Burden of Thalassemia in Iraq
Thalassemia is a common hereditary hemoglobinopathy that occurs all over the world, mostly in the middle and low-income countries. We set this study to study the demographic and clinical profile of thalassemia patients, and to highlight the burden of this disorder on the health system, in Iraq. This cross sectional survey was carried out during the period from January through June 2022 in the two major centers of thalassemia in Baghdad. All thalassemia patients that were attending those centers during a six-month period, were included. The direct and indirect annual cost of medicines and health services were computed. The prevalence of thalassemia is slopping up, with the estimated annual cost of health care regarding diagnosis, treatment, blood transfusions and other services for each thalassemia patients is $6815. The indirect health care services were $3995, making the total annual cost for each thalassemia patient $10810. It is proven that consanguineous marriages increase the prevalence of Thalassemia. Public policies aimed at clarifying this for the population would be relevant. The annual cost for thalassemia patients in Iraq is relatively high, most of which is covered by the Ministry of Health and its institutions. This causes a burden on the health system. Also, adopting new policies to reduce the costs especially through finding substitutes (or less costly therapy) for blood chelating agents, is crucial on the long term strategy.
Introduction
Thalassemia; one of the common hereditary hemoglobinopathies, occurs all over the world, with a global prevalence of 4.4/10,000 live births, more common among Greek, Italian, Turkish, Middle Eastern, South Asian, and African descent, almost equally distributed between males and females. As of 2015, thalassemia affected 280 million people, with about 439,000 having severe disease. It is estimated that, worldwide, 60,000 to 70,000 infants are born with β-thalassemia major each year. The mortality rate is relatively high, it resulted in 16,800 deaths in 2015, mostly in the developing world, where the majority of patients die before the age of 20 years [1].
About 1.5% of the global population are carriers of β-thalassemia. In the United States, although it is rare, there are an estimated 1.25 million carriers [2].
The symptoms of thalassemia usually appear during the first two years of life, and the severity is determined to a large extent by the degree of chain imbalance. The treatment consists of repeated blood transfusions with chelating agents to reduce iron overload and hemochromatosis. In the severe cases, survival is dependent on the regular blood transfusions, which, in turn, may cause transfusion iron overload, which is a common clinical problem, arising from disorders of increased iron absorption such as hereditary hemochromatosis, thalassemia intermedia syndromes, or as a consequence of chronic blood transfusions, and may lead to secondary multi-organ damage due to iron toxicity [3, 4, 5, 6, 7].
Thalassemia is common in the East Mediterranean region, where the prevalence of β-thalassemia is 9.0 per 1000, [8] whereas it is 0. 7 per 1000 in the Sultanate of Oman, and ranges from 3 to 100 patients per 100,000 people in Iran [5, 6]. A systematic review of 18 studies in the Gulf Cooperation Council countries revealed that the prevalence of thalassemia among children below five years of age ranged from 0.25% to 33%, with 0.9% in those above five years, and from 0.035% to 43.3% among adults, where the main risk factor being consanguineous marriage [7].
The last estimated total number of registered cases of thalassemia in Iraq is 13390 giving a prevalence of 3.4/10000 [8]. A study in Iraq showed that about 66.0% of the patients were under 15 years of age, 78.8% of whom reported related parents (consanguineous marriage). Thalassemia represented 75% of all hemoglobinopathies in Iraq. The highest prevalence was registered in Basra province, with β-thalassemia major represented 67% of all types of thalassemia [9]. This causes a noticeable burden on the health budget, as the cost of the chelating agent, desferrioxamine in particular, is remarkably expensive. Thalassemia patients are susceptible to many complications, 55.9% had at least one complication, such as marked hepato- splenomegaly, attributed to excessive red cell destruction, 25.8% of the patients in Iraq have splenomegaly (4.4% of whom have hepatomegaly as well), also extra medullary hematopoiesis, iron overload, osteoporosis (67.5%) and osteopenia (9.4% of the patients) [5, 10].
Our objectives were to study the demographic and clinical profile of thalassemia patients in Iraq, and to highlight the burden of this blood disorder on the Iraqi health system.
Methods
This cross sectional survey was carried out during the period from January through June 2022 in the two major centers of thalassemia in Baghdad city; Al-Karama center in Karkh side, and Ibn-Albildy center in Russafa side. All thalassemia patients that were attending the main two centers (for periodic follow up, investigations, and blood transfusion) during a six month period, were collected using a consecutive non-probability sampling technique.
After reviewing several published articles, a specially designed semi-structured questionnaire was developed, it included questions about the demographic characteristics of the patients (age, gender, residence, consanguinity marriage of the parents, education, occupation, and family history of thalassemia). It also included questions that enquire about the clinical profile of the patients (main symptoms, age at onset, duration of illness, frequency of blood transfusion, and complications). Data were also collected from the administrative/financial department of the Ministry of Health, where we dag for the cost of each item with respect to bed occupancy, investigations, blood transfusion, and treatment, in addition to the cost of man power work in the surveyed thalassemia centers to estimate the approximate economic burden of the disease on the families and on the health system.
The questionnaire was validated by the scientific/ ethical committee in the Family and Community Medicine Department, Mustansiriyah College of Medicine, and modified for the purpose of the study. The questionnaire was developed in English, translated to Arabic, and then retranslated to English to enhance validity.
Data were collected on daily basis through a direct face to face interview with the patients (or their parents), after taking the required permissions from the health authorities and the managerial of the centers. Data collection was carried out by two teams (a male and a female in each). The interviewers were qualified, well trained, and have good experience in data collection. Each interview took about 30- 40 minutes.
All the investigations that were done during a year time period (for each patient) were collected (from the patient’s file), in addition to the treatment received, blood transfusions, and any other medications and interventions.
- Inclusion/Exclusion Criteria: Any patient (male or female) diagnosed with thalassemia, for not less than one year, was included. Patients with other hemoglobinopathies were excluded from the study.
- Ethical Issue: The interviews were conducted only after explaining to the patients the purpose of the survey, taking their full, unconditioned consent to participate. Privacy was secured during the interview, and the participants were assured that all the information they give will be dealt with confidentially, and would only be used for research purposes. Data entry was done using the statistical Packages for Social Sciences (SPSS version 26). Data were presented as numbers and percentages.
Results
Out of the 240 patient that been asked to participate, only 214 accepted, giving a response rate of 89%. The results revealed that more than half the cases (54.7%) were less than 15 years of age. Female form 64.5% of the sample with a female to male ratio of 1.8:1, and 57.9% reported a consanguinity marriage of their parents. Most of the cases (64.5%) were among large size families (>5 members), and 70.6% of the patients’ mothers and 64% of the fathers were illiterate or had only primary school education. Thalassemia was more registered among families with low socio-economic status. The vast majority of the patients (93%) reported the presence of other thalassemia patients in the same family (Table 1).
| n | % | ||
|---|---|---|---|
| Age group | 1-5 | 22 | 10.3 |
| Age group | 6-10 | 37 | 17.3 |
| Age group | 11-15 | 56 | 26.2 |
| Age group | 16-20 | 37 | 17.3 |
| Age group | 21-25 | 41 | 19.1 |
| Age group | >25 | 21 | 9.8 |
| Gender | Female | 138 | 64.5 |
| Gender | Male | 76 | 35.5 |
| Parents’ consanguinity | Yes | 125 | 57.9 |
| Parents’ consanguinity | No | 89 | 42.1 |
| Residence | Rural | 157 | 74 |
| Residence | Urban | 57 | 26 |
| Patient employment | Child | 152 | 71 |
| Patient employment | Governmental employee | 5 | 2.3 |
| Patient employment | Private employee | 11 | 5.1 |
| Patient employment | Jobless | 46 | 21.5 |
| Father employment | Public employee | 101 | 47.2 |
| Father employment | Private employee | 61 | 28.5 |
| Father employment | Jobless | 43 | 20.1 |
| Father employment | Daily workers | 9 | 4.2 |
| Father employment | Pre-school age | 22 | 10.3 |
| Father employment | Illiterate | 61 | 28,5 |
| Patient education status | Primary | 77 | 36 |
| Patient education status | Secondary | 39 | 18.2 |
| Patient education status | College and higher | 15 | 7 |
| Family size | <5 | 76 | 35.5 |
| Family size | 5-10 | 118 | 55.2 |
| Family size | >10 | 20 | 9.3 |
| Number of other thalassemia patients in the family | 1-2 | 168 | 78.5 |
| Number of other thalassemia patients in the family | 3-4 | 25 | 11.7 |
| Number of other thalassemia patients in the family | ≥5 | 6 | 2.8 |
| Duration of illness (years) | <1 | 22 | 10.3 |
| Duration of illness (years) | 2-5 | 31 | 14.5 |
| Duration of illness (years) | 6-9 | 31 | 14.5 |
| Duration of illness (years) | 10+ | 130 | 60.7 |
| Physical complications | Chronic hepatitis | 36 | 16.8 |
| Physical complications | Heart failure | 16 | 7.5 |
| Physical complications | Hypothyroidism | 8 | 3.7 |
| Physical complications | Hypogonadism | 4 | 1.9 |
| Physical complications | Hepato-splenomegaly | 3 | 1.4 |
| Physical complications | Hepatocellular carcinoma | 2 | 0.9 |
| Economic burden on the family | Yes | 54 | 25.5 |
| Economic burden on the family | No | 157 | 74.5 |
Table 1: Socio-demographic and clinical characteristics of the sample (n=214).
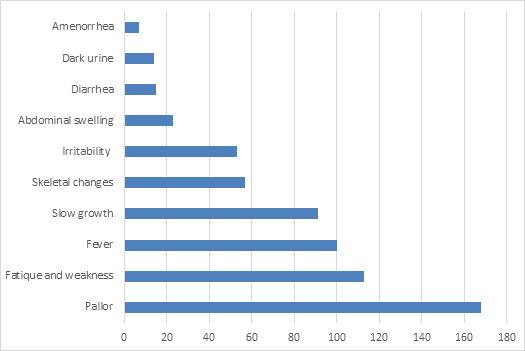
Figure 1 shows that the most common symptom that brought the patient to the hospital was pallor (78.5%), followed by fatigue (52.8%), fever (46.7%%), and slow growth (42.5%), more than 46% reported needing blood transfusion 15 times or more per year. (Figure 2) The trend of Thalassemia in Iraq for the last five years is demonstrated in Figure 3.
| Item | Cost/unit ($) | Frequency/year | Total cost /year ($) |
|---|---|---|---|
| Bed occupancy/day | 15 | 48 | 720 |
| Lab. Tests: C.B.C | 11 | 48 | 528 |
| HIV | 6 | 3 | 18 |
| HCV | 4 | 3 | 12 |
| A.S.T | 4 | 3 | 12 |
| A.L.T | 4 | 3 | 12 |
| S. Ferritin | 4 | 3 | 12 |
| HB electrophoresis | 20 | 1 | 20 |
| Blood transfusion | 88 | 15 | 1320 |
| Treatment | |||
| Folic acid | 0.2 | 365 | 73 |
| Calcium carbonate tab. | 0.4 | 365 | 146 |
| One alpha | 1.2 | 365 | 438 |
| Desferal | 4.8 | 720 | 3504 |
| Sub-total | 6815 | ||
| Indirect health care services | 3995 | ||
| Total (for a single patient) | 10810 | ||
| Total estimate for all patients | 10810* 13390 | 144,746,000 |
Table 2: Economic burden on the health system.
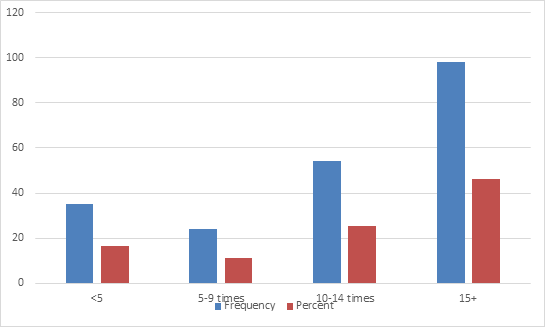
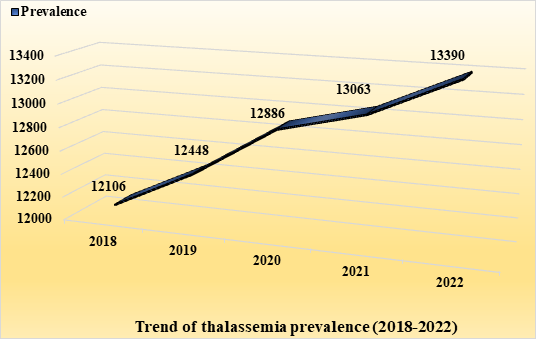
Table 2 illustrates that the estimated annual cost of health care regarding diagnosis, treatment, blood transfusions and other direct medical services for each single thalassemia patient was $6815. After calculating the expenses related to the indirect health care services (nursing, laboratory services, hospitalization, transportation, and food), we concluded that the total annual cost of such services equals to $3995, and when adding this to the direct medical cost, the estimated total amount spent for each thalassemia patient per year was shown to be $10810. Multiply this number by the total number of patients (prevalence), gave an overall annual cost of $144,745,900.
Discussion
Chronic non-communicable diseases form the main burden on the Iraqi health system [11]. Thalassemia is one of these diseases that needs, in addition to investigations, medicines, and follow up, repeated blood transfusions, causing more burden on the already exhausted health system [12].
The results of the current study showed that the mean age of the respondents was 14.5 year, and a female to male ratio of 1.8:1, with a high rate of consanguinity among parents. This is comparable to a previous study in Iraq, which concluded that the mean age is 13 years, and the female to male ratio is 1.2:1 [13]. With respect to the age at diagnosis; 73. 4% of the patients were diagnosed before completing their second year of age. The Saudi Arabian guideline stated that the symptoms usually appear during the first two years of life [4].
Anemia was the chief complaint in more than three quarters of the patients, while slow growth (short stature) was seen in 42.5%, and skeletal changes in 26.6%. A previous study in Iraq showed that short stature was found in 33.9% of those aged ≤ 20 years, and skeletal changes were seen in 50.7% [13]. In India; about 40 % presented with severe anemia (a hemoglobin level of 5.0 gm/dl) [14].
In the present study, the main complications were chronic hepatitis and heart failure, while hypothyroidism and hypogonadism were detected in few patients. Previous studies in Iraq revealed that at least 55.9% of the surveyed patients had one complication, while Iron overload associated complications, including hypogonadism, hypothyroidism, hypoparathyroidism, and heart failure, were seen in more than half of the patients [9, 13]. More complications result in more medical interference, leading to an increase in the cost, and causing more burden.
The trend of thalassemia for the last five years shows a clear up slop; although not much, but there is an increase in the number of cases each year which adds more burden on the health system. This goes with the findings of a previous national study [9].
The results revealed that the average blood transfusions for each patient was 15 per year. This is comparable to the findings of studies from other countries [15, 16, 17]. However, the increased number of blood transfusions with increasing age can be an important factor in increasing the burden, moreover, patients with more complications need more blood transfusion which adds to the direct medical cost.
The findings confirmed that the rough estimate of the annual cost for each single patient was about $10,810. When this is multiplied by the total number of patients, then the total cost will be around $145 million. This is apart from other (invisible costs) such as: reception, building, cleaning, and other logistic services). These expenses are adding more burden on the health system, in which the health investment is already directed towards the secondary and tertiary care more than the primary health care. This estimate is lower than that recorded in Italy (EUR 31,883) [15] and United States ($ 43,969 and $ 128,969) [18], but higher than that found in studies conducted in India ($1135) [18], and Iran (EUR 1,731) [19]. A study in Iran revealed that the average cost estimate per patient per year was $ 8321.8 apart from the cost of lost welfare, of this amount, $ 7286.8 was related to direct medical costs, $ 461.4 to direct non-medical costs, and $ 573.5 to indirect costs [20], while a study in Dubai concluded that the mean annual direct medical cost was estimated at $ 35,713, with the annual direct non-medical costs being $ 605 [21].
The highest portion of the cost is related to the large amount of medicines that the patient has to take continuously for the whole year (especially iron chelating therapy), and blood transfusion which can reach up to twenty times per year. Deferasirox (considering its high price) is associated with the highest percentage change in the total direct medical costs. A study in Dubai, United Arab Emirates revealed that the main driver of the medical cost for the participants was iron chelation therapy followed by blood transfusions [21].
It is important to note that most of the health care services for thalassemia in Iraq are almost free, which means that the cost is afforded by the health facilities, and so, the main burden will be on the governmental health expenditure, however, more than a quarter of the sampled families reported that (in addition to the physical and social burden), they are suffering a significant economic burden due to the frequent shortages of medicines (especially iron chelating agents), this urges the families to buy these (relatively expensive medicines) out of their pockets causing more economic burden on them, especially that most of those families are among the low socio-economic stratum, and when this is covered by the health facilities, this will be backfired on the health system resulting in failure to provide essential medicines in the long run, particularly iron chelating therapy, and this will be negatively reflected on the patients, causing more complications, such as iron overload, not mentioning the effect on the national economy due to the repeated sick leaves, absenteeism from work, and premature death. This is in addition to the psychological and social sequels that add more burden on the patients.
Conclusion
The annual cost for thalassemia patients in Iraq is relatively high, most of which is covered by the Ministry of Health and its institutions. This causes a burden on the health system. Adopting new policies to reduce the costs especially through finding substitutes (or less costly therapy) for blood chelating agents, is crucial on the long term strategy.
- Financial Support and Sponsorship: Nil
- Conflicts of Interest: There are no conflicts of interest.
References
-
Modell B, Darlison M (2008) Global epidemiology of haemoglobin disorders and derived service indicators. Bull World Health Organ 86(6): 480-487.
-
Weatherall DJ (2018) The Evolving Spectrum of the Epidemiology of Thalassemia. Hematology/ Oncology Clinics North Am 32(2): 165-175.
-
(2022) Saudi Arabian guidelines, Saudi MoH.
-
Angastiniotis M, Vives Corrons JL, Soteriades ES, Eleftheriou A (2013) The impact of migrations on the health services of Europe: the example of haemoglobin disorders Scientific World Journal 2013: 727905.
-
Abu-Shaheen A, Heena H, Nofal A, Abdelmoety D, Almatary A, et al. (2020) Epidemiology of Thalassemia in Gulf Cooperation Council Countries: A Systematic Review. BioMed Research International 2020: 1509501.
-
Memish ZA, Saeedi MY (2011) Six-year outcome of the national premarital screening and genetic counseling program for sickle cell disease and β-thalassemia in Saudi Arabia. Ann Saudi Med 31(3):229-235.
-
Al-Riyami A, Ebrahim GJ (2003) Genetic blood disorders survey in the Sultanate of Oman. J Trop Pediatr 49: i1-20.
-
(2021) Iraqi Ministry of Health Report.
-
Kadhim AK, Baldawi KH, Lami FH (2017) Prevalence, Incidence, Trend, and Complications of Thalassemia in Iraq. Hemoglobin international journal 41(3): 164-168.
-
Majid M, Mutar TM, Hashim TH (2020) Thalassemia awareness among Iraqi people in 2018 Baghdad, Iraq. Baghdad College of Medicine. Thalassemia Reports 10(1): 8655.
-
Hussain AM, Lafta RK (2019) Burden of non- communicable diseases in Iraq after the 2003 war. Saudi Medical Journal 40(1):72-78.
-
Lafta RK, Al-Nuaimi AM (2019) War or health, a four decade armed conflict in Iraq. Medicine Conflict and Survival 35(3): 209-226.
-
Sadullah RK, Sulav DA, Al-Allawi NA (2020) Complications and Challenges in the Management of Iraqi Patients with β-Thalassemia Major: A Single-center Experience. Oman Medical Journal 35(4): e152.
-
Trehan A, Sharma N, Das R, Bansal D, Marwaha RK (2015) Clinicoinvestigational and Demographic Profile of Children with Thalassemia Major. Indian J Hematol Blood Transfus 31(1):121–126.
-
Angelucci E, Antmen A, Losi S, Burrows N, Bartiromo C, et al. (2017) Direct Medical Care Costs Associated with β-Thalassemia Care in Turkey. Blood 130: 2094.
-
Weiss M, Jun MP, Sheth S (2019) Clinical and economic burden of regularly transfused adult patients with β-thalassemia in the United States: A retrospective cohort study using payer claims. Am J Hematol 94(5): E129-E132.
-
Safdar S, Mirbahar A, Sheikh MA, Taseer IUH, Mustafa A, et al. (2017) Economic Burden of Thalassemia on Parents of Thalassemic Children A Multi-Centre Study. Pak J Med Res 56(3): 68-72.
-
Moirangthem A, Phadke SR (2018) Socio-demographic Profile and Economic Burden of Treatment of Transfusion Dependent Thalassemia. Indian journal of pediatrics 85(2): 102-107.
-
Sattari M, Sheykhi D, Nikanfar A, Pourfeizi AH, Nazari M, et al. (2012) The financial and social impact of thalassemia and its treatment in Iran. Pharm sci 18(3): 171-176.
-
Esmaeilzadeh F, Azarkeivan A, Emamgholipour S, Sari AA, Yaseri M, et al. (2016) Economic Burden of Thalassemia Major in Iran, 2015. JRHS 16(3): 111-115.
-
Alshamsi S, Hamidi S Narci HO (2022) Healthcare resource utilization and direct costs of transfusion- dependent thalassemia patients in Dubai, United Arab Emirates: a retrospective cost-of-illness study. BMC Health Services Research 22(1): 304.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines