One Health Implication of Leptospirosis in Ethiopia: A Review
Leptospirosis is a globally important zoonotic disease caused by the pathogenic Gram-negative bacteria of the genus Leptospira. The disease occurs in nearly all mammalian species and it is more common in the tropical regions because of the longer survival organism in the environment. In contaminated environment frequent exposure to animals and humans indicate one health approaches. It caused by numerous serovars of leptospira interrogans that belong to the genus Leptospira. Leptospira interrogans is not the only serovar that resembles the disease, which affects almost all mammalian species. The primary reservoir animals are known as rats and mice. Direct human transmission through exposed mucosal membranes and damaged skin to the urine of infected animals. The laboratory testing on various animal species do not significantly alter the clinical indications of leptospirosis. The best control for the disease are vaccination, quarantine, and rodent management. Tropical regions with warm, humid weather and alkaline or neutral soil are better suited for leptospira survival. Applying effective control measures and raising public awareness of leptospirosis zoonotic transmission is recommended. Concerned body should involve in supporting the study of the leptospirosis situation in deprived nations, such as Ethiopia.
Abbreviation
WHO: World Health Organization; ELISA: Enzyme Linked Immune Sorbent Assay; PCR: Polymerase Chain Reaction; MAT: Microscopic Agglutination Test; DCP: Disease Control and Prevention; IgM: Immunoglobulin M; IgG: Immunoglobulin G; CSF: Cerebrospinal Fluid.
Introduction
Leptospirosis is a reemerging bacterial disease and one of the most common zoonosis in the world. It causes severe illness in animals and humans and caused by pathogenic species of spirochetes of the genus Leptospira that thrive directly within hosts and reservoirs (such as rodents), and indirectly within the environment [1]. In many tropical and subtropical areas, leptospirosis is an endemic disease. Leptospirosis causes more than 60,000 fatalities in humans each year, and it is estimated that about one million people are infected [2].
Leptospirosis acute infectious sickness with enlargement of spleen, jaundice, and nephritis. The first distinct visual observation of Leptospira was made in 1907 by Stimson from sliced human post-mortem renal tissue, and its presence in rats was recorded in 1916. Leptospirosis were first isolated in pure culture by Japanese investigators in 1914 [3]. Rats is the primary source of leptospirosis in urban areas because of inadequate sanitation infrastructure like open sewage systems. When damaged skin or mucous membranes of the eyes, mouth, nose, or vagina come into contact with infected kidneys, urine, or settings contaminated with urine, humans get infected. The main methods of infection transmission are direct contact with rat urine and indirect contact with rat urine-contaminated water, soil, or food [4].
A wide range of clinical signs define leptospirosis in animals. Infertility, mastitis, milk drop syndrome, stillbirth, abortion, and stillbirth are its chief reproductive losses. Leptospirosis in people can result in headaches, fever, chills, sweating, and myalgia. Lethargy, sore joints, and protracted illness are possible additional symptoms. Some extremely pathogenic serovars can result in fatal pulmonary hemorrhaging [5].
Leptospirosis, classified as a neglected a pathogenic spirochete bacteria of the genus Leptospira causes tropical illness. In addition, there are two different types of leptospira: L. biflexa, a non-pathogenic species, and L. interrogans, a pathogenic species that causes leptospirosis. Leptospirosis, which is categorized as a direct anthropozoonosis and is one of the most common bacterial diseases in the world, affects both people and a wide variety of animals. Leptospirosis is typically thought of as a disease that only affects rural areas, although it has been claimed that an urban outbreak of the disease’s severe form happens every year and causes a large amount of mortality [6].
Pathogenic Leptospira are pathogens that dwell in the kidneys of their natural hosts, primarily mammals, and are discharged into the environment with the urine. Under the right environmental circumstances, they can survive for several months. Like, exposure to infected animals, their urine, or a urine-contaminated environment can cause infection (mostly mud and water). The mucous membranes and open skin are the entry points for infection. Numerous sylvatic and domestic animals act as a reservoir for Leptospira, which is widely identified in a variety of animal species. Leptospirosis is a human infection brought on by L. interrogans, of which there are more than 200 identified pathogenic serovars and many routes of transmission [7]. Humans are considered accidental hosts of Leptospira whereas animals are called reservoir hosts. Leptospirosis has a wide range of clinical symptoms and is brought on by recreational contact with water polluted with Leptospira. Leptospirosis is diagnosed based on the sample’s accessibility and the disease’s temporal stage. Laboratory tests used to find leptospira include molecular techniques, serology, culture, microscopy examination, and animal inoculation. Medications like tetracycline, penicillin, ampicillin, doxycycline, streptomycin, and erythromycin are used to treat leptospirosis [8]. Leptospirosis control measures are intended to reduce the occurrence of clinical disease based on integrated actions in several links of the transmission in order to reduce the risk of infection resulting from contact with contaminated environments, infected wild animals, as well as with synanthropic animals and rodents. Leptospirosis is a largely obscure illness in Ethiopia. Therefore, the goals of this work were to provide an one health implication of leptospirosis significance that affects both animals and people [9].
Literature of Leptospirosis
Etiology
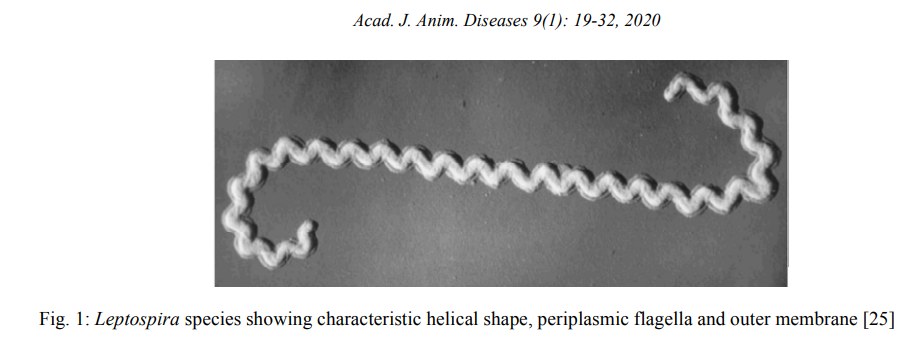
The spirochaetes that cause leptospirosis belong to the genus Leptospira, which now has 20 species: nine of them are pathogenic, six are saprophytic, and five are intermediate [2]. These are obligatory, thin, motile, spirochaetes with finely wound ends that grow slowly. Leptospirosis is gram- negative, however post-mortem diagnosis using fixed or unfixed tissues can benefit from immunological staining and silver staining procedures, which can provide improved results [10]. Leptospirosis bacteria have a corkscrew-shaped morphology, and their end hooks set them apart from other spirochaetes. Leptospirosis has two or more axial filaments, which may be seen under dark field microscopy and are in charge of the spirochete’s motility. There are over 280 serovars and 20 serogroups in the spirochete L. interrogans [11].
Nearly all mammalian species have pathogenic spirochaetes of the genus Leptospira, which cause leptospirosis. The genus Leptospira is separated into two species: L. interrogans, which includes all pathogenic strains, and L. biflexa, which includes saprophytic strains isolated from the environment. It is a member of the Order Spirochaetes, Family Leptospiraceae, and Class Spirochaetes. Pathogenic leptospirosis are invasive, highly mobile spirochetes with the ability to proliferate and live in tissue by evading host defenses. Serovar Pomona, Canicola, Bratislava, Graphityphosa, Hardjo, and Interohemorrhagie are frequent serovars of L. interrogans [12]. There are two types of hosts for the leptospirosis agent: accidental hosts and maintenance hosts. Animals infected with the organism’s adapted serovar are known as maintenance or reservoir hosts, while incidental or accidental hosts are created when vulnerable animals are exposed to serovars that are not adapted to the host [13]. Leptospira differs morphologically from other spirochete bacteria in that they have distinctive hooked ends and are tightly coiled (Figure 1).
Phylogeny of Leptospira
The Leptospira bacteria enters the body and makes its way to the bloodstream through lymphatic capillaries. The bacteria will proliferate in the circulation and go to various organs such as the liver, kidneys, spleen, eyes, and reproductive organs. Following systemic circulation, there are three likely directions. If the animal has a high enough antibody titer, the body will be free of leptospires and there won’t be any clinical symptoms. An animal with a substantial antibody may have a mild or transient leptospiremia, which is followed by mild clinical signs. The animal will cease leaving behind leptospires once the kidneys have eliminated them. In particular, leptospires will persistently shed in the urine for days, months, or even years if the animal has a low or nonexistent antibody titer, which allows leptospires to grow in the bloodstream [14].
Through intact mucous membranes (mouth, nose, eyes, and vagina), or through skin that has sores and scrapes, the bacteria can enter the body through pathogenesis. As soon as they get inside the vascular system, they start to grow quickly and spread to numerous organs, including the kidney, liver, spleen, central nervous system, eye, and genital tract [15, 16, 17]. Epidemiology of Leptospirosis 1.1.1. Host Range and Distributions All mammalian species are susceptible to leptospirosis infection; however cats are less likely to contract the disease than are cattle, sheep, goats, dogs, horses, and pigs. Although it is widespread around the world, it is most prevalent in warm, developing nations where it is more probable that people will come into touch with diseased animals or water that has been tainted by their urine. When the surrounding temperature is warm, Leptospira can thrive in muck, surface water, moist soil, and ponds, rivers, and other water bodies [18].
Interohaemorrhagiae, L. canicola, L. pomonai, L. hardijo, and L. gripotyphosa serovars are present on all continents, and outbreaks have been linked to natural disasters such flooding and hurricanes. Variations in soil and water conditions in contaminated areas are crucial for an organism’s survival in its environment. Drying and pH values between 6 and 8 can make the organism vulnerable. The life of the organism is harmed by ambient temperatures around 7.1°C or below 34°C [19].
Transmission of the Disease Contact with urine or other bodily fluids containing live Leptospira can result in the direct or indirect transmission of leptospirosis from one carrier animal to another healthy animal. Depending on the virulence of the organism and host, congenital transmission is potentially a possibility. For several weeks after birth, a live, infected neonate might harbor the virus and serve as a source of infection. There have also been reports of sexual transmission in rats, pigs, and dogs. Although it is uncommon, transmission can occur through natural breeding or artificial insemination. Humans can contract the virus by direct contact with infected animal tissues, consumption of tainted food and water, sexual contact, trans-placental transmission from an infected mother to her fetus, and breastfeeding [20].
Leptospirosis in Animals
Leptospirosis can affect animals of any age; however young animals are more sensitive to the illness than adult animals are. Access to contaminated water sources, such as streams, rivers, floodwater, or drainage water, as well as obtaining or borrowing diseased male animals for natural insemination are some management practices that increase the risk of infection. Leptospirosis is frequently referred to as a seasonal disease because it mostly affects temperate regions throughout the summer and fall. The peak incidence occurs during the rainy season in tropical climates [21]. Leptospirosis in cattle is typified by a wide range of clinical symptoms that vary slightly amongst affected species: During the leptospiremic phase, clinical signs of acute or sub-acute disease can be observed. These signs include septicemia, high fever, anorexia, mucosal petechiae, depression, and acute hemolytic anemia with jaundice, mucosal pallor, and hemoglobinuria [22].
Reproductive losses from abortion, stillbirth, infertility, mastitis, and milk drop syndrome are typically linked to chronic infections. Pregnancy is most commonly terminated in the final trimester. Anorexia, lethargy, and vomiting were the three most prevalent clinical signs in dogs with leptospirosis, though there are other nonspecific signs as well. Severe disease manifestations in horses include petechial hemorrhages on the mucosa, anemia, conjunctiva suffusion, and general depression. Renal failure in foals and placentitis, abortion, and stillbirths may also be present in pregnant mares. Only pregnant or nursing cows experience infertility and milk drop because the Leptospira organisms need a pregnant uterus and a nursing mammary gland to multiply. Up to50% of cows may experience a sudden decline in milk production at one time, which could lead to [23].
The Role of Rodent Leptospirosis spread by rodents is a significant factor. They may excrete up to 100 million leptospirosis in the urine, which can contaminate water, soil, and food. As a result, they are one of the main sources of human infection. It is believed that these reservoirs serve as a source of infection for domesticated animals and people, who may subsequently infect additional animals and people. The presence of rodents in developing nations could serve as a reservoir for human infection. Human illness has also been brought on by contact with adopted wild rodents in wealthy nations. Rodents are the main host responsible for transmitting leptospirosis to people in urban and rural slum areas [24].
Many species of murine rodents have been recorded as carriers of this pathogen around the world. Due to their wide distribution and high abundance in rural areas with Feral and per domestic rodents are thought to be the most significant reservoirs in farmlands and in cities with high human population density. This is supported by the numerous cases of human and animal leptospirosis that have been linked to rats in more than 40 different nations [4]. Interohaemorrhagiae is the most common serogroup despite the fact that numerous strains and serovars are involved in human cases, highlighting the significance of rodents as a significant reservoir. It is thought that people contract it from the commensal brown rat (Rattus norvegicus), which is intimately associated with human activities. Rats can infiltrate houses, factories, and other buildings through broken sewers and come into touch with food, among other things, putting humans at risk of contracting Leptospira [25].
Factor that Increase Rodent Infestation Climate and season: as rats move indoors to seek shelter, winter is linked to an increase in complaints about rats. Urban rats may grow at a faster rate in the winter because there is less competition (more food available) due to the population being smaller overall and because the colder weather slows down the breakdown of waste. Leptospirosis outbreaks have been shown to be caused by a combination of anthropogenic factors and environmental drivers that interact with climatic changes in many regions of the world. Natural disasters that can lead to an increase in rodent populations include heavy rainfall and extreme weather [26]. Food and shelter availability: The number of rats is influenced by the availability of food sources. Rat infestation is associated with improperly stored or disposed of food and organic waste, messy gardens, and the presence of domestic animals (dogs, cats, pets, and livestock) in homes, yards, or city blocks. The harborage’s availability dictates whether or not the population settles down. Any abandoned building that is easily accessible could serve as a breeding ground for infestations. Rat infestations are linked to access points near utility lines and sewer systems, holes or cracks in the roof, walls, ceiling, and building foundation, and especially abandoned structures [24].
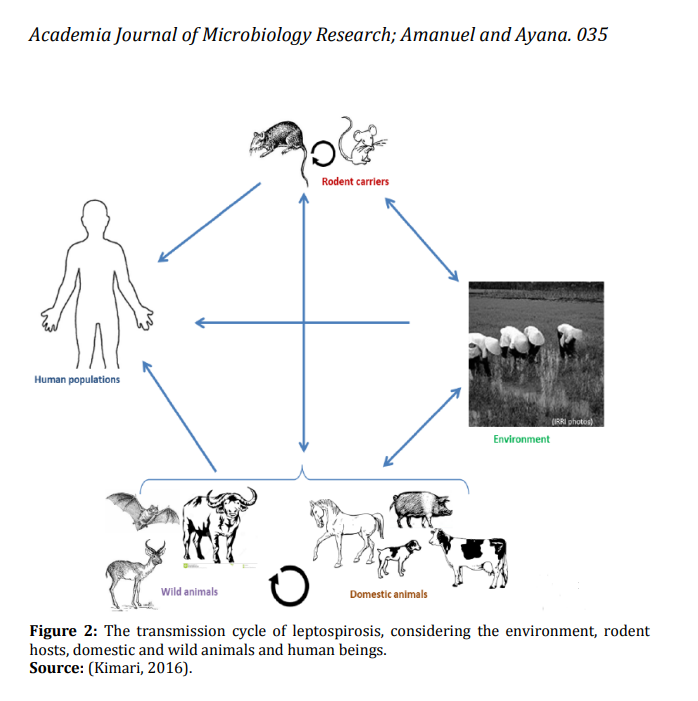
Urban rodent infestations may be linked to higher housing densities because the spread and colonization of one home can have an impact on nearby residences. Rats have a higher chance of successfully spreading over short distances. Rat infestations disproportionately affect impoverished neighborhoods. Rats typically find suitable harborage and food sources in lower socioeconomic neighborhoods, where properties may be old, dilapidated, and abandoned, and public services, such as waste disposal, may be inadequate, creating unsanitary conditions that could serve as food sources [27]. High rodent densities and the close proximity of rodents to humans and their food supplies are expected to lead to potential disease epidemics, even though data on actual disease prevalence in humans and rodents, as well as their environmental and socioeconomic correlates, are extremely scarce globally for both rural and urban communities, as shown in Figure 2 below [28].
Public Health Significance of Leptospirosis
The major burden attributed to leptospirosis has been its severe life-threatening manifestations. Leptospirosis has emerged as an important cause of pulmonary haemorrhage syndrome and acute kidney injury due to Weil’s disease. In many regions where transmission is endemic. Case fatality for pulmonary haemorrhage syndrome and Weil’s disease is more than 10% and 70% respectively. In addition, leptospirosis is increasingly recognized as an important cause of undifferentiated fever. The majority of leptospirosis patients are not recognized or misdiagnosed as malaria, dengue, and other causes of an acute febrile illness. The lack of an adequate diagnostic test has further contributed to under- reporting of cases as well as deaths. Underestimation of the morbidity and mortality due to leptospirosis is therefore common and has directly contributed to its neglected disease status. In humans, more than 500,000 estimated cases of severe leptospirosis are reported annually, with case fatality rate exceeding 10% [29].
Mode of Transmission in Human The main sources of infection for the incidence of disease are urine of infected or carrier animals, contaminated surface water, mud, feed, soil, aborted fetuses and uterine discharges. From these sources, the organism enters the body via mucous membranes of the eyes, mouth, nose, vagina, or leptospirosis penetrate through small and sometimes invisible abrasions in the skin. Modes of transmission of leptospirosis are often categorized as direct or indirect depending on the immediate source of infection.
Transmission is direct if the immediate source of infection is animal tissue, body fluids, urine, trans placental, or venereal, whereas immediate source of infection is an environment contaminated with urine of carrier animals and is indirect [30]. Contact with rodents and water sources are significant factors, particularly in flood periods. Transmission between humans are very rare and it occurs through blood transfusion, organ transplantation, breast feeding and sexual intercourse. Leptospirosis affects risk groups that are exposed to animal reservoirs or contaminated environments, such as abattoir and sewage workers, salver workers, coal mines, plumbers, farm workers, trappers, veterinarians, pet shop owners, meat handlers, military personnel, laboratory workers, and workers in fishing industry. Recreational activities that increase the risk of leptospirosis are gardening and water sports such as canoeing, kayaking, swimming and white water rafting residents of some urban areas. Household exposure with in pet dogs, domesticated livestock, rainwater catchment systems, infestation by infected rodents. And also walking barefoot through surface water, skin lesions, contact with wild rodents, accidental laboratory exposure [30].
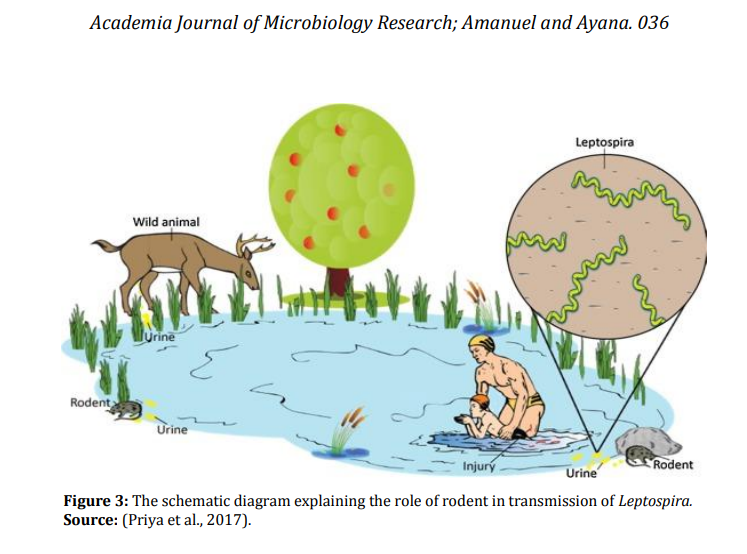
Leptospirosis is diagnosed in men more often than in women, and this has generally been linked to the prevalence of men in high-risk occupational groups. Contact with rodents and water sources, particularly during times of flooding, are significant concerns (Figure 3). Human-to- human transmissions are extremely uncommon and can happen through sexual activity, breast-feeding, organ transplantation, blood transfusions, and organ donation [31].
Clinical Sign in Human In humans, the incubation period can range from 2 to 29 days, but it typically lasts 7 to 12 days. Human infections range from mild, flu-like cases that may not be identified as leptospirosis to severe, atypical syndromes, and progressive fulminant illnesses without two distinct phases. While the classic presentation of leptospirosis is a biphasic illness, leptospirosis can occur in many forms. The acute phase, also known as the septicemic phase, is the initial stage of the classical biphasic illness. It is typified by nonspecific symptoms like fever, chills, headache, and conjunctival suffusion, and it typically starts suddenly [32]. Myalgia is usually a severe pain that primarily affects the thighs, calves, and back. Other symptoms that some patients experience include weakness, photophobia, lymphadenopathy, nausea, vomiting, sore throat, coughing, and chest pain in addition to abdominal pain, nausea, and vomiting. The stage lasts three to seven days. The second stage, known as the “immune phase,” is named so because anti-leptospiral antibodies start to form during this phase. Three to four days later, the septicemic phase follows. Anicteric or icteric disease can develop in leptospirosis patients in the second stage. This syndrome usually lasts a few days and is characterized by a severe headache, stiff neck, and other meningeal symptoms. Less severe and more common is the anicteric form. The more severe form of leptospirosis is called Weil disease. That happens in 5–10% of of all patients, is often rapidly progressive, and may be associated with multiorgan failure [33].
Diagnosis of Leptospirosis
Direct Microscopy
Leptospires may be seen on microscopic evaluation of blood, urine, CSF and peritoneal or pleural exudate during the first 10 days of the infection. Dark field microscopy is required as the leptospires are very small, however more than 10000 organisms/ml are required to be able to see them. The method of direct examination by using dark field microscopy is limited to urine because other body fluids contain artefacts similar to Leptospira organism and the method has both low sensitivity (40.2%) and specificity (61.5%). A range of staining methods has been applied to direct detection, including immune fluorescence staining, immune peroxidase staining, and silver staining. These methods are not widely used because they lack commercially available reagents and their relatively low sensitivity [17].
Isolation and Identification
For the first 7 to 10 days, like an infection, the bacteria can be found in the blood and cerebrospinal fluid (CSF), before spreading to the kidneys. Due to the wide variety of symptoms, the microorganism can be detected in fresh urine after 7 to 10 days; however, due to early diagnostic efforts, such as isolation from blood or other clinical materials through culture of pathogenic leptospira [17]. It is also difficult to isolate Leptospira from patient samples; the organisms often take 1-2 weeks. Isolation of the microorganism from fetal tissue (kidney, liver, lungs) confirms maternal infection. Isolation requires expensive and properly prepared and kept culture media. Inoculated media are incubated at 28-30°C for several weeks or months. Cultures are performed in albuminpolysorbate media such as Ellinghausen-McCulloughJohnson-Harris (EMJH) medium, which is available commercially. Older media contained serum. Primary cultures are performed in semisolid medium, to which 5-fluorouracil is usually added as a selective agent [34].
Molecular Technique
DNA amplification using PCR and DNA primers have become an excellent diagnostic tool for detecting the presence of Leptospira in animal tissues and fluids and it can be applied to blood, urine, CSF and tissue samples anti or post mortem. The chief advantage of PCR is the prospect of confirming the diagnosis during the early acute (leptospiremic) stage of the illness, before the appearance of immunoglobulin M (IgM) antibodies, when treatment is likely to have the greatest benefit. In fulminating cases, in which death occurs before sero conversion, PCR may be of great diagnostic value [35].
Serological Methods
Macroscopic and microscopic agglutination tests, complement fixation test and ELISA technique are used for the detection of leptospirae in serum. The macroscopic agglutination examination is a screening test that uses dead Ag but suffers from specificity. Microscopic Agglutination Test (MAT) is the standard method for the serological diagnosis of leptospirosis. To execute MAT, leptospires are grown in liquid media and used alive. Serum is mixed with this live liquid grown leptospires in order to test for agglutination. Agglutination indicates that the serum contains anti-leptospiral antibodies [35]. As the leptospires are thin and small, dark field microscopy is used to evaluate the agglutination. Agglutinating antibodies are most frequently IgM and to a lesser extent IgG. Enzyme linked immuno sorbent assay (ELISA) test of leptospirosis can be performed either by using commercial kits or within house produced antigen. A broadly reactive so-called genus-specific antigen is generally used to detect IgM and sometimes also IgG antibodies against leptospiral antigen. The presence of IgM antibodies indicates current or recent leptospirosis. Common commercially-available Leptospira IgM ELISA is used to serologically detect acute leptospiral infections in patient serum samples. This ELISA works on the principle that any Leptospira IgM antibodies present in patient serum will bind to the leptospiral antigen attached to the polystyrene surface of the micro wells. The ELISA test is more accurate than other tests and has much advantage from the point of view of laboratory practices. It has excellent diagnostic specificity and sensitivity, convenient technical feature including automation and can be used efficiently as serenity test for large number of serum samples [36].
Control and Prevention
Due to the disease’s resistance to routine laboratory tests, leptospirosis has been a disease that has been underreported, and there are just a few accurate global incidence figures. Leptospirosis is extremely difficult to find in a population. Although avoiding contact with potentially infected animals or water tainted with animal urine can considerably reduce the incidence of leptospirosis. Workers should wear protective gear or footwear, just like in their occupations. While swimming in fresh water, any skin cuts should be treated with a waterproof covering to guard against a variety of illnesses. Human immunization helps to provide a certain level of protection against illness in companion dogs, providing both the animal and the home with some degree of protection from the germs [37].
Given the prevalence of rodent species that act as infection reservoirs, the disease’s total eradication appears to be impractical. Therefore, understanding the epidemiology and transmission mechanisms of leptospirosis is essential to developing effective preventative methods. By limiting exposure and putting preventative measures, vaccinations, and pre- or post-exposure chemoprophylaxis into place, the disease can be avoided. The danger of infection is significantly decreased by housing construction that keeps rodents out of water sources and residential living areas. Avoid swimming in hazardous water and going barefoot through floodwaters. The choice of animal relocation must take into account the herds’ lack of leptospirosis responsiveness. Due to serovar- specific immunity and the fact that vaccines only provide protection against the serovars covered by the immunogens, leptospirosis vaccines for domestic animals are only able to reduce the severity of the disease [21].
Status of Leptospirosis in Ethiopia
There is little information on leptospirosis in humans and animals in Ethiopia, despite the fact that the country’s climate, socioeconomic conditions, and other factors are very favorable for the disease’s occurrence and spread. As they are in other parts of the world, rats may be a major source of leptospirosis. Wonji Hospital is conducting a pilot study on human leptospirosis. A study conducted on 59 feverish patients who visited Wonji Hospital’s outpatient department found that 47.46% of the patients tested positive for leptospirosis, and that males were more likely than females to contract the illness [38].
In Ethiopia, seropositivity has been shown in domestic animals under work [21], found that 91.2% of horses, 70.7% of cows, 57.1% of pigs, 47.3% of goats, 43.4% of sheep, 15.4% of camels, and 8.3% of dogs had the condition. A total of 184 out of 418 horses exhibited antibody titres of 1:100 or higher to at least one of the 16 serovars, indicating that horses from Central and Southern Ethiopia are home to 16 different serovars of the Leptospira species. This indicates that 44% of the equines in the sample tested positive for at least one serovar. Drinking river water and having dogs on nearby neighboring properties were the two main risk factors for horses that tested positive for Leptospira. Dogs’
capacity to manage rodents may have contributed to their protective effect against seropositivity to serovars Bratislava and Djasiman [39].
Conclusion and Recommendation
The most prevalent and pathogenic Leptospirosis interrogans are the cause of leptospirosis, the most prevalent zoonotic disease of worldwide significance. Leptospira is unique among the spirochetes. Humans and animals are both affected by it. Although skin abrasions and the urine of sick animals tend to propagate the germs. In animals like rats and mice, the bacteria enter the body through minute wounds, mucosa, conjunctiva, and vaginal tracts. Natural hosts, primarily mammals, have kidneys where pathogenic Leptospira thrives and is discharged into the environment with urine. Where it can endure under ideal circumstances for a number of months. Leptospirosis can be effectively treated with antibiotics, and current immunization programs for domestic animals can lessen the severity of the condition.
Consequently, Ethiopia and other African countries lack the understanding on leptospirosis. Leptospirosis is a highly contagious disease that can affect humans and animals that are susceptible. Therefore, it is best to prevent getting urine on cuts or mucous membranes. Protective gear, including as gloves, eye protection, and face masks, should be worn when handling contaminated objects or animals. Although, most antibiotics are effective in treating it. Diagnosing leptospirosis is simple using microscopy, culture, serological and PCR methods.
Based on the above information, the following points were forwarded as recommendation:
- Applying effective control measures and raising public awareness of leptospirosis zoonotic transmission is advised.
- Additionally, collaboration in the fields of environmental, animal, and human health should be used to strength one Health.
- Since there are currently so few findings that have been reported, more studies on the prevalence and incidence of leptospirosis in Ethiopia are needed.
- In order to protect themselves from animal reservoirs and contaminated settings, communities at risk should wear protective gloves.
References
-
Levett PN (2001) Leptospirosis. Clin Microbiol Rev 14(2): 296-326.
-
Monteiro MB, de Sousa IE, Piteira M, Coelho S, Freitas P (2021) Leptospirosis, a Re-emerging Threat. Cureus 13(4): e14295.
-
Rajapakse S (2022) Leptospirosis: Clinical aspects. Clin Med (London) 22(1): 14-17.
-
Boey K, Shiokawa K, Rajeev S (2019) Leptospira infection in rats: A literature review of global prevalence and distribution. PLoS Negl Trop Dis 13(8): e0007499.
-
Mori M, Bakinahe R, Vannoorenberghe P, Maris J, de Jong E, et al. (2017) Reproductive disorders and Leptospirosis: A case study in a mixed-species farm (cattle and swine). Vet Sci 4(4): 64.
-
Cilia G, Bertelloni F, Albini S, Fratini F (2021) Insight into the Epidemiology of Leptospirosis: A Review of Leptospira Isolations from “Unconventional” Hosts. Animals (Basel) 11(1): 191.
-
Sayanthi Y, Susanna D (2024) Pathogenic Leptospira contamination in the environment: a systematic review. Infect Ecol Epidemiol 14(1): 2324820.
-
WHO (2009) Leptospirosis Fact Sheet. pp: 1-12.
-
Ame MM (2021) Review on Leptospirosis and its Public Health Significance. Vet Med Open J 6(2): 51-59.
-
Md-Lasim A, Mohd-Taib FS, Abdul-Halim M, Mohd- Ngesom AM, Nathan S (2021) Leptospirosis and coinfection: Should we be concerned?. Int J Environ Res Public Health 18(17): 9411.
-
Mohammed H, Nozha C, Hakim K, Abdelaziz F (2011) LEPTOSPIRA: Morphology, Classification and Pathogenesis. Journal Bacteriol Parasitol 2(6): 1-4.
-
Piredda I, Ponti MN, Palmas B, Noworol M, Pedditzi A, et al. (2021) Molecular typing of pathogenic leptospira species isolated from wild mammal reservoirs in Sardinia. Animals (Basel) 11(4): 1-13.
-
Mgode GF, Machang’u RS, Mhamphi GG, Katakweba A, Mulungu LS, et al. (2015) Leptospira Serovars for Diagnosis of Leptospirosis in Humans and Animals in Africa: Common Leptospira Isolates and Reservoir Hosts. PLoS Negl Trop Dis 9(12): e0004251.
-
Sun AH, Liu XX, Yan Y (2020) Leptospirosis is an invasive infectious and systemic inflammatory disease. Biomed Journal 43(1): 24-31.
-
Gonçalves-de-Albuquerque CF, Coeli da Cunha CM, de Azevedo Martins C, Barnese MRC, Burth P, et al. (2023) Cellular Pathophysiology of Leptospirosis: Role of Na/K- ATPase. Microorganisms 11(7): 1695.
-
Lehmann JS, Matthias MA, Vinetz JM, Fouts DE (2014) Leptospiral pathogenomics. Pathogens 3(2): 280-308.
-
Budihal SV, Perwez K (2014) Leptospirosis diagnosis: Competancy of various laboratory tests. J Clin Diagnostic Res 8(1): 199-202.
-
Motto SK, Shirima GM, Clare B, Cook KAJ (2021) Epidemiology of leptospirosis in tanzania: A review of the current status, serogroup diversity and reservoirs. PLoS Negl Trop Dis 15(11): e0009918.
-
Fentahun T, Alemayehu M (2012) Leptospirosis and its Public Health Significance: A Review. Eur J Appl Sci 4(6): 238-244.
-
WHO (2003) Human leptospirosis: guidance for diagnosis, surveillance and control.
-
Yadeta W, Michael BG, Abdela N, Box PO (2016) Leptospirosis in Animal and its Public Health Implications: A Review. World Apllied Sci J 34(6): 845- 853.
-
Tulu D (2020) Epidemiology and Zoonotic Implication of Leptospirosis in Domestic Animals in Ethiopia. Acad J Anim Dis 9(1): 19-32.
-
Bolin CA (2005) Leptospirosis in cattle: disease review and update. North Am Vet Conf pp: 1475-1478.
-
Bradley EA, Lockaby G (2023) Leptospirosis and the Environment: A Review and Future Directions. Pathogens 12(9): 1167.
-
Maas M, Vries A, Reusken C, Buijs J, Goris M, et al. (2018) Prevalence of Leptospira spp. and Seoul hantavirus in brown rats (Rattus norvegicus) in four regions in the Netherlands, 2011-2015. Infect Ecol Epidemiol 8(1): 1490135.
-
Feng AYT, Himsworth CG (2014) The secret life of the city rat: A review of the ecology of urban Norway and black rats (Rattus norvegicus and Rattus rattus). Urban Ecosyst 17(1): 149-162.
-
Almeida A, Corrigan R, Sarno R (2013) The Economic Impact of Commensal Rodents on Small Businesses in Manhattan’s Chinatown: trends and possible causes. Suburb Sustain 1(1): 1-17.
-
García-Peña GE, Rubio AV, Mendoza H, Fernandez M, Milholland MT, et al. (2021) Land-use change and rodent- borne diseases: Hazards on the shared socioeconomic pathways. Philos Trans R Soc B Biol Sci 376(1837): 20200362.
-
Costa F, Hagan JE, Calcagno J, Kane M, Torgerson P, et al. (2015) Global Morbidity and Mortality of Leptospirosis: A Systematic Review. PLoS Negl Trop Dis 9(9): e0003898.
-
American P, Bureau S (2001) Zoonoses and Communicable Diseases Common to Man and Animals. 1(580).
-
Pavli A, Maltezou HC (2008) Travel-acquired leptospirosis. J Travel Med 15(6): 447-453.
-
Goarant C (2016) Leptospirosis: risk factors and management challenges in developing countries. Res Rep Trop Med 7: 49-62.
-
Lemon M, Dorsch M, Street K, Cohen R, Hale P (2001) Splenic rupture after vomiting. J R Soc Med 94(10): 527- 528.
-
Narkkul U, Thaipadungpanit J, Srilohasin P, Singkhaimuk P, Thongdee M, et al. (2020) Optimization of culture protocols to isolate Leptospira spp. From environmental water, field investigation, and identification of factors associated with the presence of Leptospira spp. in the environment. Trop Med Infect Dis 5(2): 94.
-
Merien F, Amouriaux P, Perolat P, Baranton G, Girons IS (1992) Polymerase chain reaction for detection of Leptospira spp. in clinical samples. J Clin Microbiol 30(9): 2219-2224.
-
Adler B, Murphy AM, Locarnini SA, Faine S (1980) Detection of specific anti-leptospiral immunoglobulins M and G in human serum by solid-phase enzyme-linked immunosorbent assay. J. Clin. Microbiol 11(5): 452-457.
-
Sykes JE, Reagan KL, Nally JE, Galloway RL, Haake DA (2022) Role of Diagnostics in Epidemiology, Management, Surveillance, and Control of Leptospirosis. Pathogens 11(4): 1-24.
-
Yimer E, Koopman S, Messele T, Wolday D, Newayeselassie B, et al. (2004) Human leptospirosis, in Ethiopia: a pilot study in Wonji. Ethiop J Heal Dev 18(1): 48-51.
-
Tsegay K, Potts AD, Aklilu N, Lötter C, Gummow B (2016) Circulating serovars of Leptospira in cart horses of central and southern Ethiopia and associated risk factors. Prev. Vet Med 125: 106-115.
- Measuring What Matters: Data Gaps, Certificate of Need Reform, and Pediatric Psychiatric Inpatient Capacity in North Carolina
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal