A Study among the Vendors Near Selected Educational Institutes in Chandigarh, India on Awareness of Cigarette and Other Tobacco Product Act, 2003 (COTPA)
Introduction: Cigarettes are the only legal consumer products in the world that cause one-half of their long-term users to die prematurely. As this epidemic continues to take its toll in the United States, it is also increasing in low- and middle-income countries that are least able to afford the resulting health and economic consequences. Aim: To see the awareness of Cigarette and Other Tobacco Products Act (COTPA), 2003 in selected Educational Institution in Chandigarh. Methodology: Chandigarh was the area chosen to study the to see the awareness of Cigarettes and other Tobacco Products Act (COTPA), 2003 in Chandigarh. A Cross-sectional study was conducted from January 2018 to May 2018 to study the awareness of Cigarettes and other Tobacco Products Act (COTPA), 2003 in Chandigarh. A Self-structured questionnaire was used for collecting information on Cigarettes and other Tobacco Products Act, (COTPA) 2003. Results: Our study revealed that selling of Tobacco products to Minor then 56% respondents out of total accepted that there is selling of Tobacco products to Minor but 44% did not accept so. 40% respondents out of total accepted that there is selling of Tobacco products by Minor but 60% did not accept so. 53% respondents hold the opinion that the current level of enforcement of pictorial health warning on Tobacco products can motivate people to quit tobacco use. 47% respondents opined that the current level of enforcement of pictorial health warning on Tobacco products cannot motivate people to quit tobacco use and according to the result majority of respondents believed that current level of enforcement of pictorial health warning on Tobacco products can motivate people to quit tobacco use Conclusion: It can be concluded that majority of respondents (70%) are aware about the Cigarettes and other Tobacco products Act, 2003 as they know that there is law regarding prohibition of use of Cigarette and Tobacco product but 30% respondents were not aware about the COTPA Act, (2003).
Introduction
Tobacco use is a global epidemic that kills 5.4 million people annually, tragically, more than 80% of those deaths occurs in the developing world. Considering the enormity of the problem, member nations of the WHO negotiated and adopted the first public health treaty – the Framework Convention on Tobacco Control (FCTC) – in 2003. India was the eighth country to ratify the treaty that gives a vital opportunity to reduce the global burden of tobacco.
This is also a time in life of heightened sensitivity to normative influences: as tobacco use is less tolerated in public areas and there are fewer social or regular users of tobacco, use decreases among youth. And so, as we adults quit, we help protect our children [1]. It is past time to end this epidemic. To do so, primary prevention is required, for which our focus must be on youth and young adults. As noted in this report, we now have a set of proven tools and policies that can drastically lower youth initiation and use of tobacco products. Fully committing to using these tools and executing these policies consistently and aggressively is the most straight forward and effective to making future generations tobacco-free [2].
However, in India, the high prevalence of tobacco consumption remains one of the major challenges to the health and wellbeing of its citizens. Each year more than 900,000 (0.9 million) people die as a result of tobacco use in India, which translates to 2500 deaths every day. Findings from the Global Adult Tobacco Survey (GATS) 2009- 2010 reveal that the estimated number of tobacco users in India is 274.9 million and this number is growing rapidly, especially among women. Research shows that 5500 youth in India start using tobacco daily. A survey of tobacco use among young people, the Global Youth Tobacco Survey-2009, reveals that nearly 15% of youth in India use tobacco [3].
Tobacco was introduced in India by Portuguese barely 400 years ago during the Mughal era. Mainly due to a potpourri of different cultures in the country, tobacco rapidly became a part of socio cultural milieu in various communities, especially in the eastern, north eastern and southern parts of the country [4].
India is also the second largest consumer of tobacco in the world, second only to china. The prevalence of tobacco among adults (15 years and above) is 35%. The prevalence of overall tobacco use among males is 48 percent and that among females is 20 percent. Nearly two in five (38 %) adults areas and one in four (25%) adults in urban areas use tobacco in some form [5].
The challenges posed by tobacco has been countered by different countries with various levels of success. While economically advanced democracies share a broad commitment to liberal political values and demonstrate an interesting range of beliefs and practices with respect to privacy, autonomy, and paternalism, there are examples of developing countries with liberal political values and autonomy such as India, the world’s largest democracy South Africa, and the Philippines which go unmentioned [6].
In south Asia, Bhutan (2004), Thailand (2006) and India (2008) are some of the countries that have successfully enforced a smoking ban in public places. Bhutan is the first country in the world to impose a total ban on tobacco products-sale and use [7]. China introduced a smoking ban in public buildings in Beijing form May 2008 as run-up to the Olympic games [8] and ban on smoking in public places came into effect from 1st May 2011. Singapore has had smoke free legistion since 1970, but has strengthened it recently. 4 Honk Kong enacted the smoking ban law in 1982 but could enforce it only since 2007 [9]. Countries like Indonesia (2006), Kazakhstan (2003), Malaysia (2004), Bangladesh (2006), Pakistan (2003), Philippines (2002), Vietnam (2005), Brunei Barussalam (1988) have banned smoking in public places.
Tobacco Control Developments
Since 1994, multiple legal and scientific developments have altered the tobacco control environment and thus have affected smoking among youth. The states and the U.S. Department of Justice brought lawsuits against cigarette companies, with the result that many internal documents of the tobacco industry have been made public and have been analyzed and introduced into the science of tobacco control. Also, the 1998 Master Settlement Agreement with the tobacco companies resulted in the elimination of billboard and transit advertising as well as print advertising that directly targeted underage youth and limitations on the use of brand sponsorships (National Association of Attorneys General [NAAG] 1998). This settlement also created the American Legacy Foundation. In 2009, the U.S. Congress passed a law that gave the U.S. Food and Drug Administration authority to regulate tobacco products in order to promote the public’s health [10]. Certain tobacco companies are now subject to regulations limiting their ability to market to young people. In addition, they have had to reimburse state governments (through agreements made with some states and the Master Settlement Agreement) for some health care costs. Due in part to these changes, there was a decrease in tobacco use among adults and among youth following the Master Settlement Agreement
Tobacco Control Legislation in India
India has played a leadership role in global tobacco control. With the growing evidence of harmful and hazardous effects of tobacco, the government of India enacted various legislations and comprehensive tobacco control measures [11]. The Government enacted the Cigarettes Act (Regulation of Production, Supply and Distribution) in 1975 [12].
The statutory warning “Cigarette smoking is injurious to health” was mandatorily displayed on all cigarette packages, cartons and advertisements of cigarettes. Some states like Maharashtra and Karnataka restricted smoking in public places. In the case of Maharashtra, specification of the size of boards in English and Marathi were prescribed, declaring certain premises as smoke free [13]. Tobacco smoking was prohibited in all health care establishment, educational institutions, domestic flights, air-conditioned buses, through a Memorandum issued by the Cabinet Secretariat in 1991. Since these were mainly Government or administrative orders; they lacked the power of a legal instrument. Without clear enforcement guideline and awareness of the citizens to their right to smoke-free air [14].
Under the Prevention of Food Adulteration Act (PFA) (Amendment) 1990, statutory warnings regarding harmful health effects were made mandatory for Paan masala and chewing Tobacco [15].
In 1992, under the Drugs and Cosmetics Act 1940 (Amendment), Use of tobacco in all dental products was banned [16]. The Cable Television Networks (Amendment) Act 2000 prohibited tobacco advertising in state controlled electronic media and publications including cable television [17]. Under the chairmanship of Shri Amal Datta, the 22 Committee on Subordinate Legislation in November 1995 recommended to the Ministry of Health to enact Legislation to protect non-smokers from second hand smoke [18]. In addition, the committee recommended stronger warnings for tobaco users, stricter regulation of the electronic media and creating mass awareness programmes to warn people about the harms of tobacco. In a way, this Committee’s recommendations laid the foundation of developing the existing tobacco control legislation in the country.
The law also mandates testing all tobacco products for their tar and nicotine content. Although the Rules pertaining to various provisions under the law were notified during 2002 to 2006, there were many legal challenges which the Government had to face in view of the tobacco industry countering most of these Rules in the court of law. However after a long legal battle and interventions by the civil society, Revised Smoke-free Rules came into the effect from 2 October 2008 [19]. The ban on smoking in public places, which included work places also, was remarkable achievement in terms of political will and national commitment. Subsequently the law pertaining to pictorial warnings on tobacco products packages was applied with effect from 31 May 2009. In 2004, the Government ratified the WHO Framework Convention on Tobacco Control (WHO FCTC), which enlists key strategies for reduction in demand and reduction in supply of tobacco. Some of the demand reduction strategies include price and tax measures and non-price measures (statutory warnings, comprehensive ban on advertisements, promotion and sponsorship, tobacco product regulation etc. The supply reduction strategies include combating illicit trade, providing alternative livelihood to tobacco farmers and workers and regulating sale to and by minors. India has been in the forefront of negotiations under various Working Groups of the WHO FCTC and also played a leadership role in bringing region specific issues e.g. smokeless tobacco products. India provided valuable contribution to development of guidelines for Article 9 and 10, 12, 13, 14, 17 & 18 of WO FCTC.
Fctc & Cotpa To counter this pandemic, FCTC recommends evidence based measures and parallel to the treaty India adopted a comprehensive tobacco control law i.e. the Cigarettes and Other Tobacco Products (Prohibition of Advertisement and Regulation of Trade and Commerce, Production, Supply and Distribution) Act, 2003 (COTPA). Though the national law came into force on May 1, 2004 and the Treaty obligations got effective from February 27, 2005. The later developments in COTPA may be attributed to India’s commitment to appliance the Treaty. Further, the Ministry of Health and Family Welfare, Government of India, as an express commitment to appliance the treaty obligations, took a step towards translating the law into practice and adopted the National Tobacco Control th Programme (NTCP) under the 11 Five Year Plan of 2007- 12 [20].
India also played a strong leadership role in the global fight against tobacco and in the development of FCTC. In terms of legislation in India, a beginning was made in the form of the Cigarettes Act, 1975. However, a comprehensive tobacco control Bill was tabled in the Parliament in late February, 2003. The Bill finally became the tobacco control law of India (COTPA) after receiving assent from the President of India
on May 18, 2003. The Legislation came into force on May 1, 2004 [21].
A law is as good as it is applied. The enactment of COTPA per se does not amount to creation of smoke-free public places or decrease in minors’ access to tobacco products. Unless a committed effort is made to effectively appliance and enforce the law, both at national and sub-national levels, it will have no actual impact on the tobacco control status in the country. In this chapter we review and present the status of overall applianceation of COTPA, and thereby FCTC mandates, in the country.
National Tobacco Control Programme
As the applianceation of various provisions under COTPA lies mainly with the State Governments, effective enforcement of tobacco control law remains a big challenge. To strengthen applianceation of tobacco control provisions under COTPA and policies of tobacco control mandated under the WHO FCTC, the Government of India piloted National Tobacco Control Program (NTCP) in 2007-2008 [22]. The programme is under applianceation in 21 out of 35 States Union territories in the country. In total, 42 districts are covered by NTCP at present. This was a major leap forward for the tobacco control initiatives in the country as for the first time dedicated funds were made available to appliance tobacco control strategies at the central state and sub state levels.
WHO Tobacco Free Initiative in India
During-a series of tobacco Cessation Clinics were set-up in states across the country in diverse settings such as cancer treatment hospitals, psychiatric hospitals, medical colleges, NGOs and community settings to help users to quit tobacco use. This network of Tobacco Cessation Clinic was further expanded in 2005 to cover five new clinics in Regional Cancer Centers (RCCs) in 5 states of which two centers were in North-Eastern States Mizoram and Assam, having high prevalence of Tobacco use. The Tobacco Cessation Clinics were renamed as Tobacco Cessation Centers (TCCs) and their role was expanded to include trainings on cessation and developing awareness generation on tobacco cessation. In 2009, two new TCCs were set up in Rajasthan and Delhi. A model for Workplace TCC was also set up in Nirman Bhawan in Delhi, where the Ministry of Health and Family Welfare is housed [23].
The role of TCCs was further expanded in 2009 and they were designated as ‘Resource Centers for Tobacco Control (RCTC)’. Besides providing tobacco cessation services, these RCTCs helped in capacity building of other institutes to develop tobacco cessation facilities. Many of them have developed outreach programs for the community and are regularly doing awareness programs schools, college, slums and workplaces.
With support from WHO, the following trainings and IEC materials has been developed for facilitating tobacco cessation in the country. National Guidelines for Treatment of Tobacco Depedence have also been developed and disseminated by the Government in 2011, to facilitate training of health professionals in tobacco cessation. Various intervention and research studies were also supported to develop community based tobacco cessation [24]. Various intervention and research studies were also supported to develop community based tobacco cessation models. These included, “An Intervention study on tobacco us practices and impact of cessation strategies among women of Jodhpur districts of Rajasthan,” An intervention study on community based tobacco cessation among women in Varanasi district’ undertaken by Banaras Hindu university, UP and a “Community based Tobacco Cessation Interventions project” in 4 states (Bihar, Assam, Tamil Nadu and Goa), coordinated by RCTC Goa (WHO India supported projects, unpublished).
Under GOI-WHO collaborative Tobacco Free Initiative, consultants have been provided in 12 out of 21 NTCP state to support state governments in applianceation of the programme. WHO has also been supporting activities on World No Tobacco Day (WNTD), every year on 31st May.
Other Initiatives for Tobacco Control
Advocacy for tobacco control-low awareness regarding the anti-tobacco law and its provisions at all levels of governance and policy making has been an important impeding factor for effective applianceation of tobacco control policies. The states had not trained enforcement officials from various departments e.g. police, food, drug, health, labor, railways, transport etc. who have been authorized to enforce provisions under COTPA, resulting in failure to initiate action for violations and the applianceation of the Suffered [25].
Positive Response to Ban on Smoking in Public Places
In a cross sectional study conducted in Tamil Nadu, it was found after a survey among 127 health providers that, 94% of the smokers and 83% of the nonsmokers were aware of the proposed ban on smoking at public places and 50% of the smokers and 69% of non-smokers wanted the ban to be applied. It was also reported that 43.8% of the smokers and 52.3% of the non-smokers were confident that the ban on smoking in public places will be effective [26].
Effect of Smoke-Free Home and Smoke-Free Workplace Policies
It is imperative that progressive steps be taken to protect children from exposure to tobacco smoke at homes. It is suggested that childhood SHS exposure could be considerably reduced by adopting voluntary smoke-free home restrictions. While a mandate for a comprehensive workplace and indoor smoke-free policies imply an apparent benefit in decreased pre-birth risks and reduced asthma disease among children [27]. It is observed that financial incentives work in favour of enforcement of a smoke-free workplace policy and motivates people to quit smoking. The smoke-free workplace has an impact on the exposure to SHS in public places has reduced. Studies have acknowledged that the new regulations provide a basis for enforcing smoke-free initiatives and for the protection of the public, particularly children, women and workforce, from unwanted exposure to SHS) [28].
Rationale of the Study
India is the second largest consumer of tobacco in the world, Tobacco control being a major public health challenge in India; the Government has enacted various tobacco control policies and applied various tobacco control policies and programmes with various level of success. Need of the study to know the current status of awareness of Cigarettes and Other Tobacco Act (COTPA), 2003 in Chandigarh [29, 30, 31, 32].
Aim: To see the awareness of Cigarette and Other Tobacco Products Act (COTPA), 2003 in selected Educational Institution in Chandigarh.
Objectives:
- To study the awareness level of Cigarette and Other Tobacco Products Act (COTPA), 2003.
- To observe awareness of smoking in educational institutes regarding tobacco products and sale of tobacco to minors within 100 yards of Educational Institutes in Chandigarh. It explains procedure and design followed in selection of sample, hypotheses, gives description of tools employed and procedure adopted in data collection, besides the statistical operations carried out for the treatment of the data.
Statement of the Problem: The present study therefore, is an endeavor to find aforementioned -relationships. The title of the study reads as under: Awareness of COTPA (2018) among the vendors near selected educational Institutes in Chandigarh [33].
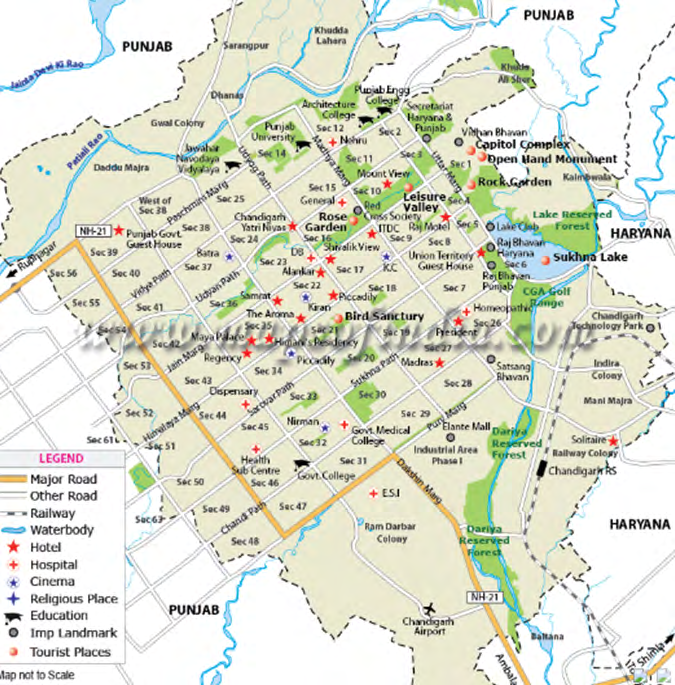
Study area: Chandigarh was the area chosen to study the to see the awareness of Cigarettes and other Tobacco Products Act (COTPA), 2003 in Chandigarh [34].
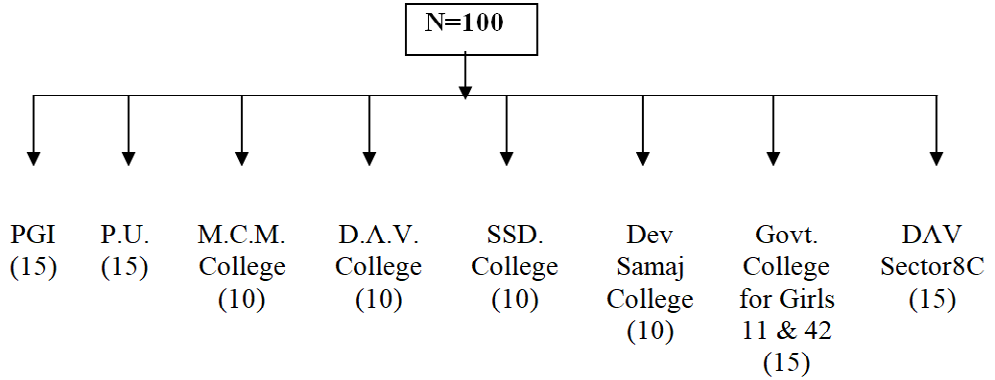
Study design: A Cross-sectional study was used to study the awareness of Cigarettes and other Tobacco Products Act (COTPA), 2003 in Chandigarh [35]. Study period: January 2018 to May 2018. Study tool: A Self-structured questionnaire was used for collecting information on Cigarettes and other Tobacco Products Act, (COTPA) 2003 [36]. Sampling technique and sample size: In view of the time and resources available for the study, an attempt was made to include purposively Vendors (N=100) near Educational Institutions in Chandigarh.
Map showing study area:
Detailed Procedure I have selected ten major institute of Chandigarh. The daily visit was made to Educational Institutions in Chandigarh. Questionnaire was filled by the Vendors. In this way all 100 subject were examined and interviewed in the required period of time [37].
Sample Size N=100 was selected purposely
Statistical Analysis: The data collected was analyzed using Microsoft Excel. Percentage, tables, pie charts, graphs were used to interpretation of data.
Results
The organization, analysis, and interpretation of data, the formation of conclusions, and generalizations are necessary steps for getting a meaningful picture out of the raw information collected. The analysis and interpretation of deal with the objective material and subjective reactions of the material. The data has been used for deriving some inherent meanings in its relation to the problem. An analysis of data means studying the tabulated material in order to determine inherent facts or meanings. It entails breaking down the existing complex factors into simple parts, and thereafter putting those parts together in new arrangements for the purpose of interpretation [38].
For the sake of convenience, data have been presented in tabular form. The data was analyzed in accordance with the objectives of the study.
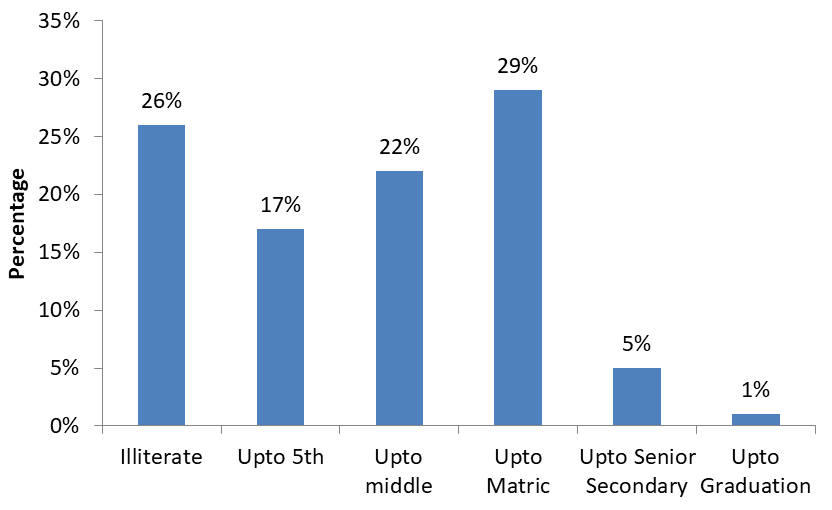
Figure 2 shows that from the total respondents, 75% are male and 25% are female vendors who are taken near from the area of educational institutions in Chandigarh.
Table 1 shows the age wise distribution of the respondents and it is found that majority of respondents i.e. 43% belongs to the age group of 32-45 years, 40% respondents belongs to the age group of 46-69 years whereas 17% belongs to the age group of 16-31 years.
| Age | Frequency | Percentage |
|---|---|---|
| 16-31 | 17 | 17% |
| 32-45 | 43 | 43% |
| 46-69 | 40 | 40% |
| Total | 100 | 100% |
Table 1: Age wise distribution of the respondents.
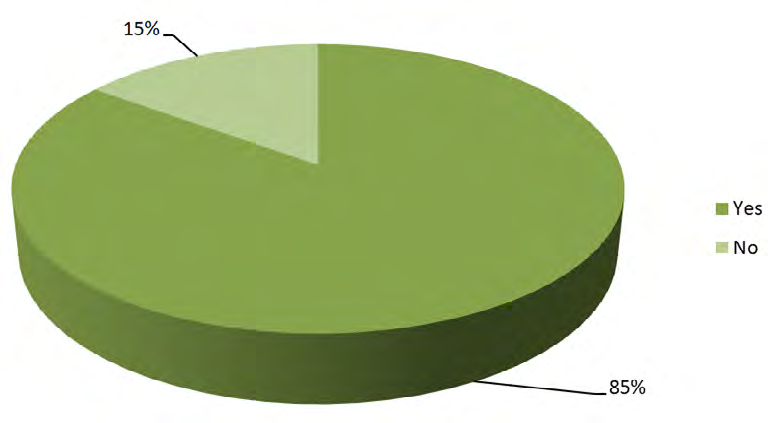
Figure 3 shows the qualification wise distribution of the respondents and it is found that 29% respondents have the qualification upto matric, 22% upto middle, 17% upto 5th and only 5% have the qualification upto sen. secondary whearas 1% have qualification upto graduation but 26% out of total respondents were illiterate or have nil qualification.
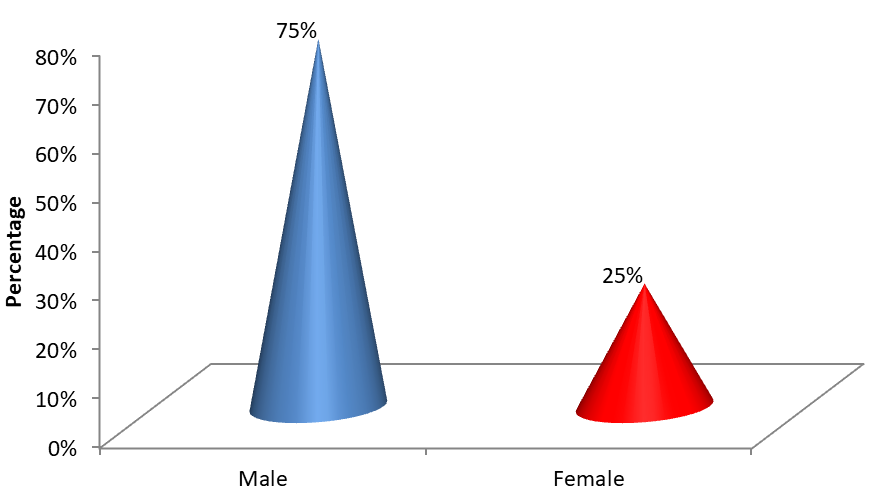
Figure 4 shows the awareness about the smoking in vendors near the educational institutions in Chandigarh and it is found that 85% respondents from near educational institutions do smoking whereas only 15% don’t smoke.
| Awareness about COTPA (2003) | Frequency | Percentage |
|---|---|---|
| Yes | 70 | 70% |
| No | 30 | 30% |
| Total | 100 | 100% |
Table 2: Awareness about COTPA (2003).
Table 2 shows the awareness in respondents regarding the Cigarettes and other Tobacco Products Act (COTPA), 2003 and it is found that majority of respondents i.e. 70% are awared about the Cigarettes and other Tobacco Products Act (COTPA), 2003 as they know that there is a law regarding prohibition of use of Cigarettes and Tobacco products but 30% respondents do not aware about the Act.
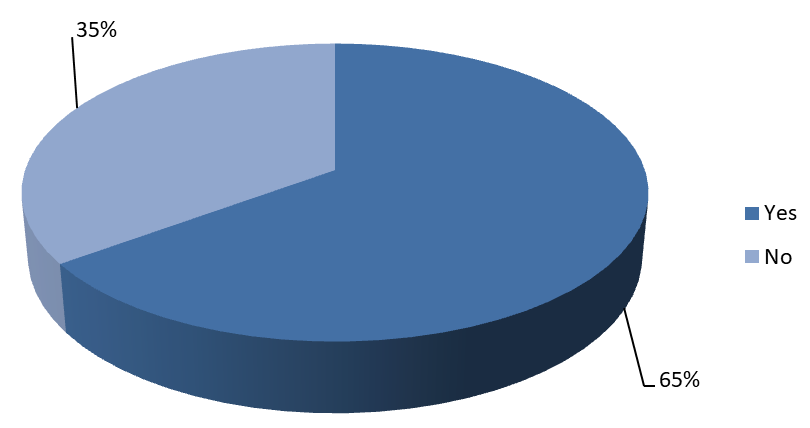
Figure: 5 Awareness about COTPA (2003) i.e. application to all products containing Tobacco in any form i.e. Cigarettes, Cigars, Bidis, Gutka, Panmasala (containing tobacco), Mawa. Khaimi, Snuff etc.
Figure 5 shows the Awareness about COTPA (2003) i.e. application to all products containing Tobacco in any form i.e. Cigarettes, Cigars, Bidis, Gutka, Panmasala (containing tobacco), Mawa. Khaimi, Snuff etc. and it is found that majority of respondents i.e. 65% are aware about the COTPA (2003) i.e. application to all products containing Tobacco in any form i.e. Cigarettes, Cigars, Bidis, Gutka, Panmasala (containing tobacco), Mawa. Khaimi, Snuff etc but 35% respondents were not aware about COTPA (2003) i.e. application to all products containing Tobacco in any form i.e. Cigarettes, Cigars, Bidis, Gutka, Panmasala (containing tobacco), Mawa. Khaimi, Snuff etc [39].
| Smoking in banned in all public places | Frequency | Percentage |
|---|---|---|
| Yes | 69 | 69% |
| No | 31 | 31% |
| Total | 100 | 100% |
Table 4: Smoking in banned in all public places.
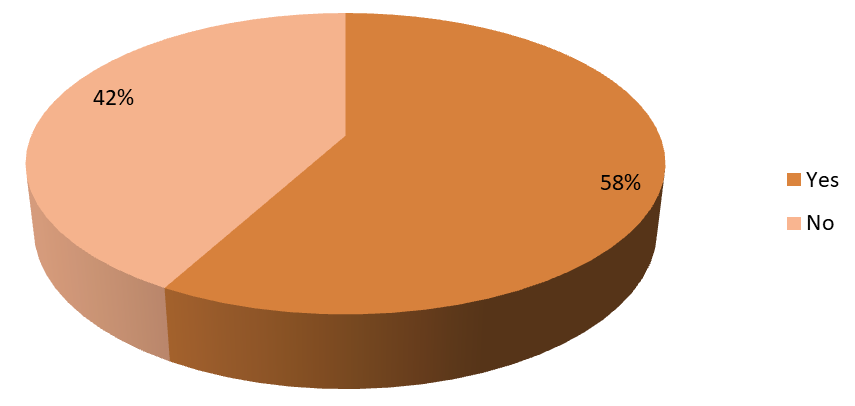
Figure 6 provide the information regarding Awareness in respondents about COTPA (2003) i.e. smoking in banned in all public places and it is found that majority of respondents i.e. 69% were aware about the ban of smoking in all public places as mention in COTPA (2003) but 31% respondents were not aware about the same.
| Every package of cigarette or other tobacco products must bear on its label the specified the health warning | Frequency | Percentage |
|---|---|---|
| Yes | 58 | 58% |
| No | 42 | 42% |
| Total | 100 | 100% |
Table 3: Every package of cigarette or other tobacco products must bear on its label the specified the health warning.
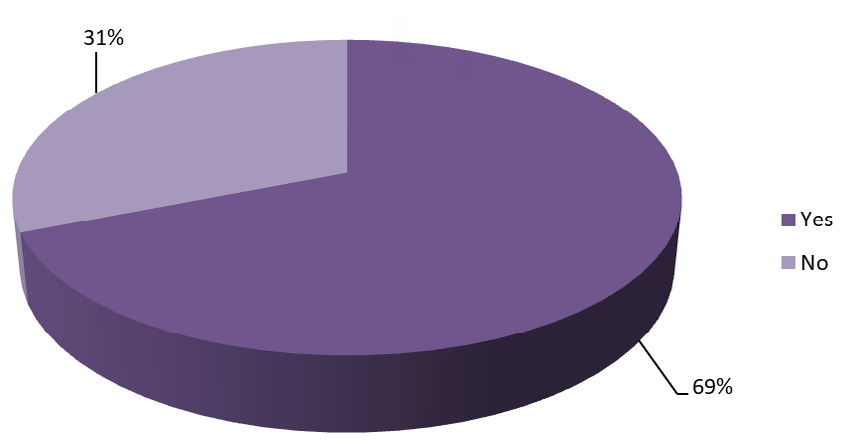
Figure 7: Every package of cigarette or other tobacco products must bear on its label the specified the health warning Figure 7 describes about the Awareness in respondents about COTPA (2003) i.e. every package of cigarette or other tobacco products must bear on its label the specified the health warning and it is found that majority of respondents i.e. 58% were aware and accepted that every package of cigarette or other tobacco products must bear on its label the specified the health warning but 42% respondents were not aware about the same.
| Frequency | Percentage | |
|---|---|---|
| Yes | 56 | 56% |
| No | 44 | 44% |
| Total | 100 | 100% |
Table 5: Does it is sell Tobacco products to Minor.
According to Table 5, when it is asked about the selling of Tobacco products to Minor then 56% respondents out of total accepted that there is selling of Tobacco products to Minor but 44% did not accept so.
| Frequency | Percentage | |
|---|---|---|
| Yes | 40 | 40% |
| No | 60 | 60% |
| Total | 100 | 100% |
Table 6: Does it is seen Tobacco products being sold by a Minor
According to Figure 8, when it is asked about the selling of Tobacco products by Minor then 40% respondents out of total accepted that there is selling of Tobacco products by Minor but 60% did not accept so.
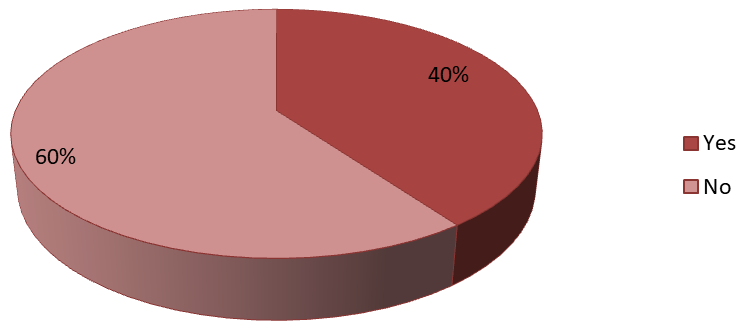
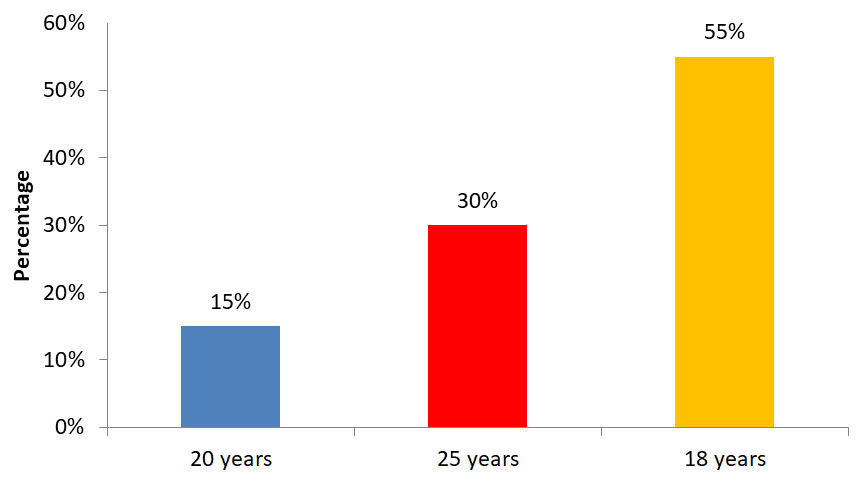
Figure 9 shows that when it is asked about the awareness about the sale of Tobacco products is prohibited to a person under what age then majority of respondents i.e. 55% answered in 18 years, 30% answered in 25 years whereas 15% respond in 20 years.
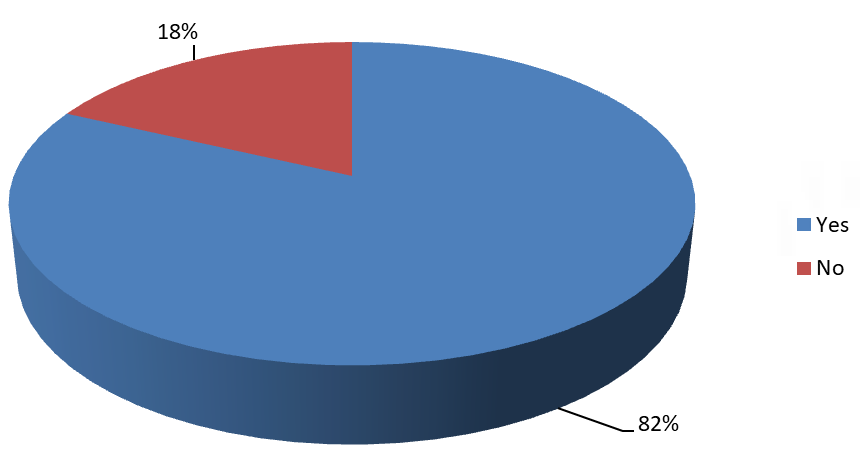
Figure 10 shows that when it is asked about the awareness regarding knowledge of the sale of Tobacco products near Educational Institution is Prohibited then according to 82% respondents sale of Tobacco products near Educational Institution is Prohibited but 18 respondents respond in no.
| Frequency | Percentage | |
|---|---|---|
| Yes | 79 | 79% |
| No | 21 | 21% |
| Total | 100 | 100% |
Table 7: Does the display of non-smoking sign i.e. “Smoking here is strictly prohibited” is mandatory at all public places.
Table 7 shows that when it is asked about the awareness regarding knowledge of the display of non-smoking sign i.e. “Smoking here is strictly prohibited” is mandatory at all public places then according to 79% respondents accepted that the display of non-smoking sign i.e. “Smoking here is strictly prohibited” is mandatory at all public places but 21% respondents did not accept so [40].
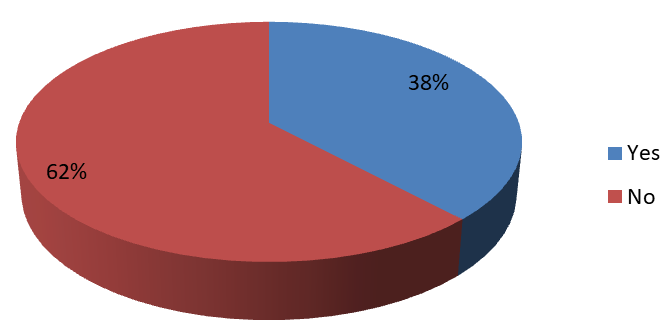
Figure 10 shows that when it is asked about the awareness regarding Whether they seen Warning Boards banning sale of tobacco products to minor, placed at the point of sale in shops kiosks etc. then according to 62% respondents they did not seen Warning Boards banning sale of tobacco products to minor, placed at the point of sale in shops kiosks etc. whereas 38% respondents accepted that they seen Warning Boards banning sale of tobacco products to minor, placed at the point of sale in shops kiosks etc [41].
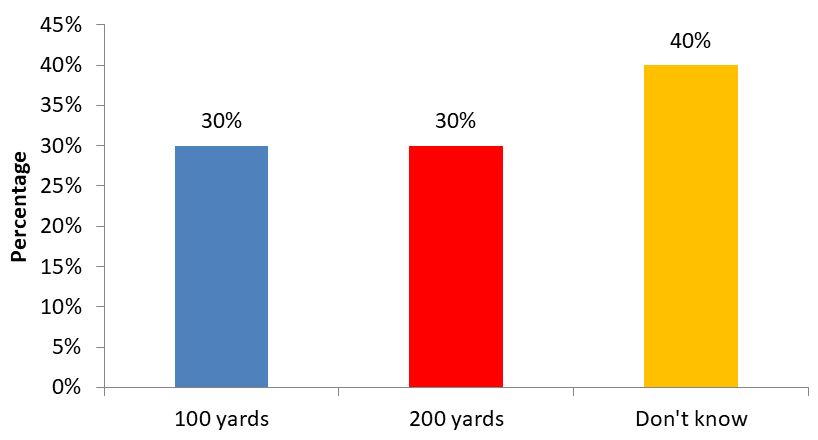
Figure 12 shows that when it is asked about the awareness regarding whether the sale of tobacco products is prohibited in an area within radius of..... yards of any educational institutional then according to 30% respondents sale of tobacco products is prohibited in an area within radius of 100 yards and according to 30% respondents sale of tobacco products is prohibited in an area within radius of 100 yards but 40% respondents do not know about the according radius of area where sale of tobacco products is prohibited.
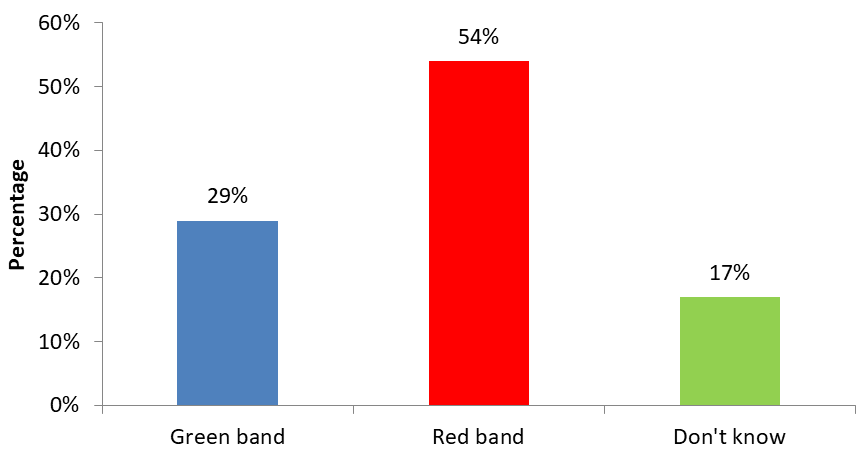
Figure 13 shows that when it is asked about the awareness about the warning written on display board 35% respond about No smoking area whereas 25% respond about No smoking area smoking here is an offence but majority of respondents i.e. 40% did not aware about the warning written on display board.
| Frequency | Percentage | |
|---|---|---|
| Beedi or Cigarette | 38 | 38% |
| Khaini | 22 | 22% |
| Don’t know | 40 | 40% |
| Total | 100 | 100% |
Table 8: Awareness about the display board shall contain a picture of.
Table 8 shows about the Awareness in respondents about the display board shall contain a picture and according to 38% respondents display board should contain a picture of Beedi or Cigarette, according to 22% respondents display board should contain a picture of Khaini but 40% respondents do not know or aware about the picture which should contain on display board.
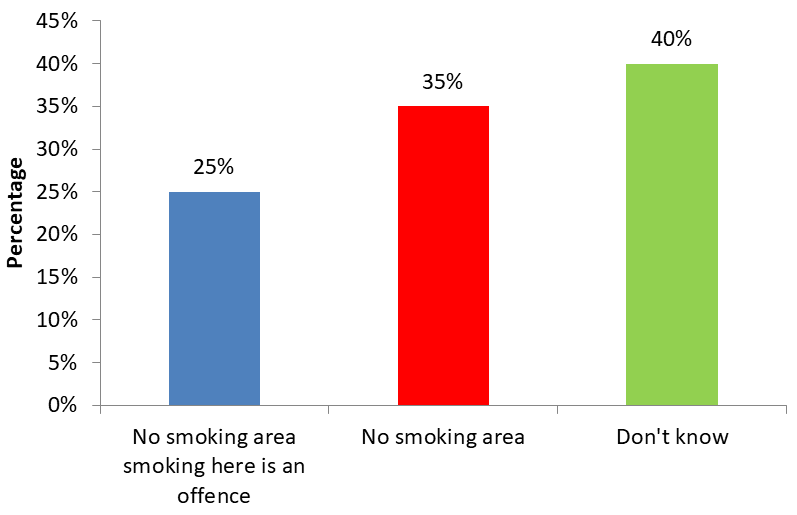
Figure 14 shows about the Awareness in respondents about the product displayed at the center of the display board shall be crossed by and according to majority of respondents i.e. 54% respondents product displayed at the center of the display board should be crossed by red band whereas according to 29% respondents product displayed at the center of the display board should be crossed by green band but 17% respondents respond in don’t know.
| Frequency | Percentage | |
|---|---|---|
| Yes | 68 | 68% |
| No | 32 | 32% |
| Total | 100 | 100% |
Table 9: Awareness about fine being imposed on people smoking in public places.
Table 9 shows that when it is asked about fine being imposed on people smoking in public places then majority of respondents i.e. 68% respond in yes whereas 32% respond in no.
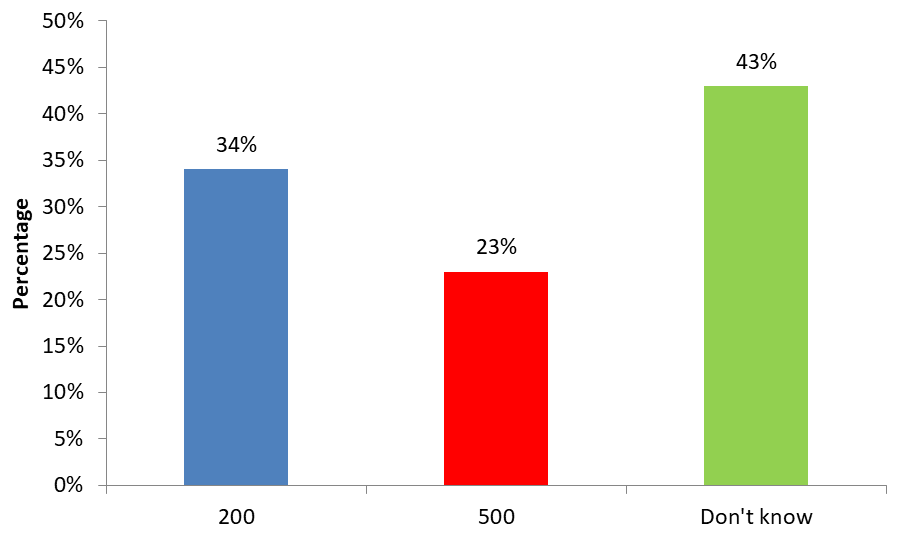
Figure 15 show that when it is asked about the amount of fine being imposed on people smoking in public places then 34% respondents respond that 200 Rs. fine being imposed on people smoking in public places, 23% respondents respond that 500 Rs. fine being imposed on people smoking in public places whereas majority of respondents do not know about this.
| Frequency | Percentage | |
|---|---|---|
| Yes | 26 | 26% |
| No | 74 | 74% |
| Total | 100 | 100% |
Table 11: Awareness about whether the direct and indirect advertisement of tobacco products in the form of audio visual and print
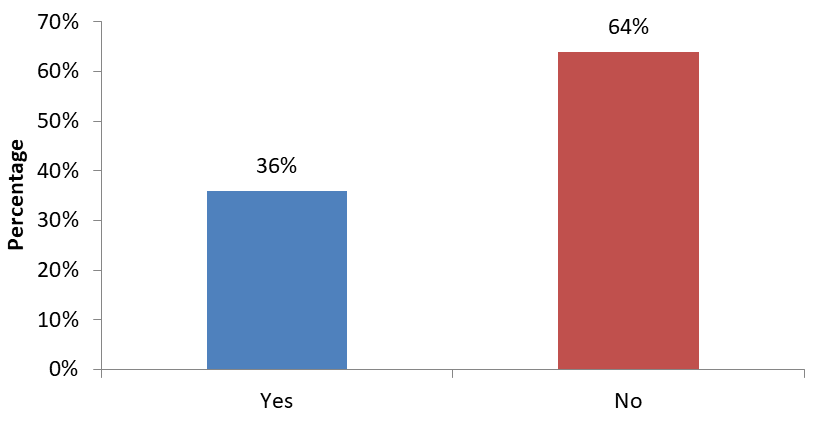
Figure 16 show that when it is asked about the Awareness about whether the direct and indirect advertisement of tobacco products in the form of audio visual and print media prohibited then majority of respondents i.e. 74% respond in no whereas 26% respond in yes.
| Frequency | Percentage | |
|---|---|---|
| Yes | 36 | 36% |
| No | 64 | 64% |
| Total | 100 | 100% |
Table 10: Awareness about whether the Cigarette and other tobacco product companies can sponsor any sport and cultural events.
As per the Figure 17, 64% respondents correctly know that Cigarette and other tobacco product companies cannot sponsor any sport and cultural events whereas 36% respondents said that Cigarette and other tobacco product companies can sponsor any sport and cultural events.
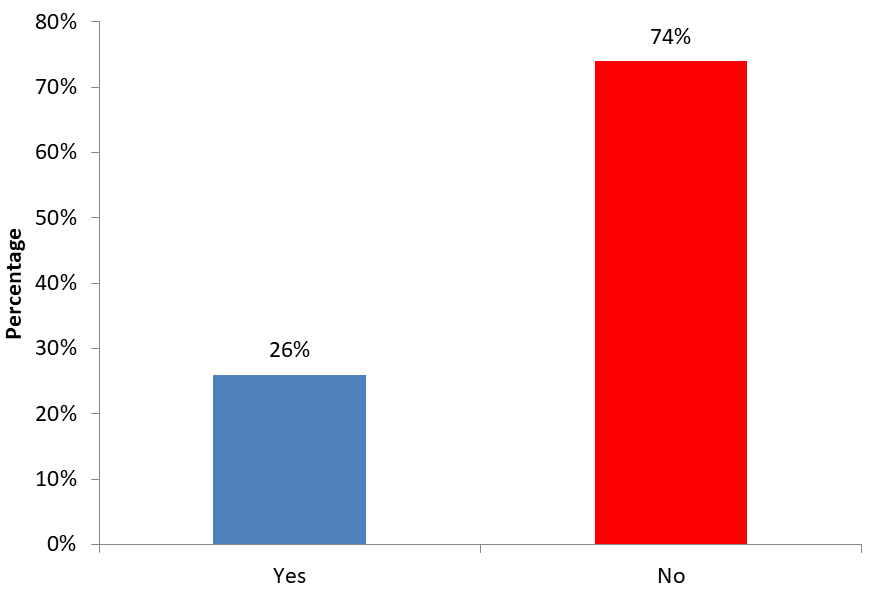
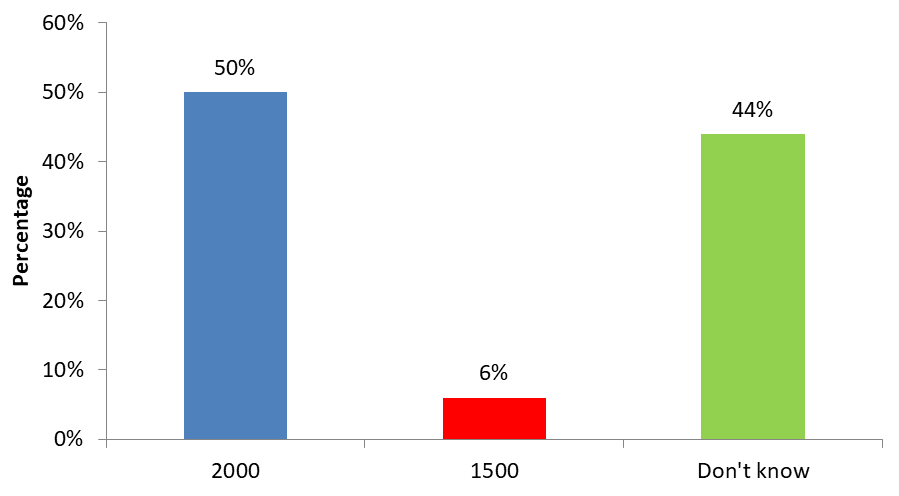
Figure 18 shows that 50% respondents correctly know that the fine for direct and indirect advertisement of Tobacco
products is INR 2000, 44% respondents did not know about the amount of fine for direct and indirect advertisement of Tobacco products whereas 6% respondents respond that the fine for direct and indirect advertisement of Tobacco products is Rs. 1500.
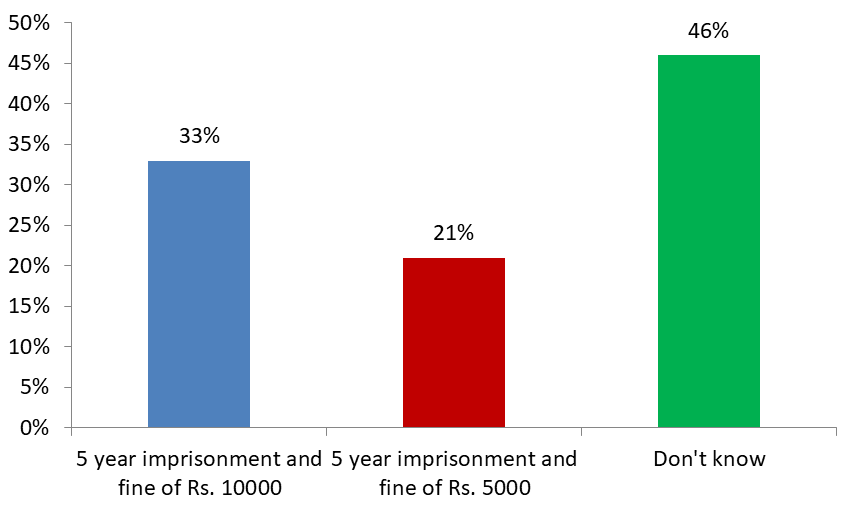
Figure 19 shows that 43% respondents correctly know that punishment for the advertisement of Tobacco products is 2 years and Rs. 1000 whereas 6% respond in 2 years and Rs. 100 but 47% did not have any idea regarding punishment for the advertisement of Tobacco products.
| Frequency | Percentage | |
|---|---|---|
| 2 year imprisonment and fine of Rs. 5000 or both | 52 | 52% |
| 5 year imprisonment and fine of Rs. 10000 or both | 8 | 8% |
| Don’t know | 40 | 40% |
| Total | 100 | 100% |
Table 12: Awareness about punishment for the manufactures of Cigarettes and Tobacco products who do not specify health warnings an
Table 12 shows that 52% respondents correctly know that punishment for the manufactures of Cigarettes and Tobacco products who do not specify health warnings and nicotine and tar content on the label of their products is 2 year imprisonment and fine of Rs. 5000 or both whereas 8% respondents respond that punishment for the manufactures of Cigarettes and Tobacco products who do not specify health warnings and nicotine and tar content on the label of their products is 5 year imprisonment and fine of Rs. 10000 or both but 40% did not have any idea regarding punishment for the manufactures of Cigarettes and Tobacco products who do not specify health warnings and nicotine and tar content on the label of their products [42, 43].
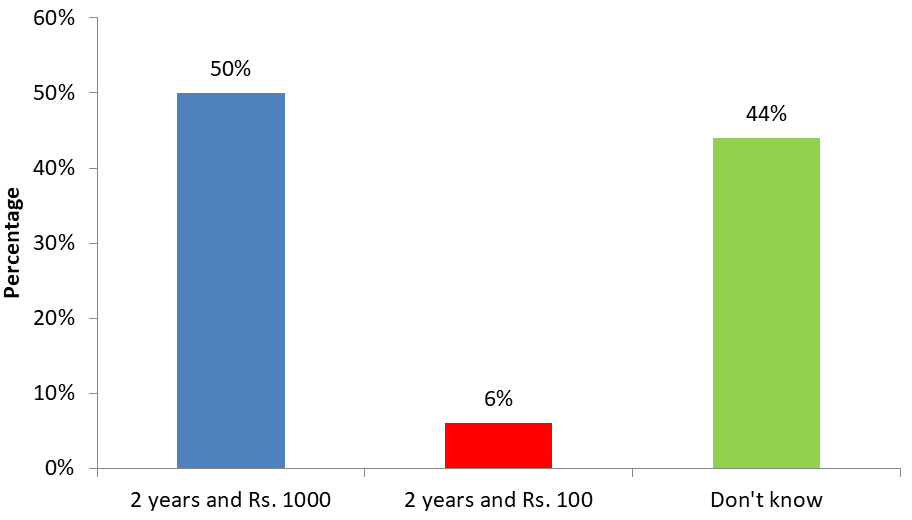
Figure 20 shows that 33% respondents correctly know that punishment for the second and subsequent conviction related to the direct and indirect advertisement of Tobacco products is 5 year imprisonment and fine of Rs. 10000 whereas 21% respondents respond that punishment for the second and subsequent conviction related to the direct and indirect advertisement of Tobacco products is 5 year imprisonment and fine of Rs. 5000 but 46% did not have any idea regarding punishment for the second and subsequent conviction related to the direct and indirect advertisement of Tobacco products [44].
It is observed that 53% respondents hold the opinion that the current level of enforcement of pictorial health warning on Tobacco products can motivate people to quit tobacco use. 47% respondents opined that the current level of enforcement of pictorial health warning on Tobacco products cannot motivate people to quit tobacco use and according to the result majority of respondents believed that current level of enforcement of pictorial health warning on Tobacco products can motivate people to quit tobacco use.
About 52% respondents hold the opinion that the current level of enforcement of ban on smoking in public places can motivate people to quit tobacco use. 48% respondents opined that the current level of enforcement of ban on smoking in public places cannot motivate people to quit tobacco use and according to the result majority of respondents believed that current level of enforcement of ban on smoking in public places can motivate people to quit tobacco use.
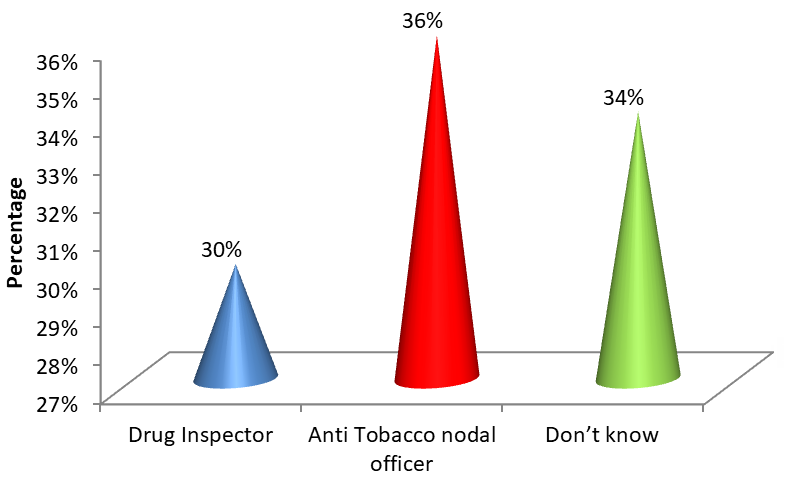
As per Figure 21, 36% respondents correctly know that Anti Tobacco Nodal Officer is the Enforcement officer. 30% were wrong by giving the answer Drug Inspector whereas 34% respondents did not know about the answer.
It was found that 62% respondents experienced fine by authority whereas 38% respondents did not experience any fine by any authority. Result shows that majority of respondents experience fine by any authority.
Analysis of data reveals the information regarding the time period since the tobacco product is selling by the vendors or respondents in the particular area near an educational institution and it is found that majority of respondents i.e. 55% selling the product from 2011-2017 whereas 45% were selling the product from 2004-2010.
Discussion
India is also the second largest consumer of tobacco in the world, second only to china. The prevalence of tobacco among adults (15 years and above) is 35%. The prevalence of overall tobacco use among males is 48 percent and that among females is 20 percent. Nearly two in five (38 %) adults areas and one in four (25%) adults in urban areas use tobacco in some form.
The Government enacted the Cigarettes and Other Tobacco Products (Prohibition of Advertisement and Regulation of Trade of Commerce, Production, Supply and Distribution) Act (COTPA), in 2003.
Rao, et al. [41] in their study on knowledge attitude and practices regarding the cigarettes and other tobacco products act (COTPA) in Khammam, Andhra Pradesh concluded that nearly half the participants had awareness of COTPA and nearly two thirds had an overall positive attitude towards COTPA. Yet participants opined that the applianceation of the Legislation was not effective. Hence a concerted effort has to be made to increase the awareness of the Act amongst the vulnerable population, i.e., younger population, people from lower SES, and less educated people. Also the Act should be applied in true spirit so as to dissuade the population from falling victims to the tobacco epidemic.
Annadurai, et al. [42] on Tobacco usage among Males in Rural Tamil Nadu, India shows that Prevalence of smoking was found to be 36.7%. Cigarette smoking was more common than beedi and smokeless tobacco. This study concluded that strict enforcement of anti-tobacco legislation and awareness measures targeting ill-effects of tobacco can be intensified to reduce tobacco releated morbidity and mortality.
Sharma, et al. [31] reported that lack of complete information and awareness of the Act, public opposition, cultural acceptance of tobacco use, lack of political support, and less priority for tobacco control were noted barriers for applianceation of COTPA in the state.
Majority of respondents i.e. 69% were aware about the ban of smoking in all public places as mention in COTPA (2003) that smoking in banned in all public places but 31% respondents were not aware about the same.
Regarding awareness in respondents about COTPA (2003) i.e. every package of cigarette or other tobacco products must bear on its label the specified the health warning, it is found that majority of respondents i.e. 58% were aware and accepted that every package of cigarette or other tobacco products must bear on its label the specified the health warning but 42% respondents were not aware about the same.
It was found in our study that when it is asked about the amount of fine being imposed on people smoking in public places then 34% respondents respond that 200 Rs. fine being imposed on people smoking in public places, 23% respondents respond that 500 Rs. fine being imposed on people smoking in public places whereas majority of respondents do not know about this.
The present study shows that 50% respondents correctly know that the fine for direct and indirect advertisement of Tobacco products is INR 2000, 44% respondents did not know about the amount of fine for direct and indirect advertisement of Tobacco products whereas 6% respondents respond that the fine for direct and indirect advertisement of Tobacco products is Rs. 1500.
Tripathy, et al. [40, 45, 46] in their study compliance monitoring of prohibition of smoking (under section-4 of COTPA) at a tertiary health-care institution in a smoke-free city of India showed that a total of 40 public places were visited during the study. Overall compliance rate for section-4 of COTPA was to be a mere 23% [47, 48].
Our study revealed that selling of Tobacco products to Minor then 56% respondents out of total accepted that there is selling of Tobacco products to Minor but 44% did not accept so. 40% respondents out of total accepted that there is selling of Tobacco products by Minor but 60% did not accept so. 53% respondents hold the opinion that the current level of enforcement of pictorial health warning on Tobacco products can motivate people to quit tobacco use. 47% respondents opined that the current level of enforcement of pictorial health warning on Tobacco products cannot motivate people to quit tobacco use and according to the result majority of respondents believed that current level of enforcement of pictorial health warning on Tobacco products can motivate people to quit tobacco use.
Conclusion
It can be concluded that majority of respondents (70%) are aware about the Cigarettes and other Tobacco products Act, 2003 as they know that there is law regarding prohibition of use of Cigarette and Tobacco product but 30% respondents were not aware about the COTPA Act, (2003). About 79% respondents accepted that display of non-smoking signs i.e. smoking here is strictly prohibited is mandatory all the public places. 30% respondents sale of Tobacco products is prohibited in an area within the radius of 100 yards of the Educational Institutes.
Acknowledgements
The authors would like to acknowledge all the participants for their consent and cooperation.
Funding
No funding sources
Conflict of Interest
None declared
Ethical Considerations
The subjects were informed about the purpose of the study. They were assured that all personal information would be kept confidential and used only for research and study purpose. The study was approved by the Institutional Ethics Committee.
References
-
Dalton MA, Beach ML, Adachi-Mejia AM, Longacre MR, Matzkin AL, et al. (2009) Early exposure to movie smoking predicts established smoking by older teens and young adults. Pediatrics. 123(4): e551-e558.
-
Fagerström K (2002) The epidemiology of smoking: health consequences and benefits of cessation. Drugs 62: 1-9.
-
Lovato C, Watts A, Stead LF (2011) Impact of tobacco advertising and promotion on increasing adolescent smoking behaviours. Cochrane Database of Systematic Reviews 2011(10): CD003439.
-
Government of India. Ministry of Health & Family Welfare, Global Adult Tobacco Survey, India, 2010.
-
Feldman EA, Bayer R (2004) Unfiltered: Conflict over tobacco policy and public health. pp: 394.
-
Government of India (1975) The Cigarettes Act (Regulation of Production, Supply and Distribution).
-
(1987) Government of Maharashtra, Public Health Department, Resolution No. CNC 1036/CR 241/PH-6.
-
Government of India (1990) Cabinet Secretariat O.M.
-
Family Smoking Prevention and Tobacco Control Act 2009.
-
Rao V, Chaturvedi P (2010) Tobacco and health in India. Indian J Cancer 47(1): 3-8.
-
(1990) Government of India. Prevention of Food Adulteration Act (PFA) (Amendment).
-
Government of India. Drugs and Cosmetics Act 1940.
-
Government of India. The Cable Television Networks (Amendment) Act 2000.
-
(2003) The Cigarettes and Other Tobacco Products (Prohibition of Advertisement and regulation of Trade and Commerce, production, Supply and Distribution) Act, 2003. An Act enacted by the Parliament of Republic of India by notification in the Official Gazette.
-
(2008) Revised Smoke free Rules. Notification in the Official Gazette GSR 417 (E) dated 30 th May, 2008.
-
http://pib.nic.in/PressReleaseIframePage. aspx?PRID=1530950.
-
Government of India. National Tobacco Control Programme 2008.
-
Government of India. Ministry of Health & Family Welfare (2011) Directorate General of Health Services. Tobacco Dependence Treatment Guidelines.
-
Government of India. Ministry of Health and Family Welfare. Directorate General of Health Services. National Tobacco Control Programme. Handbook: Comparative analysis of FCTC and Indian Laws relating Tobacco.
-
Jaleel MA, Hussain A, Rauf S, Ali L, Tanoli T, et al. (2001) An epidemological study of smoking at Abbottabad. J Ayub Med coll Abbottabad 13(1): 34-36.
-
Kabir Z, Alpert HR, Goodman PG, Haw S, Behm I, et al. (2010) Effect of smoke-free home and workplace policies on second-hand smoke exposure levels in children: An evidence summary. Pediatric Health 4(4): 391-403.
-
Ferry LH, Grissino LM, Runfola PS (1999) Tobacco dependence curricula in US undergraduate medical education. JAMA 282(9): 825-829.
-
Chapman SLC, Wu LT (2004) E-cigarette prevalence and correlates of use among adolescents versus adults: A review and comparison. J Psychiatr Res 54: 43-54.
-
Jindal SK (2004) Why did India need WHO Framework convention on tobacco control?. Lung India 3 (2): 42-43.
-
Kabir Z, Alpert HR, Goodman PG, Haw S, Behm I, et al. (2007) Effect of smoke-free home and workplace policies on second-hand smoke exposure levels in children: an evidence summary. Pediatric Health 4(4): 391-403.
-
Chaudhry S, Chaudhry K (2007) Point of sale tobacco advertisements in India. Indian J Cancer 44(4): 131-136.
-
Jandoo T, Mehrotra R (2008) Tobacco control in India: present scenario and challenges ahead. Asian Pac J Cancer Prev 9(4): 805-810.
-
Anandh K (2009) Comment on the Tobacco Products Act, 2003. Social Science Research Network.
-
Kaur P (2010) Monitoring tobacco use and implementation of prevention policies is vital for strengthening tobacco control: an Indian perspective. Int J Public Health 55(3): 229-30.
-
Thakur JS (2007) Chandigarh The first smoke-free city in India. Indian Journal of Community Medicine 32(3): 169-170.
-
Sharma DC (2004) India bans tobacco advertising and smoking in public places. Lancet 363(9403): 135.
-
Mathur N, Tripathy V, Perry C, Reddy KS, Arora M (2011) Tobacco control among disadvantaged youth living in lowincome communities in India: introducing Project Activity. Asian Pac J Cancer Prev 11(1): 45-52.
-
Chaturvedi P (2011) Tobacco and health in India. Indian J Cancer 47(1): 3-8.
-
Sinha DN (2011) Gutka Advertisement and Smokless Tobacco Use by Adolescents in Sikkim, India. Indian Journal of Community Medicine pp: 43.
-
Choudhury CR, Dey A (2011) India should ban chewing tobacco as well as smoking. Bulletin of the World Health Organization 82: 473-474.
-
Panda B, Rout A, Pati S, Chauhan AS, Tripathy A, et al. (2011) Tobacco control law enforcement and compliance in Odisha, India--implications for tobacco control policy and practice, Asian Pac J Cancer Prev 13(9): 4631-4237.
-
Murthy P, Manjunatha N, Subodh BN, Chand PK, Benegal V (2011) Substance use and addiction research in India. Indian J Psychiatry 52(1): 189-199.
-
De-Addiction Centre, National Institute of Mental Health and NeuroSciences. Bangalore-560029, India.
-
Rajiv N, Rimal (2020) George Washington University, from the Institute for Global Tobacco Control at the Johns Hopkins Bloomberg School of Public Health with funding from the Bloomberg Initiative to Reduce Tobacco Use.
-
Tripathy JP, Goel S, Patro BK (2013) Compliance monitoring of prohibition of smoking (under section-4 of COTPA) at a tertiary health-care institution in a smoke- free city of India. Lung India 30(4): 312-315.
-
Rao AS, Dudala SR, Bolla CR, Kumar RPB (2013) Knowledge attitude and practices regarding the cigarettes and other tobacco products act (COTPA) in Khammam, Andhra pradesh. International Journal of Research in Health Sciences 1(2): 96-102.
-
Annadurai K, Geetha M, Dhanasekaran R (2013) Tobacco Usage among Males in Rural Tamil Nadu, India: A Cross-sectional Study, International Journal of Medical Students 2(1): 93-94.
-
Jena KP, kishor J, Sarkar KB (2013) Global Adult Tobacco Survey (GATS): a case for change in definition, analysis and interpretation of “cigarettes” and “cigarettes per day” in completed and future surveys. Asian Pac J Cancer Prev 14(5): 3299-3304.
-
Shinha DN, Gupta PC, Pednekar MS (2003) Tobacco use among students in Eight Northeastern States of India. Indian J Cancer 40(2): 43-59.
-
Reddy KS, Gupta PC (2004) Report on tobacco control in India. Ministry of Health & Family Welfare, Government of India.
-
Venugopal DC, Vidhubala E, Sundaramoorthy C (2017) Does Awareness on Tobacco Control Legislations Pertaining to Tobacco Sellers Lead to Compliance? – A Study from Chennai, India. Asian Pac J Cancer Prev 18(9): 2349-2354.
-
Mathers CD, Loncar D (2006) Projections of global mortality and burden of disease from 2002 to 2030. PloS Med 3(11): e442.
-
Shimkhada R, Peabody JW (2003) Tobacco control in India. Bull World Health Organ 81(1): 48-52.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines