Response to the Covid-19 Pandemic: Looking Back and Looking Forward from the Perspective of Local Health Departments in Nebraska
Context: The scale and complexity of the COVID-19 pandemic response has revealed some significant successes and limitations of our public health system.Objective: Focused on the pandemic response from the viewpoint of local health departments (LHDs) in Nebraska, this study aimed to identify successes, barriers, lessons learned, and changes needed to improve the local response for future pandemics.Methods: A mixed-methods approach was used to gather information from LHDs in Nebraska. In June 2021, a survey was sent to all LHD directors (n=19), and 17 (89%) participated in the survey. To supplement the survey results, four LHD directors from different areas of the state were interviewed.Results: Successful efforts of the pandemic response included developing stronger partnerships with K-12 schools, distributing the COVID-19 vaccines, and expanding the number of people reached through contact tracing. Barriers included a shortage of staff with the competencies and expertise to respond to a crisis, the lack of funding prior to the pandemic, inconsistent guidance, the politicization of the COVID-19 response, resistance to masking, and misinformation about COVID-19.Conclusions: This pandemic taught many lessons, including the importance of timely and frequent communication with all partners and the public, the need to share accurate data broadly and frequently as possible, the lack of knowledge of public health’s authority to implement emergency public health measures (e.g., quarantine and isolation), and the persistence of staff burnout and retention. Looking forward, baseline funding for LHDs should be expanded to strengthen capacity to hire additional staff, particularly in the areas of epidemiology and communications. Additional investments in common information technology platforms are also essential. Finally, more creative staff resilience solutions are needed to address staff burnout. While essential for LHDs during times of pandemic, such investments can also benefit LHDs when pandemics don’t rage.
Introduction
The scale and complexity of the COVID-19 pandemic has posed the greatest public health emergency response in over 100 years. Limited resources related to the inadequate number of public health and medical professionals and supplies have forced public officials at the national, state, and local levels to prioritize resource allocation and push the boundaries of our existing resource capabilities [1]. The COVID-19 pandemic also revealed the limitations of our nation’s public health system when it is forced to respond to a major public health emergency. Many of these limitations such as a shortage of public health workers and outdated communication and electronic data collection strategies stem from sharp cutbacks in funding over the past 15 years [2, 3, 4].
In a recent report, the Bipartisan Policy Center concluded that federal, state, and local public health agencies “have lacked the workforce and modern data systems to support surveillance, contact tracing, testing, guidance on mitigation measures, administration of vaccines, and clear communication that is needed to stop the spread of infectious diseases …”[5]. De Salvo KB, et al. [6] and others argue that although health departments have been the foundation to the nation’s response to the COVID-19 pandemic, they have experienced numerous challenges such as underfunding, workforce shortages, outdated information technology, and the politicization and mistrust of the guidance provided by public health leaders.
Background and Purpose of the Study
Although the LHDs in urban areas were created many years ago, most rural counties in Nebraska lacked public health services. In 2001, however, the state legislature used Tobacco Settlement funds to develop and finance 16 multicounty LHDs which now cover all the 93 counties in the state. Based on the NACCHO classification system, a total of 5 LHDs would be classified as small (i.e., less than 50,000 people), 13 would be considered medium (i.e., 50,000 to 499,999 people), and 1 would be categorized as large (i.e., over 500,000 people). The majority of the LHD directors have been in their position for more than 5 years. Prior to the COVID-19 pandemic, every LHD had an emergency response coordinator and most of them had experience in responding to various types of public health emergencies. The governance structure of LHDs in Nebraska is considered decentralized which means that the local board of health has the authority to make decisions about how to improve the health of people in their jurisdiction. However, the Executive branch of state government has the authority to implement directed public health measures for infectious disease outbreaks. In November 2020, the College of Public Health at the University of Nebraska Medical Center awarded five internal grants to faculty and staff to explore various aspects of the COVID-19 pandemic. This grant project is focused mainly on the COVID-19 response from the viewpoint of local health departments (LHDs) in Nebraska. More specifically, this project aims to examine the factors that have contributed to a successful response by the local public health system and the barriers and challenges that limited the response. It will also identify the lessons learned and the changes that are needed to improve the local response in future pandemics.
Methods
A mixed-methods approach was used to collect the data and information from LHDs. A survey was initially developed by faculty in the College of Public Health based on a review of the literature and then sent to the staff at the Nebraska Association of Local Health Directors (NALHD) for their review and comment. In June of 2021, the survey was sent via email using Survey Monkey to the directors of each of the 19 LHDs in Nebraska. The surveys were returned by the end of June and consisted of 8 questions covering the following topics:
- The most successful response areas,
- The most significant barriers limiting response efforts,
- The most important changes to improve response efforts,
- The public’s perception and support,
- New partnerships formed,
- The lessons learned, and
- Transformational opportunities. The data were analyzed based on the percentage of survey participants (n=21) who agreed with a specific statement (e.g., the most significant barrier limiting the LHD’s response was the shortage of qualified staff.).
To supplement the results of the survey, four LHD directors were interviewed in July of 2021 for 35 to 60 minutes via Zoom. The interviewees were from LHDs in different parts of the state and included three rural and one urban LHD. There were 11 interview questions, including the most successful response areas, the most significant barriers, the general level of understanding of the LHD’s authority to authorize and enforce directed health measures, the level of support from the board of health, receptiveness of community to masks and social distancing, effectiveness of the guidance and support from state government, and the changes needed to improve the LHD response in future pandemics. The interviews were recorded and transcribed so that common themes could be identified.
Results
A total of 17 or 89 percent of the LHDs participated in the survey, and the total number of people responding was
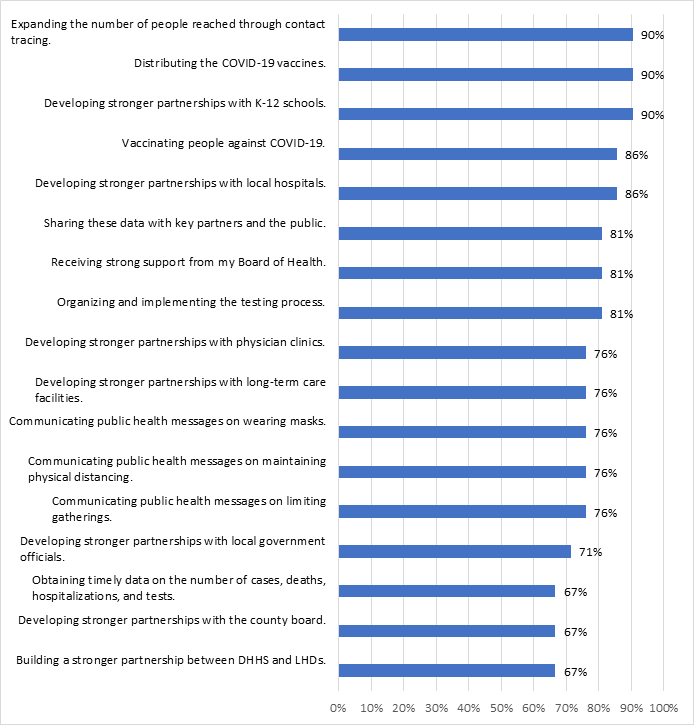
21. The results revealed that many factors contributed to the success of the COVID-19 response by LHDs. Figure 1 shows that the survey participants believed that the most successful efforts in responding to the COVID-19 pandemic involved the following efforts:
- Developing stronger partnerships with K-12 schools (90 percent)
- Distributing the COVID-19 vaccines (90 percent)
- Expanding the number of people reached through contact tracing (90 percent)
Over 80 percent of the respondents indicated that other successful efforts included developing stronger partnerships with local hospitals (86 percent), vaccinating people against COVID-19 (86 percent), organizing and implementing the testing process (81 percent), receiving strong support from my Board of Health (81 percent), and sharing data with key partners and the public (81 percent). In contrast, LHDs noted less success building a stronger partnership between the Nebraska Department of Health and Human Services (State Health Department) and LHDs (67 percent), developing stronger partnerships with the local city county board of commissioners (67 percent), and obtaining timely data on the number of cases, deaths, hospitalizations, and tests (67 percent).
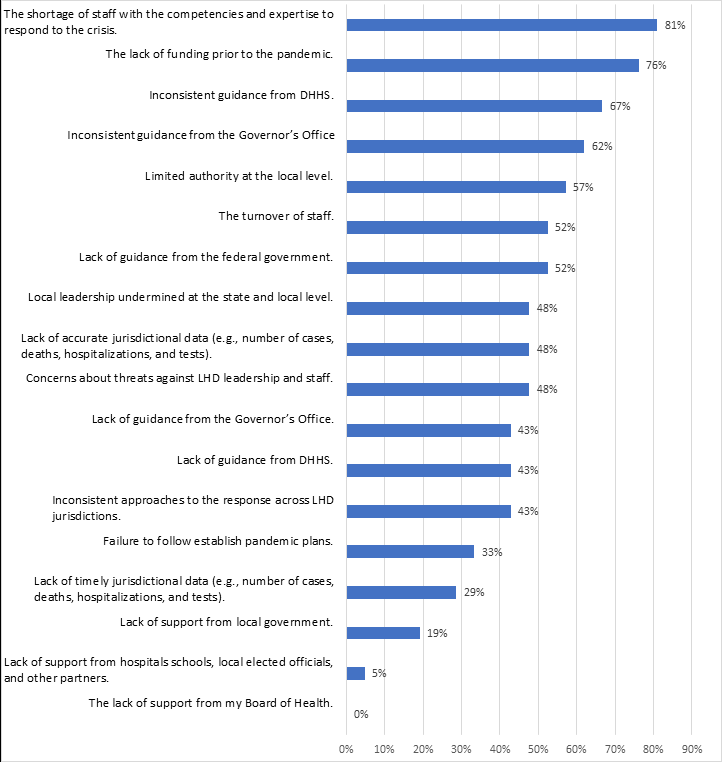
The second question asked the survey respondents to identify significant partnership and capacity barriers that limited the LHDs’ COVID-19 response. Figure 2 indicates the existence of several significant barriers, including:
- A shortage of staff with the competencies and expertise to respond to the crisis (81 percent)
- The lack of funding prior to the pandemic (76 percent)
- Inconsistent guidance from Nebraska DHHS (67 percent)
- Inconsistent guidance from the Governor’s office (62 percent)
- Limited authority at the local level (57 percent)
- The turnover of staff (52 percent)
- Lack of guidance from the federal government (52 percent)
- Concerns about threats against LHD leadership and staff (48 percent)
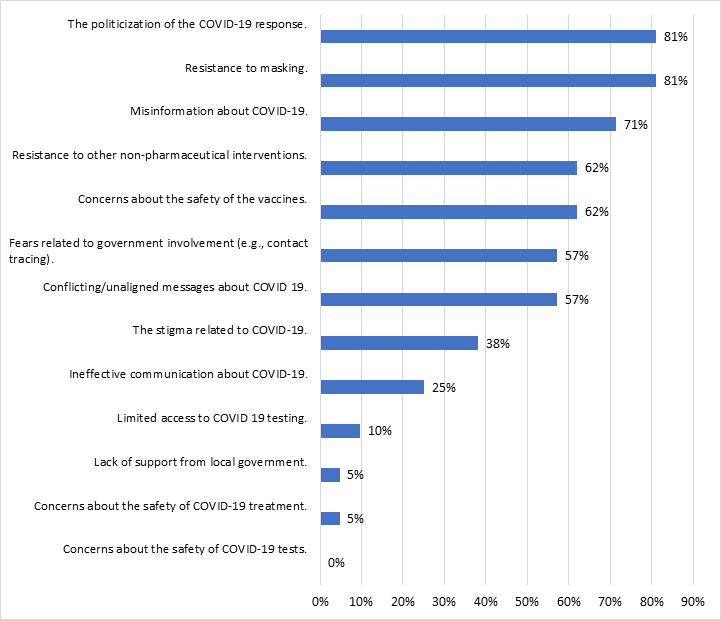
The third question asked about the barriers within the community that posed a challenge to LHDs in responding to the COVID-19 pandemic. As shown in Figure 3, the most significant barriers were:
- The politicization of the COVID-19 response (81 percent)
- Resistance to masking (81 percent)
- Misinformation about COVID-19 (71 percent)
- Resistance to other non-pharmaceutical interventions (62 percent)
- Concerns about the safety of the vaccines (62 percent) The least identified factors were concerns about the safety of the COVID-19 tests and treatment and lack of support from local government.
When respondents were asked whether they thought the public’s perception of and support for local public health has improved or worsened due to COVID-19, 76 percent indicated that it had improved. Another 14 percent believed there was no change and only 10 percent felt that it had worsened.
Lessons Learned
There were many lessons learned from the COVID-19 pandemic that can be applied to future public health emergencies. Some of the major lessons learned were:
- Timely and effective communication between the state and LHDs and between LHDs and key partners is critical. At times, inconsistent messages between the state and LHDs caused confusion among the partners and the public. During the interviews, LHDs stressed the importance of communicating frequently (e.g., multiple times per week) with their partners (e.g., school officials, hospitals, physicians, long-term care facilities, and local government officials) and some held almost daily briefings that were often attended by the local media.
- Both the key partners and the public rely on the LHDs to provide up-to-date and relevant information and data on the number of cases, hospitalizations, deaths, and vaccination status. Without these data, many partners cannot make good policy decisions. For example, most school officials want to understand the trends at the county level so they can make better decisions on masks for children and in-school learning.
- During a pandemic, LHDs must be nimble and creative. One LHD began using community health workers to work with racial and ethnic minority populations and other underserved populations. Another LHD began using mobile clinics to provide vaccinations to hard-to- reach groups.
- An effective response to the COVID-19 pandemic requires good coordination and collaboration between state and LHDs. It was suggested that agency representatives get together to discuss a common vision, determine clear roles and responsibilities (e.g., what activities and decisions should be made at the local level vs the state level), and develop performance criteria to assess agency performance.
- Local data and information are essential in making decisions related to PPE and testing prioritization, exemptions, social distancing requirements, reopening businesses (e.g., restaurants), and mask requirements. However, inconsistent data dashboards and risk dials led to confusion and mixed messages across the state.
- Most policymakers and the public did not understand the directed public health measures and evidence-based practices (e.g., quarantine, isolation, contact tracing) prior to the pandemic. As a result, LHDs were forced to spend considerable time on educational activities and defending these evidence-based practices.
- The stress and duration of the pandemic led to staff burnout and retention issues.
Recommended Changes
Survey participants were asked about the changes that are needed to improve the LHD response to COVID-19 and future pandemics. Most recommendations were focused on communication strategies, building stronger data and surveillance systems, and continuing to develop and strengthen partnerships.
- There was a strong consensus that the public health system in Nebraska was not ready to respond to a major pandemic. As a result, it is critical to assess the current gaps in the system and build a stronger public health infrastructure that will be better prepared to respond to future pandemics. At a minimum, LHDs need a higher level of baseline funding that is adequate to develop their epidemiology and communications capacity. Flexible reserve funds are also needed to allow LHDs to add new employees quickly. For example, contact tracing is more effective at the local level, but the capacity is often inadequate during major surges. In addition, more funds should be invested in data sharing platforms between state and LHDs.
- State and LHD representatives should work together to design a data dashboard and risk dials that are consistent across all LHDs. Decisions should be made on metrics, dashboards and risk dials, and system design.
- The state’s vaccine registry has several major limitations so it is imperative to convene a group of key stakeholders, including representatives from LHDs, hospitals, physician clinics, pharmacies, and others to develop recommendations that would lead to improvements in the functioning of the registry.
- During some stages of the pandemic, the messages between LHDs were inconsistent between LHDs. To overcome this problem, a Joint Information Center (JIC) that would have the capability of creating template messages that could be tailored by LHDs and customized to local audiences should be established. These messages should be culturally appropriate that have the capability of reaching various target populations, including rural and non-English speaking populations.
- An outside entity should be used to assist LHDs in developing and implementing resilience strategies (e.g., flexible work schedules and behavioral health programs) to address staff burnout Figure 4.
Discussion
This study examined the COVID-19 response from the perspective of LHD directors in Nebraska. Most directors felt their overall response was very positive, particularly in view of the inadequate staffing, limited analytic data capabilities and outdated information technology, and inconsistent messaging between federal, state, and local public health officials. Based on their perceptions, the most successful activities were building strong partnerships (e.g., K-12 schools and local hospitals), distributing and vaccinating people, contact tracing efforts, and sharing data (e.g., number of cases, tests, hospitalizations, and deaths). Many of these successes have also been identified by studies. For example, Hawkins and colleagues have noted that public health officials across the U.S. have regularly communicated with the public about the state of the pandemic, communicated evolving measures to bring it under control, planned and implemented an efficient and fair vaccine distribution system, and hired and trained many new contact tracer workers [7].
Although many barriers and challenges were identified, including a shortage of staff with the competencies and expertise to respond to the crisis, inconsistent guidance from the state health agency, the Governor’s Office, and the federal government, limited authority at the local level, and turnover of staff, many of these barriers existed in other states. Other barriers such as the politicization of the COVID-19 response, resistance of masking, misinformation about COVID-19, and concerns about the safety of the vaccines were also issues found in other states. De Salvo KB, et al. [6] believe that many of the infrastructure challenges stem from persistent and widening resource gaps prior to the pandemic. The COVID-19 pandemic exposed and further exacerbated the inadequate funding, workforce shortages, outdated data systems, and politicization and mistrust of public health leaders and guidance. Juliano C, et al. [8] and others have discussed the impact of the extremely polarized political response about personal liberty, among a small but very vocal minority of Americans concerned about government intrusion in their personal liberties. She notes, “Not wearing a face covering has become a statement about personal liberty, despite potentially infecting others” [8].
One of the key challenges revealed by the pandemic was the inability to share data between the state and LHDs because of ineffective information technology platforms. In addition, these platforms are usually not compatible with hospital EMR data (e.g., admissions, transfers, discharges). Castrucci B, et al. [9] has referred to public health data systems as neglected, archaic, and siloed with limited accuracy. To make more accurate and timely decisions about reopening’s and mask protocols, a “data superhighway” for public health is essential [6]. In Nebraska, this challenge is exacerbated by the state’s narrow interpretation of HIPAA law’s application to local public health data, an interpretation that has significantly limited most rural LHDs’ ability to share local data about the number of COVID-19 cases, hospitalizations, and deaths. The state has interpreted the HIPAA privacy law to mean that no data can be shared in counties that have a population of less than 20,000 people. However, most states suppress information in jurisdictions with fewer than five cases or deaths [10].
From a workforce capability perspective, many rural LHDs lack the necessary knowledge and expertise in epidemiology and data analytics. Those LHDs with these capabilities were overwhelmed by the demand for their expertise during the pandemic. While it is unlikely that every LHD in Nebraska will be able to hire an epidemiologist, LHDs already are accustomed to sharing technical public health capacity across local jurisdictions. It may be possible to add local epidemiological capacity across the state by taking advantage of LHDs’ partnerships with each other and with experts at institutions such as the College of Public Health. Having up-to-date data platforms and the ability to analyze the data would assure a greater likelihood of identifying new trends more quickly and would lead to more consistent reporting across the state.
Finally, both the findings from the interviews and surveys revealed that significant differences in interpretations related to local public health authority led to communication gaps between LHDs, DHHS, and the Governor’s Office. At times, it also resulted in confusing and inconsistent messages to the public. A pandemic response requires leaders to consider not only the epidemiological science, but also the broad factors that influence health. Answers to questions such as: (1) Can we mitigate the disease spread? (2) Can we mitigate the impact on families’ incomes? and (3) Can we mitigate the impact on students’ school success? Need to be carefully considered. In many cases, LHDs were not meaningfully included in decision-making processes related to state guidance even though they were expected to implement the policies and practices that impacted the lives of individuals and families in their jurisdiction. While state and local entities do not always agree on every issue, a clear process should be in place to ensure that all appropriate experts are included in both critical decisions and related communication about this and future pandemic responses.
Although many organizations have already prepared after-action reports that have identified the strengths and weaknesses of the response to the COVID-19 pandemic, these evaluations while extremely useful tend to be narrower in scope. Given the broad and far-reaching impact of the pandemic across both public and private sectors of the state, it is critical to organize some type of public forum such as a legislative interim study to identify some of the major successes, the overarching barriers and challenges, the lessons learned, and recommendations to improve the response in future pandemics. Potential topics for discussion should include the flow of data and information between public health, health care providers, and others; communication issues between the state and LHDs; the possible expansion of directed health measures at the local level; the effectiveness of the current vaccine registry; the potential impact on health equity; and the funding levels for public health. In this forum, input is needed from a broad array of organizations and sectors, including LHDs, NALHD, DHHS, hospitals, physician clinics, pharmacies, schools, the COPH, and the Governor’s Office [11].
Limitations
Although this study was the first to focus on the response to the COVID-19 pandemic from the perspective of LHDs in Nebraska, it does have some limitations. First, although nearly all LHDs participated in the survey, the information relied on perceptions which may be subject to recall biases. Second, the survey was conducted in early June so the information will not reflect the most recent surge in the COVID-19 pandemic. Third, the interview data were collected from only four LHDs and may not reflect the views of all LHDs. Finally, this project is a case study of Nebraska from a LHD perspective, and it may not be generalizable to other states.
Implications for Policy & Practice
From the viewpoint of LHDs in Nebraska, there were many positive aspects to the COVID-19 response, but several barriers and challenges were also identified. Many of the challenges are directly related to the infrastructure gaps (e.g., workforce shortages, cutbacks in funding, and obsolete data platforms) that existed prior to the pandemic.
- While some of these resource gaps will require sustained funding over an extended period, there are some short-term problems that need immediate attention. These short-term issues include an infusion of staff to conduct contact tracing and vaccine distribution, an investment in epidemiologists and data analysts as well as new, mutually agreed-upon, information technology platforms so that data can be shared more easily between state and LHDs, and the creation of a locally governed Joint Information Center, so that LHDs can communicate consistent messages to key partners and the public throughout the state.
- Finally, although public health staff has been incredibly resilient throughout the pandemic, creative programs and strategies should be developed more systematically to address staff burnout.
Declarations
• Funding: This project was funded by an internal University of Nebraska Medical Center College of Public Health grant.
• Conflicts of Interest: The authors have no conflicts of interest.
References
-
(2021) COVID-19 pandemic after action report. National Homeland Security Center.
-
(2021) The impact of chronic underfunding on America’s public health system: trends, risks, and recommendations. Trust for America’s Health.
-
Mckillop M, Lieerman DA (2021) The impact of chronic underfunding on America’s public health system: trends, risks, and recommendations. Trust for America’s Health, pp: 1-48.
-
(2020) NACCHO’s 2019 Profile Study: Changes in Local Health Department Workforce and Finance Capacity Since 2008. Research brief, National Association of County and City Health Officials, pp: 1-5.
-
Daschle T, Frist B, Wilensky G, Burke S, Capretta J, et al. (2021) Positioning America’s public health system for the next pandemic. Bipartisan Policy Center, pp: 66.
-
DeSalvo KB, Wang YC, Harris A, Auerbach J, Koo D, et al. (2017) Public Health 3.0: A Call to action for Public Health to Meet the Challenges of the 21st Century. Prev Chronic Dis 14: E78.
-
Hawkins R, Ruebush E, Plescia M (2021) Public health strengths during the COVID-19 response. J Public Health Manag Pract 27(3): 329-331.
-
Juliano C, Castrucci B, Fraser M (2021) COVID-19 and public health: looking back, moving forward. J Public Health Manag Pract 27: S1-S4.
-
Castrucci B, Juliano C, Inglesby T (2021) Four steps to building the public health system needed to cope with the next pandemic. J Public Health Manag Pract 27: S98-S100.
-
Haasan A, Jones LW (2021) Nebraska restores its covid data dashboard after taking it down over the summer. The New York Times.
-
(2020) New data on state health agencies shows shrinking workforce and decreased funding leading up to the COVID-19 pandemic. Association of State and Territorial Health Officials.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines