Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
Euthanasia is one of the most controversial aspects, not only in medicine but also in other fields such as ethics, law, sociology, ontology, philosophy, etc. This is because it involves a decision in which a patient's life is ended with their absolute consent and supervised by a medical team. Currently, only ten countries have legalized euthanasia. The first of these was the Netherlands on April 1, 2002, and subsequently followed by Belgium (2002), Luxembourg (2009), Colombia (2014), Canada (2016), Spain (2021), New Zealand (2021), Portugal (2023), Cuba (2023), and Ecuador (2024). Uruguay has approved the euthanasia bill in the Chamber of Deputies (2025), and its respective treatment in the Senate is still pending for it to become law. Thus, of the 195 currently recognized countries, only 5.12% have legalized euthanasia. Given that euthanasia is a highly controversial topic due to its moral, ethical, and regulatory contradictions, there is an urgent need to implement a corresponding regulatory framework in those countries that still lack one.
Abbreviations
ACHR: The American Convention on Human Rights; ICCPR: International Covenant on Civil and Political Rights; UDHR: Universal Declaration of Human Rights; ADHR: The American Declaration of the Rights and Duties of Man; WHO: World Health Organization.
Introduction
The principle of autonomy of the will implies that people can establish and regulate their own interests, desires, and values, and thus freely decide about their own lives, always within the legal and moral limits established for a given time and place. Autonomy of the will is essential for the full realization of human dignity and personal development. This context is subsumed within a broader aspect, the right to self- determination, a right embodied in the power of a person or a society to decide about their own future, not only in their personal sphere but also in economic, social, and cultural aspects. Thus, autonomy of the will is an essential structural element of self-determination, with self-determination being the genus and autonomy of the will being the species.
The autonomy of will is a right with broad legal recognition. In Argentina, it is not only based at the national level (through our Constitution and regulatory laws) but has also been incorporated normatively in international treaties with constitutional hierarchy (Article 75, paragraph 22) since the constitutional reform of 1994.
International treaties equate the concept of autonomy of will with the notion of freedom and dignity. This has at least three consequences: 1) on the personal level, it grants a person the possibility of making their own decisions; 2) in the social sphere, it is manifested through the viability of a voluntary agreement in the non-patrimonial sphere, giving rise to a right to family life; and 3) in the business context, it entails the possibility of entering into contracts.
The American Convention on Human Rights (ACHR), in its Article 11, paragraph 1, establishes that everyone has the right to respect for their honour and recognition of their dignity (as a consequence of the adequate exercise of their autonomy of will), a concept consistent with its articles 5.2, 6, 22, and 27. Furthermore, a broad body of legislation is consistent with this legal position: article 5 of the American Declaration of the Rights and Duties of Man (ADHR); articles 10, 14, and 17 of the International Covenant on Civil and Political Rights (ICCPR); article 1 of the Universal Declaration of Human Rights (UDHR); article 12 of the Universal Declaration of Human Rights (UDHR).
Tripartite Moralistic Contradiction of Principles Implicit in Euthanasia
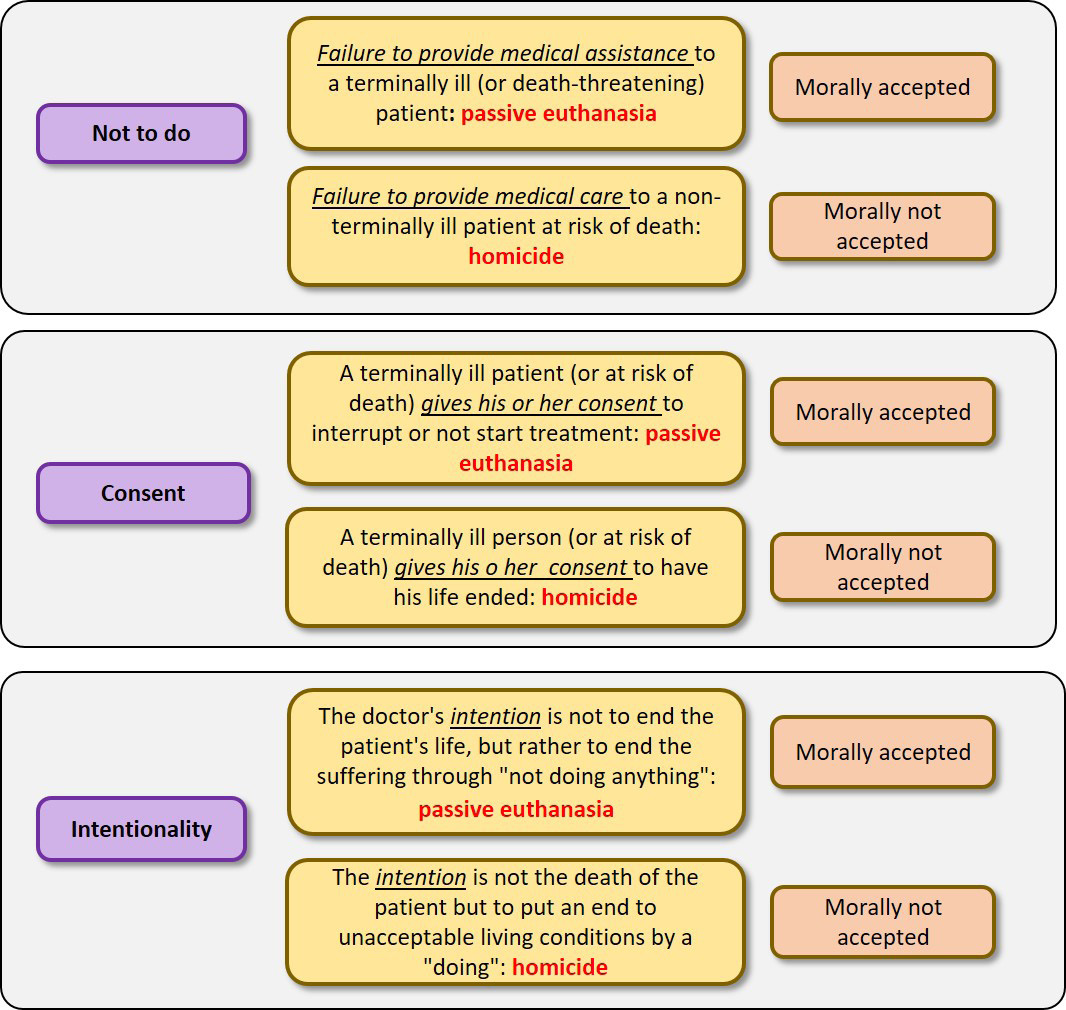
Proponents of the conceptual and moral divergence between passive and active euthanasia find support in the natural course of the disease, closely linked to the physician’s “failure to act.” According to this position, active euthanasia would interrupt the “natural course” of the disease, ending the patient’s life, a morally rejected situation. In contrast, passive euthanasia would “respect” the intrinsic nature of the disease1, and death would be a consequence of “natural evolution,” allowing nature to take its course and therefore a morally accepted situation, where the physician “fails to act or performs an action by omission.” This position’s main criticism is that the natural course of the patient’s condition is modified by appropriate and timely therapeutic interventions, and the interruption of these interventions (disconnection from mechanical ventilation) is what effectively causes death, morally equating passive euthanasia with active euthanasia. Furthermore, in the event that a physician deliberately denies professional care to a patient at risk of death and the patient dies, the healthcare professional is not exempt from liability by claiming that he or she allowed the disease to “run its natural course.” On the contrary, it would be an act classified as homicide (classified as an act of omission) under current regulations, as he or she is deemed to have a reprehensible attitude. In this case, the physician also “fails to act,” as with passive euthanasia, which inevitably raises certain questions: What makes the same conduct (a failure to act or an act of omission) morally opposed in both situations? Why is the conduct of withholding care for a non-terminal patient reprehensible, but not for a terminal patient?
For passive euthanasia to be legally and morally accepted, the patient’s consent is an essential requirement, since disconnection against the patient’s will would constitute homicide. Now, if the difference between “killing” and allowing someone to “die” lies fundamentally in the patient’s consent, what would the difference be in cases where the patient gives consent for active euthanasia? A clash of moral principles is inevitable in this position that differentiates active from passive euthanasia.
Completing this analysis, we incorporate the third variable: the intention of the treating professional. From this perspective, the balance or proportionality between the therapeutic objective and the side effects of a given therapeutic approach is analysed. Every medical action has two potential effects: the intended or beneficial effects and the undesirable or collateral effects. In clinical practice, consideration of the risk-benefit ratio is part of proper due diligence in medical action, which Thomson defines as the “doctrine of double effect.”6 This relationship conceives the potential for causing harm as an inseparable variable of a therapeutic action. Potential harm is subsumed within the permissible risk of medical practice. A given medical indication should maintain adequate proportionality where
1 This doctrinal position is applicable in cases of advance di- rectives (Law 26.529, art. 11), specifically to cases of non-connection, where the natural evolution of the patient’s condition is effectively re- spected since no therapeutic procedure is initiated.
the benefit outweighs the risks to be considered viable. From this perspective, the action is morally permissible and accepted. It is at this point where professional intentionality takes on a very important feature because the doctrine requires that an action maintain proportionality between both effects and that the intention of the professional has not pursued the harmful effects of the act in order to achieve the beneficial objective. This argument, applied to the difference established above between active and passive euthanasia, leads us to interpret that, in consented passive euthanasia, the action of ceasing to act pursues the beneficial objective of alleviating the patient’s suffering; the physician’s intention is not to end the patient’s life, but rather to end the suffering as a primary and fundamental objective. This is the proportionality of the double effect. Translated to active euthanasia or assisted suicide, this argument would imply that the end sought is not the death of the patient but rather to put an end to the unacceptable living conditions they endure as a consequence of their illness (Figure 1).
Once again, we find ourselves in a moral collision of conflicts. Current legislation mandates imprisonment for active euthanasia. So, if the physician’s intention is primarily to relieve the patient (and not death) in an intolerable condition, would this represent a justification and, therefore, an exception to the penalty? If in situations where a professional, having previously obtained the patient’s consent, considers the patient’s suffering intolerable and/or undignified (intentionality) and ends life, why is this same situation legally punishable in the case of active euthanasia when the benefit of the action (ending the suffering with prior consent) outweighs the undesirable effect (death)?
Beyond the extremely difficult task of assessing professional intentionality, the theory of double effect could place the physician’s intention in a higher order of priority over the patient’s intention.
At this point, it is inevitable to consider Kant’s deontological theories regarding the morality of human action. Kant establishes that man is a person who belongs to two worlds: the sensible and the intelligible. The former is subject to the laws of nature, and the latter is subject to the laws of reason. Consequently, human actions can be determined by both reason and inclinations (thus alleviating the epistemological tension between empiricism and rationalism). Based on this conception, Kant defines three classes of acts, with their corresponding examples [9]:
Acts contrary to duty: These are morally incorrect. For example, a merchant who charges less experienced buyers a higher price for his goods.
Acts in accordance with duty: These are morally neutral. Here, Kant distinguishes between acts performed out of mediate inclination (for example, if a merchant sells his merchandise to everyone at the same price because it is convenient for his business, he does not act this way because duty demands it, but because this act is a means to a desired end) and those performed out of immediate inclination (for example, if the merchant sells his merchandise to everyone at the same price out of love for humanity). In both cases, he acted in accordance with duty (he charged the merchandise the price he owed), but not out of duty. His inclinations (interests, desires, and passions) were the reason for his actions. Kant establishes that these acts deserve praise and encouragement but not esteem.
Acts of duty: These are morally correct acts. In this case, the merchant should charge everyone the same price, even if this would be against his interests and he had no desire to act this way. For Kant, these are the acts that have moral value.
For this reason, the right to die should be interpreted as an act of duty, thus ensuring equal treatment.
In conclusion, we can conclude that the procedural measures of passive euthanasia (disconnection from mechanical ventilation) have no relevant moral difference from the procedures used in active euthanasia, such as the administration of lethal drugs. A common denominator in all the positions analyzed is the patient’s request or consent. If the patient’s consent is present in both practices, then we are faced with unequal treatment for the same request. This inevitably leads to the question of the vulnerability of the right to equality contained in the normative body of Article 16 of the National Constitution and its legal concordances. Is the legal axiom that states “equality for equals under equal conditions” true?
An aspect closely linked to euthanasia is that, in our country, active euthanasia, but not passive euthanasia, constitutes simple homicide according to Article 79 of the Penal Code (CP), and medically assisted suicide is punishable as complicity in suicide according to Article 83 of the CP, in addition to the provisions regarding the prohibition of euthanasia practices in Articles 2 and 11 of Law 26,742.
In conclusion, it can be stated that euthanasia is an extremely sensitive procedure from various perspectives; it implies the imperative need to reconcile not only legal and medical aspects, but also philosophical, ethical, moral, historical, cultural, economic, sociological, dikeological, and ontological aspects, among others. This context gives euthanasia a necessary integrative, experimental, and three- dimensional approach. In this context, euthanasia has been and continues to be widely analyzed, debated, contradicted, and legally accepted.
Current Situation in Argentina
The lack of legislation on euthanasia practices leads to punishable medical care practices, aggravated by medical personnel’s lack of knowledge. Therefore, adequate and urgent regulation of euthanasia practices is essential.
To establish a situational assessment of medical procedures and euthanasia in Argentina, a strictly anonymous survey was conducted among a group of medical professionals in the city of Rosario. The survey was sent to 79 physicians. It included qualitative and quantitative data structured into 16 questions. Among the most significant questions related to this work, only the following four will be presented: • Have you received training regarding euthanasia in your current workplace?
• Do you agree with euthanasia practices?
• Have you ever assisted a patient in dying?
• How did you help a patient die?
The results are listed below.
- Have you received training regarding euthanasia in your current workplace?
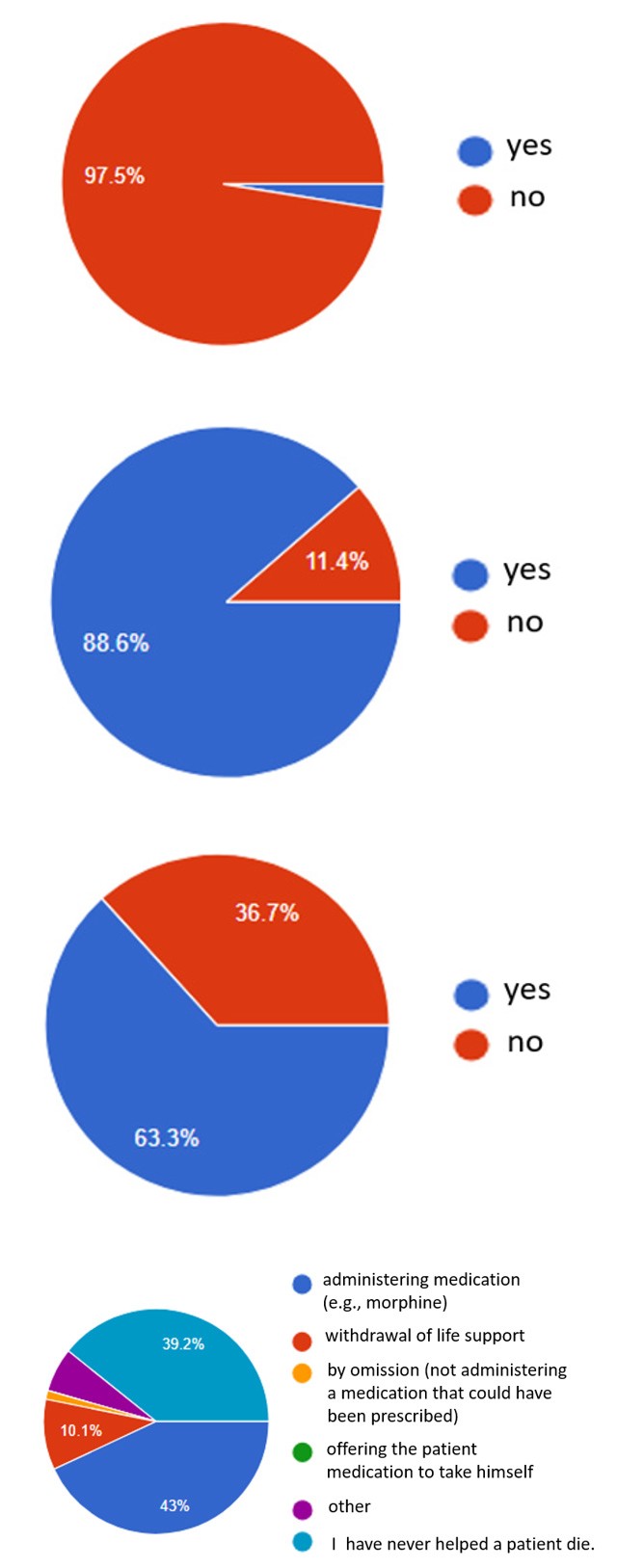
- Do you agree with euthanasia practices?
- Have you ever assisted a patient in dying?
- How did you help a patient die?
The human right to live with dignity reciprocally implies the right to die with dignity. Otherwise, the person is forced to “prolong their existence for a short time, when they do not wish it and suffer profound affliction, amounts not only to cruel and inhuman treatment, but also to the nullification of their dignity and autonomy as a moral subject.”2,3 Euthanasia practices have historically been a source of argumentative confrontations, not only legal but also philosophical, medical, spiritual, and even metaphysical. Our current legal system suffers from a serious problem in that it does not establish a definition of “euthanasia.” Not only does it reveal a definitional deficiency, but it also permits passive euthanasia (without express reference) by offering a normative framework for it by referring to “the refusal of surgical procedures, artificial resuscitation, or the withdrawal of life-support measures...” and also to “...the refusal of hydration or feeding procedures...” But, contradictorily, the same law states: “Directives must be accepted by the attending physician, except for those that involve euthanasia practices, which will be deemed nonexistent.” This contradiction should be interpreted as an error within our institutional background.
References
-
Stewart, Biobasics: Suicide and Euthanasia, p: 15 2. Harris NM (2001) The euthanasia debate. 147(3): 360- 370. 3. Álvarez Del Río Asunción, Practice and Ethics of Euthanasia. pp: 24-25. 4. Art. 260 CCCN “A voluntary act is one executed with discernment, intention and freedom, which is manifested by an external fact.” 5. Rodriguez-Arias D Portal de Éticas aplicadas. 6. Thomson JJ (1999) Physician-assisted suicide: two moral arguments. Ethics 109: 497-518. 7. Kluge EW (1981) The ethics of deliberate death. National University Publications, Nueva York. 8. Rachel J (1988) Euthanasia matters of life and death. New Introductory Essays in Moral Philosophy. Random House, New York. 9. Kant I (1981) Groundwork for the Metaphysics of Morals, 2 File 4597-D-2021. Honorable Chamber of Deputies of the Na- tion. Retrieved on February 24, 2022, from: https://www4.hcdn.gob.ar/dependencias/dsecretaria/Periodo2021/ PDF2021/TP2021/4597-D-2021.pdf File 2577/2021. Honorable Senate of the Nation. Retrieved on February 24, 2022, from: https://www.senado.gob.ar/parlamentario/comisio- nes/verExp/2577.21/S/PL. 3 File 2577/2021. Honorable Senate of the Nation. Retrieved on February 24, 2022 from: https://www.senado.gob.ar/parlamentario/comisiones/ verExp/2577.21/S/PL
- Measuring What Matters: Data Gaps, Certificate of Need Reform, and Pediatric Psychiatric Inpatient Capacity in North Carolina
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines