Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
South Sudan continues to face recurrent outbreaks of malaria, cholera, and measles due to intersecting pressures from conflict, mass displacement, weak health-system performance, and climate variability. This paper examines epidemiological trends from 2016–2025 and analyzes the systemic and environmental determinants contributing to recurrent epidemics among displaced populations. Using a mixed-methods approach—combining surveillance data, national reports, and One Health and Health System Maturity analyses—the study identifies core gaps in governance, financing, service delivery, climate preparedness, and multisectoral coordination. Findings show pronounced vulnerability among flood-affected and conflictimpacted counties, where weak routine immunization, poor WASH conditions, and drought-and-flood cycles intensify disease transmission. The absence of an operational One Health platform further constrains epidemic preparedness. A Humanitarian-Resilient Health System Framework is proposed to enhance epidemic intelligence, strengthen Boma-level service delivery, integrate climate-informed early warning, and expand domestic financing for community health.
Abbreviations
BHI: Boma Health Initiative; IDP: Internally Displaced Populations; EPI: Expanded programme on Immunization; HPF: Health Pooled Fund; CHS: Community Health System; EWS: Early Warning System; NMS: National Management System; PPP: Public–Private Partnerships; UHC: Universal Health Coverage; IHR: International Health Regulations; MoH: Ministry of Health; MTEF: Medium-Term Expenditure Framework; PFM: Public Financial Management; RDQA: Routine Data Quality Assessments.
Introduction
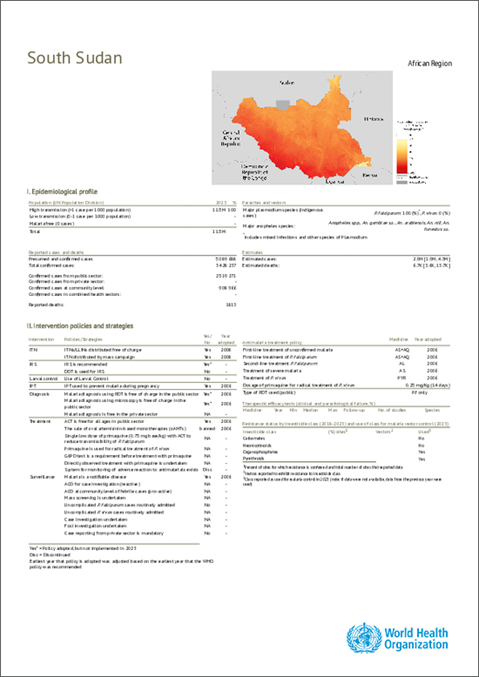
South Sudan, emerging from protracted conflict, remains highly susceptible to epidemic-prone diseases, particularly among displaced and flood-affected populations. Recurrent malaria, cholera, and measles outbreaks reflect the combined pressures of population mobility, weak infrastructure, inadequate immunization coverage, and worsening climate extremes. The country’s fragile health system—anchored by the Boma Health Initiative (BHI) has not yet matured sufficiently to deliver reliable community- based surveillance, prevention, and care. Although policy frameworks exist, operationalization is hindered by limited financing, governance fragmentation, and insufficient multisectoral collaboration.
The intersection of conflict, climate, and systemic weaknesses necessitates an integrative approach grounded in One Health principles and health-system resilience. This study provides an epidemiological and systems-level analysis of the drivers of recurrent outbreaks, with recommendations for a more sustainable, climate-resilient, and community- centered response.
Methods
Study Design
A mixed-methods sequential explanatory design integrated quantitative surveillance data with qualitative document analysis to explore epidemiological patterns and systemic determinants of outbreaks in South Sudan [1].
Quantitative Data Sources
- MoH DHIS2 (2016–2025): Morbidity and mortality data for malaria, cholera, and measles.
- WHO Country Dashboards and Weekly Epidemiological Records: Trend validation and outbreak timelines.
- UNICEF Situation Reports: WASH (Water, Sanitation and Hygiene conditions), Internally displaced populations (IDP) estimates, and the Expanded programme on Immunization (EPI) performance.
- Climate Data: Flood maps and rainfall anomalies from UN OCHA, FAO, and the South Sudan Meteorological Authority.
Quantitative Analysis
Descriptive analyses produced incidence, attack rates, and case-fatality ratios. Trend analysis and seasonality plots examined associations between climate events and disease peaks. Pearson correlations assessed relationships between rainfall anomalies and outbreak intensity [2].
Qualitative Data and Analysis
Over 40 national, donor, and humanitarian documents— including the BHI Policy, Health pooled fund (HPF) reports, MoH–ICHESS Maturity Assessment (2024), and climate- risk profiles—were reviewed to identify themes related to governance, financing, service delivery, and coordination.
Analytical Framework
Two conceptual models guided interpretation: 1. WHO Health System Building Blocks—for structural determinants of vulnerability. 2. One Health Framework—for multisectoral risk drivers across human, animal, and environmental systems [3].
Ethics
The study used secondary data aggregated at national/ state levels under MoH data-sharing protocols [4]. No individual identifiers were used.
Results
Epidemiological Trends
Table 1 Malaria remains hyperendemic, contributing over 40% of outpatient attendance annually, with rising caseloads since 2016. Cholera outbreaks show strong seasonality, peaking in high-flood years (2016–2017, 2021–2022). Measles resurged sharply between 2020–2024, driven by disruptions to routine immunization during COVID-19 and persistent access barriers in insecure counties.
| Year | Malaria Cases (000s) | Malaria Deaths | Cholera Cases | CFR (%) | Measles Cases | Immunization Coverage (%) | Major Drivers |
|---|---|---|---|---|---|---|---|
| 2016 | 2,700 | 3,200 | 18,000 | 2.1 | 3,500 | 49 | Conflict, WASH collapse |
| 2017 | 2,950 | 3,400 | 12,500 | 1.9 | 2,800 | 52 | Flooding, displacement |
| 2018 | 3,100 | 3,100 | 2,200 | 1.2 | 5,000 | 57 | Insecurity, stock-outs |
| 2019 | 3,350 | 3,600 | 3,400 | 1.5 | 4,600 | 59 | Weak surveillance |
| 2020 | 3,700 | 3,900 | 5,600 | 2 | 7,200 | 54 | COVID-19 disruption |
| 2021 | 3,850 | 4,000 | 6,100 | 1.7 | 8,000 | 53 | Flood displacement |
| 2022 | 4,100 | 4,200 | 8,500 | 2.3 | 5,500 | 58 | Heavy rainfall |
| 2023 | 4,300 | 4,100 | 4,200 | 1.6 | 9,000 | 61 | EPI gaps |
| 2024 | 4,450 | 4,000 | 1,200 | 1.1 | 6,800 | 64 | Improved access |
Table 1: Disease Burden in South Sudan, 2016–2024 (DHIS2 data trends).
South Sudan’s disease burden from 2016–2024 reveals a health system under chronic strain, characterized by rising endemic infections, recurrent epidemics, and widening inequities between rural, urban, and displaced populations. These patterns are further exacerbated by persistently low DHIS2 reporting completeness averaging only 44% nationally which limits the accuracy of disease trend interpretation and early outbreak detection [4].
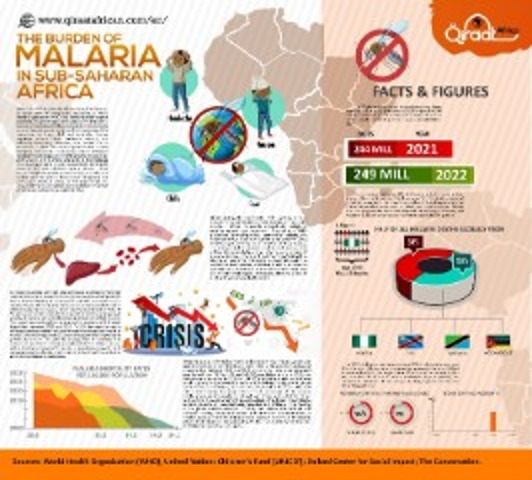
Malaria remains the country’s leading cause of illness and death. Reported cases increased from 2.7 million to 4.45 million approximately a 65% rise while deaths increased from 3,200 to 4,000. This escalation reflects the combined effects of climate shocks, expansive flooding, displacement, and poor access to timely treatment, particularly in rural and hard-to-reach settings. Despite some gains in diagnostic availability, mortality remains high due to late care-seeking and fragile PHC systems [5, 6]. Rural areas such as Jonglei, Unity, Upper Nile, and Lakes continue to experience the most intense transmission, whereas urban areas benefit from comparatively better access to diagnosis and treatment [5, 6, 7, 8].
Cholera shows a cyclical epidemic pattern. Major outbreaks occurred in 2016–2017 and again from 2020–2022, each with high case-fatality ratios (1.1–2.3%), exceeding the WHO target of <1%. Although DHIS2 reported only 1,200 cases for 2024, WHO documented a large national outbreak beginning in late 2024 linked to mass returnee movements from Sudan, indicating that national figures represent partial or under-reported data [9]. Cholera transmission is highest in overcrowded informal settlements, urban IDP camps, and rural riverine communities where WASH infrastructure is weak or non-existent.
Measles outbreaks recurred nearly every 1–2 years throughout the period, with major spikes in 2018, 2020– 2021, and 2023. Routine immunization coverage improved gradually from 49% to 64%, yet remains far below the ≥95% herd-immunity threshold required to prevent sustained outbreaks [10]. Zero-dose and under-immunised children are disproportionately concentrated in remote, mobile, and displaced communities, where irregular outreach services, poor cold-chain access, and insecurity hinder coverage expansion [11]. States with low reporting completeness (<40%) consistently underestimate measles incidence, complicating timely outbreak response [4].
Substantial rural–urban and displacement disparities persist. Rural areas bear the heaviest burden of malaria, diarrhoeal diseases, pneumonia, measles, and maternal deaths due to distance to facilities, limited outreach services, and weaker PHC/BHI structures. Urban and peri-urban centres—including Juba, Wau, Bor, Malakal, and Renk— experience explosive outbreaks of cholera, measles, hepatitis E, and COVID-19 because of population density, slum expansion, and collapsing sanitation systems [12, 13]. IDP camps and border hubs combine both risk profiles, acting as epidemic amplifiers that seed infections into surrounding counties.
These epidemiological patterns are driven by reinforcing structural determinants. Protracted conflict continues to disrupt health services, destroy infrastructure, and displace populations [13]. Climate shocks, including unprecedented flooding since 2019 and cycles of drought and heavy rainfall, have expanded mosquito breeding habitats and intensified cholera transmission through WASH damage [13]. WASH collapse in both rural communities and urban slums sustains recurrent cholera, hepatitis E, and high baseline childhood diarrhoea [13]. Primary health care and community health systems remain fragile, with incomplete BHI rollout, shortages of salaried staff, irregular supervision, and continued dependence on external financing. Low and inequitable immunization coverage, combined with repeated service disruptions during conflict and COVID-19, has left large pockets of vulnerable children susceptible to measles and cVDPV2 outbreaks [11]. High levels of acute and chronic malnutrition further weaken immunity and elevate disease severity.
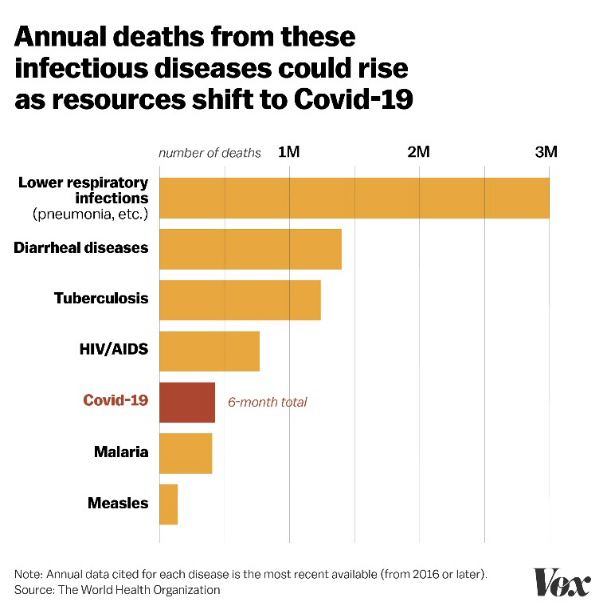
As a result, South Sudan faces a cluster of priority epidemic-prone diseases, including malaria and kala- azar; cholera, hepatitis E, and AWD; measles, cVDPV2, and meningitis; acute respiratory infections; COVID-19; TB; and HIV, all of which are magnified in fragile, overcrowded, and climate-vulnerable settings [12, 13]. The combined pressures of conflict, environmental instability, displacement, and systemic fragility create a perpetual “acute-on-chronic” emergency Figures 1-4.
In summary, the 2016–2024 trends underscore four key implications
- Endemic diseases such as malaria and measles are intensifying, especially in rural and flood-prone regions.
- Epidemic-prone infections—including cholera and measles—follow a predictable boom-and-bust cycle driven by climate shocks, displacement, and poor immunization coverage.
- System shocks such as COVID-19 and major flooding rapidly reverse health-system gains and create large pools of susceptible populations.
- Without strengthened community health systems, resilient WASH, climate-adaptive planning, improved surveillance, and increased domestic financing, South Sudan will remain vulnerable to recurrent, large-scale epidemics Tables 2-9.
Graphical Figure / Infographic: Disease Burden Trends, 2016–2024
- Infographic: Major Disease Burden Trends in
- South Sudan (2016–2024)
- Cholera
- Major outbreaks: 2016–17, 2020–22, 2024
- CFR often >2%, above WHO target
- Urban informal settlements + riverine rural areas most affected
Table 2: Cholera.
- Malaria
- Cases ↑ from 2.7M → 4.45M
- Deaths fluctuating 3,200 → 4,000
- Highest in rural flood-prone counties
- Strong link to climate shocks and displacement
Table 4: Malaria.
- Measles
- Recurrent outbreaks nearly every 1–2 years
- Immunization improved 49% → 64%, still far below herd immunity
- Rural + mobile populations have greatest zero-dose burden
Table 6: Measles.
- Reporting Completeness
- National average: ≈44%
- Only a minority of States >70%
- Underestimation of disease burden likely by 30–50%
Table 9: Reporting Completeness.
- Infographic Panel
- Cholera: Cyclic Epidemics
- 🔄 Large outbreaks every 2–3 years
- 🚨 CFR consistently above global standards
- 🏙 Outbreaks concentrate in urban slums & IDP camps
- 🌊 Rural riverine communities also high-risk
Table 3: Cholera: Cyclic Epidemics
- Rising Malaria Burden
- 📈 65% increase in cases (2016–2024)
- 🌧 Driven by floods, stagnant water, weak LLIN replacement
- 🏥 Rural mortality > urban mortality
Table 5: Rising Malaria Burden.
- Measles: Persistent Outbreaks
- 📉 Suboptimal immunization – slow gains
- 👶 Large zero-dose population
- 🚑 Severe outbreaks during service disruptions
- (COVID-19, flooding)
Table 7: Measles: Persistent Outbreaks.
- Low Reporting Rates Undermine Detection
- ⚠ Only 44% of facilities consistently reporting
- 🧭 Weakening accuracy of burden estimation
- 📉 States with low reporting show delayed outbreak detection
Table 8: Low Reporting Rates Undermine Detection.
Discussion
The findings of this study underscore the complex interplay between system immaturity, climate vulnerabilities, humanitarian dependence, and weak governance structures, all of which heighten the risk of recurrent epidemics in South Sudan. Understanding these dynamics is essential for designing interventions that not only respond to current outbreaks but also build long-term resilience. The following discussion examines the systemic weaknesses identified, explores the risk factors that perpetuate disease transmission and operational fragility, and outlines context-appropriate mitigation strategies [14].
System Maturity and Foundational Gaps
The Community Health System (CHS), implemented through the Boma Health Initiative (BHI), remains in an early stage of institutional maturity, as indicated by national assessments and maturity analyses [15, 16, 17, 18]. Despite the presence of an overarching policy framework, translation into consistent practice is hindered by foundational weaknesses—fragmented governance, poor supervision, weak data systems, and dependence on external financing.
Key Risk Factors 1. Fragmented Governance and Implementation Gaps Although governance structures exist at national and subnational levels, coordination remains inconsistent. The absence of standardized implementation modalities results in geographic disparities and partner-driven parallel systems that undermine uniformity and quality [15, 17].
2. Weak Supportive Supervision Only 35% of counties reported conducting quarterly supervision of BHWs, limiting accountability, mentorship, and early performance correction. Weak supervision contributes directly to stock-outs, low motivation, inconsistent community engagement, and reduced service quality [17, 18].
3. Inadequate Community Data Systems Approximately 75% of counties lack functional family folders or community registers, weakening surveillance and microplanning. Poor data quality an acknowledged challenge in post-conflict settings—compromises outbreak detection and resource allocation [4, 10, 11].
4. Financing Dependency Over 87% of community health funding originates from external donors [18]. This dependency results in funding volatility, workforce instability, and limited predictability in supply-chain operations.
5. Mitigation Strategies Strengthening CHS maturity requires robust governance reforms, consistent supervision, standardized tools, digital transformation, and increased domestic financing. Evidence suggests that structured governance compacts, digital data systems (CHMIS–DHIS2 integration), and predictable financing improve performance even in fragile contexts [12, 19].
Climate and Environmental Vulnerability
Climate variability—particularly recurrent floods and drought cycles—significantly shapes disease transmission dynamics in South Sudan. More than 60% of the country experiences seasonal flooding, which heightens malaria and cholera transmission, destroys WASH infrastructure, and displaces households [7, 14, 20].
Key Risk Factors 1. Flood-Driven Vector-Borne Disease Transmission Flooding creates stagnant water that favors Anopheles mosquito breeding. Surveillance data consistently link malaria surges to hydrological anomalies and seasonal flooding patterns [5, 6].
2. Waterborne Disease Outbreaks Floods frequently damage boreholes and sanitation systems, forcing reliance on contaminated water sources conditions strongly associated with cholera transmission [9, 13, 20].
3. Limited One Health Operationalization Although One Health is endorsed in national frameworks, operationalization remains weak due to inadequate financing, limited technical capacity, and unclear cross- ministerial mandates [19, 20, 21, 22, 23, 24].
4. Displacement and Livelihood Disruptions Flood-induced displacement forces populations into crowded settlements with poor WASH services, increasing vulnerability to cholera, measles, and AWD outbreaks [7, 8].
5. Mitigation Strategies Mitigation requires operationalization of a functional One Health Secretariat, climate-informed early warning systems (EWS), integration of meteorological and disease data, climate-resilient infrastructure investments, and community-level adaptation initiatives. These approaches are supported by global evidence linking climate adaptation to reduced epidemic severity [14, 20].
Humanitarian Dependence and Donor Fragmentation
Humanitarian partners provide essential services due to limited fiscal space but often operate parallel systems characterized by short funding cycles, vertical programming, and inconsistent reporting [21, 22].
Key Risk Factors 1. Parallel Systems and Fragmentation Vertical programs malaria, EPI, nutrition use separate supervision, reporting, and procurement systems, undermining government ownership and integration [12, 17].
2. Short-Term Funding Cycles Humanitarian funds often span 6–12 months, limiting long-term workforce stability, supply reliability, and institutional capacity development [21, 22].
3. Weak and Uneven Supply Chain Support Emergency procurement often bypasses national systems (NMS), contributing to persistent stock-outs and weak last-mile distribution [15, 21].
4. Mitigation Strategies Mitigation requires alignment behind a government-led Community Health and PHC Investment Plan (2025–2030), multi-year donor transition frameworks, integration of parallel systems into national LMIS/DHIS2 platforms, and joint government–partner annual reviews. Global analyses confirm that such alignment advances health sovereignty and improves efficiency in fragile contexts [22].
Weak Public–Private Partnerships (PPP)
Despite PNFP and FBO providers delivering nearly 60% of health services, South Sudan lacks a formalized PPP ecosystem to leverage private-sector innovation, logistics capacity, and financing [19].
Key Risk Factors 1. Absence of Policy and Legal Frameworks Lack of formal PPP guidelines limits structured engagements and discourages private investment in key areas such as solar cold-chain systems, diagnostics, and supply-chain operations.
2. Limited Private Sector Confidence Political instability, currency volatility, and unclear regulatory environments deter investment in health services and digital health solutions.
3. Weak Linkages Between Private Providers and National Systems Local pharmacies, private clinics, and NGOs remain underutilized in national surveillance, supply chains, and coordinated service delivery [19].
4. Mitigation Strategies Developing a national PPP policy, establishing a PPP Unit within MoH, contracting private logistics firms, expanding digital health PPPs, and formalizing service agreements with PNFP/FBO providers can significantly strengthen health system performance. Experiences from comparable fragile settings show strong returns on PPP investments in cold- chain, supply-chain, and digital health systems [19, 21].
5. Synthesis of Findings The convergence of structural system weaknesses, climate vulnerabilities, donor-driven fragmentation, and underdeveloped PPP frameworks creates a fragility–epidemic trap in which outbreaks become recurrent and predictable. Breaking this cycle requires comprehensive reforms that strengthen governance, improve climate-smart health systems, expand domestic financing, align humanitarian and development actors under a unified national plan, and operationalize a multisectoral One Health approach.
These findings align with global evidence demonstrating that resilience in fragile contexts emerges from sustained investment in governance, climate adaptation, community systems, and multisectoral collaboration [12, 14, 20, 21].
Limitations of the Study
This study has several limitations that should be acknowledged when interpreting the findings. First, the analysis relies heavily on secondary data sources, particularly the DHIS2 platform, WHO and UNICEF situation reports, and national assessments. In South Sudan, routine surveillance data often suffer from incomplete reporting, inconsistent data quality, and delayed submissions, especially in conflict- affected and flood-prone counties where health facilities are non-functional or inaccessible. This limitation may lead to underestimation or misclassification of disease burden, particularly for cholera and measles outbreaks in remote settlements and internally displaced persons (IDP) camps.
Second, population denominators used for incidence estimates are based on projections rather than verified census data, due to the absence of nationwide census since 2008. High mobility, displacement, and return migration introduce uncertainties that may affect trend interpretation and inter- county comparisons. These demographic fluctuations also limit the precision of immunization coverage estimates and disease attack rates.
Third, the qualitative component draws from policy documents, evaluations, and humanitarian reports rather than primary interviews. While these sources offer valuable insights into systemic constraints, they may not fully capture local perspectives, frontline challenges, and community-level innovations within Boma and Payam settings. A stronger ethnographic or participatory component would enhance the granularity of findings.
Fourth, climate-related analyses—though supported by OCHA, FAO, and meteorological datasets—are constrained by limited longitudinal environmental data and incomplete integration of hydrological and ecological indicators. This may understate the full complexity of climate–disease interactions, including vector ecology, water systems collapse, and land-use changes.
Finally, the study was conducted in a rapidly evolving humanitarian and political landscape, where ongoing subnational conflict, seasonal floods, and donor reprogramming can shift priorities and operating conditions. These dynamics impose constraints on generalizability and necessitate cautious interpretation when projecting future epidemic trends or recommending national-level reforms.
Despite these limitations, triangulation across multiple datasets and alignment with global evidence provide confidence in the overarching patterns and conclusions presented.
Implications for Policy, Practice, and Research
The findings have significant implications for South Sudan’s health sector, humanitarian operations, and global health discourse, particularly in contexts characterized by fragility, conflict, and climate stress.
National Policy and Health System Implications The systemic weaknesses identified highlight an urgent need for comprehensive health system strengthening, anchored in the Boma Health Initiative and aligned with national decentralization reforms. Strengthening governance, institutionalizing supportive supervision, and accelerating digital transformation through CHMIS–DHIS2 integration are essential for improving surveillance, service delivery, and accountability. The evidence demonstrates that community health—if properly resourced—is the backbone of epidemic preparedness and resilience. Domestic financing reforms, including earmarked budget lines, PPP legislation, and fiscal space expansion, are critical for sustainability as external funding declines.
Implications for Humanitarian Operations and Donor Engagement The study underscores the need for donors and humanitarian partners to shift from fragmented, short-term interventions toward coordinated, multi-year, government- led investment models. Donor transitions should be sequenced with capacity-building, predictable funding for BHW incentives, and integration of parallel systems into national structures. Humanitarian adaptation strategies must increasingly incorporate climate risk modelling, anticipatory action, and alignment behind the national One Health framework.
Implications for One Health and Climate Adaptation Planning The findings reinforce the urgency of operationalizing One Health in South Sudan. Human disease outbreaks cannot be fully understood or effectively mitigated without integrating animal health, environmental monitoring, hydrological forecasting, and community-level reporting. Climate adaptation strategies—including flood-resilient infrastructure, ecosystem monitoring, and strengthened WASH systems—are essential for reducing the recurrent cycles of malaria, cholera, and other climate-sensitive diseases. South Sudan’s context highlights the importance of designing climate-smart primary health care models for fragile ecologies.
Implications for Regional and Global Health Security South Sudan’s epidemic vulnerabilities have wider implications for the East and Central African region. Cross- border population movements, livestock migration, and transboundary ecosystems mean that recurrent outbreaks pose risks beyond national borders. Strengthening surveillance, early warning systems, and laboratory capacity contributes to regional health security under the International Health Regulations (IHR 2005). For global health, South Sudan exemplifies the intersection of fragility, climate change, and infectious disease threats, underscoring the need for differentiated approaches to universal health coverage (UHC) and global preparedness frameworks.
Implications for Future Research The study exposes several areas where further empirical research is needed:
- Longitudinal analyses integrating climate, hydrological, and ecological data with epidemiological trends.
- Mixed-methods research capturing community-level lived experiences of epidemics, WASH disruptions, and displacement.
- Rigorous impact evaluations of digital tools (CHMIS, mHealth, geospatial surveillance) on data quality and outbreak detection.
- Studies on public–private partnerships, exploring the feasibility of local manufacturing, solar cold-chain systems, and community logistics models.
- Implementation research assessing How One Health can be operationalized in fragile, decentralized settings.
- Future research should prioritize participatory approaches and invest in local research institutions to strengthen national ownership of evidence generation.
Policy and Programmatic Recommendations
Building a climate-resilient, community-anchored, and sustainable health system in South Sudan requires coordinated investments across governance, surveillance, financing, service delivery, digital transformation, and multisectoral collaboration. The following recommendations synthesize the epidemiological, systemic, and environmental vulnerabilities revealed in the findings and are grounded in evidence from national assessments and global frameworks on health systems in fragile contexts [12, 14, 17, 19, 21, 23].
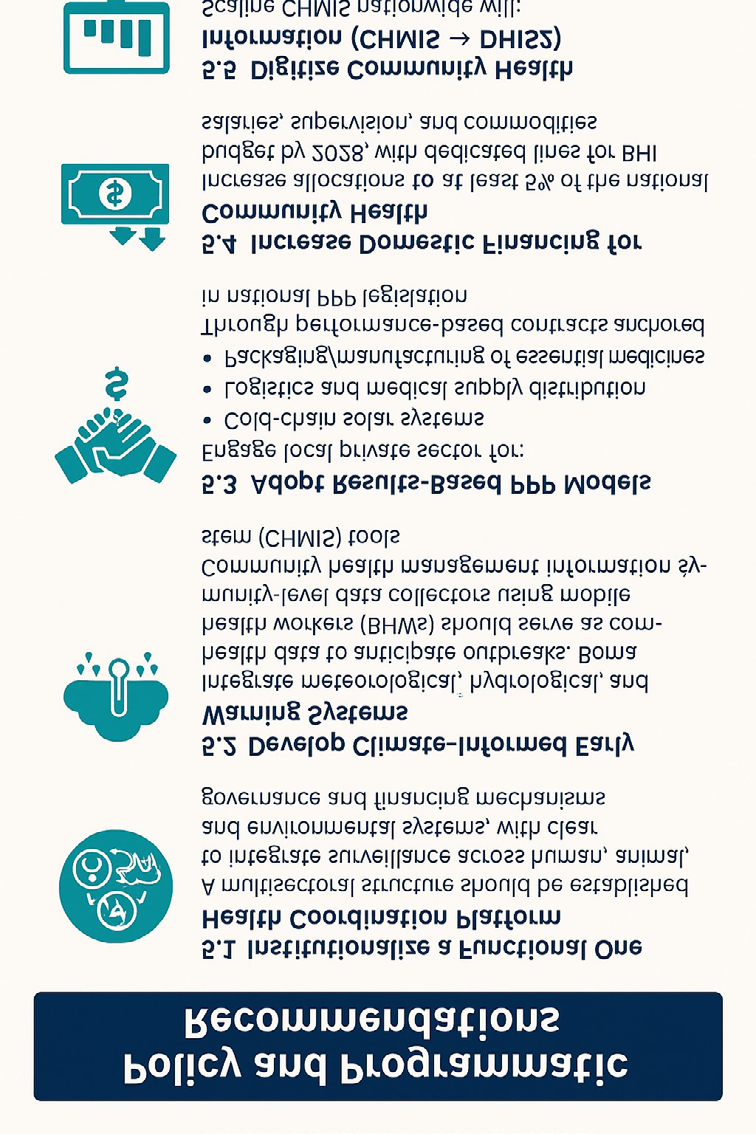
Institutionalize a Functional One Health Coordination Platform
South Sudan’s high burden of zoonotic and climate- sensitive diseases including malaria, cholera, and emerging infectious threats requires a multisectoral approach that integrates human, animal, and environmental health systems. Although a One Health framework has been endorsed at the national level, operationalization remains weak due to insufficient financing, fragmented mandates, and lack of cross-ministerial coordination [19, 24].
Rationale
- Outbreaks in South Sudan frequently emerge at the interface of livestock movement, water contamination, vector ecology, and population displacement domains that cannot be addressed through the health sector alone [13, 14].
- Evidence from the One Health approach demonstrates improved epidemic preparedness when human, veterinary, and environmental surveillance systems share data and conduct joint analyses [20, 24].
Key Actions
- Establish a fully operational One Health Secretariat hosted jointly by the Ministry of Health (MoH), Ministry of Livestock and Fisheries, and Ministry of Environment.
- Develop a unified One Health governance framework defining roles, data-sharing protocols, and joint- response mechanisms.
- Allocate a specific annual national budget to support multisectoral surveillance and joint outbreak investigations.
- Integrate BHWs and community structures into the One Health surveillance pipeline for early risk detection.
Expected Impact A functional One Health platform enhances epidemic intelligence, supports integrated responses to zoonotic and waterborne outbreaks, and strengthens compliance with International Health Regulations (IHR) [23].
Develop Climate-Informed Early Warning Systems
Climate change is a key structural determinant of disease transmission in South Sudan, with more than 60% of counties experiencing recurrent flooding that accelerates malaria vector proliferation, disrupts WASH systems, and facilitates cholera spread [7, 14, 20]. Current disease surveillance systems rely primarily on retrospective case reporting, limiting the ability to predict and prevent outbreaks.
Rationale
- Surveillance data reveal that malaria and cholera peaks correlate closely with hydrological and rainfall patterns [5, 6].
- Integrating seasonal climate forecasts with epidemiological signals has been shown globally to improve timely pre-emptive interventions, particularly in flood-affected environments [14].
Key Actions
- Integrate meteorological, hydrological, and health surveillance data into a national Climate-Informed Early Warning System (EWS).
- Use satellite imagery and flood-intensity modelling (OCHA, FAO) to identify hotspots at risk of vector or waterborne outbreaks [7].
- Enable BHWs to serve as community-level data collectors, reporting environmental and disease indicators through CHMIS mobile tools [4].
- Pre-position essential supplies (RDTs, ACTs, ORS, chlorine) in areas predicted to flood before the rainy season.
Expected Impact A climate-informed EWS enables anticipatory action, reduces disease burdens, and supports targeted allocation of scarce resources in fragile contexts.
Adopt Results-Based Public–Private Partnership (PPP) Models
South Sudan’s health system depends heavily on humanitarian partners, yet the domestic private sector— including PNFPs, faith-based organizations, logistics firms, and community pharmacies—remains underutilized [19, 21]. A well-structured PPP framework can expand capacity for supply-chain resilience, cold-chain maintenance, diagnostics, and digital health solutions.
Rationale
- Private and FBO facilities provide nearly 60% of health services in South Sudan [19].
- PPP models in fragile settings have successfully strengthened cold-chain systems, last-mile distribution, and the availability of essential medicines through results-based contracting [22].
- Macroeconomic shocks and currency volatility necessitate risk-sharing mechanisms to attract investment.
Key Actions 1. Develop and adopt national PPP legislation for health, defining contractual modalities, risk-sharing, and performance metrics.
2. Engage private renewable-energy firms to deploy solar- powered cold-chain systems, especially in off-grid counties. 3. Contract private logistics companies for last-mile distribution using performance-based payment systems. 4. Support domestic manufacturing and packaging of essential medicines, including ORS, zinc, and malaria commodities. 5. Integrate private providers into national HMIS and supply-chain reporting, ensuring accountability and alignment.
Expected Impact Results-based PPPs reduce stock-outs, lower operational costs, expand renewable-energy solutions, and strengthen national health sovereignty.
Increase Domestic Financing for Community Health
South Sudan allocates less than 2% of its national budget to health—far below the Abuja Declaration target of 15% [22] and insufficient to sustain essential community services without donor subsidy. Community health funding depends on external partners for 87% of its financing [18], posing significant risks as humanitarian financing declines.
Rationale
- Predictable financing is essential for BHW salaries, supervision, commodity availability, and continuity of services [17].
- Global evidence shows that even incremental increases in domestic financing for PHC improve access, reduce child mortality, and increase resilience to shocks [21].
Key Actions
- Increase domestic community health funding to at least 5% of the national health budget by 2028, with ring- fenced allocations for BHI salaries and supervision.
- Create a National Community Health Investment Fund supported by domestic taxes, diaspora contributions, and catalytic donor grants.
- Integrate BHI financing into the Medium-Term Expenditure Framework (MTEF) to strengthen predictability.
- Adopt gender-responsive and climate-sensitive public financial management (PFM) tools to ensure equitable distribution of funds.
Expected Impact Strengthened domestic financing enhances sustainability, improves health worker motivation, reduces reliance on humanitarian budgets, and supports long-term system resilience.
Digitize Community Health Information Systems (CHMIS → DHIS2)
Reliable, timely data are critical for outbreak detection, resource allocation, and performance monitoring. Yet community-level data remain largely paper-based, incomplete, and delayed in most counties [4, 10, 17]. Digitizing CHMIS and integrating it with national DHIS2 will significantly modernize surveillance and enhance decision- making.
Rationale
- Digital health systems improve timeliness and completeness of reporting, especially in dispersed, hard- to-reach contexts [12].
- CHMIS pilots in South Sudan have demonstrated improved accuracy of community reporting and early identification of local disease clusters (MoH/ICHESS) [17].
Key Actions
- Scale CHMIS nationwide to capture household-level health data, disease alerts, zero-dose mapping, and WASH indicators.
- Integrate CHMIS outputs into DHIS2 dashboards, enabling real-time visualization of community trends at national and county levels.
- Train BHWs, supervisors, and CHD teams in digital data entry, analysis, and feedback loops to ensure data quality.
- Equip frontline workers with mobile devices and offline- capable tools to support reporting during network disruptions.
- Institutionalize routine data quality assessments (RDQA) to ensure reliability and accuracy.
Expected Impact Digitization strengthens epidemic intelligence, enhances accountability, accelerates response times, and provides the data infrastructure needed for climate-informed decision- making.
Conclusion of Recommendations
Together, these policy and programmatic recommendations provide a roadmap for transitioning South Sudan from a humanitarian-dependent health landscape to a resilient, climate-adaptive, digitally enabled, and community- driven health system. Implementing these strategies will strengthen epidemic preparedness, enhance equity, and advance progress toward universal health coverage (UHC) in one of the world’s most fragile settings.
Conclusion
South Sudan’s epidemic vulnerability is shaped by the intersecting forces of protracted conflict, climate variability, systemic fragility, and widespread population displacement. These structural determinants amplify the transmission of malaria, cholera, measles, and other climate- and conflict- sensitive diseases, while simultaneously constraining the capacity of national and subnational systems to prevent, detect, and respond to outbreaks. The Boma Health Initiative (BHI) remains a critical and visionary platform for extending primary health care to the last mile; however, its transformative potential is undermined by persistent gaps in financing, governance coherence, and operational maturity, alongside limited integration of One Health principles.
This paper demonstrates that epidemic control in South Sudan cannot rely on fragmented humanitarian responses or short-term emergency programming. Instead, it requires a Humanitarian-Resilient Health System Framework— one that strengthens national ownership, institutionalizes climate-adaptive and multisectoral approaches, and ensures continuity of essential community-based services across crises. Such a framework must embed predictable domestic financing, robust coordination mechanisms, climate- informed early warning systems, strengthened community health systems, and digital transformation capable of delivering timely, actionable intelligence.
If implemented cohesively and sequenced within a national roadmap, these reforms can fundamentally shift South Sudan’s health trajectory—from reactive outbreak response to proactive epidemic preparedness, from fragmented service delivery to integrated community health systems, and from external dependency to long-term national resilience. The convergence of climate change, demographic pressures, and shifting humanitarian financing makes this transition not only urgent but indispensable. Investing in resilient, community-anchored, One Health–aligned primary health care is therefore the most strategic and sustainable path toward safeguarding population health, strengthening health security, and advancing South Sudan’s progress toward universal health coverage (UHC).
Acknowledgements
This work is dedicated to the blessed memory of my beloved parents, Mr. John Agbo and Mrs. Janet Agbo, whose unwavering love, sacrifice, and guidance laid the foundation for every step of my life and career. Their legacy of integrity, compassion, and service continues to inspire my commitment to improving health and humanity.
I extend my deepest gratitude to my loving children and grandchildren, whose encouragement, patience, and joy strengthen my purpose and sustain my resolve.
I also acknowledge the duty bearers, colleagues, and friends—across government, academia, multilateral agencies, and community structures—who tirelessly strive to make the public health space, and indeed the world, a better and more equitable place. Their dedication and partnership continue to shape and advance the vision of resilient, people- centered health systems.
To all who contribute, openly or quietly, to the survival, dignity, and wellbeing of vulnerable communities, I offer my profound appreciation.
Conflict of Interest
The author declares no conflict of Interest References
1. Creswell JW, Plano Clark VL (2018) Designing and conducting mixed methods research. 3rd(Edn.), SAGE.
2. Global Fund (2024) South Sudan country portfolio review and sustainability assessment.
3. ICHESS (2024) Community Health System (CHS) maturity and foundational elements assessment report. Ministry of Health, South Sudan.
4. Intergovernmental Panel on Climate Change (2022) Climate change 2022: Impacts, adaptation and vulnerability. Cambridge University Press.
5. Integrated Food Security Phase Classification (2023) IPC acute food insecurity analysis: South Sudan. IPC Global Support Unit.
6. McMichael AJ, Woodruff RE, Hales S (2006) Climate change and human health: Present and future risks. The Lancet 367(9513): 859-869.
7. Ministry of Health (MoH), Republic of South Sudan (2023) Boma Health Initiative (BHI) review and PHC system assessment.
8. Ministry of Health, Republic of South Sudan (2024) DHIS2 reporting completeness summary.
9. Ministry of Health & UNICEF (2023) Community health financing and partnership review. MoH & UNICEF.
10. OCHA (2023) South Sudan humanitarian needs overview 2023. United Nations Office for the Coordination of Humanitarian Affairs.
11. Spiegel PB, Checchi F, Robinson C, Gross R (2021) Health- care needs of people affected by conflict: Future trends and changing frameworks. The Lancet 397(10273): 2036-2047.
12. UNHCR (2024) South Sudan regional refugee response plan. United Nations High Commissioner for Refugees.
13. UNICEF (2023) Children on the move and zero-dose mapping in South Sudan. UNICEF.
14. WHO & UNICEF (2024) Immunization coverage estimates: South Sudan, 2016–2024 (Joint Reporting Form).
15. World Bank (2023) South Sudan public expenditure review: Fiscal space for health and education.
16. World Health Organization (2010) Monitoring the building blocks of health systems: A handbook of indicators and their measurement strategies.
17. World Health Organization (2022) Health systems in fragile settings: Strengthening governance and partnerships.
18. World Health Organization (2023) World malaria report 2023.
19. World Health Organization (2024a) Global Health Observatory: Malaria and vector-borne diseases.
20. World Health Organization (2024b) Cholera outbreak updates: South Sudan 2024–2025. WHO Regional Office for Africa.
21. WHO Communicable Diseases Network (2023) Communicable disease patterns and epidemic risks in South Sudan. World Health Organization.
22. WHO Health Emergencies Programme (2023) South Sudan Health Cluster and PHSA updates.
23. World Medical Association (2013) Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 310(20): 2191-2194.
24. Zumla A, Dar O, Kock R, Muturi M, Ntoumi F, et al. (2016) Taking forward a One Health approach for zoonotic pathogens. The Lancet Infectious Diseases 16(5): e268-e275.
- Measuring What Matters: Data Gaps, Certificate of Need Reform, and Pediatric Psychiatric Inpatient Capacity in North Carolina
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines