The Spectrum and Trends of Glomerulonephritis in Bangladesh: A Single Center Study
The wide variation of the spectrum of Glomerulonephritis (GN) is noted worldwide. In Bangladesh, the spectrum and trends of GN cannot be determined definitely due to the absence of central kidney biopsy registry. The aim of this study was to see the spectrum and trends of Glomerulonephritis in our population. All the kidney biopsies were done in Shaheed Sheikh Abu Naser Specialized hospital, Khulna, Bangladesh from 2015 to 2020, and reviewed retrospectively. A total of 151 native kidney biopsies were examined by light and immunofluorescence microscopy. The mean age of the study patients was 31.3 ± 13.79 years with a range of 11-66 years, 52% were male and 48 % were female. Primary glomerulonephritis was observed in 91% of cases and secondary glomerulonephritis was in 9% of cases. Mesensialproliferative glomerulonephritis (36.48%) is on the slight decline in Bangladesh, though it still remains the commonest glomerulonephritis in this study. Membranoproliferative glomerulonephritis (27%) was the second observed GN followed by Membranous nephropathy (11.48%). Minimal change disease was observed very low in number e.g. 2.02%. Lupus Nephritis was the commonest secondary GN. Mesangialproliferative and Membranoproliferative glomerulonephritis were found in high incidence in our population. So it is essential to improve our socioeconomic and hygienic conditions for the prevention of these infection-related glomerulonephritis. This study may be helpful to establish a biopsy registry in this part of the world, which would be opened a platform for future research and planning.
Introduction
Incidence of Chronic Kidney Disease (CKD) is increasing annually worldwide [1, 2]. Glomerulonephritis (GN) is one of the leading causes of CKD and End Stage Kidney Disease (ESKD). Rashid HU stated that 25% to 45% cases of ESKD were caused by GN in developing country like Bangladesh [3, 4, 5, 6, 7]. Several studies demonstrated IgA Nephropathy is the most prevalent glomerulonephritis in Asia, Europe and America [4, 8, 9, 10]. The spectrum of the glomerular disease varies from country to country. This variation is may be due to geographical, socioeconomic, hygienic condition, genetic and racial variation [11, 12, 13, 14, 15, 16, 17]. It is known that socioeconomic and hygienic conditions vary between the countries and between the different regions of the same country. The prevalence and distribution of GN also depends on the policy and indication of kidney biopsy. The policy and indication of biopsy also differs among center to center, even in the same country [18, 19, 20, 21, 22, 23]. A kidney biopsy is the gold standard tool for the diagnosis of the specific type of GN, the disease activity, and prognosis. It also helps in treatment decision [21, 22, 23, 24, 25, 26, 27]
A central kidney biopsy registry is essential for getting a complete picture of glomerular diseases of a country or region. But Bangladesh does not have any central biopsy registry like many other developing countries [28, 29, 30, 31, 32]. Due to the lack of biopsy registry, the pattern and definitive trends of GN cannot be determined in our population. There were few studies pertaining to this entity in our country but most of them were from Dhaka, Bangladesh. The representative data including studies from other parts of the country are limited. Therefore, the aim of our study was to see the spectrum of GN in patients undergoing native kidney biopsy in this geographical area [32, 33, 34].
Data Sources and Methods
This was a cross-sectional hospital-based study. All patients with clinically diagnosed GN, who underwent native kidney biopsy performed in the department of nephrology, Shaheed Sheikh Abu Naser Specialized hospital, Khulna, Bangladesh during five years period starting from 2015, was analyzed. A total of 158 kidney biopsies were performed during this period. Out of these, 7 biopsies were inadequate (less than 5 glomeruli) and excluded from final analysis; the remaining 151 adequate biopsies were analyzed. The recorded data for each patient includes name, age, sex, an indication of kidney biopsy, histopathological diagnosis and laboratory investigations such as serum creatinine, 24- hour urinary protein, urine microscopy, virology; hepatitis B surface antigen (HBsAg), hepatitis C antibody (anti-HCV), Human Immunodeficiency Virus (HIV) and serology; anti- double stranded DNA antibody, antinuclear antibody (ANA), complements levels 3&4 (C3, C4).
All kidney biopsy specimens obtained were prepared according to the standard protocol and examined by the same renal pathologists at a single center. It was ideal for the following trends in glomerulonephritis [26, 32]. The clinical summary of the patient was available to the pathologist at the time of reporting. The biopsy policy was not changed during this study period. Informed written consent was taken prior to doing the biopsy. Kidney biopsy was performed under ultrasound guidance for all patients using Tru-cut needles with 16 G automated biopsy guns. At least two cores of tissue were obtained from each patient for light microscopy and direct immunofluorescence (DIF) techniques. For light microscopy, biopsy specimens were fixed in 10% formalin and embedded in paraffin, and sections were stained with hematoxylin and eosin (H&E), periodic acid Schiff (PAS) and silver stain in some cases [32, 33, 34]. Tissue sections were cut at 4μm thickness. The other sample was preserved in normal saline for DIF microscopy and immediately frozen. The sections were then stained with fluorescence conjugated anti-sera against human IgM, IgG, IgA, C3, and C1q. The electron microscope was not available in our country for clinical use.
The biopsy indications in diabetic patients were more selective, with biopsies undertaken only in cases of albuminuria with the absence of diabetic retinopathy, presence of hematuria, presence of active urinary sediment, less than 7 years duration of diabetes, rapid deterioration of renal function and clinical features of systemic diseases [35]. The Classification of GN (World Health Organization, Collaborating Centre for the Histological Classification of Renal Diseases) used in this paper [36]. Results were expressed as median or mean ± standard deviation for continuous data and as frequencies with percentages for categorical data. All analyses were done using SPSS version 20 (IBMCorp, Chicago, IL, USA). 𝑃 values less than 0.05 indicated statistical significance. The chi-squared test was used to investigate the statistically significant relationships between patients’ sex and different histological patterns of glomerulonephritis.
Procedure or Steps of Data Collection
All the patients of Glomerulonephritis were diagnosed clinically by a nephrologist in outpatient department of shaheed Sheikh Abu Naser Specialized hospital, Khulna. And advise for admission in inpatient department. After admission all patients were evaluated by history taking, clinical examination and proper investigations. Those who had contraindication to kidney biopsy were excluded. After taking informed written consent, kidney biopsy was done. After getting biopsy report, appropriate treatment was given to all patients. All data and relevant reports were kept in nephrology registry. At the time of study all data were retrieved nephrology registry.
Results
A total of 151 patients were included in this study. Among
them, 79 were male and 72 were female. The male to female ratio was 1.1:1. There was a slight male preponderance observed in the whole study population. A significant sexual predilection was observed only in two diseases, namely lupus nephritis, and IgA nephropathy. In all other glomerulonephritis, the sex difference was not statistically significant. A very strong female preponderance was observed in LN as shown in Table 1.
| Male | Female | N | p-value | |
|---|---|---|---|---|
| MesPGN | 25 | 29 | 54 | 0.586 |
| MPGN | 18 | 12 | 30 | 0.273 |
| MN | 10 | 7 | 17 | 0.467 |
| IgA | 10 | 3 | 13 | 0.052* |
| FSGS | 4 | 5 | 9 | 0.739 |
| IgM | 4 | 4 | 8 | 1 |
| MCD | 2 | 1 | 3 | 0.564 |
| LN | 0 | 9 | 9 | .003** |
| Crescentic | 3 | 0 | 3 | 0.083 |
| DM | 0 | 1 | 1 | 0.317 |
Table 1: Sex Distribution of Glomerulonephritis. The mean age of patients at the time of biopsy was 31.3 ± 13.79 years with a ran
| Glomerulonephritis | Age Ranges | |||||
|---|---|---|---|---|---|---|
| 20-Nov | 21-30 | 31-40 | 41- 50 | 51-60 | 61-70 | |
| MesPGN(Mean age-29.5) | 18 | 16 | 9 | 6 | 4 | 1 |
| MPGN (Mean age-34.5) | 7 | 6 | 7 | 6 | 4 | - |
| MN (Mean age-31.5) | 7 | 1 | 2 | 4 | 3 | - |
| IgA(Mean age-28.8) | 4 | 4 | 3 | 2 | - | |
| FSGS (Mean age-38.33) | 1 | 3 | 1 | 1 | 3 | - |
| IgM (Mean age-19.3) | 5 | 2 | 1 | - | - | - |
| MCD(Mean age-19.6) | 2 | - | 1 | - | - | - |
| LN (Mean age-26.5) | 2 | 5 | 1 | 1 | - | - |
Table 2: Distribution of GN in Different Age Groups.
There were no HBsAg, anti-HCV, and HIV positive patients in the biopsy cohort. In this study primary Glomerulonephritis (PGN) were the most common renal disease and accounted for 135 (91%) of the total study population as shown in Figure 1.
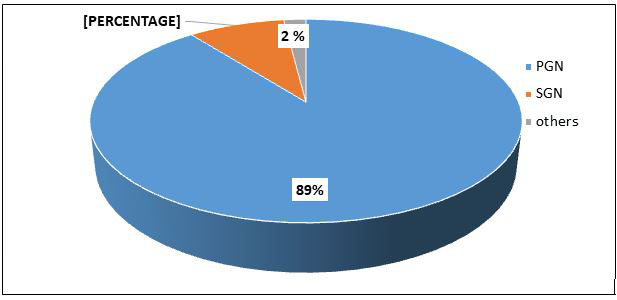
Figure-1: Distribution of Histological Diagnosis of Renal Diseases. *PGN=Primary glomerulonephritis, SGN=Secondary glomerulonephritis.
Mesangialproliferative glomerulonephritis (MesPGN) was the most common primary glomerulonephritis in 54 (36.48%) cases. Membranoproliferative glomerulonephritis (MPGN) and Membranous nephropathy (MN) came second and third in 30 (20.27%) and 17 (11.48%) cases, respectively.
Secondary glomerulonephritis (SGN) was diagnosed in 13 cases (9%) whereas Lupus Nephritis (LN) was the most common secondary glomerulonephritis seen in 9 cases (6.08%) as Shown in Table 3.
| Type of renal disease | Number of cases | Percentage |
|---|---|---|
| Primary GN:(n-135) | ||
| MesPGN | 54 | 36.48 |
| MPGN | 30 | 20.27 |
| MN | 17 | 11.48 |
| IgA | 13 | 8.78 |
| FSGS | 9 | 6.08 |
| IgM | 8 | 5.40 |
| MCD | 3 | 2.02 |
| Crescentric GN( Immune) | 1 | |
| Secondary GN: (n-13) | ||
| LN | 9 | 6.08 |
| RPGN(Pauciimmne) | 2 | 1.35 |
| DM | 1 | 0.67 |
| Ch. Sclerosing GN | 1 | 0.67 |
| Others(Non GN):n-3 | ||
| ATN | 2 | |
| Renal cortical necrosis (Large vessel vasculitis) | 1 | |
| Total | 151 |
Table 3: Histopathological Pattern of Kidney Biopsies.
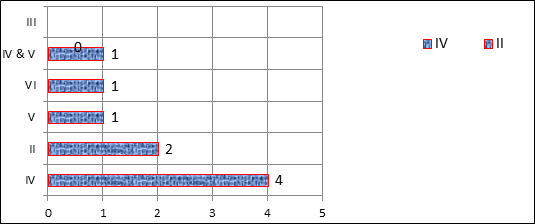
There were three cases of crescentic GN; out of which, one case showed immune complex deposition on IF and the rest of the two cases were pauci-immune. Among LN, the most common histological pattern observed was Class IV (45%) followed by Class II (22%) as Shown in Figure 2. Also a comparison of data of this study with few Bangladeshi studies is shown in Table 4.
| Components | This study | Gupta RD, et al. [42] | Islam SM, et al. [41] | Samad T, et al. [38] | Ahmed PI, et al. [39] | Habib MA, et al. [40] | Das RK, et al. [37] |
|---|---|---|---|---|---|---|---|
| N | 148 | 206 | 164 | 53 | 128 | 95 | 327 |
| Mean age (Years) | 31.3 | 34.5 | 31.39 | 42.3 | 32.92 | 30.29 | - |
| Sex M:F | 1.09:1 | 01:01.6 | 01:01.1 | 1.2:1 | 1.8:1 | 01:01.5 | 1.3:1 |
| MesPGN | 36.48% | 34.30% | 21.34% | 40.50% | 25% | 45% | 34.30% |
| MPGN | 20.27% | 12%% | 18.29% | 27% | 11.50% | 4.20% | 20.20% |
| IgA | 8.78% | 5.80% | 14.63% | - | 11.50% | 6.80% | 3.40% |
| MN | 11.48% | 3.90% | 10.37% | 8% | 22.10% | 7.30% | 10.70% |
| FSGS | 6.08% | 11.60% | 19.51% | 5.40% | 7.90% | 11.60% | 1.80% |
| LN | 6.08% | 15% | 17.68% | 11.20% | - | 6.30% | 7.90% |
| MCD | 2.02% | 5.30% | 3.40% | - | 10.60% | 10.50% | 2.10% |
| IgM | 5.40% | 2.90% | - | 1.88% | - | - | - |
Table 4: Comparisons with Few other Studies from Bangladesh.
Discussion
Our hospital is the only tertiary care center with well-developed nephrology department in this Southwestern region. Kidney biopsy was routinely done as a part of nephrological workup. As such, the pattern of glomerulonephritis observed was relatively representative of prevalent renal diseases in Southwestern Bangladesh. In this study there was a slight male predominance in the overall cases except for lupus nephritis. Some recently published studies from Bangladesh showed a similar sex distribution [37, 38, 39]. The mean age of this study population at the time of biopsy was relatively similar to other studies from Bangladesh with the exception of the study by Samad T, et al. [37, 38, 39, 40, 41] . The study by Samad T et al. was conducted in Diabetic hospital so major portion patients were diabetic and the mean age of these population was higher [5, 6, 7, 28, 29, 30, 38]. The majority of the patients who underwent kidney biopsy were in the age group of 11-30 years but no specific histological pattern observed in any age group except IgM nephropathy, MCD, and LN. Patients of these entities like MCD, IgM were in younger age group. PGN was the most common pathological lesion in this cohort followed by SGN. This result was concordant with studies from Bangladesh and other countries [38, 39, 40, 41, 42, 43, 44, 45, 46, 47].
In this study, Mesangialproliferative glomerulonephritis (MesPGN) was the most common GN. In several studies from Bangladesh also showed similar results that mean MesPGN was the commonest glomerulonephritis in Bangladesh [37, 38, 39, 40, 41, 42]. MesPGN was also one of the leading forms of glomerulonephritis in many of the Asian countries namely Singapore, Malaysia, China, Japan, Thailand, and India [11, 47, 48, 49, 50, 51, 52, 53]. Heaf also found a high prevalence of MesPGN in Denmark [5, 6, 7, 54, 55, 56, 57]. A study from Serbia, it was the second most common type of GN (28.9%) following membranoproliferative glomerulonephritis (MPGN) [15, 16, 17, 19, 20, 55, 56, 57]. However, in Singapore, Japan, China, Malaysia, and India, the frequency MesPGN has been steadily decreasing as seen in follow up and recent study [11, 56, 57, 58]. The same trend of decreasing MesPGN was also observed in the studies from Bangladesh but the change was not as remarkable as other Asian countries.
Membranoproliferative glomerulonephritis (MPGN) was the second most common glomerulonephritis found in 27 % of all cases in this study. This result was concordant with the reports from other Bangladeshi studies [17, 19, 20, 37, 38, 41]. The higher rates of MPGN were also observed in studies from Serbia and Romania [55, 59]. A study by Rabbani et al from Pakistan found MPGN to be the most common glomerulonephritis [16, 60]. It is proposed in different studies that MesPGN and MPGN are related to infection [11, 38, 61]. Patients from developing countries with poor housing facilities and sanitation exposed to parasitic, bacterial and other infective agents predisposing to MesPGN consistent with large size immune complex deposited in the mesangium and hence triggering the immune response [11, 20, 62]. The frequency of MesPGN and MPGN have been decreased in those developed countries might be due to improved sanitation, housing, and urbanization. But In Bangladesh, we are improving our socioeconomic indicators very slowly. For this reason, the frequency of MesPGN has been decreased a little in this current study in comparison with previous studies from Bangladesh.
Membranous Nephropathy was found to be the third or fourth causes of glomerulonephritis in different studies [25, 53, 63, 64, 65]. This study result regarding MN (11.48%) was similar to Das RK et al and Islam SM et al showing MN 10.7% and 10.37% respectively [37, 41]. Study from the neighboring country, India also depicted a similar frequency of MN (10%) [44, 45, 46, 47, 48]. Ibrahim S. from Egypt showed 10.93% of the GN was Membranous nephropathy [17, 19, 66]. MN is mostly idiopathic. Phospholipase A2 receptor antibody (Anti PLA2R) is an important marker for idiopathic MN. We did not perform antiPLA2R antibody in this study due to unavailability [46, 47, 67]. Bangladesh is a country with intermediate endemic hepatitis B virus (HBV) and a chronic HBV carriage rate of 2-6%.45 Some studies suggested that MN might be also related to occult Hepatitis B infection along with overt hepatitis B infection [68, 69].
IgA nephropathy (IgAN) is the commonest PGN in most of the studies throughout the world [68, 69, 70, 71, 72]. The frequency of IgAN in our country ranges from 3.4% -14.6% including this study (8.78%) [37, 39, 40, 41, 42]. Mubarak M, et al. from Pakistan in showed a very low prevalence of IgAN (2%) whereas a recent study from south India showed 21.3% of IgAN in their cohort [44, 73]. Different centers adopted different renal biopsy policies for the patient with kidney diseases especially in asymptomatic urinary abnormalities or isolated microscopic hematuria. That may be the reason for the variability of IgAN in different regions as well as the reason of the low incidence of IgAN in our country.
FSGS was low (6.08% of the GN) in this study which was identical with Samad T, et al. (5.4%) Ahmed P, et al. (7.9%) from Bangladesh [15, 38, 39]. Whereas other few studies from Bangladesh found FSGS in 11.6% and 19.5% which were slightly higher in comparison with this study [41, 42]. An increasing trend of FSGS was also observed in many developed countries like USA, Singapore, Australia, Thailand, and India [11, 16, 52, 74]. European kidney biopsy registry showed that the similar lower prevalence FSGS [31, 32, 33, 34, 55, 56, 59, 75, 76, 77]. This variation of FSGS may be due to obesity, exposure to allergens, ethnic and racial predilections.
IgM nephropathy (IgMN) is a spectrum of morphological pattern ranging from minimal change to FSGS. IgMN is more common in developing countries [13, 14, 76, 77, 78]. The frequency of IgMN varied widely from 2% – 18.5% in different literature [79, 80]. In this study, IgM nephropathy was in 5.4% of the glomerulonephritis. Samad T et al and Gupta RD et al from Dhaka, Bangladesh described IgMN in 1.88 % and 2.9% respectably [38, 42].
Minimal change disease (MCD) was rare in this study observed in 2.02% of glomerulonephritis. The mean age of study was 31.3 years. We know MCD is the most common GN in children. This finding was similar to other studies from Bangladesh [41, 42]. And other neighboring countries named Pakistan, India, and Singapore [44, 56, 81].
Lupus Nephritis (LN) was the commonest secondary GN in this study which comprises 6.09 % of total GN. Among the secondary glomerulonephritis, lupus nephritis was in 69.23%. This result was comparable with that reported in many other studies all over the world [4, 13, 73, 82, 83, 84]. Usually renal biopsy was done to see the class of LN. Like other studies, class IV LN was the most common lesion in our study [13, 14, 15, 38, 39, 85, 84]. Indication of kidney biopsy in diabetic kidney disease was mentioned in Methods.
Kidney biopsy was rarely performed in diabetes patients in our center due to the conservative biopsy approach. This might be the reason of the low prevalence of diabetic kidney disease in this study.
Limitation
One of the limitations of this study that all patients were from a single center. But this center is the only referral hospital for nephrology in this Southwestern region. Therefore this study included patients from both rural and urban areas. Another limitation of our study was the lack of electron microscopic examination of the biopsy. If it was available it can modify the diagnosis of some glomerulonephritis. But would not change the final diagnosis in most of the cases [85, 86, 87].
Conclusion
The mean age of this study population at the time of biopsy was relatively similar to other studies from Bangladesh. Primary glomerulonephritis was observed in 91% of cases and secondary glomerulonephritis was in 9% of cases. Mesensialproliferative glomerulonephritis (36.48%) is on the slight decline in Bangladesh, though it still remains the commonest glomerulonephritis in this study. Membranoproliferative glomerulonephritis (27%) was the second observed GN followed by Membranous nephropathy (11.48%). Minimal change disease was observed very low in number e.g. 2.02%. Lupus Nephritis was the commonest secondary GN. In this study, Mesangialproliferative glomerulonephritis (MesPGN) was the most common GN. In several studies from Bangladesh also showed similar results that mean MesPGN was the commonest glomerulonephritis in Bangladesh so that it could be the pathway for future research in this arena.
Funding: There is no funding support for this study
Data Availability
The datasets generated during and/or analyzed during the current study are available from the first author on reasonable request.
Code Availability
Not applicable
Compliance with Ethical Standards
There are no conflicts of interest in this study.
Ethics Approval
After getting biopsy report, appropriate treatment was given to all patients. All data and relevant reports were kept in nephrology registry. At the time of study all data were retrieved nephrology registry. All the patients of Glomerulonephritis were diagnosed clinically by a nephrologist in outpatient department of shaheed Sheikh Abu Naser Specialized hospital, Khulna, Bangladesh.
References
-
Luxardo R, Kramer A, Gonzalez BMC, Massy ZA, Jager KJ, et al. (2018) The epidemiology of renal replacement therapy in two different parts of the world: the Latin American Dialysis and Transplant Registry versus the European Renal Association-European Dialysis and Transplant Association Registry. Rev Panam Salud Publica 42: e87.
-
McCullough KP, Morgenstern H, Saran R, Herman WH, Robinson BM (2019) Projecting ESRD Incidence and Prevalence in the United States through2030. J Am Soc Nephrol 30(1): 127-135.
-
Rashid HU (2003) Nephrotic syndrome- evidence based management. Bangladesh Renal J 22: 1-4.
-
Chang JH, Kim DK, Kim W, Sun YP, Tae HY, et al. (2009) Changing prevalence ofglomerular diseases in Korean adults: A review of 20 years of experience. Nephrol Dial Transplant 24(8): 2406-2410.
-
Alexander MP, Sethi S (2019) Membranoproliferative Glomerulonephritis, Adult. In: Trachtman H, et al. (Eds) Glomerulonephritis. Springer, Cham, pp: 403-419.
-
Malaga-Dieguez L (2019) Infection-Associated Glomerulonephritis. In: Trachtman H, et al. (Eds) Glomerulonephritis. Springer, Cham.
-
Altiparmak MR, Pamuk GE, Pamuk ON, Tabak F (2002) Brucella glomerulonephritis: review of the literature and report on the first patient with brucellosis and mesangiocapillary glomerulonephritis. Scand J Infect Dis 34(6): 477-480.
-
Utsonomiya Y, Koda T, Kado T, Okada S, Hayashi A, et al. (2003) Incidence of pediatric IgA nephropathy. Pediatr Nephrol 18(6): 511-515.
-
Gesualdo L, Di Palma AM, Morrone LF, Stripolli GF, Schena FP (2004) The Italian experience of the national registry of renal biopsies. Kidney Int 66(3): 890-894.
-
Hanko JB, Mullan RN, O’Rourke DM, McNamee PT, Maxwell AP, et al. (2009) The changing pattern of adult primary glomerular disease. Nephrol Dial Transplant 24: 3050-3054.
-
Woo KT, Chan CM, Chin YM, Choong HL, Tan HK, et al. (2019) A Global Evolutionary Trend of the Frequency of Primary Glomerulonephritis over the Past Four Decades. Kidney Dis 5(4): 247-258.
-
Ashraf H, Alam NH, Rothermundt C, Brooks A, Bardhan P, et al. (2010) Prevalence and risk factors of hepatitis B and C virus infections in an impoverished urban community in Dhaka, Bangladesh. BMC infectious diseases. 10: 208.
-
Park S, Park J, Kim M, Kim JE, Yu MY, et al. (2020) Socioeconomic dependency and kidney transplantation accessibility and outcomes: a nationwide observational cohort study in South Korea. J Nephrol 34(1): 211-219.
-
Nixon AC, Brown J, Brotherton A, Harrison M, Todd J, et al. (2020) Implementation of a frailty screening programme and Geriatric Assessment Service in a nephrology centre: a quality improvement project. J Nephrol.
-
Cupisti A, Avesani CM, D’Alessandro C, Garibotto G (2020) Nutritional management of kidney diseases: an unmet need in patient care. J Nephrol 33(5): 895-897.
-
Weng H, Yang F, Chien Y, Chen P, Lin Z, et al. (2020) Lessons for the clinical nephrologist: dietary management of adult-onset type II citrullinemia in chronic kidney disease: a nutritional dilemma. J Nephrol 33(5): 1111- 1113.
-
Molcho M, Rozen-Zvi B, Shteinmats T, Dor N, Vahav I, et al. (2020) Temporal changes of proteinuria after kidney transplantation: association with cardiovascular morbidity and mortality. J Nephrol 33(5): 1059-1066.
-
Ponticelli C, Glassock RJ (2019) A definition, modern classification, and global epidemiology of primary glomerulonephritis. 2nd (Edn.), Oxford University Press.
-
Di Mario F, Regolisti G, Greco P, Maccari C, Superchi E, et al. (2020) Prevention of hypomagnesemia in critically ill patients with acute kidney injury on continuous kidney replacement therapy: the role of early supplementation and close monitoring. J Nephrol.
-
Pedrini LA, Comelli M, Ruggiero P, Feliciani A, Manfrini V, et al. (2020) Mixed hemodiafiltration reduces erythropoiesis stimulating agent’s requirement in dialysis patients: a prospective randomized study. J Nephrol 33(5): 1037-1048.
-
Hussien Y, Abdalkadim H, Mahbuba W, Hadi N, Jamil D, et al. (2020) The Nephroprotective Effect of Lycopene on Renal Ischemic Reperfusion Injury: A Mouse Model. Indian J Clin Biochem 35(4): 474-481.
-
Lim BJ (2020) The spectrum of biopsy-proven renal diseases in Korea. Kidney Res Clin Pract 39(1): 1-3.
-
Golay V, Trivedi M, Abraham A, Roychowdhary A, Pandey R (2013) The spectrum of glomerular diseases in a single center: A clinicopathological correlation. Indian J Nephrol 23(3): 168-175.
-
Fuiano G, Mazza G, Comi N, Caglioti A, Nicola LD, (2000) Current indication for renal biopsy: A questionnaire- based survey. Am J Kidney Dis 35: 448-457.
-
Das U, Dakshinamurty KV, Prayaga A (2011) Pattern of biopsy-proven renal disease in a single centerof south India: 19 years experience**.** Indian J Nephrol 21(4): 250- 257.
-
Yau T (2019) Approach to Renal Biopsy. In: Trachtman H, et al. (Eds) Glomerulonephritis. Springer, Cham, pp: 1-15.
-
Paparello JJ (2019) Diagnostic Testing in Glomerular Disease. In: Trachtman H, Herlitz L, Lerma E, Hogan J (Eds) Glomerulonephritis. Springer, Cham, pp: 29-41.
-
Anders D, Agricola B, Sippel M, Thoenes W (1977) Basement membrane changes in membranoproliferative glomerulonephritis. II. Characterization of a third type by silver impregnation of ultra-thin sections. Virchows Arch A Pathol Anat Histol 376(1): 1-19.
-
Burkholder PM, Marchand A, Krueger RP (1970) Mixed membranous and proliferative glomerulonephritis. A correlative light, immunofluorescence, and electron microscopic study. Lab Invest 23(5): 459-479.
-
Khan MA, Akhtar M, Taher SM (1988) Membranoproliferative glomerulonephritis in a patient with primary Sjogren’s syndrome. Report of a case with review of the literature. Am J Nephrol 8(3): 235-239.
-
Larsen CP, Messias NC, Walker PD, Fidler ME, Cornell LD, et al. (2015) Membranoproliferative glomerulonephritis with masked monotypic immunoglobulin deposits. Kidney Int 88(4): 867-873.
-
Marini G, Gabriele PW, Tanghetti B, Castellani A, Olivetti G, et al. (1976) Membranoproliferative glomerulonephritis associated with infected ventriculoatrial shunt. Report of two cases recovered after removal of the shunt. Mod Probl Paediatr 18: 207-210.
-
Rodriguez-Poncelas A, Coll-de-Tuero G, Blanch J, Comas- Cufí M, Saez M, et al. (2018) Prediabetes is associated with glomerular hyperfiltration in a European Mediterranean cohort study. J Nephrol 31(5): 743-749.
-
Schüttler D, Schönermarck U, Wenner F, Toepfer M, Rizas ED, et al. (2020) Large potassium shifts during dialysis enhance cardiac repolarization instability. J Nephrol.
-
Espinel E, Agraz I, Ibernon M, Fort J, Seron D (2015) Renal biopsy in Type 2 diabetic Patients. J clin Med 4(5): 998-1009.
-
Jacob C (1987) Renal Disease: Classification and Atlas of glomerular diseases.
-
Das RK, Saleh AF, Kabir AN, Talukder SI, Kamal M (2008) Immunofluorescence studies of Renal Biopsies. Dinajpur Med Coll J 1: 8-13.
-
Samad T, Iqbal S, Haque WMM, Rahim MA, Haque HF (2016) Histopathological Pattern of Glomerulonephritis: Experience from BIRDEM General Hospital, Dhaka, Bangladesh. BIRDEM Med J 6(2): 67-73.
-
Ahmed PI, Zaman SU, Jahan F, Gupto RD, Chowdhury MN, et al. (2014) Pattern of primary Glomerulonephritis in Dhaka Medical College Hospital, Bangladesh. Bangladesh J Medicine 25: 42-46.
-
Habib MA, Badruddoza SM (2012) Pattern of glomerular diseaseamong adults in Rajshahi, the northern region of Bangladesh. Saudi J kidney Dis Transpl 23(4): 876-80.
-
Islam MJI, Haque WS, Akhter S, Alam SMM (2018) Histomorphological Pattern of Renal Biopsy in Dhaka: A Single Center Study. Saudi J kidney Dis Transpl 29(5): 1159-1164.
-
Gupta RD, Mamun AA, Morshed SM, Roy GC, Ahsan HMN (2019) Pattern of Glomerulonephritis in Bangladesh-A Single Center Study at a tertiary care hospital. KI REPORTS 4(7): S316.
-
Chowdry AM, Bhat MA, Najar MS, Sharma A, Azad H, et al. (2018) Pattern of Glomerulonephritis in the Kashmir Valley. Saudi J kidney Dis Transpl 29(5): 1192-1198.
-
Mubarak M, Kazi JL, Naqvi R, Ahmed E, Akhter F, et al. (2011) Pattern of renal disease observed in native renalbiopsies in adult in a single center in Pakistan. Nephrology 16: 87-92.
-
AlYousef A, AlSahow A, AlHelal B, Alqallaf A, Abdallah E, et al. (2020) Glomerulonephritis Histopathological Pattern Change. BMC Nephrology 21(1): 186.
-
Hashmi AA, Hussain ZF, Edhi MM, Mumtaz S, Faridi N, et al. (2016) Insight to changing morphologic patterns of glomerulopathy in adult Pakistani patients: an institutional perspective. BMC Res Notes 9: 73.
-
Prathap K, Looi LM (1982) Morphological patterns of glomerular disease in renal biopsies from 1000 Malaysian patients. Ann Acad Med Singap 11(1): 52-56.
-
Khoo JJ (2001) Renal biopsies in Johor: a 7-year study. Malays J Pathol 23(2): 101-104.
-
Li LS, Liu ZH, (2004) Epidemiologic data of renal diseases from a single unit in China: analysis based on 13,519 renal biopsies. Kidney Int 66(3): 920-923.
-
Chen H, Tang Z, Zeng C, Hu W, Wang Q, et al. (2003) Pathological demography of native patients in a nephrology center in China. Chin Med J (Engl) 116(9): 1377-1381.
-
Honma M, Toyoda M, Umezono T, Kato M, Kobayashi K, et al. (2008) An investigation of 2,093 renal biopsies performed at Tokai University Hospital between 1976 and 2000. Clin Nephrol 69(1): 18-23.
-
Parichatikanond P, Chawanasuntorapoj R, Shayakul C, Choensuchon B, Vasuvattakul S, et al. (2006) An analysis of 3,555cases of renal biopsy in Thailand. J Med Assoc Thai S2: S106-111.
-
Balakrishnan N, John GT, Korula A, VisalakshiJ, Talaulikar GS, et al. (2003) Spectrum of biopsy proven renal disease and changing trends at a tropical tertiary care centre 1990-2001. Indian J Nephrol. 13(1): 29-35.
-
Heaf J, Lokkegaard H, Larsen S (1999) The epidemiology and prognosis of glomerulonephritisin Denmark 1985- 1997. Nephrol Dial Transplant 14(8): 1889-1897.
-
Naumovic R, Pavlovic S, Stojkovic D, Basta JG, Nesic V (2009) Renal biopsy registry form a single centre in Serbia: 20 years of experience. Nephrol Dial Transplant 24(3): 877-885.
-
Xu X, Ning Y, Shang W, Li M, Ku M, et al. (2016) Analysis of 4931 renal biopsy data in central China from 1994 to 2014. Ren Fail 38(7): 1021-1030.
-
Bavanandan S (2012) LSK: 5th Report of the Malaysian Registry Of Renal Biopsy. Chapter 2: Primary Glomerulonephritis, pp: 19-51.
-
Golay V, Trivedi M, Abraham A, Roychowdhary A, Pandey R (2013) The spectrum of glomerulardiseases in a single center: A clinicopathological correlation. Indian J Nephrol 23(3): 168-175.
-
Covic A, Schiller A, Volovat C, Gheorghe G, Paul GT, et al. (2006) Epidemiology of renal disease in Romania**:** a 10 year review of two regional biopsy databases. Nephrol Dial Transplant 21: 419-424.
-
Rabbani MA, Memon GM, Ahmad B, Memon S, Tahir SA, et al. (2012) Percutaneous renal biopsy results: a retrospective analysis of 511 consecutive cases. Saudi J Kidney Dis Transpl 23(3): 614-618.
-
Hurtado A, Johnson RJ (2005) Hygiene hypothesis and prevalence of glomerulonephritis. Kidney Int 68(S97): s62-67.
-
Woo KT, Chiang GS, Edmondson RP, Wu AY, Lee EJ, et al. (1986) Glomerulonephritisin Singapore: an overview. Ann Acad Med Singap 15(1): 20-31.
-
Choi In J, Jeong HJ, DS Han, Lee JS, Choi KH, et al. (2001) An analysis of 4,514 Cases of Renal Biopsy in Korea. Yonsei Med J 42(2): 247-254.
-
(1999) Nationwide and Long-Term Survey of Primary Glomerulonephritis in Japan as Observed in 1,850 Biopsied Cases. Research Group on Progressive Chronic Renal disease. Nephron 82(3): 205-213.
-
Rychlik I, Eva J, Tesa V, Alexander K, Jiri L, et al. (2004) The Czech registry of renal biopsies. Occurrence of renal diseases in the years 1994-2000. Nephrol Dial Transpl 19(12): 3040-3049.
-
Ibrahim S, Fayed A, Fadda S, Belal D (2012) A five-year analysis of the incidence of glomerulonephritis at Cairo University Hospital-Egypt. Saudi J Kidney Dis Transpl 23(4): 866-870.
-
Rathi M, Bhagat RL, Mukhopadhyay P, Kohli HS, Jha V, et al. (2014) Changing histologic spectrum of adult nephrotic syndrome over five decades in north India: a single center experience. Indian J Nephrol 24(2): 86-91.
-
Kong D, Wub D, Wang T, Li T, Xu S, et al. (2013) Detection of viral antigens in renal tissue of glomerulonephritis patients without serological evidence of hepatitis B virus and hepatitis C virus infection. Int J Infect Dis 17(7): e535-e538.
-
Floege J, Amann K (2016) Primary glomerulonephritides. Lancet 387(10032): 2036-2048.
-
Riispere Z, Ots-Rosenberg M (2012) Occurrence of kidney diseases and patterns of glomerular disease based on a 10-year kidney biopsy material: A retrospective single- centre analysis in Estonia. Scand J Urol Nephrol 46(5): 389-394.
-
Sugiyama H, Yokoyama H, Sato H, Saito T, Kohda Y, et al. (2013) Japan Renal Biopsy Registry and Japan Kidney Disease Registry: Committee Report for 2009 and 2010. Clin Exp Nephrol 17(2): 155-173.
-
Xie J, Chen N (2013) Primary glomerulonephritis in mainland China: An overview. Contrib Nephrol 181: 1-11.
-
Bandi VK, Nalamati A, Kasinaboina B, Chundru SS (2019) Epidemiologic data ofbiopsy-proven renal diseases: Experience from a single center in SouthIndia. Saudi J Kidney Dis Transpl 30(2): 478-491.
-
Sim JJ, Batech M, Hever A, Harrison TN, Avelar T, et al. (2016) Distribution of biopsy-proven presumed primary glomerulonephropathies in 2000-2011 among a racially and ethnically diverse US population. Am J Kidney Dis 68(4): 533-544.
-
Carvalho E, do Sameiro Faria M, Nunes JPL, Sampaio J, Valbuena C (2006) Renal diseases: a 27-year renal biopsy study. J Nephrol 19(4): 500-507.
-
Rivera F, Lopez-Gomez JM, Perez-Garcia R (2004) Clinicopathologic correlations of renal pathology in Spain. Kidney Int 66(3): 898-904.
-
Schena FP (1997) Survey of the Italian Registry of Renal Biopsies. Frequency of the renal diseases for 7 consecutive years. The Italian Group of Renal Immunopathology. Nephrol Dial Transplant 12(3): 418-426.
-
Mubarak M, Kazi JI (2012) IgM Nephropathy Revisited. Nephrolurol Mon 4(4): 603-608.
-
Mubarak M, Kazi JI, Shakeel S, Lanewala A, Hashmi S, et al. (2011) Clinicopathologic characteristics and steroid response of IgM nephropathy in children presenting with idiopathic nephrotic syndrome. APMIS 119(3): 180-186.
-
Cohen AH, Border WA, Glassock RJ (1978) Nehprotic syndrome with glomerular mesangial IgM deposits. Lab Invest 38(5): 610-619.
-
Chandrika BK (2007) Non-neoplastic renal diseases in Kerala, India - Analysis of 1592 cases, a two year retrospective study. Indian J Pathol Microbiol 50(2): 300-302.
-
Krishna A, Vardhan H, Singh PP, Kumar O (2018) Analysis of Native Kidney Biopsy: Data from a Single Center from Bihar, India**.** Saudi J Kidney Dis Transpl 29(5): 1174- 1180.
-
Khakurel S, Agrawal RK, Hada R (2015) Pattern of Glomerular Disease in Nepal: A Single-center experience. Saudi J Kidney Dis Transpl 26(4): 833-838.
-
Wang H, Ren YL, Chang J, Gu L, Sun LY (2017) A Systematic Review and Meta-analysis of Prevalence of Biopsy- Proven Lupus Nephritis. Arch Rheumatol 33(1): 17-25.
-
Collan Y, Hirsimaki P, Aho H, Wuorela M, Sundstrom J, et al. (2005) Value of electron microscopy in kidney biopsy diagnosis. Ultrastruct Pathol 29(6): 461-468.
-
Jegatheesan D, Nath K, Reyaldeen R, SivasuthanG, John GT, et al. (2016) Epidemiology of biopsy-proven glomerulonephritis in Queensland adults. Nephrology (Carlton) 21(1): 28-34.
-
Ganesh K, Nair RR, Seethalekshmy NV, Kurian G, Mathew A, et al. (2018) A Study of Clinical Presentation and Correlative Histopathological Patterns in Renal Parenchymal Disease. Indian J Nephrol 28(1): 28-34.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines