Establishment of Public Health Management Cadre in India and Guidelines for Implementation – 2022
National Health Policy (NHP) 2017 (Para 11.8) proposed that a multi/interdisciplinary health workforce is necessary for managing programs under National Health Mission. National Health Policy 2017 considered creating Public Health Management Cadre (PHMC) in all States. In the 13th CONFERENCE of CENTRAL COUNCIL OF'HEALTH & FAMILY WELFARE (CCHFW), 2019 under the chairpersonship of Hon’ble central Health Minister of India the decision evolved to establish PHMC in all States by year 2022 . The key objective of establishment of PHMC is best utilization of expertise and talent for ensuring health for all. Another objective is to segregate clinical and public health functions among cadres with flexibilities as per requirement of the state. Four types of structures and frameworks are developed, and the states are given flexibility to modify the structures according to the local situation and context. Medical and Health professionals would form a major part, but professionals from other backgrounds like sociology, economics, anthropology, hospital management, communications, etc., who have undergone public health management training/course would also be considered. States could decide to locate public health managers (medical/non-medical) into same or different cadre streams belonging to Directorates of Health. In states like Bihar where there is lack of Directorates of Health the situation is very worse indicated by NITI Aayog annual Health Index reports. In such states the researcher found that public health management untrained persons are posted on key public health management posts while the public health trained doctors (sponsored by Government revenue) are not posted for public health management. The specialists are not involved in PHM and it may be due to the fact that there is shortage of specialist at country and state levels. The public health cadre is a misnomer if they will also work for clinical treatments then the key goal of PHMC will be affected particularly in states like Bihar. This is the first ever decision at national level for establishing PHMC and the details of pay structure , transparency etc. are not available and although the objectives are quite clear; the PHMC cadre may be affected in states like Bihar where it seems that lack of Directorate and unscrupulous management have grabbed the health system.
Introduction
Background/Rationale
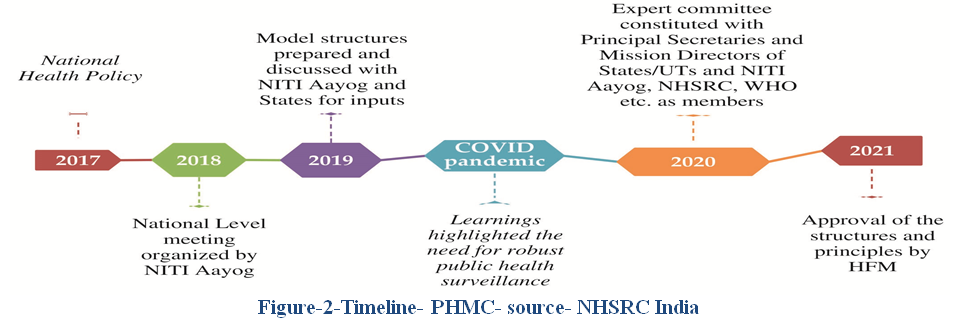
National Health Policy (NHP) 2017 (Para 11.8) proposed that a multi/interdisciplinary health workforce is necessary for managing programs under National Health Mission [1]. National Health Policy 2017 considered creating Public Health Management Cadre (PHMC) in all States. In the 13th CONFERENCE of CENTRAL COUNCIL OF’HEALTH & FAMILY WELFARE (CCHFW), 2019 under the chairpersonship of Hon’ble central Health Minister of India the decision evolved to establish PHMC in all States by year 2022 [2]. MoHFW (Ministry of Health and Family Welfare) has formed an expert committee (F.No. - NHSRC/PHA/18-19/Public Health Cadre/07 Government of India Ministry of Health and Family Welfare (National Health Mission) Nirman Bhawan, New Delhi Dated the 17th July 2020) on PHMC in 2020 under chairpersonship of JS (joint secretary) (Policy) and Dr. Rajani Ved, ED-NHSRC- Co-chair, the secretariat of this committee is PHA (Public Health Administration) division [3]. The PHA (Public Health Administration) division has developed a guidance for all states about principles, career pathways and organograms (organization graph) for PHM cadre, in collaboration with NITI Aayog, PHM experts, selected states (with interest in establishing a public health management cadre), WHO, PHFI, etc. States where some structure of public health cadre already existed like Tamil Nadu, Odisha, Maharashtra, West Bengal, Chhattisgarh, etc., are found to be performing better in NITI Aayog annual health index ranking compared to states like Bihar where there are irregularities in PHMC continue to be ranking lowest in NITI Aayog annual health index ranking [4]. The states like Bihar are providing Post Graduate Diploma in Public Health Management Course to healthcare workers at IIPH, Delhi since 2009-10 as evident from Data Base and also directs candidates that after successful completion of course/training they have to work in the faculty of public health management for 05 years for which SHS (state health society) is making a bond agreement but selection for training and posting after successful completion of training are suffering from irregularities/scam etc [5]. During ongoing SARS-CoV-2 pandemic, the delivery of essential healthcare services was disrupted in India [6]. Why PHMC is Needed The challenges and barriers of the current public health system, institutional set-ups need an integrated co-ordinated intersectional approach to rectify public health issues of emerging diseases, pandemics, disasters, injuries, illnesses, social and environmental issues [7]. PHMC is also required to increase the capacity and capability of health system for estimating disease burden, need assessment and framing plans for preventive, promotive, curative, rehabilitative and palliative services [8]. Public health surveillance for early detection and responding to various outbreaks is also required.
Objectives
The key objective of establishment of PHMC is best utilization of expertise and talent of people from different sector for ensuring health for all. Another important objective is to segregate clinical and public health functions among cadres with flexibilities as per requirement of the state.
Design
Four types of structures and frameworks are suggested by the center, and the states have flexibility to modify the structures according to the local situation, need and context. Medical and Health professionals would form a major part, but professionals from other backgrounds like sociology, economics, anthropology, hospital management, communications, etc., who have undergone public health management training/course would also be considered. States could decide to locate public health managers (medical/non-medical) into same or different cadre streams belonging to Directorates of Health. In states like Bihar where there is lack of Directorates of Health the situation is very worse indicated by NITI Aayog annual Health Index reports. In such states the researcher found that untrained persons are posted on key public health management posts while the public health trained doctors fully sponsored by government revenue are not posted for public health management. This may be related to corruption/scam etc. as shouted by media in such states and vigilance department reports [9]. PHMC is also needed to encourage specialized skills like entomology, housekeeping, bio-medical waste management, biomedical engineering, communication skills, management of call centres, and ambulance services. Example-The national green tribunal (NGT) had recently found that a lot of public health facilities have violated covid-19 bio-medical waste management rules and health department Bihar (more than 15000 health facilities are running without authorization/ licence from pollution control board) was on the top, which have been imposed with a fine of rupee 1, 00, 00,000 / month for damaging environment. The fine for spreading covid-19 to humans by improper covid-19 generated waste management, which may have infected several lakh and killed several thousand people, is still pending [10, 11]. Posting untrained personals for management can be so dangerous for life of people and environment is clearly indicated by above example. There may be ignorance/ posting scam/corruption with intention for unscrupulous
Setting / Framework of PHMC
loot of government funds behind such acts of negligence which is a matter of investigation by the government.
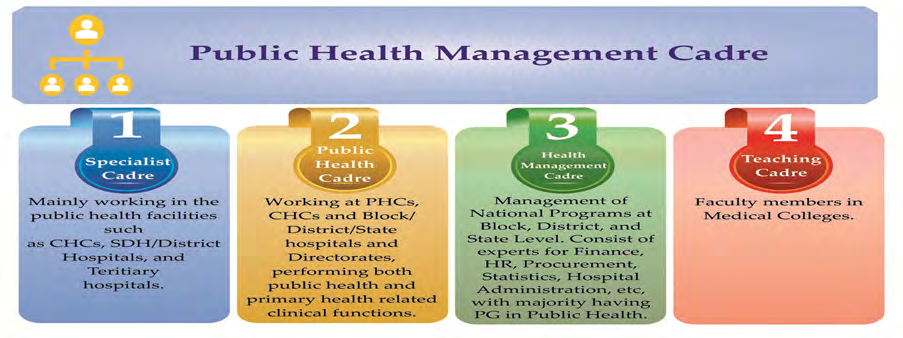
The PHMC structures at state, district and block level will be guided by the following principles: see figure-1 Essential core cadre of PHMC- principles:
- Specialists: clinical specialists with PG degree/ diploma/ MD/MS in streams like Medicine, Surgery, Orthopaedics, Eye, ENT, Obs/Gyn, Dermatology, Psychiatry, etc [8].
- Public Health Cadre: public health professionals with MBBS degree having MD (PSM) or PG (Public Health) Degree/ Masters/ Diploma. All new MBBS doctors will be required to acquire public health qualification within certain time (3-5 years) if not already achieved [8].
- Health Management Cadre: health and other professionals PG qualification in Public Health (70%) and MBA (HR), MBA (Procurement/ Supply Chain), MBA (Finance), MBA (Operations), MBA (Hospital/ Health Management) or with a relevant qualification, etc., (30%). States will have the flexibility to change the percentage as per the local context and requirement [8].
- Teaching cadre will be as per the NMC guidelines, as revised from time to time [8].
- The career progression for each cadre will be distinctive in their own respective streams with flexibility for inter- cadre deputation wherever necessary, if criteria for qualification are met. Existing GDMOs in Public Health Cadre with certain years (3-5 years) of seniority will be required to do a one/two/three year master’s course in public health for advancement in Public Health Cadre [8]. In states like Bihar having low ranking continuously in NITI Aayog annual SHI report it seems that the MBBS doctors are not given preference as well as there is lack of transparency in training selection process and postings after successful completion of the PG course in public health management [5]. The researcher found that the selection seems too biased and the PG seats may be sold out to anyone for personal benefit/ corruption which are a matter of investigation by the centre/state. The state program officer posted in states like Bihar seems to be untrained and most of them may not perform data analysis, operate computer or laptop etc. as found by the researcher [5]. This possible corruption in posting and training etc. may be one of the reasons why such states are not improving in health sector.
- For new recruitment to Public Health Cadre, MBBS doctors with MD PSM/Community Medicine, PG degree/ diploma in Public Health can be given preference [8].
- Increments/special pay for acquired qualification should be encouraged for in-service doctors [8]. In states like Bihar there is wastage of government revenue on PHM training as the selection process is questionable as well as competency of candidates after training are also doubted [5]. The researcher have found that a candidate is present at the same time on government duty and also doing PGDPHM course from IIPH-Delhi and this seems to be some big scam of selling out diploma qualification. The researcher asked IIPH (PHFI) about this but they denied disclosing the facts. With such acts the future of public health will be limited to degree and diploma only and a big zero on real grounds. Even what kind of training such IIPH institutes are providing that candidates from Bihar after 13 years of training except a few are unable to do a simple research or analysis? It may be possible that with government funds candidates are going for enjoyment at Delhi and institute is passing all the candidates due to government pressure, which is a matter of investigation? How many research publications came from IIPH trained candidates of Bihar and what works they have done in the field of public health management is a matter of investigation to stop corruption and loot of government revenue in the name of public health management by such institutes having nexus with administration. This may be some big conspiracy to grab the government revenue coming from taxes levied upon the citizens of India.
- The head of the district/ block i.e., Chief/Block Medical Officer, shall be from a Public Health Cadre, however, if so desired by the state Specialist Cadre may also be considered for district level positions, and the ratio for which may be decided by the State. In states like Bihar it is found by the researcher that there is total violation of such rules by concerned authorities and this may be due to personal benefit/corruption etc, which is a matter of investigation [12]. Although there is pre-existing rule to make head from MBBS/MD/MS/DM/Mch cadre in Bihar but it is violated at most places which may be due to personal benefit/ corruption etc. and for these reasons Bihar continue to be on lower rankings since 2014.
• Specialists and super-specialists will join at a higher scale in Specialist Cadre, to attract them in government sectors. Specialists will work in public health facilities as per Indian Public Health Standards (IPHS) [8]. Figure 2 shows the timeline for developing PHMC.
Desirable principles
- Incentive schemes may be proposed for motivating the existing workforce to take up public health courses for their professional growth and continuing education [8]. In states like Bihar it seems that corruption have superseded motivation. In Bihar if a candidates applies for public health management work after successful completion of training the candidate is harassed badly and this may be due to getting unscrupulous profit in posting unsuitable / untrained candidates [5]? The state Health society does not provide public health management work after PGDPHM training and it seems to be wastage of government revenue and time of doctors. It seems some very big corruption is going on and to hide this untrained people are utilized in place of trained. [See Annexure-1]
- District Health Society shall serve as a platform of convergence between public health and clinical functions [8].
- The convergence of functions of public health cadre and specialist cadre at various levels needs to be established by the State [8].
- For all cadres, method of recruitment, number of posts at various health locations and career progression needs to be clearly defined. States will take initiatives in scaling up and expanding public health courses identify relevant institutions to support the states with qualified professionals. Various types of professionals which may support public health functions are also broadly defined in NHP 2017.
- Initiate urgent and time bound actions for creation of Public Health Cadre, Health Management Cadre, and Specialist Cadre [8].
Bias in PHMC
The specialists are not involved in PHM and it may be due to the fact that there is shortage of specialist at country and state levels. The public health cadre is a misnomer if they will also work for clinical treatments than the key goal of PHMC will be affected particularly in states like Bihar. Added to this the public health management is a very broad field and very high level of competency is required to control the explosion of public health problems in states and at country level. Already the public health management goal is shattered by unscrupulous selection and posting scams in states like Bihar. Without a dedicated public health cadre again the situation can be worsened in states like Bihar where it seems that there is complete violation of rules/regulations/ merit in postings and selection. The health management cadre selection should be made transparent. The teaching cadre must incorporate doctors from public health cadre to teach future doctors about PHM which is not available in current curriculum. Stepwise Implementation Plans
- Mapping of existing GDMOs and specialists in the present health cadre and their positions at various facilities [8].
- Making a structure both in Public Health and Specialist Cadre based on IPHS norms in existing facilities [8].
- Impart Public Health training to the in-service candidates [8].
- Recruitment of doctors as per the sanctioned positions [8].
- Making Health Management Cadre with public health professionals and other postgraduates such as MBA etc. [8]
- Action plan for cadre strength and fill up vacant posts preferably over next six months to one year. [8]
Limitations
This is the first ever decision at national level for establishing PHMC and the details of pay structure , transparency etc. are not available and although the objectives are quite clear; the PHMC cadre may be affected in states like Bihar where it seems that lack of Directorate and unscrupulous management have grabbed the health system.
Discussion
There is a shortage of medical practitioners and some scholars suggest that other graduates are placed in this field. I have a simple question that can an automobile engineer after getting MPH degree from such institutes which seems to sale out degree and diploma will be able to do this task [13]? Actually such scholars may be agents of some big NGO who are writing to attract policy makers to grab the funds for NGO. Moreover the whole labour and expenditures in becoming an automobile engineer will be shattered. Without a sound background of health field a person cannot do health management as the terminology of health field is quite complex. The future version will be more detailed.
Other Information
This is the first version of this work and more versions will evolve in future with more information and analysis of PHMC.
Declarations
- This version of paper has not been previously published in any peer reviewed journal and is not currently under consideration by any journal. The document is Microsoft word with English (India) language & 2501 words excluding reference and declaration etc. (3263words Total including all).
- Ethics approval and consent to participate: Not applicable. This study has not involved any human or animals in real or for experiments. The submitted work does not contain any identifiable patient/participant information.
- Consent for publication: The author provides consent for publication.
- Availability of Data and Materials: Electronic records from HMIS (health management information system) of MoHFW (ministry of health and family welfare), Government of India, NITI Aayog, NHSRC.
- Conflicts of Interest/ Competing Interest: There are no conflicts / competing of interest
- Funding-Self sponsored. No aid taken from individual or agency etc.
- Authors’ Contributions: The whole work is done by the Author - Dr Piyush Kumar, M.B.B.S., E.M.O.C., P.G.D.P.H.M., -Senior General Medical Officer- Bihar Health Services- Health Department- Government of Bihar, India and Advocate Anupama-Senior Lawyer, Bar Council, Patna.
- Acknowledgements: I am thankful to Advocate Anupama my wife and daughters Aathmika-Atheeva for cooperation.
- Author information: The author is currently working as Senior General Medical Officer for the government of Bihar and Advocate Anupama-Senior Lawyer, Bar Council, Patna.
- Financial Support & sponsorship: Nil
- Funding: The author declares that no funds are taken from any individual or agency-institution for this study.
References
-
(2017) National Health Policy. Ministry of health and family welfare government of India.
-
National Health Systems Resource Centre.
-
National Health Systems Resource Centre.
-
Kumar P, Anupama A (2022) Analysis of NITI AAYOG (National Institution for Transforming India) health index report on the ranking of states and union territories: A cross sectional observational research study Round 1 (2014-2016)-V1.
-
State Health Society Bihar.
-
Kumar P (2022) What is the impact of Covid-19 on the Antenatal Care Services Utilization in Public-Private- Rural-Urban Hospitals of India during the COVID-19 Pandemic Period of 2020-2021 compared to pre- pandemic era 2018-2019?. Modern Applied Medical Research 2(2): 1-10.
-
WHO (2020) Health Systems and Policy Analysis Policy Brief How to enhance the integration of primary care and public health? Approaches, facilitating factors and policy options. World Health Organization.
-
National Health Systems Resource Centre.
-
Vigilance Department Bihar.
-
Health Department, Government of Bihar.
-
National Green Tribunal
-
Health Department, Government of Bihar.
-
Kumar P (2021) Op-ed---- Public Health as I See It- India &lmics1.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines