Measuring What Matters: Data Gaps, Certificate of Need Reform, and Pediatric Psychiatric Inpatient Capacity in North Carolina
Access to pediatric inpatient psychiatric services is increasingly constrained, yet statewide psychiatric infrastructure remains difficult to measure due to fragmented and inconsistent public reporting systems. This study examined the relationship between Certificate of Need (CON) reform, infrastructure visibility, and the measurability of pediatric inpatient psychiatric capacity in North Carolina. A cross-sectional health policy and infrastructure analysis was conducted using publicly accessible regulatory, licensing, organizational, and secondary reporting systems. The analysis evaluated the extent to which pediatric psychiatric infrastructure could be identified and quantified across facility types and reporting pathways. A total of 16 facilities and health system entities were identified as providing or planning paediatric inpatient psychiatric services in North Carolina. Among these, 12 facilities had publicly measurable pediatric psychiatric bed counts, while 4 acknowledged paediatric psychiatric services without reporting quantitative capacity information. Freestanding psychiatric hospitals were substantially more visible within regulatory reporting systems than hospital-based psychiatric units. Most measurable paediatric psychiatric bed counts were derived from historical Certificate of Need findings and approval documents. These findings suggest that fragmented reporting environments limit statewide behavioural health planning and infrastructure assessment. The inability to consistently measure paediatric psychiatric capacity represents a healthcare infrastructure and policy problem in itself.
Parks A¹*, Workman K¹, Lazari M² and McCart A1
¹Department of Nutrition and Healthcare Management, Appalachian State University, USA ²Baptist Health, Louisville, Kentucky, USA
Introduction
Access to inpatient psychiatric services for children and adolescents has emerged as a growing concern across the United States, with increasing rates of depression, anxiety, suicidality, and emergency department utilization among pediatric populations [1, 2, 3, 4]. North Carolina is the ninth most populous state in the United States, with more than 11.2 million residents and approximately 2.3 million individuals under age 18 [5]. The state includes a mixture of densely populated urban centers and large rural regions, creating substantial variation in healthcare infrastructure and behavioral health service availability. Similar to many states, North Carolina has experienced increasing demand for pediatric behavioral health services while facing ongoing concerns regarding psychiatric workforce shortages, emergency department boarding, and inpatient psychiatric bed availability [6]. Despite growing demand for behavioral health services, the ability to evaluate whether inpatient psychiatric capacity is sufficient to meet population needs remains limited by fragmented and inconsistent reporting systems [6, 7, 8]. Although several national healthcare infrastructure datasets maintained by organizations such as the Centers for Medicare & Medicaid Services (CMS), the American Hospital Association (AHA), and state licensing agencies report inpatient hospital and psychiatric facility information, pediatric inpatient psychiatric capacity is frequently absent, inconsistently categorized, or aggregated within broader psychiatric service classifications. As a result, publicly accessible national datasets often do not allow reliable identification or measurement of pediatric psychiatric bed availability specifically. This limitation affects not only North Carolina, but also broader national efforts to evaluate pediatric psychiatric infrastructure, geographic access, psychiatric boarding, and behavioral health system adequacy. While national studies have documented shortages in pediatric psychiatric bed availability and substantial geographic variation in access [8, 9, 10, 11, 12], less attention has been given to the infrastructure required to measure and monitor inpatient psychiatric capacity at the state level [13, 14].
Nationally, pediatric inpatient psychiatric capacity remains limited and unevenly distributed. Recent analyses have estimated that pediatric psychiatric bed availability averages approximately 14–16 beds per 100,000 children nationwide, with substantial variation across states and regions [15]. These differences have contributed to growing concerns regarding psychiatric boarding, delayed transfers, and geographic inequities in access to inpatient behavioral health services. Consequently, accurate measurement of pediatric psychiatric infrastructure has become increasingly important for healthcare planning and policy development.
In North Carolina, the challenge of measuring pediatric inpatient psychiatric capacity is particularly important given recent policy changes affecting the regulation of inpatient psychiatric services. Historically, psychiatric inpatient facilities and expansions were subject to Certificate of Need (CON) oversight through the North Carolina Division of Health Service Regulation (DHSR) [16]. Under the CON process, facilities seeking to establish or expand psychiatric services were required to submit detailed documentation regarding projected need, proposed bed complements, service lines, and operational plans [14, 17, 18, 19]. These records provided a valuable and publicly accessible source of facility-level data regarding inpatient psychiatric capacity.
However, recent legislative reforms significantly altered this regulatory structure. Session Law 2023-7 removed psychiatric inpatient services from Certificate of Need oversight in North Carolina, fundamentally changing how future psychiatric capacity expansions are documented and monitored [16]. Although this policy shift was intended to reduce regulatory barriers and increase flexibility in behavioral health service expansion, it also reduced one of the state’s most standardized mechanisms for documenting inpatient psychiatric capacity.
At the same time, pediatric inpatient psychiatric services in North Carolina are delivered through a fragmented network of freestanding psychiatric hospitals, hospital- affiliated psychiatric facilities, and general acute care hospitals with embedded behavioral health units [6, 20, 21]. Freestanding psychiatric hospitals are more consistently represented in publicly accessible regulatory datasets, while hospital-based pediatric psychiatric units are frequently identified only through health system webpages, service descriptions, or secondary reports. In many cases, hospitals publicly acknowledge the presence of pediatric psychiatric services without reporting the number of available beds or operational capacity.
This inconsistency creates substantial challenges for healthcare planners, policymakers, researchers, and communities attempting to assess statewide behavioral health infrastructure [10, 20, 22]. Without standardized reporting requirements or publicly accessible facility-level data, it becomes difficult to determine whether pediatric psychiatric capacity is adequate, where geographic gaps exist, or whether recent policy reforms are improving access to care. The inability to accurately measure pediatric psychiatric capacity has important implications for healthcare access and accountability [7, 8, 23, 24]. Existing literature has linked pediatric psychiatric bed shortages to prolonged emergency department boarding, delayed psychiatric transfers, increased travel burden for families, and inequities in access to care [4, 24, 25, 26, 27, 28, 29, 30, 31]. Yet the absence of consistent reporting systems means that capacity limitations may themselves be underestimated.
The purpose of this study is to examine the intersection of data transparency, Certificate of Need reform, and pediatric inpatient psychiatric capacity in North Carolina. Using a facility-level dataset constructed from publicly available regulatory and health system sources [6], this study evaluates the extent to which current public reporting systems are capable of characterizing statewide pediatric inpatient psychiatric infrastructure and discusses the policy implications of fragmented capacity reporting.
Conceptual Framework
This study is grounded in a health services policy and infrastructure framework examining how regulatory oversight structures influence the availability, transparency, and standardization of publicly accessible behavioral health infrastructure data and, subsequently, the ability to evaluate pediatric psychiatric capacity and geographic equity in access to care. The conceptual framework underlying this study posits that regulatory structures influence the availability and standardization of publicly accessible behavioral health infrastructure data, which in turn affects the ability to measure inpatient psychiatric capacity, conduct effective health system planning, and evaluate equity in access to care. Under this framework, regulatory processes such as Certificate of Need requirements influence the availability and standardization of publicly accessible infrastructure data [13, 14, 17]. Changes in these reporting systems may subsequently affect the ability of policymakers and healthcare organizations to measure unmet need, identify geographic disparities, and evaluate access to pediatric psychiatric services.
Materials and Methods
Study Design
This study employed a cross-sectional health policy and infrastructure analysis designed to evaluate the extent to which pediatric inpatient psychiatric capacity in North Carolina can be identified, quantified, and geographically characterized through existing public reporting systems. Unlike traditional facility-level capacity studies focused primarily on estimating psychiatric bed supply, this analysis examined the visibility, completeness, and consistency of publicly accessible behavioral health infrastructure reporting across regulatory, organizational, and secondary reporting pathways. The study was designed to assess how existing public reporting systems support, or are limited in their ability to support, the evaluation of statewide pediatric psychiatric capacity, particularly following the removal of psychiatric inpatient services from Certificate of Need (CON) oversight in North Carolina.
Regulatory and Reporting Environment
Historically, inpatient psychiatric facility development and expansion in North Carolina were subject to Certificate of Need (CON) review through the North Carolina Division of Health Service Regulation (DHSR) [18, 32]. Under the CON process, facilities seeking to establish or expand psychiatric inpatient services were required to submit formal findings and approval documentation specifying proposed bed complements, populations served, operational characteristics, and projected community need. These materials functioned not only as regulatory documents but also as standardized public reporting mechanisms for behavioral health infrastructure.
Recent policy changes significantly altered this reporting environment. Session Law 2023-7 removed psychiatric inpatient services from CON oversight, reducing the use of standardized CON findings for future psychiatric infrastructure projects [16]. This policy change created uncertainty regarding the long-term availability of publicly accessible psychiatric capacity data and provided the policy context for the present analysis. The current reporting environment for pediatric inpatient psychiatric services in North Carolina consists of multiple fragmented pathways, including regulatory licensing systems, health system operational reporting, public-facing hospital webpages, and secondary public announcements [33]. These systems vary substantially in structure, transparency, and level of detail regarding pediatric psychiatric infrastructure.
Public Reporting Systems Evaluated
The analysis evaluated multiple publicly accessible reporting systems to determine the extent to which pediatric inpatient psychiatric infrastructure could be identified and measured.
Regulatory and Administrative Reporting Systems
Regulatory reporting systems included North Carolina DHSR Mental Health Hospital licensing rosters, Certificate of Need findings and approval documents, and State Medical Facilities Plan documentation. These systems were evaluated for: facility identification, explicit pediatric psychiatric bed complements, operational status, licensure conditions, and geographic distribution. Regulatory sources were considered the highest-confidence reporting pathway because they provided formal, standardized documentation of inpatient psychiatric infrastructure.
Organizational and Secondary Reporting Systems
Organizational reporting systems included official health system websites, hospital behavioral health service pages, facility profile pages, and operational service descriptions. These systems were evaluated to determine whether hospitals publicly acknowledged pediatric inpatient psychiatric services and whether quantitative capacity measures, including pediatric bed counts, were publicly reported. Secondary reporting sources included press releases, public announcements, media reports, and facility expansion notices. These sources were evaluated primarily for evidence of planned facilities, service expansion, or acknowledgment of pediatric psychiatric services when higher-level reporting pathways were incomplete or unavailable.
Infrastructure Visibility Classification
The primary analytic objective of the study was to evaluate the extent to which pediatric inpatient psychiatric infrastructure could be identified, quantified, and geographically characterized through existing public reporting systems. To accomplish this objective, each identified facility was assigned an infrastructure visibility classification based on the availability of publicly reported pediatric psychiatric capacity information.
Facilities were classified into one of three categories. Fully measurable infrastructure referred to facilities for which publicly accessible sources explicitly reported pediatric inpatient psychiatric bed counts. These facilities could be quantitatively incorporated into statewide capacity assessments because pediatric psychiatric capacity was directly documented through regulatory records, organizational reporting systems, or other authoritative public sources.
Partially measurable infrastructure referred to facilities that publicly acknowledged the existence of pediatric inpatient psychiatric services but did not provide quantitative pediatric bed counts. Although the presence of services could be verified, available reporting systems did not permit direct measurement of pediatric psychiatric capacity.
Non-measurable infrastructure referred to facilities for which available public reporting systems were insufficient to determine whether pediatric inpatient psychiatric services were present or to characterize the nature of those services. These facilities could not be incorporated into quantitative capacity analyses due to the absence of verifiable infrastructure information.
This classification framework was developed to assess infrastructure visibility rather than operational performance. The objective was not to evaluate actual service utilization, staffed bed availability, or real-time capacity, but rather to determine the extent to which existing public reporting systems support measurement of pediatric inpatient psychiatric infrastructure. Facilities lacking publicly reported pediatric bed counts were retained in the analysis because incomplete reporting was considered a substantive feature of the reporting environment rather than a source of random missing data. The inability to publicly identify or quantify pediatric psychiatric infrastructure was therefore treated as a policy-relevant finding.
Comparative Reporting Analysis
Comparative analyses were conducted to evaluate differences in reporting visibility across facility types and reporting pathways. Facilities were stratified by the following classifications: freestanding psychiatric hospitals, hospital- affiliated psychiatric facilities, hospital-based psychiatric units embedded within general acute care hospitals; and integrated health system psychiatric services. The analysis specifically examined whether certain facility types were more likely to have publicly measurable pediatric psychiatric capacity than others. Differences in visibility across reporting pathways were also evaluated. Regulatory sources, organizational reporting systems, and secondary public sources were compared based on level of detail, availability of pediatric bed counts, consistency of reporting, and ability to support statewide infrastructure measurement. The study utilized a previously constructed facility-level dataset of pediatric inpatient psychiatric services in North Carolina. The dataset was derived from publicly accessible regulatory and organizational reporting systems and included facilities identified as providing pediatric inpatient psychiatric services. Facility-level variables included facility name, county, facility type, pediatric inpatient psychiatric bed counts when publicly available, operational status, source type, verification status, and notes on ambiguity or data limitations. Only explicitly reported pediatric psychiatric bed counts were retained as quantitative measures. No estimation or extrapolation of missing bed counts was performed. Facilities with publicly acknowledged pediatric psychiatric services but without reported bed counts were retained in the analysis to evaluate reporting incompleteness and infrastructure visibility gaps.
Policy Analysis Framework
The policy analysis examined the relationship between regulatory oversight structures, public reporting mechanisms, infrastructure visibility, and statewide capacity measurement. The analysis was guided by a conceptual framework proposing that regulatory structures influence the availability and standardization of publicly accessible behavioral health infrastructure data, which subsequently affects the ability to measure psychiatric capacity, conduct statewide planning, and evaluate equity in access to pediatric psychiatric services. Particular attention was given to the role of CON documentation as a de facto infrastructure reporting mechanism and the implications of removing psychiatric inpatient services from standardized regulatory reporting pathways.
Analysis
Analyses were descriptive and focused on evaluating the extent to which pediatric inpatient psychiatric infrastructure could be publicly identified, quantified, and geographically characterized through existing reporting systems in North Carolina. Specific attention was given to the proportion of facilities with publicly measurable pediatric psychiatric bed counts, differences in infrastructure visibility across facility types, and the relative contribution of regulatory versus non-regulatory reporting pathways to statewide capacity measurement. The analysis also examined how fragmented reporting environments may influence geographic interpretation of pediatric psychiatric infrastructure and considered the potential implications of Certificate of Need reform for future transparency and infrastructure visibility [34, 35]. Importantly, the study emphasized statewide infrastructure measurability and reporting completeness rather than operational, staffed, or real-time bed availability. In this context, incomplete or inconsistent reporting was treated as a substantive feature of the reporting environment rather than solely as a methodological limitation.
State-operated psychiatric hospitals were excluded from the primary analysis because these facilities function primarily as high-acuity, referral-based, and forensic behavioral health institutions rather than general-access pediatric psychiatric service providers [15, 36]. The study focused specifically on publicly measurable pediatric psychiatric infrastructure accessible through standard healthcare delivery pathways, including freestanding psychiatric hospitals and hospital- based pediatric psychiatric services. Exclusion of state- operated facilities also reduced potential distortion in evaluating infrastructure visibility and public reporting consistency across facility types.
Quality Assurance and Reproducibility
Several procedures were implemented to improve consistency and reproducibility of the analysis. Public reporting systems were evaluated using standardized criteria, and facilities with ambiguous reporting underwent structured cross-source review. Source attribution was maintained for all facility-level observations, including regulatory documents, organizational reporting sources, and secondary public materials. The study prioritized transparency and reproducibility over completeness. Pediatric psychiatric capacity was recorded only when explicitly supported by public evidence. No undocumented assumptions were used to estimate missing bed counts or infer operational capacity.
Ethical Considerations
This study used publicly available facility-level and organizational reporting data and did not involve human subjects, patient-level information, or protected health information. Institutional review board review was therefore not required.
Results
Objective 1: Infrastructure Visibility and Reporting Completeness
A total of 16 facilities and health system entities were identified as providing or planning pediatric inpatient psychiatric services in North Carolina. Among these, 12 facilities had publicly verifiable pediatric psychiatric bed counts, while 4 facilities publicly acknowledged pediatric psychiatric services without reporting quantitative bed capacity information as outlined in Figure 1 below. Reporting completeness varied substantially across facility types, with freestanding psychiatric hospitals demonstrating considerably greater infrastructure visibility than hospital- based psychiatric units.
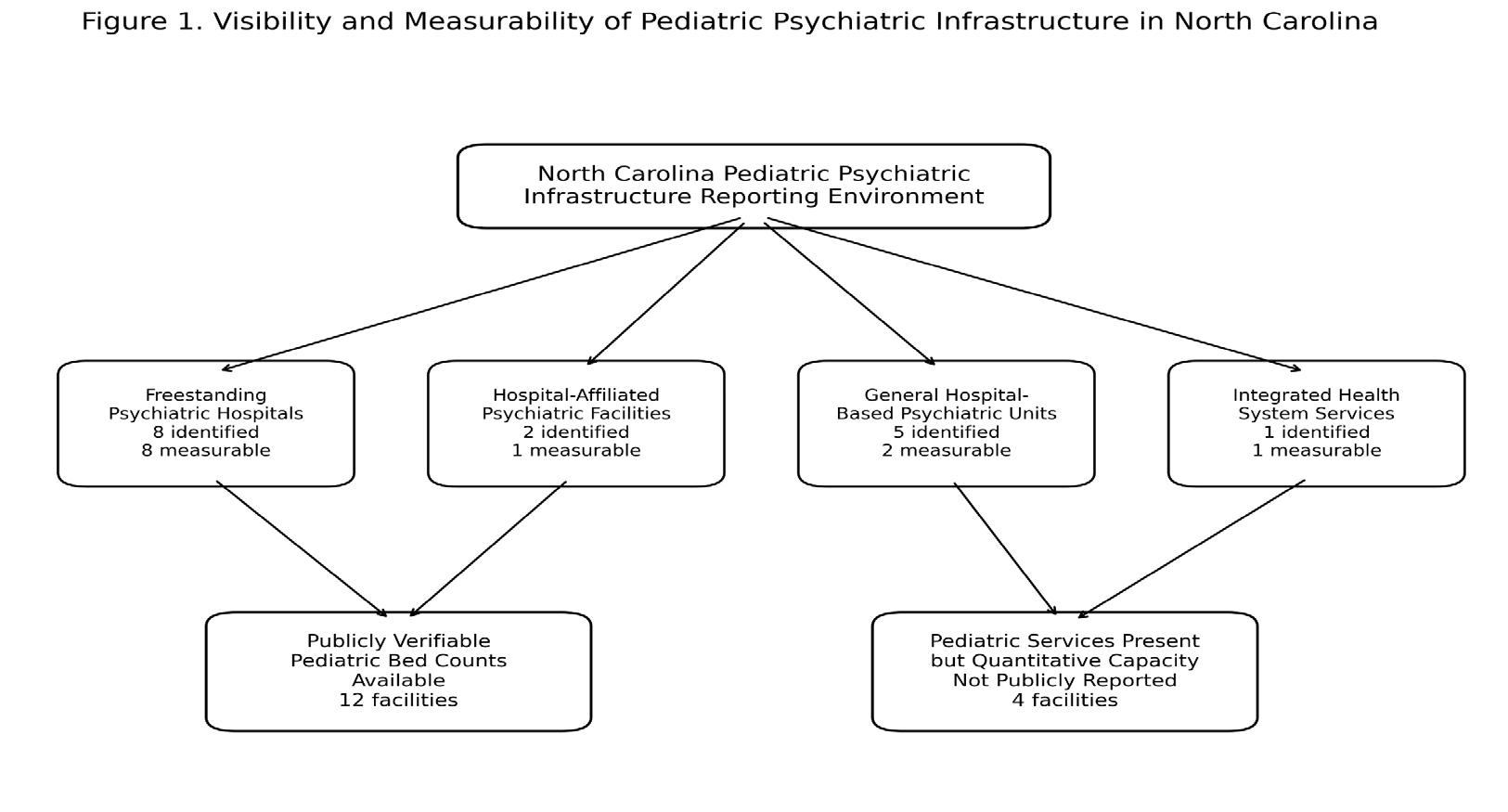
Among identified facilities, only a subset publicly reported pediatric inpatient psychiatric bed counts in a manner sufficient to support quantitative statewide capacity measurement. Eight freestanding psychiatric hospitals were identified, although one lacked publicly verifiable pediatric psychiatric bed counts. In contrast, several hospital-based pediatric psychiatric programs publicly acknowledged inpatient pediatric psychiatric services without reporting pediatric bed counts. These included major academic and integrated health system facilities that confirmed pediatric psychiatric services but did not provide quantitative capacity information through publicly accessible sources. As a result, statewide pediatric psychiatric capacity could not be fully quantified using existing public reporting systems. Facilities lacking publicly reported pediatric bed counts were retained in the analysis as examples of partially measurable infrastructure rather than excluded as missing observations. Table 1 summarizes infrastructure visibility and reporting completeness by facility type.
| Facilities Identified | Public Pediatric Bed Count Available | Missing Bed Counts | Reporting Visibility | |
|---|---|---|---|---|
| Freestanding Psychiatric Hospitals | 8 | 7 | 1 | High |
| Hospital-Affiliated Psychiatric Facilities | 2 | 2 | 0 | Moderate–High |
| General Hospital-Based Psychiatric Units | 5 | 2 | 3 | Low |
| Integrated Health System Psychiatric Services | 1 | 1 | 0 | Moderate |
| Total | 16 | 12 | 4 | Fragmented |
Table 1: Infrastructure Visibility and Reporting Completeness by Facility Type.
Objective 2: Visibility Differences Across Facility Types
Substantial differences in infrastructure visibility were observed across facility types. Freestanding psychiatric hospitals were consistently represented in publicly accessible regulatory reporting systems, particularly through DHSR licensing records and historical Certificate of Need findings. In contrast, hospital-based pediatric psychiatric services were considerably less visible within standardized public reporting pathways. Most publicly measurable pediatric psychiatric bed counts originated from freestanding psychiatric hospitals subject to historical CON documentation requirements. Hospital-based psychiatric units were more likely to be identified through organizational webpages or service-line descriptions, which frequently acknowledged pediatric psychiatric services without specifying operational bed complements.
This asymmetry in reporting created a two-tiered infrastructure visibility environment in which freestanding psychiatric facilities were substantially more measurable than embedded pediatric psychiatric services operating within larger health systems. Table 2 presents the primary reporting pathways used to identify pediatric psychiatric infrastructure.
| Typical Information Available | Strengths | Major Limitations | |
|---|---|---|---|
| DHSR Licensing Rosters | Facility identification, license status | Standardized statewide reporting | No pediatric bed complements |
| CON Findings and Approval Documents | Pediatric bed counts, facility scope, licensure conditions | High transparency and specificity | Limited applicability following CON removal |
| Hospital/Health System Websites | Service availability, operational descriptions | Identifies hospital-based services | Bed counts inconsistently reported |
| Press Releases / Media Reports | Planned expansions, public announcements | Useful for emerging facilities | Non-standardized and incomplete |
Table 2: Reporting Pathways and Infrastructure Visibility.
Objective 3: Dependence on Certificate of Need Documentation
The majority of publicly measurable pediatric psychiatric bed complements identified in this study were derived from historical Certificate of Need findings [18, 33] and approval documents. These documents frequently provided explicit pediatric psychiatric bed counts, operational conditions, service-line descriptions, and facility-level infrastructure details that were not consistently available through other reporting systems. In contrast, facilities developed or expanded outside standardized CON pathways frequently lacked equivalent publicly accessible quantitative capacity documentation. As a result, the removal of psychiatric inpatient services from CON oversight may reduce the future availability of standardized infrastructure reporting mechanisms for pediatric psychiatric services in North Carolina.
This finding suggests that CON documentation historically functioned not only as a regulatory approval mechanism but also as an important source of publicly accessible behavioral health infrastructure data. Table 3 summarizes the implications of Certificate of Need removal for infrastructure visibility.
| Historical CON Environment | Post-CON Environment | |
|---|---|---|
| Standardized pediatric bed reporting | Common | Inconsistent |
| Public facility-level findings | Routinely available | Reduced availability |
| Operational detail transparency | High | Variable |
| Visibility of hospital-based psychiatric units | Limited but partially recoverable through findings | Increasingly fragmented |
| Ability to conduct statewide infrastructure measurement | More feasible | More difficult |
Table 3: Implications of Certificate of Need Removal for Infrastructure Visibility.
Objective 4: Geographic Implications of Fragmented Reporting
Fragmentation in reporting systems had important geographic implications for statewide pediatric psychiatric infrastructure assessment. Counties containing freestanding psychiatric hospitals generally had publicly measurable pediatric psychiatric capacity due to the availability of regulatory documentation. However, counties served primarily through hospital-based psychiatric units frequently lacked measurable capacity despite public acknowledgment of pediatric psychiatric services. As a result, geographic analyses relying exclusively on publicly reported pediatric psychiatric bed counts may underestimate the presence of pediatric psychiatric infrastructure in some regions while simultaneously obscuring the true magnitude of statewide capacity gaps. The inability to consistently quantify hospital- based pediatric psychiatric services complicates efforts to identify underserved regions, evaluate geographic equity, and conduct statewide behavioral health planning.
Discussion
Infrastructure Visibility and Reporting Completeness
This study demonstrates that pediatric inpatient psychiatric infrastructure in North Carolina is only partially measurable through existing public reporting systems. Although multiple facilities publicly acknowledge pediatric inpatient psychiatric services, the availability of quantitative capacity information varies substantially across facility types and reporting pathways. Freestanding psychiatric hospitals were consistently represented within regulatory reporting systems and were more likely to have publicly verifiable pediatric psychiatric bed counts [6]. In contrast, hospital- based pediatric psychiatric units embedded within general acute care hospitals were substantially less visible within standardized public reporting environments.
A major finding of this analysis is that the ability to measure pediatric psychiatric capacity in North Carolina depends heavily on historical Certificate of Need (CON) documentation and related regulatory reporting systems. Many of the pediatric psychiatric bed counts identifiable through public sources originated from CON findings and approval documents rather than from ongoing operational reporting systems maintained by hospitals or health systems. This finding is in alignment with existing literature and suggests that while reporting mechanisms exist for inpatient adult psychiatric bed availability [37], current public reporting systems do not consistently provide sufficient information to support comprehensive statewide pediatric psychiatric infrastructure assessment [6, 15]. The analysis also demonstrated that infrastructure visibility itself varies systematically by facility structure. Freestanding psychiatric hospitals were generally measurable through DHSR licensing and CON documentation, while hospital-based pediatric psychiatric units frequently acknowledged pediatric psychiatric services without reporting quantitative capacity information. This asymmetry in reporting creates an uneven infrastructure visibility environment that complicates statewide planning and behavioral health system evaluation.
A central implication of this study is that data transparency should itself be understood as a component of healthcare infrastructure [38, 39, 40]. Health system planning, workforce development, resource allocation, and geographic access evaluation all depend upon the existence of reliable, standardized, and publicly accessible infrastructure data [41, 42]. When healthcare infrastructure cannot be consistently identified or quantified, policymakers and healthcare organizations face substantial limitations in their ability to assess unmet need or evaluate whether system expansion efforts are improving access. In the context of pediatric psychiatric services, fragmented reporting environments create uncertainty regarding both the true magnitude and geographic distribution of inpatient capacity. This uncertainty may contribute to underestimation of access gaps, particularly in regions where pediatric psychiatric services exist operationally but remain poorly represented within public reporting systems. As a result, incomplete infrastructure visibility may itself contribute to inequities in behavioral health planning and access evaluation.
Importantly, the findings of this study suggest that missing capacity data should not necessarily be interpreted as random data absence. Rather, fragmented reporting appears to be structurally associated with specific facility types and organizational arrangements. Hospital-based psychiatric services embedded within larger health systems may be operationally active while remaining effectively invisible within statewide infrastructure measurement efforts [37].
Visibility Differences Across Facility Types
One of the most significant findings of this study is the extent to which hospital-based pediatric psychiatric services remain only partially measurable within current public reporting systems. Several large academic medical centers and integrated health systems publicly acknowledged pediatric psychiatric services while failing to report quantitative pediatric bed capacity information. This creates what may be conceptualized as “invisible infrastructure,” in which behavioral health services may exist operationally but cannot be consistently quantified within statewide planning analyses. As a result, statewide capacity assessments may simultaneously underestimate existing infrastructure while also obscuring the true magnitude of unmet need. This issue may have important downstream operational consequences.
Recent pediatric psychiatric boarding literature demonstrates that emergency departments and inpatient medical units increasingly function as de facto psychiatric care environments despite lacking dedicated psychiatric staffing and behavioral health infrastructure [30, 43, 44, 45]. Incomplete visibility of hospital-based psychiatric infrastructure may therefore obscure both existing system strain and unmet pediatric psychiatric capacity needs. The absence of standardized pediatric psychiatric capacity reporting may also limit the ability of healthcare systems and policymakers to monitor psychiatric boarding, transfer delays, and regional access inequities documented throughout the pediatric psychiatric access literature [15, 27, 28].
The visibility imbalance between freestanding psychiatric hospitals and embedded hospital-based psychiatric units is particularly important because many pediatric psychiatric services are increasingly integrated within larger health systems. If standardized reporting systems do not evolve to account for these organizational structures, future infrastructure measurement may become increasingly fragmented. This issue has practical implications for families, policymakers, healthcare administrators, and researchers. Publicly accessible infrastructure information influences referral pathways, planning decisions, grant allocation, regional coordination efforts, and public understanding of available behavioral health resources. Incomplete visibility may therefore contribute not only to measurement limitations but also to barriers in navigating care systems.
Certificate of Need Documentation and Infrastructure Measurement
Although Certificate of Need programs are traditionally evaluated primarily through the lens of healthcare regulation and market oversight [13, 32, 46], the findings of this study suggest that CON processes also functioned as de facto infrastructure reporting mechanisms for behavioral health services in North Carolina.
Historical CON findings and approval documents frequently provided detailed facility-level information regarding:
- pediatric psychiatric bed complements;
- populations served;
- operational conditions;
- service-line scope; and
- projected community need.
These materials created a relatively standardized public documentation pathway for psychiatric infrastructure that extended beyond the licensing process itself. As demonstrated in this analysis, many of the pediatric psychiatric bed counts currently measurable through public sources remain identifiable largely because they were historically documented through CON proceedings. The removal of psychiatric inpatient services from CON oversight may therefore have implications extending beyond regulatory flexibility alone. While removal of CON requirements may reduce barriers to psychiatric facility expansion [13, 47], it may simultaneously reduce the availability of standardized infrastructure reporting and public visibility regarding pediatric psychiatric capacity. Without replacement reporting mechanisms, future psychiatric infrastructure expansion may become increasingly difficult to monitor using publicly accessible data systems. This distinction is important because the findings of this study should not be interpreted as an argument for or against Certificate of Need regulation itself. Rather, the analysis highlights the role that standardized regulatory documentation previously played in supporting infrastructure transparency and statewide capacity measurement.
Geographic Equity and Planning Implications
Fragmented infrastructure visibility also has important implications for geographic equity in behavioral health access. Counties with freestanding psychiatric hospitals were substantially more likely to have measurable pediatric psychiatric capacity because these facilities were historically represented within standardized regulatory reporting pathways. In contrast, regions dependent upon hospital-based psychiatric units may appear to have limited pediatric psychiatric infrastructure even when services exist operationally. As a result, geographic analyses based solely on publicly measurable capacity may incompletely represent statewide pediatric psychiatric infrastructure. This limitation complicates efforts to identify underserved regions, allocate behavioral health resources, evaluate referral networks, and conduct population-level planning analyses. The inability to consistently characterize pediatric psychiatric infrastructure is particularly concerning given existing evidence of prolonged emergency department boarding, interfacility transfer delays, and geographic disparities in behavioral health access for children and adolescents. Without comprehensive reporting systems, it becomes difficult to determine whether statewide infrastructure expansion efforts are effectively addressing these access challenges. To illustrate the relationship between regulatory oversight, infrastructure visibility, and statewide capacity measurement, Figure 2 presents a conceptual comparison of the historical Certificate of Need reporting environment and the fragmented reporting landscape that has emerged following the removal of psychiatric inpatient services from CON oversight.
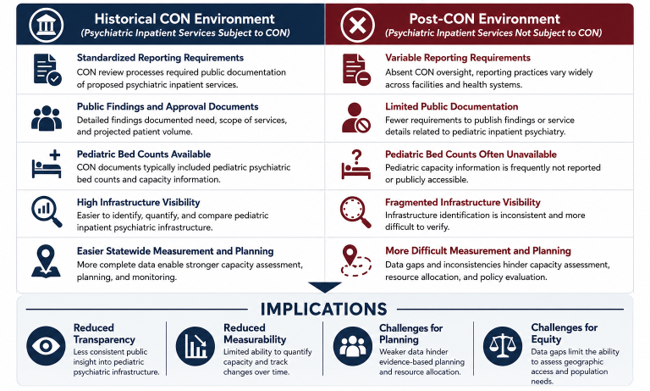
Figure 2: Conceptual Impact of Certificate of Need (CON) Reform on Infrastructure Visibility and Capacity Measurement. Note: The figure illustrates the proposed relationship between regulatory reporting mechanisms and the ability to measure pediatric inpatient psychiatric infrastructure. Historically, Certificate of Need (CON) processes generated standardized public documentation regarding psychiatric capacity. Removal of psychiatric inpatient services from CON oversight may reduce infrastructure visibility and complicate statewide capacity assessment.
Policy Implications
The findings of this study suggest several policy implications related to pediatric psychiatric infrastructure reporting and behavioral health system planning. The fragmented reporting environment identified in North Carolina may reflect broader national limitations in pediatric psychiatric infrastructure measurement. Existing national hospital reporting systems frequently lack standardized pediatric psychiatric capacity indicators, limiting the ability of researchers and policymakers to evaluate pediatric psychiatric access consistently across states and health systems. As a result, pediatric psychiatric infrastructure may remain systematically under characterized within national behavioral health planning efforts despite growing concern regarding psychiatric boarding, access strain, and workforce shortages. North Carolina may benefit from development of a standardized statewide pediatric psychiatric infrastructure reporting system. Such a system could include:
- facility-level pediatric psychiatric bed counts;
- operational status;
- populations served;
- age ranges;
- service specialization; and
- geographic coverage.
Standardized reporting requirements for hospital-based psychiatric units may be necessary to improve infrastructure visibility. Existing reporting systems disproportionately capture freestanding psychiatric hospitals while underrepresenting embedded hospital-based services. In addition, annual statewide pediatric psychiatric infrastructure reporting could support more effective behavioral health planning and facilitate identification of geographic gaps in access. Standardized public reporting could also improve transparency regarding system expansion following the removal of psychiatric inpatient services from CON oversight. In summary, future behavioral health policy discussions should consider the relationship between regulatory structures and infrastructure measurability. As healthcare delivery systems become increasingly integrated and decentralized, maintaining reliable infrastructure reporting systems may become increasingly important for ensuring equitable access to pediatric psychiatric services.
Future Research
Future research should evaluate how post-CON psychiatric infrastructure expansion is documented over time and whether reporting fragmentation increases following removal of standardized regulatory reporting pathways. Additional analyses examining operational versus licensed capacity, psychiatric workforce availability, and real-time bed accessibility may further improve understanding of pediatric behavioral health infrastructure limitations. Qualitative research involving hospital administrators, behavioral health leaders, and policymakers may also help clarify how reporting practices influence planning, resource allocation, and behavioral health system coordination. Longitudinal analyses examining infrastructure visibility before and after CON reform may provide additional insight into the policy implications of evolving reporting systems.
Limitations
This study has several limitations. First, the analysis relied exclusively on publicly available data sources and therefore may not capture all operational pediatric psychiatric services. Second, the study evaluated infrastructure visibility rather than real-time operational capacity or staffed bed availability. Third, public reporting practices may change over time, particularly following the removal of psychiatric inpatient services from CON oversight. Finally, because the study focused on reporting systems and publicly measurable infrastructure, some hospital-based psychiatric services may remain incompletely represented despite active operation.
Conclusions
This study demonstrates that pediatric inpatient psychiatric infrastructure in North Carolina cannot be comprehensively characterized using existing public reporting systems. Infrastructure visibility varies systematically across facility types, with freestanding psychiatric hospitals substantially more measurable than hospital-based pediatric psychiatric units embedded within larger health systems. The findings suggest that historical Certificate of Need processes functioned not only as regulatory mechanisms but also as important infrastructure reporting pathways for pediatric psychiatric services. The removal of psychiatric inpatient services from CON oversight may therefore reduce future standardization and transparency of pediatric psychiatric infrastructure reporting unless alternative reporting systems are developed. Ultimately, the inability to consistently measure pediatric psychiatric capacity represents a healthcare infrastructure and policy problem in itself. Improved transparency and standardized reporting mechanisms may be necessary to support evidence-based behavioral health planning, geographic equity evaluation, and accountability in pediatric psychiatric service delivery.
References
-
CDC (2026) YRBS Data Summary & Trends Report. Centers for Disease Control and Prevention, USA.
-
Close J, Arshad SH, Soffer SL, Lewis J, Benton TD (2024) Adolescent Health in the Post-Pandemic Era: Evolving Stressors, Interventions, and Prevention Strategies amid Rising Depression and Suicidality. Pediatr Clin North Am 71(4): 583-600.
-
Overhage L, Hailu R, Busch AB, Mehrotra A, Michelson KA, et al. (2023) Trends in Acute Care Use for Mental Health Conditions Among Youth During the COVID-19 Pandemic. JAMA Psychiatry 80(9): 924-932.
-
Hoffmann JA, Foster AA, Gable CJ, Carlin KE, Pergjika A, et al. (2025) Pediatric Mental Health Boarding in US Emergency Departments, 2018–2022. J Am Coll Emerg Physicians Open 6(4): 100180.
-
OSBM MN (2026) North Carolina Urban/Rural Classifications.
-
Parks A, Workman K, Lazari M (2026) Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina. J Qual Health Care Econ 9(2): 1-11.
-
Ghose SS, Beehler S, Pinals DA, Crocker L, Hoey T, et al. (2025) Youth Inpatient and Residential Treatment Psychiatric Beds: National Trends and Potential Causal Factors, 2010–2022. Psychiatr Serv 76(4): 343-349.
-
Geller JL, Biebel K (2006) The Premature Demise of Public Child and Adolescent Inpatient Psychiatric Beds. Psychiatr Q 77(3): 251-271.
-
Krugman SD, Rauch D (2022) An Unexpected Shortage: Hospital Beds for Children. Health Aff Forefront.
-
McBain RK, Cantor JH, Eberhart NK (2022) Estimating Psychiatric Bed Shortages in the US. JAMA Psychiatry 79(4): 279-280.
-
McBain RK, Cantor JH, Eberhart NK, Huilgol SS, Estrada- Darley I (2022) Adult Psychiatric Bed Capacity, Need, and Shortage Estimates in California—2021. Rand Health Q 9(4): 16.
-
M La E, Lich KH, Wells R, Ellis AR, Swartz MS (2016) Increasing Access to State Psychiatric Hospital Beds: Exploring Supply-Side Solutions. Psychiatr Serv 67(5): 523-528.
-
Hellinger FJ (2009) The Effect of Certificate-of-Need Laws on Hospital Beds and Healthcare Expenditures: An Empirical Analysis. Am J Manag Care 15(10): 737-744.
-
Yuce TK, Chung JW, Barnard C, Bilimoria KY (2020) Association of State Certificate of Need Regulation With Procedural Volume, Market Share, and Outcomes Among Medicare Beneficiaries. JAMA 324(20): 2058-2068.
-
Cushing AM, Nash KA, Foster AA, Zima BT, West AE, et al. (2024) Pediatric Inpatient Psychiatric Capacity in the US, 2017 to 2020. JAMA Pediatr 178(10): 1080-1082.
-
Bill H (2023) General Assembly of North Carolina Session 2023.
-
John Locke Foundation (2026) Certificate of Need in North Carolina.
-
NC DHSR HPCON (2026) Overview of Certificate of Need.
-
Ho V (2020) Revisiting States’ Experience With Certificate of Need. JAMA 324(20): 2033-2035.
-
Brathwaite D, Emergency Department-Based Psychiatric Services for Children and Adolescents: An In-Depth Investigation of Care in North Carolina. ProQuest.
-
From Idea to Paradigm: The Integrated Primary and Mental Health Care Model in North Carolina.
-
Lanier P, Rose R, Gibbs D, Hyman J, Kamdar N, et al. (2024) Psychiatric Residential Treatment Facilities for Child Behavioral Health Services in North Carolina Medicaid. N C Med J 85(3): 215-221.
-
Salinsky E, Loftis C (2007) Shrinking Inpatient Psychiatric Capacity: Cause for Celebration or Concern? National Health Policy Forum.
-
Thompson A, Simmons S, Wolff J (2021) Nowhere to Go: Providing Quality Services for Children With Extended Hospitalizations on Acute Inpatient Psychiatric Units. J Am Acad Child Adolesc Psychiatry 60(3): 329-331.
-
Afzal S, Gunnison C, Rudofker A, Esposito J, Geddings W (2025) Stabilizing Pediatric Patients During Psychiatric Boarding: A Quality Improvement Project. Pediatrics 155(2): e2023063262.
-
McCarty EJ, Nagarajan MK, Halloran SR, Brady RE, House SA, et al. (2022) Healthcare Quality During Pediatric Mental Health Boarding: A Qualitative Analysis. J Hosp Med 17(10): 783-792.
-
Wharff EA, Ginnis KB, Ross AM, Blood EA (2011) Predictors of Psychiatric Boarding in the Pediatric Emergency Department: Implications for Emergency Care. Pediatr Emerg Care 27(6): 483-489.
-
Overhage LN, Lê Cook B, Rosenthal MB, McDowell A, Benson NM (2024) Disparities in Psychiatric Emergency Department Boarding of Children and Adolescents. JAMA Pediatr 178(9): 923-931.
-
O’Neil AM, Sadosty AT, Pasupathy KS, Russi C, Lohse CM, et al. (2016) Hours and Miles: Patient and Health System Implications of Transfer for Psychiatric Bed Capacity. West J Emerg Med 17(6): 783-790.
-
Wolff JC, Davis S, Liu RT, Cha CB, Cheek SM, et al. (2018) Trajectories of Suicidal Ideation among Adolescents Following Psychiatric Hospitalization. J Abnorm Child Psychol 46(2): 355-363.
-
McEnany FB, Ojugbele O, Doherty JR, McLaren JL, Leyenaar JK (2020) Pediatric Mental Health Boarding. Pediatrics 146(4): e20201174.
-
Ghosh S, Roy Choudhury A, Plemmons A (2020) Certificate-of-Need Laws and Healthcare Utilization During COVID-19 Pandemic. SSRN.
-
North Carolina Department of Health and Human Services, Division of Health Service Regulation (2026) Certificate of Need (CON) Decisions and Findings.
-
Zuiderwijk A, Janssen M (2014) Open Data Policies, Their Implementation and Impact: A Framework for Comparison. Gov Inf Q 31(1): 17-29.
-
Tinajero J (2017) The Need to Repeal Certificate of Need Laws to Improve America’s Health Care System: A Dormant Commerce Clause Analysis. J Leg Med 37(3-4): 597-612.
-
Cushing AM, Liberman DB, Pham PK, Michelson KA, Festekjian A, et al. (2023) Mental Health Revisits at US Pediatric Emergency Departments. JAMA Pediatr 177(2): 168-176.
-
Liu MX, McGinty EE, Schpero WL (2025) Regional Changes in Inpatient Psychiatric Bed Capacity and Availability of Alternative Psychiatric Services, 2012- 2022. Health Aff Sch 3(11): qxaf204.
-
Kadakia KT, DeSalvo KB (2023) Transforming Public Health Data Systems to Advance the Population’s Health. Milbank Q 101(Suppl 1): 674-699.
-
Sorter M, Stark LJ, Glausar T, McClure J, Pestian J, et al. (2023) Addressing the Pediatric Mental Health Crisis: Moving from a Reactive to a Proactive System of Care. J Pediatr: 113479.
-
DuBose BM, Fry-Bowers EK (2021) Achieving Access Parity for Inpatient Psychiatric Care Requires Repealing the Medicaid Institutions for Mental Disease Exclusion Rule. Policy Polit Nurs Pract 22(1): 63-72.
-
National Governors Association (2026) State Health Workforce Toolkit.
-
Nutley T, Reynolds HW (2013) Improving the Use of Health Data for Health System Strengthening. Glob Health Action 6.
-
Penwill NY, Wong CT, Taylor DB, Freyleue SD, Bordogna AL, et al. (2023) Hospitalists’ Perceptions of Pediatric Mental Health Boarding: Quality of Care and Moral Distress. Hosp Pediatr 13(3): 233-245.
-
Worsley D, Bowden C, Keating C, Cassidy K, Doupnik SK (2024) Impact of Mental Health Boarding on Clinicians at a Children’s Hospital: A Qualitative Analysis. J Hosp Med 19(3): 193-199.
-
Dalton EM, Krass P, Bouchelle Z, Fillmore A, Katz T, et al. (2023) Characteristics, Disposition, and Outcomes of Children Hospitalized for Mental Health Boarding at a Children’s Hospital. J Hosp Med 18(12): 1113-1117.
-
Sigaud L (2025) Certificate-of-Need Laws and Access to Health Care Services. SSRN.
-
Mitchell MD (2025) Certificate-of-Need Laws in Healthcare: A Comprehensive Review of the Literature. South Econ J 92(1): 6-43.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines