Effective Anti-Fogging Agent for Glasses and Face Shields in the Treatment of Ebola in Uganda: Implications for Healthcare Worker Safety and Patient Care
Evidence on the effective Antifogging Agents (AFA) for use during Donning of goggles and face shields in Ebola Treatment Centres (ETC) is lacking. This study aimed at establishing an effective antifogging agent, the side effects of fogging, and the impact of fogging. It was a cross-sectional study conducted from 26 September to 08 October 2022 in Fort Portal Regional Referral Hospital Ebola Treatment Centre in which 21 Health Care Workers (HCWs) managing Ebola patients were recruited. All were healthy no signs or symptoms. AFA used were Liquid Soap & Alcohol 80%. The Control was Standard of Care. As they donned goggles the time taken to fog was noted, side effects and impact were all noted for each HCW after they had doffed off their Personal Protective Equipment (PPE). AFA was significant if P < 0.05 with a 95% Confidence Interval. Study findings; 66.7% of those that used liquid soap never fogged after 4 hours in PPE with p <0.001, The participants who used Alcohol all fogged 30 minutes after donning with p=0.030, and on the standard of care all of them fogged within 21 minutes of donning PPE with p=0.552. In this study over 90% who fogged could not see and stopped working. Of those who fogged 43 % developed dizziness and 53% developed headache. This study has demonstrated liquid soap is a superior AFA and thus increased the time the health care workers spend attending to critically ill Ebola patients and it reduces chances of infection among health care workers resulting from fogging of goggles. This study recommends WHO and MoH to include in their IPC guidelines the use of liquid soap as an antifogging agent for the goggles and face shields during donning in order to improve the level of care in the Isolation Treatment Centres.
David Francis Olebo1*, Gerald Kanyomozi2, Jacqueline Nalikka3 and Moses Asiimwe4
PCR: Polymerase Chain Reaction; MoH: Ministry of Health; MUWRP: Makerere University Walter Reed Project; IDI: Infectious Diseases Institute; WHO: World Health Organization; COR: Correlation; AOR: Adjusted Odds Ratio.
Introduction
Ebola patients are highly infectious and end up being critically ill requiring the need for intensive clinical care in the isolation treatment Centres. This has made frontline healthcare workers to be at risk of aerosol exposure and infection during their care. Therefore, the use of effective personal protective equipment (PPE) is paramount and the World Health Organization (WHO) recommended the use of; masks, gloves, coveralls, face shields, aprons, and face shields in their management [1, 2]. Eye protection for procedures with a reasonable probability of infection/injury is paramount. Eye protection (goggles) and face shields are made of plastic material and play an important role in preventing exposure of eyes to aerosols and pathogens and serve as an important barrier to breaking the chain of infection [3]. Despite the use of protective Goggles and Face shields (GFS), health workers have continued to fog and in the Ebola outbreak in West Africa, healthcare workers were 21 to 32 times more likely to be infected with Ebola than the general population [4] and by the time the outbreak was over Guinea had lost all in total; Doctors, Nurses and Midwives 5317, Liberia 946 and Sierra Leone had lost 1074. This would be attributed to a large number of patients they had to attend and the PPE like googles and face shields could fog within a short time posing a risk of exposure to the health workers who ended up contracting and dying of Ebola as they tried to save the patients Evans DK, et al. [5] in a systematic review on 94 articles related to 22 outbreaks published before 27 December 2017, the health care workers infections to Ebola was 0.6% to 92%. It was consistent throughout the outbreaks and the health worker’s exposure would be attributed to Fogging of their google [6]. However, the WHO updated guidelines on use of protective goggles and face shields emphasized the role of eye protection for healthcare workers involved in the management of patients with highly infectious diseases like Ebola but the guidelines do not highlight need for use of antifogging agents on the goggles or face shields [7]. In the recent Ebola pandemic in Uganda with high morbidity of critically ill Ebola patients overwhelmed the healthcare teams managing cases requiring more contact time for the healthcare workers to attend to the patients yet putting on PPE like goggles and face shields shields recommended by WHO fog in the short time, limiting the work of the health care workers in the overwhelming Ebola Treatment Centres with critically ill patients. Fogging hinders effective patient care hence increased mortality out come on the patients, and impaired vision with increased risk of failure to carry out aerosol generating procedures and contracting the infection. Fogging has been due to improper fitting mask, which redirects the warm exhaled gases upward instead of forward. This warm water vapor in exhaled breath condenses on the relatively cold lenses of the goggles and causes fogging [8]. This observational study therefore was seeking to establish an effective antifogging agent, side effects associated with fogging, and impact of fogging to patient’s health outcome in the Ebola treatment Centres with the over whole aim of coming up with an effective antifogging agent to be used to improve the time health care workers spend attending to critically ill Ebola Patients which was achieved.
Materials and Methods
Study Location
The study was conducted at Fort Portal Regional Referral Hospital, situated in Fort Portal Tourism City, Uganda. This hospital encompasses various specialized units, including the Isolation Unit (Ebola Treatment Centre), Mental Unit, Imaging Unit, Paediatrics Department, Medical Department, Surgical Department, Obstetrics and Gynaecological Department, Outpatient Department, and the Laboratory Department.
Fort Portal Regional Referral Hospital serves as a vital healthcare institution, offering both inpatient and outpatient services to residents from 11 districts in the southwestern part of Uganda. These districts include Kyenjojo, Kagadi, Kamwenge, Kibaale, Kasese, Bundibugyo, Kabarole, Kyegegwa, Ntoroko, Bunyangabu, and Kitagewenda. The hospital is staffed by a diverse range of healthcare professionals, including paediatricians, physicians, surgeons, gynaecologists, psychiatrists, pharmacists, medical doctors, clinical officers, anaesthetists, physiotherapists, nutritionists, laboratory technologists, nurses, and midwives, totaling 430 healthcare workers. With a bed capacity of 333 beds, Fort Portal Regional Referral Hospital plays a crucial role in providing healthcare services to the local community.
Geographically, Fort Portal Regional Referral Hospital is situated within the city of Fort Portal, approximately 148 kilometers (92 miles) west of Mubende Regional Referral Hospital by road. Furthermore, it is approximately 294 kilometers (183 miles) west of Mulago National Referral Hospital, which is located in Kampala, Uganda’s capital and largest city
Study Design and Setting
It was an Observational cross-sectional study conducted from 26 September to 08 October 2022. This study applied descriptive and analytical quantitative approaches. The observational study was conducted in Fort Portal Regional Referral Hospital Ebola Treatment Centre (FPRRH-ETC) one of the Centres that was involved in the management of Ebola infected patients in Uganda that was declared an epidemic on 26 September 2022.
The Study Population
The hospital employs a total of 430 healthcare workers. However, 30 of them have received specialized training and were assigned to work exclusively in the Isolation Unit, specifically designed for managing Ebola patients at Fort Portal Regional Referral Hospital (FPRRH-ETC). Consequently, our observations were carried out on 21 out of these 30 healthcare workers who were responsible for the care of Ebola patients.
It is essential to highlight that all of these healthcare workers were in excellent health, displaying no signs or symptoms of illness. Importantly, no unwell or unhealthy healthcare worker was allowed access to the Ebola Treatment Centre (ETC).
Within the ETC, healthcare workers operated in 12-hour shifts, providing a comprehensive range of services, including physical assessments, history taking, vital signs monitoring, point-of-care ultrasound scans, fluid monitoring, medication administration, nasogastric tube insertion, phlebotomy, bed baths, oral care, blood transfusions, and changing diapers in cases of profuse diarrhea. They were also responsible for laundering patient linens, cannulation, urine sample collection, turning critically ill patients every two hours, maintaining cleanliness in patient environments, offering psychosocial support, managing waste, handling deceased bodies and cleaning of the Green Zone environment.
In addition to these clinical duties, the healthcare workers in the ETC conducted various laboratory tests, such as urinalysis, Malaria Rapid Diagnostic Tests (MRDT), blood gases analysis, Complete Blood Count (CBC), chemistries, Random Blood Sugar (RBS) testing, viral load assessments, pregnancy tests, and blood group determinations with cross- matching.
Description of the Interventions
1. Liquid Soap: composed of; Cocamidopropyl betaine, Methyllisothiazolinone (MIT) and Methylchoroisothiazolinone (CMIT), Sodium laureth sulfate, sodium benzoate and benzoic acid, sodium chloride, citric acid cocodietanolamide and Gliserin. In many cases, this has been used for hand washing and it’s reported to form a thick film on the plastic or glass surface and reduces surface tension; this reduced surface tension causes rapid spread of condensed droplets over the whole coated surface, thus clearing vision hence preventing fogging [9]. The concentrated liquid soap general purpose synthetic organic Liquid Detergent Advanced formula lemon dash was used manufactured by Mukwano industries Uganda limited.
2. Alcohol 80%: Alcohol-based: antifogging action forms a thin film on the plastic or glass surface and reduces surface tension; this reduced surface tension causes rapid spread of condensed droplets over the whole coated surface, thus clearing vision and prevents fogging from occurring [10]. The alcohol concentration of 80% was used for the alcohol intervention. The alcohol had 80% ethanol with the following ingredients; Hydrogen Peroxide, Glycerol and Purified water.
Data Collection Technique and Study Procedures
The study utilized a semi-structured questionnaire administered to each participant after they had doffed their PPE. Each participant was assessed using the tool three times: once after applying Liquid Soap, once after applying Alcohol 80%, and once without applying any antifogging agent.
The questionnaire covered key areas, including the duration taken to experience fogging, the expected time to complete the task, and any side effects reported after fogging or any side effects reported by those that did not fog and overall impact.
Study Procedure Intervention 1: Liquid Soap Antifogging Agent
During donning of Personal Protective Equipment (PPE) to go and care for the patients in the Hot zone (Red Zone) the 21 healthcare workers applied a thick layer of concentrated liquid soap on their goggles and left them for 2-5 minutes to air dry before donning on them. The time taken to fog was noted, they were requested to report any side effects they would get after fogging or without fogging and they were also requested to exit the red zone as soon as possible when they fog.
Study Procedures Intervention 2: Alcohol 80% Antifogging Agent
During donning of Personal Protective Equipment (PPE) to go and care for the patients who were suspects but Polymerase chain reaction (PCR) test was negative for Ebola. The same 21 health care workers applied a thin layer of alcohol 80% on their goggles and left them for 2-5 minutes to air dry before donning on them as they when to care for patients whose PCR Test was negative. The time taken to fog was noted, they were requested to report any side effects they would get after fogging or without fogging and they were also requested to exit the patient ward as soon as possible when they fog. This intervention was only implemented for 72 hours on suspect ward that had patients with negative PCR Test for Ebola Sudan Virus Disease. After 72 hours we stopped using the intervention because it had showed to be less effective.
Control: Standard of Care without use of any Antifogging Agent
Since both WHO and MoH Uganda guidelines do not have the guide to use antifogging agents during donning of the goggles and face shields when taking care of the patients in the hot zone, 21 Health care workers donned goggles in the Green Zone (safe Zone) as they did clean of the surfaces, time taken to fog was noted. They were requested to report any side effects they would get after fogging or without fogging. Each participant experimented this once only.
Sample Size and Sampling Technique
This study included 21 healthcare workers out of the 30 healthcare workers involved in patient care in the ETC, all of whom were healthy and had provided their consent. We employed a purposive sampling technique because they were the only highly trained in IPC that had been approved to manage the Ebola patients in the ETC.
Ethical Consideration and Quality Control
Since at the time of the outbreak the IPC guidelines did not have antifogging agents for health care workers to apply on their googles and Face Shields as they Donned to go and take care of the patients, we obtained clearance from FPRRH to allow the use of the liquid soap and alcohol 80% to safe guard the health care workers and only liquid soap was used for Donning when entering into the red zone since preliminary data was promising. All the participants gave informed consent and participation was voluntary. The quality control was done; pre-testing of the tool, ensuring reliability and validity of the tool.
Data Analysis
The study considered 30 Health Care Workers who were working in the ETC but 21 consented to take part in the study at the time of the outbreak. Data Analysis the study used SPSS version 20 for the analysis of the data. Logistic regression analysis; bivariate and multivariate with (Pearson correlation, odds ratios and P Values) was used to measure associations. The confidence level was set at 5% in which probability of effectiveness being significant if P < 0.05 with 95% Confidence Interval.
Results
Demographic Characteristics
Table 1 shows 21 out of 30 health care workers took part in the study from FPRRH-ETC a majority; 47% of the participants were 20-30 years old, 57.1% were females, 42.9% had university bachelor’s degree, and 33.3% were Nurses while 71.4% of them had 1-2 years’ experience in working in the isolation units. We also found out that FPRRH-ETC had 12-hour shifts; day duty and night duty with majority 42.9% of them donning 3 to 4 times in the shift and 28.6% of them donned 5 to 6 times in the shift. The study highlights that health workers were educated, with a lot of experience in managing highly infectious diseases but overwhelmed with work in that they had to don up to 6 times in a single shift.
| Demographic characteristics | Frequency | Percentage (%) | |
|---|---|---|---|
| Age in years | |||
| 20-30 | 10 | 47% | |
| 31-41 | 8 | 38.10% | |
| 42-52 | 3 | 14.30% | |
| Sex | |||
| Male | 9 | 42.90% | |
| Female | 12 | 57.10% | |
| Education Level | |||
| University with Bachelor | 9 | 42.90% | |
| Tertiary with certificate | 4 | 19.00% | |
| Tertiary with Diploma | 6 | 28.60% | |
| University with Masters | 2 | 9.50% | |
| Cadres | |||
| Nurse | 7 | 33.30% | |
| Medical Officers | 3 | 14.30% | |
| Clinical Officers | 2 | 9.50% | |
| Hygienist | 2 | 9.50% | |
| Social Worker | 2 | 9.50% | |
| Lab Technologist | 1 | 4.80% | |
| Physician | 2 | 9.50% | |
| Midwife | 2 | 9.50% | |
| Experience in Isolation Unit | |||
| <1 year | 1 | 4.80% | |
| 1-2 years | 15 | 71.40% | |
| 3-4 years | 5 | 23.80% | |
| Number of times donned in a shift | |||
| 1-2 | 6 | 28.60% | |
| 3-4 | 9 | 42.90% | |
| 5-6 | 6 | 28.60% | |
Table 1: ** Demographic characteristics of the participants (n=21).
Source: Primary field data 2022. Table 1: Demographic characteristics of the participants (n=21).
Effectiveness of Antifogging Agents
The Table 2 demonstrates the effectiveness of antifogging agents. Among participants who applied liquid soap to their glasses and experienced no fogging, 66.7% of them were expected to spend 1-2 hours and 3-4 hours in the red zone, with each group accounting for 33.35%. Those who fogged after 4 hours constituted 9.5% and were expected to spend 3-4 hours performing tasks. Additionally, those who fogged after 3 hours comprised 9.5%, with 4.75% of them expected to spend 1-2 hours and 3-4 hours, respectively. Finally, 14.3% experienced fogging after 2 hours, and all of them were expected to spend 1-2 hours performing their tasks. These results were statistically significant, indicating a positive correlation (COR 0.836; AOR 0.223; P < 0.001). These was in line with the study conducted on sulfonated polymer-coated eyewear in which those that did not use coated eyewear fogged their duration was 2 hours Keschner YG, et al. [11] and antifogging comparison study [12].
For Participants who applied alcohol 80% concentration. Among those who fogged within 1-20 minutes, 76.2% of them were expected to take 1-2 hours to complete their tasks, and 42.85% were expected to spend 3-4 hours on assigned tasks. Among those who fogged within 21-40 minutes, accounting for 23.8%, 19% were expected to take 1-2 hours to complete their tasks, and 4.8% were expected to spend 3-4 hours. This result was statistically significant, indicating a negative correlation (COR -0.475; AOR 0.048; P 0.030). These was in line with the study that compared the antifogging agents [9, 12].
For participants who did not apply any antifogging agent, the majority (95.2%) experienced fogging within 1-20 minutes. Among them, 47.6% were expected to take 1-2 hours to complete their tasks, and the same proportion (47.6%) was expected to spend 3-4 hours on their tasks. A minority experienced fogging within 21-40 minutes, and all of them were expected to take 1-2 hours to complete their tasks. This result was not statistically significant and showed a negative correlation (COR -0.138; AOR -0.005; P 0.552). These was in line with the study conducted on anti-fog polymer coating [9, 11, 12].
| Antifogging Agents | Expected Time for the Tasks | Bivariate | Multivariate | |||
|---|---|---|---|---|---|---|
| 1-2 Hours | 3-4 Hours | Total | COR | AOR | P Value | |
| Duration to Fog with Liquid Soap | 0.836 | 0.223 | <0.001 | |||
| Never Fogged | 7 (33.35%) | 7 (33.35%) | 14 (66.7%) | |||
| 4 Hours | 0 | 2 (9.50%) | 2 (9.5%) | |||
| 3 Hours | 1(4.75%) | 1(4.75%) | 2 (9.5%) | |||
| 2 Hours | 3 (14.30%) | 0 | 3 (14.3%) | |||
| 21 (100%) | ||||||
| Duration to Fog with Alcohol 80% | -0.475 | 0.048 | 0.03 | |||
| 1-20 Minutes | 7 (33.35%) | 9 (42.85%) | 16 (76.2%) | |||
| 21-40 Minutes | 4 (19.00%) | 1 (4.80%) | 5 (23.80%) | |||
| 21 (100%) | ||||||
| Duration to Fog with No Antifogging Agent | -0.138 | -0.01 | 0.552 | |||
| 1-20 Minutes | 10 (47.60%) | 10(47.60%) | 20 (95.2%) | |||
| 21-40 Minutes | 1(4.8%) | 0 | 1 (4.8%) | |||
| 21 (100%) |
Table 2: ** Level of Effectiveness of Antifogging Agents (n=21).
Source: Primary field data 2022 Table 2: Level of Effectiveness of Antifogging Agents (n=21).
Impact of Fogging
The Figure 1 shows over 90% of the participants who fogged could not see and stopped working that had a negative impact on their work (ref-figure 1). Fogging puts the HCWs at risk of falling hence fractures [13, 14].
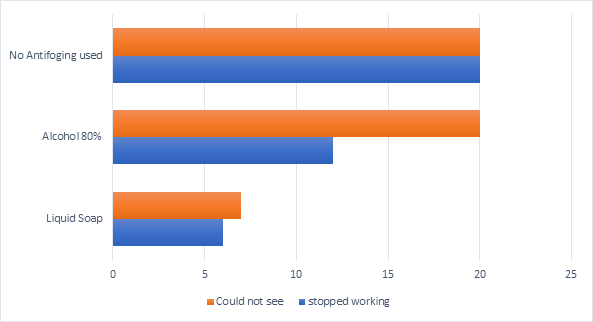
Source: Primary field data 2022. Figure 1: Impact of Fogging to Patients Care in ETC (n=21).
Side Effects of Fogging
The Figure 2 shows reported side effects that were specific to only health care workers who fogged with 53% of them reporting headache, 43% reporting dizziness and only 4% reporting anxiety. These would be attributed to low oxygen circulation in the brain resulting from fogging and it was in line with the study that assessed the physiological effects of PPE among healthcare workers [14, 15, 16, 17].
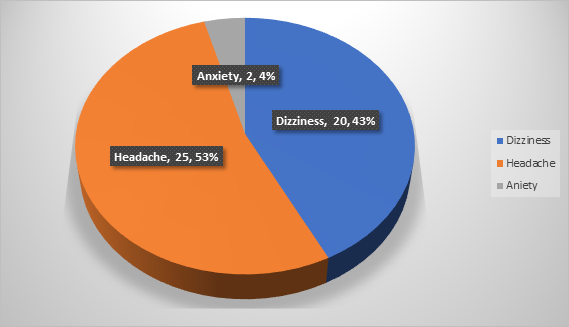
Source: Field Data 2022. Figure 2: Reported Side Effects that were Specific to Health care workers who fogged (N=42).
Discussion
Eye protection has been established as an essential and mandatory component of personal protection for health care workers attending to patients with highly contagious infections in high containment areas such as the Ebola treatment Centres [18]. The risk of transmission of Ebola virus disease among health workers is so high due to the nature of activities in an ETC and the infectiveness of the Ebola virus. However, fogging of eye shields and goggles remains a challenge and poses additional risks to health workers. Fogging obstructs clear vision for the health care worker to perform tasks in an ETC, and the need to adjust the goggles to restore vision is one of the most risky manoeuvres that can lead to potential transmission of the Ebola virus [19].
This study aimed to determine a more effective antifogging agent to be used by health care workers who are taking care of patients with highly contagious infections such as Ebola virus disease. The study also sought to establish the side effects of fogging and the impact of fogging on clinical care of patients in an ETC.
Results of this study show that the use of surfactant- based solutions in form of liquid soap offered superior benefits to health care workers in Ebola treatment Centres. The use of liquid soap delayed fogging and thus increased the time spent in an ETC for each health care worker. This was of particular benefit to the treatment teams who were usually stretched in terms of human resource capacity, and reduced the number of dangerous incidents among health care workers. This finding is in line with a study conducted by T. Varshney and others who found out that washing soap application on goggles and face shields offered antifogging properties for up to six hours [9].
The fogging of eye goggles and face shields reduced the ability to provide critical care needed by the patients. This is because of reduced vision that was experienced by health care workers who fogged. Saskia Den Boon and colleagues noted that impaired visibility was a challenge to health care workers, particularly those who used goggles. These was inline with a study that used washing soap [20].
Conclusions
Despite the small number of worker studies, Liquid Soap is a superior and effective antifogging agent for use in the isolation Treatment Centres more so in the resource limited setting. Health Care Workers who did not use liquid soap, most of them spent less time performing their tasks. The side effects associated with fogging were headache and dizziness. No health care Ebola infections were registered in our Ebola Treatment Centre and all the Health care workers who took care of Ebola patients applied liquid soap on their glasses and were able to complete all their tasks in ETC with most of them not fogging. This study recommends WHO and MoH to include in their IPC guidelines the use of liquid soap as antifogging agent for the glasses and face shields during donning in order to improve level of care and health care worker safety in the Isolation Centres.
Acknowledgement
We acknowledge the dedication and resilience of healthcare workers at Fort Portal Regional Referral Hospital Ebola Treatment Centre. Our gratitude also goes to the Ministry of Health (MOH) Uganda, particularly recognizing the Clinical Care sub-pillar at the National task Force. Additionally, we acknowledge MUWRP and IDI Management. We also extend our heartfelt thanks to well-wishers and friends for their support and contributions in the control of the outbreak.
Funding
This work was funded by the authors themselves and no external individual or organization funded it.
Competing Interests
The authors do not have any conflict of interest in this research.
Ethics Approval
The research work was approved by Fort Portal Regional Referral Hospital Management and informed consent from the participants.
Data Availability Statement
All the relevant data in this study have been analyzed and reported in the article but data set can be availed on request.
Supplemental Material
Not Applicable.
References
-
Wax RS, Christian MD (2020) Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Canadian Journal of Anesthesia/Journal canadien d’anesthésie 67(5): 568-576.
-
WHO (2020) Infection prevention and control during health care when COVID-19 is suspected: interim guidance.
-
Li J-PO, Lam DSC, Chen Y, Ting DSW (2020) Novel Coronavirus disease 2019 (COVID-19): The importance of recognising possible early ocular manifestation and using protective eyewear. Br J Ophthalmol 104(3): 297- 298.
-
WHO (2015) Health Worker Ebola Infections in Guinea, Liberia and Sierra Leone.
-
Evans DK, Goldstein M, Popova A (2015) Health-care worker mortality and the legacy of the Ebola epidemic. The Lancet Global Health 3(8): e439-e440.
-
Selvaraj SA, Lee KE, Harrell M, Ivanov I, Allegranzi B (2018) Infection Rates and Risk Factors for Infection Among Health Workers During Ebola and Marburg Virus Outbreaks: A Systematic Review. The Journal of Infectious Diseases 218: S679-S689.
-
Sayburn A (2020) Covid-19: PHE upgrades PPE advice for all patient contacts with risk of infection. British Medical Journal Publishing Group.
-
Pandey K, Vig S, Ratre B, Gupta N (2020) Use of sterillium on protective goggles for antifogging during donning for care of COVID-19 patients: A novel technique. Turk J Anaesthesiol Reanim 48(4): 344-345.
-
Varshney T, Dudani P, Bardoloi P (2021) Comparative analysis of antifogging agents and their combination for protective eyewear in COVID-19 intensive care units. Indian Journal of Ophthalmology 69(12): 3796-3797.
-
Pandey K, Vig S, Ratre B, Gupta N (2020) Use of Sterillium on Protective Goggles for Antifogging during Donning for Care of COVID-19 Patients: A Novel Technique. Turk J Anaesthesiol Reanim 48(4): 344-345.
-
Keschner YG, Raja AS, Margolin JD, Zheng H, Olson KR (2023) Effectiveness of an anti-fog polymer coating in protective eyewear: a blinded, randomised controlled cross-over trial with healthcare providers in an emergency department setting. BMJ Innovations 9(3).
-
Agarwal P, Sharma D (2021) How to prevent fogging of spectacle glasses when wearing a face mask. Indian Journal of Surgery 83(6):1609-1610.
-
Dankert JF, Virk MS (2021) Mask-related glasses fogging: a predisposing mechanism of falls during the CoViD-19 pandemic. Case reports in orthopedics.
-
Vaidiyanathan B, Amalanathan S, Chokalingam S, Colbert K, Joseph I, et al. (2023) The burden of personal protective equipment and its effect on the work efficiency in health- care workers. Journal of Clinical Sciences 20(1): 30-34.
-
Choudhury A, Singh M, Khurana DK, Mustafi SM, Ganapathy U, Kumar A, et al. (2024) Physiological effects of N95 FFP and PPE in healthcare workers in COVID intensive care unit: A prospective cohort study. Indian journal of critical care medicine 24(12):1169-1173.
-
Jose S, Cyriac MC, Dhandapani M (2021) Health problems and skin damages caused by personal protective equipment: experience of frontline nurses caring for critical COVID-19 patients in intensive care units. Indian journal of critical care medicine 25(2):134.
-
Laxmidhar R, Desai C, Patel P, Laxmidhar F, Laxmidhar RM (2023) Adverse Effects Faced by Healthcare Workers While Using Personal Protective Equipment During the COVID-19 Pandemic in Civil Hospital, Ahmedabad. Cureus 15(5): e38485.
-
WHO (2015) Health worker Ebola infections in Guinea, Liberia and Sierra Leone.
-
Ramamoorthy KG (2020) Antifogging techniques as part of personal protective equipment (PPE). Indian Journal of Anaesthesia 64(12):1085-1086.
-
Den Boon S, Vallenas C, Ferri M, Norris SL (2018) Incorporating health workers’ perspectives into a WHO guideline on personal protective equipment developed during an Ebola virus disease outbreak. F1000Research 7: 45.
- Measuring What Matters: Data Gaps, Certificate of Need Reform, and Pediatric Psychiatric Inpatient Capacity in North Carolina
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal