges in anti-obesity pharmacotherapy. The lancet Diabetes endocrinol 6(3): 237-248.
-
Li M F, and Cheung B M (2011) Rise and fall of anti- obesity drugs. World J diabetes 2(2): 19.
-
Bracale R and Vaccaro CM (2020) Changes in food choice following restrictive measures due to Covid-19 Nutrition, Metabolism & Cardiovascular Diseases 30(9): 1423-1426.
-
Torres SJ, and Nowson CA (2007) Relationship between stress, eating behavior, and obesity. Nutrition 23(11- 12): 887-894.
-
Schiffman SS, Graham BG, Sattely Miller EA, Peterson Dancy M (2000) Elevated and sustained desire for sweet taste in African-Americans: a potential factor in the development of obesity. Nutrition 16: 886-893.
-
Muscogiuri G, Pugliese G, Barrea L, Savastano S, Colao A (2020) Obesity: The Achilles heel for COVID-19?. Metabolism 108: 154251.
-
World Health Organization (2020) Physical inactivity: a Global Public Health Problem.
-
Ammar A, Brach M, Trabelsi K, Chtourou H, Boukhris O, et al. (2020) Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 International Online Survey. Nutrients 12(6): 1583.
-
Patterson R, McNamara E, Tainio M, De Sa TH, Smith AD, et al (2018). Sedentary behavior and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta analysis. Eur J Epidemiol 33(9): 811–829.
-
Kirwan R, McCullough D, Butler T, De Heredia F P, Davies I G, and Stewart C (2020). Sarcopenia during COVID-19 lockdown restrictions: long-term health effects of short- term muscle loss. GeroScience 42(6), 1547-1578.
- Hydrogen Peroxide Scavenging by Methanolic Extracts of Coriander: An In Vitro Antioxidant Study
- Aromatherapy in Palliative Care: A Fragrant Quest for Relief
- Empowering Women, Securing Futures: Contraception’s Role in Socioeconomic Progress in India
- Effect of Crospovidone, Croscaramellose Sodium in Combination on the Drug Release of Anti diabetic Medication in Tablet Form
- Knowledge, Attitudes, Anxiety, and Preventive Behaviors Regarding Covid-19 Affliction among Healthcare Workers in Pakistan
- “Competitive Landscape and Brand Equivalents: Implications for ANDA (Abbreviated New Drug Application) Approval”