The Budget Impact of Itopride in the Treatment of Functional Dyspepsia in Vietnam
Introduction: An estimated 7.8-22.4 million Vietnamese suffer from functional dyspepsia. Prokinetic agents, such as itopride, target this group of patients by enhancing gastric motility through amplifying and coordinating gastrointestinal muscle contractions. Itopride is currently reimbursed in public hospitals at Vietnam Central level hospitals (level 1) and provincial level hospitals (level 2) for the treatment of functional dyspepsia. This study analyses the financial impact of expanding the access of itopride for patients with functional dyspepsia to include level 3 (District level) hospitals + level 4 (Commune health stations) hospitals in Vietnam. Methods: A budget impact model was developed in accordance with the good practice guidelines from the International Society for Pharmacoeconomics and Outcomes Research. The model included both drug costs and healthcare resource utilisation costs. Results: The broadening of the reimbursement of itopride to include level 3+4 hospitals was estimated to provide benefit for between 13.7% (105,923) to 24.6% (89,343) more patients at only 3.3% (VND 41,742M) to 4.2% (VND 74,617M) additional costs over five years. Conclusion: Itopride is deemed to represent great benefit for patients suffering from functional dyspepsia in Vietnam.
Abbreviations
FGID’s: Functional Gastro-Intestinal Disorders; FD-GERD: FD with Gastroesophageal Reflux Disease; EPS-IBS: Epigastric Pain Syndrome with Irritable Bowel Syndrome; PDS: Postprandial Distress Syndrome; BBB: Blood Brain Barrier; DAV: Drug Administration of Vietnam; ISPOR: International Society for Pharmacoeconomics and Outcomes Research.
Introduction
Functional Dyspepsia is a common upper gastrointestinal condition which commonly presents as postprandial fullness (post meal), early satiation, epigastric pain, and/or epigastric burning [1]. Functional dyspepsia is part of a wider group of Functional Gastro-Intestinal Disorders (FGID’s) which are often unexplained in pathogenesis. Diagnosis can be lengthy as the symptoms often overlap with other gastrointestinal conditions. Thankfully, the presence of functional dyspepsia is not associated with increase in mortality [2].
The diagnosis of functional dyspepsia is defined by the detailed ‘ROME diagnostic criteria’ (An Internationally established criteria developed by experts in the field of gastroenterology). The ROME criteria is now in its 4th iteration: ROME IV definition states that functional dyspepsia have at least one of four the following symptoms: 1) Postprandial fullness; 2) Early Satiety; 3) Epigastric pain; 4) Epigastric burning; and no underlying organic disease [3]. Several factors can affect prevalence from age, gender, ethnicity, smoking status, alcohol consumption, and dietary factors [4]. Modifiable risk factors encompass severe stress, chronic fatigue, smoking, abnormal BMI, and sleep patterns, while non-modifiable risk factors include advanced age, chronic diseases, and female sex [5]. The prevalence of functional dyspepsia globally is variable and has been difficult to determine due evolving definitions used in older literature. Also, the elimination of organic disease in selection of patients for clinical trials poses an inherent challenge for most population-based studies [4, 6]. In a 2024 systematic review and meta-analysis by Lee et al., it was found that the global prevalence of functional dyspepsia varied from 11.9% according to the Rome I criteria to 6.8% according to the Rome IV criteria from 1990 to 2020 [7]. The results were consistent with the Rome Foundation Global Study, showing that women consistently had a significantly higher prevalence than men, and that the prevalence was higher in the 18-39 age group (9.2%) [8]. The prevalence of functional dyspepsia is higher in developing or low-and middle-income countries compared to developed or high-income countries [5, 7].
The 2012 Asian Consensus report on Functional Dyspepsia has suggested that the presentation of sub-types of functional dyspepsia in Asian populations differ to those in to the West [9]. With East and South-East Asian countries, patients predominantly experience Postprandial fullness symptoms more so than the epigastric pain [9]. Two large clinical trials based on endoscopy examination of patient with dyspepsia using the ROME III diagnosis criteria demonstrate the two sperate sub conditions affecting Caucasian and East Asian populations: One trial by Ford et al 2014 based in Canada with mostly white Caucasian patients and the other by Fang et al 2014 based in Taiwan with all ethnic Chinese patients. The Taiwanese study showed 71.9% of patients had the PDS sub-type, and Canadian study showed 40.8% had PDS sub-type and 41.2% with overlap of EPS and PDS [10, 11].
Functional dyspepsia is treated with multiple agents and varying success. The treatment of Functional Dyspepsia differs in various regions. In Western countries, such as the USA and Western Europe, acid suppression with proton pump inhibition (and or Histamine-2 receptor antagonists) is the established first-line treatment [1]. Thereafter, tricyclic anti-depressants are 2nd line treatments and prokinetics are 3rd line treatments [12].
In East and South-East Asia, both acid suppression therapy and prokinetics are established 1st line treatments. The 2012 Asian consensus report on functional dyspepsia Miwa H, et al. [9] deemed prokinetics to be a first treatment for the PDS subtype, and second-line treatment for EPS. In countries such as China and South Korea, Prokinetics are often mainstay therapy recommended for patients with PDS symptoms [13]. According to the 2023 Asia-Pacific guideline by the Asian Pacific Association of Gastroenterology, the majority of functional dyspepsia patients have an overlapping disorder that is associated with overlap conditions in the Asia-Pacific, such as FD with gastroesophageal reflux disease (FD-GERD), epigastric pain syndrome with irritable bowel syndrome (EPS-IBS), postprandial distress syndrome with IBS (PDS- IBS), and FD-Constipation. The recommended treatment for FD-GERD involves dual histamine H1/H2 receptor blockade, antisecretory agents, neuromodulators, and fundic relaxants. For EPS-IBS, anti-spasmodic agents, tricyclic agents, and dual histamine blockade are typically used. In the case of PDS-IBS, treatment may include prokinetic agents, a low FODMAPs diet, Rixafimin, and herbal medicine. Fecal evacuants, Pan-GI prokinetic agents, and reducing methane production in the gut are common approaches for managing FD-constipation [14].
Due to its’ disease nature being that it is often chronic and recurring in disease course. Research estimates only 20% of patients with functional dyspepsia become symptom free in the long-term [15, 16]. A significant proportion of patients with functional dyspepsia have abnormalities in gastric motility and fundal accommodation. Prokinetic agents target this group of patients by enhancing gastric motility through amplifying and coordinating gastrointestinal muscle contractions [17]. These agents include itopride, mosapride, domperidone, and so forth. In a systematic review and meta- analysis conducted by Pittayanon, et al. [17] reviewed 29 trials which included 6 prokinetic agents showed moderate effectiveness against placebo (overall global symptom improvement 40% vs placebo 26%) [18].
Itopride works by blocking Dopamine (D2) receptors and inhibiting acetylcholinesterase. This reverses the inhibition of gastric motility caused by dopamine receptors and enhances postprandial gastric motility. Itopride’s benefit over other prokinetics is its’ favourable adverse effect profile. It does not cross the blood brain barrier (BBB), and thus does not prolong QT interval or serious cardiac events unlike metoclopramide, and domperidone. It is estimated that there are between 7.8 and 22.4 million Vietnamese people to with functional dyspepsia [6]. Vietnam has one of the highest rates of Helicobacter pylori (H. pylori) infection and related gastrointestinal diseases among Southeast Asian countries. A study conducted by Quach in 2022 found a higher occurrence of functional dyspepsia coexisting with gastroesophageal reflux disease (GERD) in Vietnamese patients, with postprandial distress syndrome being notably prevalent [19].
Vietnam like many other developing South-East Asian countries, most of the health care provided is through public hospitals. There are four levels of public hospitals in Vietnam Central level hospitals (level 1), Provincial level hospitals (level 2), District level hospitals (Level 3) and Commune health stations (level 4) [20]. Itopride is current reimbursed the only prokinetic reimbursed for the treatment of functional dyspepsia in a hospital setting in Vietnam. However, the reimbursement is only for level 1+2 hospitals. In level 3+4 hospitals patients are receiving domperidone instead to alleviate the symptoms of functional dyspepsia, though domperidone does not have formal approval from the Drug Administration of Vietnam (DAV) for the treatment of functional dyspepsia.
This study analyses the financial impact of expanding the access to itopride for patients with functional dyspepsia to include level 3+4 hospitals in Vietnam.
Methodology
Number of people Receiving Prokinetics in Vietnam
A budget impact model was developed in Microsoft Excel in accordance with the good practice guidelines from the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) [21]. The different steps of the budget impact model are displayed in Figure 1.
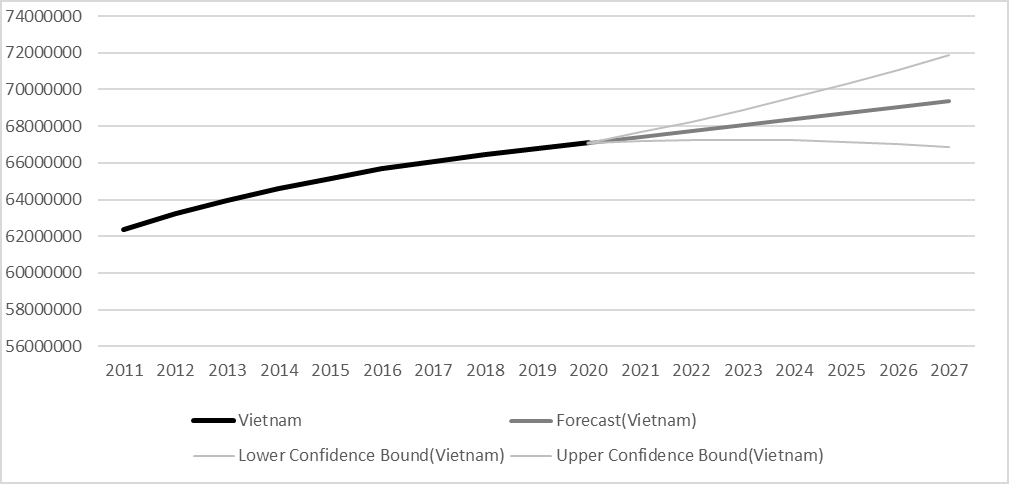
![Figure 1: Overview of the steps in the budget impact analysis. The model time frame was 5-years starting in 2023 and ending in 2027, and the perspective was from the health care payer in Vietnam. It was assumed that Vietnamese people from the age 15-64 would be the primary group to access itopride in level 3+4 hospitals in Vietnam. This population grew from 62.4M in 2011 to 67.1M in 2020 according to the World Bank [22]. This is estimated to further increase from 68, 1M in 2023 to 69,4M in 2027 (Figure 2).](/fulltextimages/13245/fig_1.png)
Figure 1: Overview of the steps in the budget impact analysis. The model time frame was 5-years starting in 2023 and ending in 2027, and the perspective was from the health care payer in Vietnam. It was assumed that Vietnamese people from the age 15-64 would be the primary group to access itopride in level 3+4 hospitals in Vietnam. This population grew from 62.4M in 2011 to 67.1M in 2020 according to the World Bank [22]. This is estimated to further increase from 68, 1M in 2023 to 69,4M in 2027 (Figure 2).
Ghoshal et al. estimated that 8%-23% of Asian people suffer from functional dyspepsia Ghoshal UC, et al [6] hence the midpoint of 15% was chosen for this model. Of these it is estimated that 13.29% are un-investigated for functional dyspepsia [6]. Of the remaining 86.71% (=100% - 13.29%) the proportion of people diagnosed with functional dyspepsia is estimated to be 55.04% based on 8 studies [6, 23, 24, 25, 26, 27]. This was calculated by weighting each study with number of patients in the study divided by the total number of studies of all the studies (Table 1).
| Diagnosed | N | Proportion diagnosed | Weighted proportion |
|---|---|---|---|
| Li 2005 (23) | 782 | 69% | 4.99% |
| Kwan 2003 (24) | 1353 | 43% | 5.38% |
| Kawamura 2001 (25) | 263 | 13% | 0.32% |
| Kim 2004 (26) | 476 | 70% | 3.08% |
| Ji 2003 (27) | 274 | 41% | 1.03% |
| Noh 2010 (28) | 2388 | 8% | 1.79% |
| Mahadeva 2008 (29) | 210 | 62% | 1.20% |
| Wai 2002 (30) | 5066 | 80% | 37.25% |
| Total | 10812 | 55.04% |
Table 1: Estimated proportion of people diagnosed with functional dyspepsia.
There was no information in the literature with respect to the proportion of diagnosed patients receiving prokinetic treatment and an assumption was made that this was 30%. This assumption will be tested in scenario analysis.
A report by the World Bank estimates that 80% of the Vietnamese population is serviced by level 1+2 hospitals [28, 29, 30, 31]. The proportion of people serviced at level 3+4 hospitals was therefore assumed to be the residual 20%.
Use and cost of the Proposed Drug
The market share of itopride and domperidone in Vietnamese level 1+2 hospitals was estimated using IQVIA market data 2021 (data on file). The market share split was 74.9% for domperidone (Motilium-M) and 25.1% for Itopride (Ganaton). The annual drug costs of itopride 50mg are based on the assumption that a patient in a one-year cycle takes one capsule three times per day for 4-week course. The price of one pack containing 20 tablets of 50mg each is VND 105,520. This equates to VND 5,276/tablet. The recommended dose is 3 tablets of 50mg per day and therefore the cost of a 4-week course is estimated to be VND 443,184.
The annual drug costs of domperidone 10mg are based on the assumption that a takes one tablet three times per day for a 4-week course. A pack of domperidone contains 100 tablets and a pack costs VND 181,400. This means that 4-weeks of treatment with domperidone costs: (VND 181,400/100) x (3 x 4 x 28) = VND 152,376.
The costs of itopride and domperidone were obtained from the Vietnamese Ministry of Health website [32].
Changes in Use and Costs of other Medical Services
The model assumes patients who are symptom-free will require less healthcare service utilization. This assumption is based off a systematic review and meta-analysis by Pittayanon, et al. [17]. Itopride showed significantly lower post‐treatment symptom scores, compared to placebo with a relative risk of 0.70 for risk of not being symptom free. The type of medical services utilized related to functional dyspepsia was based on the information provided by Chuah, et al. [32], a paper on the utilization of healthcare services by patients with functional dyspepsia in Malaysia. These services included endoscopy, colonoscopy, gastrointestinal imaging, and unscheduled general practitioner/emergency department/hospital visits. Number of services per patient per year are displayed in Table 2.
| Service | Services per 5 years (Chuah 2020) | Number of services per patient per year |
|---|---|---|
| Endoscopy | 445 | 0.201 |
| Colonoscopy | 328 | 0.148 |
| GI imaging | 213 | 0.096 |
| Unscheduled GP/ED/Hospitalisation visits | 229 | 0.104 |
Table 2: Health services per patient per year.
The costs of medical services utilised as follows endoscopy from Quach, et al. [33]. We assumed the cost of colonoscopy to be the same as endoscopy. Cost of GI imaging was taken from Nguyen, et al. a cohort study of out-of-pocket costs associated with hospitalised injuries in Vietnam. Lastly, the cost of hospitalisation/GP visits/ED visits was from a KOL survey provided by Abbott. The cost per patient per year was calculated by multiplying the cost of each service with the projected number of services per patient per year (Table 3).
| Service | Cost per service | Total costs per patient per year |
|---|---|---|
| Endoscopy | VND 785,000 | VND 158,066 |
| Colonoscopy | VND 785,000 | VND 116,507 |
| GI imaging | VND 300,000 | VND 28,914 |
| Unscheduled GP/ED/Hospitalisation visits | VND 230,000 | VND 23,833 |
Table 3: Cost of health services.
Scenario Analysis
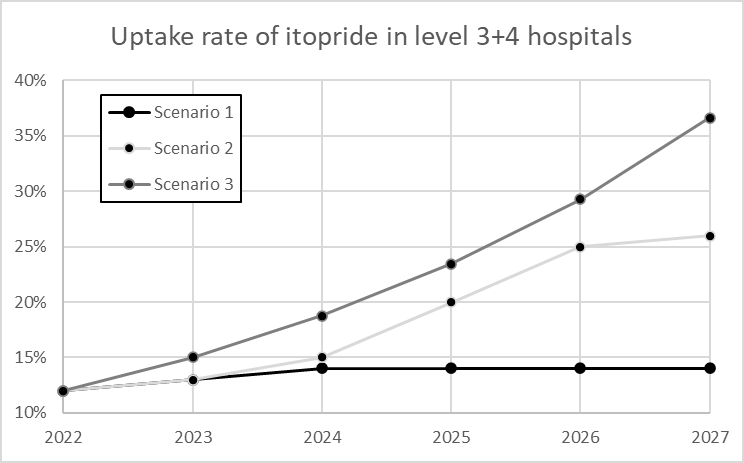
The implication for the payer is assessed by analysing different scenarios (Figure 3). The scenarios are: Current scenario: itopride not reimbursed for level 3+4 hospitals. Alternative scenario 1: itopride reimbursed for level 3+4 hospitals and a flat market uptake (base case). Alternative scenario 2: itopride reimbursed for level 3+4 hospitals and a somewhat liberal market uptake. Alternative scenario 3: itopride reimbursed for level 3+4 hospitals and high/increasing market uptake.
Sensitivity analyses are performed by varying the variables described above by +/- 25%.
Results
Current Scenario
It is estimated that there are 760,238 patients who qualify for prokinetic treatment in 2023. This is set to increase to 774,666 in 2027. Of the 576,630 who qualify for prokinetic treatment 151,931 is estimated to receive itopride and 453,373 domperidone in level 1+2 hospitals. A total of 151,326 untreated patients are estimated to be seen in level 3+4 hospitals (Table 4).
| Patient numbers | 2023 | 2024 | 2025 | 2026 | 2027 |
|---|---|---|---|---|---|
| Base population | 68,074,158 | 68,397,146 | 68,720,135 | 69,043,124 | 69,366,112 |
| Prevalence | 10,211,124 | 10,259,572 | 10,308,020 | 10,356,469 | 10,404,917 |
| Un-investigated | 1,356,842 | 1,363,279 | 1,369,717 | 1,376,155 | 1,382,593 |
| Patients investigated | 8,854,282 | 8,896,292 | 8,938,303 | 8,980,314 | 9,022,324 |
| Diagnosed | 4,873,318 | 4,896,440 | 4,919,562 | 4,942,684 | 4,965,806 |
| Patients seeking treatment | 2,534,125 | 2,546,149 | 2,558,172 | 2,570,196 | 2,582,219 |
| Patients qualifying for prokinetic treatment | 760,238 | 763,845 | 767,452 | 771,059 | 774,666 |
| Level 1+2 hospitals | |||||
| Domperidone | 455,534 | 457,696 | 459,857 | 462,018 | 464,180 |
| Itopride | 152,656 | 153,380 | 154,104 | 154,829 | 155,553 |
| Level 3+4 hospitals | |||||
| Untreated patients | 152,048 | 152,769 | 153,490 | 154,212 | 154,933 |
| Domperidone | - | - | - | - | - |
| Itopride | - | - | - | - | - |
Table 4: Current scenario: Patient numbers.
It is estimated that a total of 770,521 patients are going to be treated with itopride over the 5-year period from 2023 to 2027.
Current estimated drug costs are estimated to be VND 136,416,724,554 in 2022 which will rise to VND
139,668,405,925 in 2027. Of these the current amount of funds spent on itopride is VND 67,333,564,284 which amounts to approximately 49% of the total drug costs. Over the 5-year period from 2023 to 2027 the total cost of itopride is estimated to be VND 341,482,787,465. Costs by year is reported in Table 5.
| Drug costs (VND) | 2023 | 2024 | 2025 | 2026 | 2027 |
|---|---|---|---|---|---|
| Level 1+2 hospitals | |||||
| Domperidone | 69,412M | 69,742M | 70,071M | 70,401M | 70,730M |
| Itopride | 67,655M | 67,976M | 68,297M | 68,618M | 68,939M |
| Level 3+4 hospitals | |||||
| Domperidone | - | - | - | - | - |
| Itopride | - | - | - | - | - |
| Total costs | 137,067M | 137,717M | 138,368M | 139,018M | 139,668M |
| Health resource costs (VND) | 2023 | 2024 | 2025 | 2026 | 2027 |
| Level 1+2 hospitals | |||||
| Domperidone | 126,739M | 127,341M | 127,942M | 128,543M | 129,145M |
| Itopride | 42,472M | 42,674M | 42,875M | 43,077M | 43,278M |
| Level 3+4 hospitals | |||||
| Untreated patients | 49,768M | 50,004M | 50,240M | 50,476M | 50,716M |
| Domperidone | - | - | - | - | - |
| Itopride | - | - | - | - | - |
| Total costs | 218,979M | 220,018M | 221,057M | 222,096M | 223,135M |
Table 5: Current scenario: Drugs costs.
The cost of health resources is estimated to be VND 218,979M in 2023 which is set to increase to VND 223,135M in 2027. Itopride treated patients account for less than 20% of the estimated health resource costs with VND 42,272M in 2023 and VND 43,278M in 2027 see Table 6 for further details.
Total current costs for the treatment of functional dyspepsia in level 1+2 as well as level 3+4 hospitals is estimated to be VND 356,046M in 2023 and VND 362,804M in 2027 (Table 7).
| Total budget (VND) | 2023 | 2024 | 2025 | 2026 | 2027 |
|---|---|---|---|---|---|
| Level 1+2 hospitals | |||||
| Drugs costs | 137,067M | 137,717M | 138,368M | 139,018M | 139,668M |
| Health resource costs | 169,211M | 170,014M | 170,817M | 171,620M | 172,423M |
| Level 3+4 hospitals | |||||
| Drugs costs | - | - | - | - | - |
| Health resource costs | 49,768M | 50,004M | 50,240M | 50,476M | 50,716M |
| Total costs | 356,046M | 357,736M | 359,425M | 361,114M | 362,804M |
Table 6: Current scenario: Total costs.
Financial Implications of the Alternative Scenarios
The financial implications with each alternative scenario can be found in (Table 1).
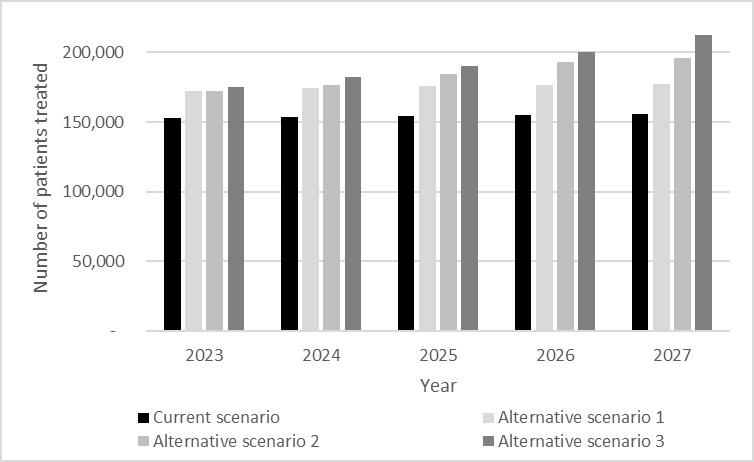
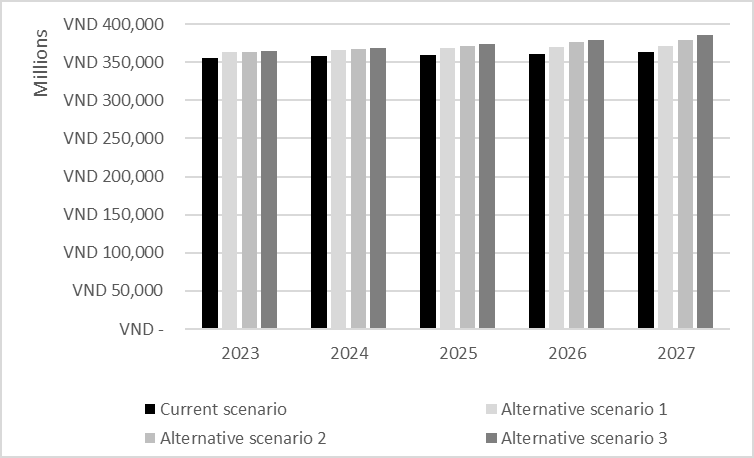
Number patients over time by scenario is depicted in Figure 4. Alternative scenario 1 will result in an increase of 13.7% patients over the 5-year period however, the increase in spending is only 2.3%. Similarly for alternative scenarios 2 and 3: increase in itopride use is 19.8% to 24.6% with spend only increasing 3.3% to 4.2%. The net costs are estimated to be between VND 363,836M (Alternative scenario 1) and VND 365,034M (Alternative scenario 3) in 2023, gradually growing to VND 371,351M (Alternative scenario 1) and VND 385,163M (Alternative scenario 3) in 2027 (Figure 5).
Alternative Scenario 1
In alternative scenario 1 the update take of itopride is assumed to only rise slightly from 13% in 2023 to 14% in 2027. A total of 19,766 patients are estimated to be treated with itopride in 2023 in level 3+4 hospitals. This number is projected to increase to 21,691 in 2027. The estimated drug costs in alternative scenario 1 are estimated to be VND 145,827M in 2023 which will rise to VND 149,281M in 2027. Of these the funds spent on itopride is VND 76,415M in 2023 and VND 78,551M in 2027 which amounts to 52%- 53% of the total drug costs. Over the 5-year period from 2023 to 2027 the total cost of itopride is estimated to be VND 463,807M. The cost of health resources is estimated to be VND 218,009M in 2023 which is set to increase to VND 222,070M in 2027. Itopride treated patients account for 22% of the estimated health resource costs with VND 47,971M in 2023 and VND 49,313M in 2027.
Alternative Scenario 2
In alternative scenario 2 the update take of itopride is assumed to grow from 13% in 2023 to 26% in 2027. A total of 19,766 patients are estimated to be treated with itopride in 2023 in level 3+4 hospitals. This number is projected to increase to 40,283 in 2027. The estimated drug costs in alternative scenario 2 are estimated to be VND 145,827M in 2023 which will rise to VND 157,521M in 2027. Of these the funds spent on itopride is VND 86,791M in 2023 which amounts to 55% of the total drug costs. Over the 5-year period from 2023 to 2027 the total cost of itopride is estimated to be VND 484,324M. The cost of health resources is estimated to be VND 218,009M in 2023 which is set to increase to VND 221,158M in 2027. Itopride treated patients account for
22%-25% of the estimated health resource costs with VND 47,971M in 2023 and VND 54,486M in 2027.
Alternative Scenario 3
In alternative scenario 3 the update take of itopride is assumed to grow from 13% in 2022 to 37% in 2027. A total of 19,766 patients are estimated to be treated with itopride in 2023 in level 3+4 hospitals. This number is projected to increase to 56,738 in 2027. The estimated drug costs in alternative scenario 3 are estimated to be VND 145,827M in 2023 which will rise to VND 164,814M in 2027. Of these the funds spent on itopride is VND 94,084M which amounts to 57% of the total drug costs. Over the 5-year period from 2023 to 2027 the total cost of itopride is estimated to be VND 500,778M. The cost of health resources is estimated to be VND 218,009M in 2023 which is set to increase to VND 220,350M in 2027. Itopride treated patients account for 27% of the estimated health resource costs with VND 59,069M in 2027.
Sensitivity Analysis
The sensitivity analysis showed that duration of treatment and variables that influence the final number of patients who receive prokinetic treatment are the main drivers of the financial impact. The difference ranges from VND 30,006M to VND 53,479M for alternative scenario 1, from VND 43,121M to VND 76,851M for alternative scenario 2 and from VND 53,639M to VND 95,596M for alternative scenario 3 (Figure 6).
a) Alternative scenario 1
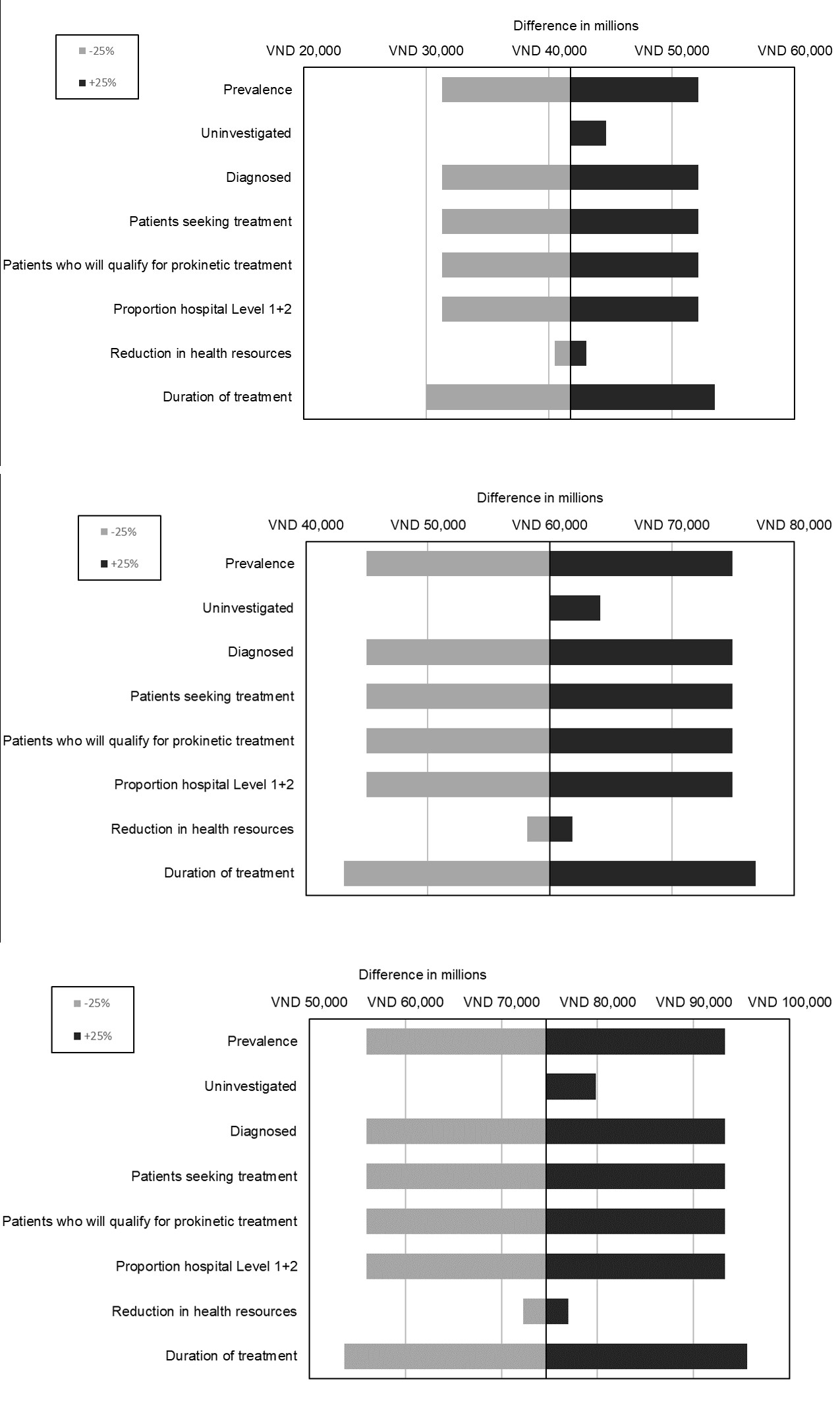
b) Alternative scenario 2
c) Alternative scenario 3
Discussion
This analysis examined the potential budgetary impact of expanding access to for level 3+4 hospitals in Vietnam. The model included both drug costs and healthcare resource utilization costs. In the base case scenario model, it assumes the base population (itopride not reimbursed for level 3+4 hospitals) treated with itopride to be 779,000. The base case cumulative net spend on Itopride is estimated to be VND 1,797,125M over 5 years.
Three alternative scenario analyses were undertaken using the model and these were 1) flat market uptake, 2) liberal market uptake, and 3) high/increasing market uptake. All three scenarios demonstrate a net budget impact range from VND 41,743M to VND 74,617M cumulative net spend on itopride (2.3% to 4.2% increase drug cost spend) over 5 years. This is considering both the drug costs of itopride and direct medical costs from the Vietnamese government payer perspective. Assuming the high market uptake scenario would only result in a 4.2% increase in overall net spend, and an increase of access treatment to an additional 195,023 patients cumulative over 5 years. Thus, within the context of Vietnamese healthcare budget, this investment would allow more patients to gain access to an efficacious treatment for functional dyspepsia who are mostly in more improvised and rural areas of Vietnam (level 3+4 hospitals).
There are different limitations related to this study. The analyses relied upon several assumptions as well as data availability. Key inputs such as prevalence of functional dyspepsia in Vietnam and proportion of patients treated for functional dyspepsia in Vietnam were based on values reported in non-Vietnamese settings and published clinical trials, many of which were conducted as multinational studies. Another limitation is that clinical inputs specific to the population of patients suffering from functional dyspepsia do not presently exist. However, while data gaps preclude investigating possible implications, this limitation is not expected to bias the results of the analysis, since the same consideration could apply to many of the interventions included in the study.
Through the sensitivity analysis of all scenarios confirmed that the main drivers of cost in the model to be the patient numbers (prevalence, diagnosed, uptake), and duration of treatment. A small cost-saving of VND 49,098 (health resource cost) per patient from reduction of health services when symptom free or experience symptom improvement. However, this does not appear to heavily affect overall financial impact. From the Vietnamese Government budgetary perspective, the financial impact of expanding funding of itopride into level 3+4 hospitals is unlikely to result in a significant financial impact. This was evidenced by the three different scenarios.
Studies examining the budget impact of pharmaceutical investments in Vietnam is limited. One example by Tran, et al. examining the Budget Impact Analysis of Erlotib in Vietnam demonstrated that the funding of this oncology agent would cost the Vietnamese Government 107.8 billion VND.
Functional dyspepsia is a chronic condition and often incurable with significant financial impacts on both the patients and wider healthcare system. Itopride is a relatively inexpensive prokinetic used commonly in Asia. Although some of the clinical evidence for prokinetics in functional dyspepsia is mixed, it should be noted that most of these studies were conducted on western patients (mostly Caucasian) and a significant proportion had already been treated with other agents. The research from Asian literature suggests that the sub-condition affecting East and South Asian populations is postprandial distress syndrome. Logically, prokinetics such as itopride should be more beneficial for PDS, and this is substantiated by the 2012 Asian consensus report and the 2023 Asian-Pacific guidelines and real-life purchasing data from these regions.
Conclusion
Itopride has a unique dual MOA on esophagus and stomach to promote gastric motility and helps patients restore their gastric natural tone. Itopride increases lower esophageal sphincter pressure, accelerates gastric emptying and improves gastroduodenal coordination and does not prolong QT Interval that is devoid of extrapyramidal side effects. As such the broadening of the reimbursement of itopride to include level 3+4 hospitals will provide benefit for between 13.7% (105,923) to 24.6% (89,343) more patients at only 3.3% (VND 41,742M) to 4.2% (VND 74,617M) additional costs over five years. Itopride is deemed to represent great benefit for patients suffering from functional dyspepsia in Vietnam.
Funding
This study was funded by Abbott Products Operations AG, Basal, Switzerland
References
-
Mounsey A, Barzin A, Rietz A (2020) Functional Dyspepsia: Evaluation and Management. Am Fam Physician 101(2): 84-88.
-
Ford AC, Forman D, Bailey AG, Axon AT, Moayyedi P (2012) Effect of Dyspepsia on Survival: A Longitudinal 10-Year Follow-Up Study. Am J Gastroenterol 107(6): 912-921.
-
Rome IV Criteria Appendix A: Rome IV Diagnostic Criteria for FGIDs: Gastroduodenal Disorders. The Rome Foundation.
-
Mahadeva S, Goh KL (2006) Epidemiology of Functional Dyspepsia: A Global Perspective. World Journal of Gastroenterology 12(17): 2661-2666.
-
Arnaout AY, Alhejazi TJ, Nerabani Y, Hamdan O, Arnaout K, et al. (2023) The Prevalence and Risk Factors of Functional Dyspepsia among Adults in Low- and Middle- Income Countries: An International Cross-Sectional Study. Medicine (Baltimore) 102(40): e35437.
-
Ghoshal UC, Singh R, Chang FY, Hou X, Wong BC, et al. (2011) Epidemiology of Uninvestigated and Functional Dyspepsia in Asia: Facts and Fiction. J Neurogastroenterol Motil 17(3): 235-244.
-
Lee K, Kwon CI, Yeniova A, Koyanagi A, Jacob L, et al. (2024) Global Prevalence of Functional Dyspepsia According to Rome Criteria, 1990-2020: A Systematic Review and Meta-Analysis. Sci Rep 14(1): 4172.
-
Sperber AD, Bangdiwala SI, Drossman DA, Ghoshal UC, Simren M, et al. (2021) Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 160(1): 99-114.e3.
-
Miwa H, Ghoshal UC, Fock KM, Gonlachanvit S, Gwee KA, et al. (2012) Asian Consensus Report on Functional Dyspepsia. J Gastroenterol Hepatol 27(4): 626-641.
-
Ford AC, Bercik P, Morgan DG, Bolino C, Pintos-Sanchez MI, et al. (2014) The Rome III Criteria for the Diagnosis of Functional Dyspepsia in Secondary Care are Not Superior to Previous Definitions. Gastroenterology 146(4): 932-940.
-
Fang Y, Liou J, Chen C, Lee J, Hsu Y, et al. (2015) Distinct Aetiopathogenesis in Subgroups of Functional Dyspepsia According to the Rome III criteria. Gut 64(10): 1517- 1528.
-
Oh JH, Kwon JG, Jung HK, Tae CH, Song KH, et al. (2020) Clinical Practice Guidelines for Functional Dyspepsia in Korea. Journal of Neurogastroenterology and Motility 26(1): 29-50.
-
Gwee KA, Lee YY, Suzuki H, Ghoshal UC, Holtmann G, et al. (2023) Asia-Pacific Guidelines For Managing Functional Dyspepsia Overlapping With Other Gastrointestinal Symptoms. J Gastroenterol Hepatol 38(2): 197-209.
-
Talley NJ, Ford AC (2015) Functional Dyspepsia. New England Journal of Medicine 373(19): 1853-1863.
-
Ford AC, Marwaha A, Lim A, Moayyedi P (2010) What is the Prevalence of Clinically Significant Endoscopic Findings in Subjects with Dyspepsia? Systematic Review and Meta-Analysis. Clinical Gastroenterology and Hepatology 8(10): 830-7.e2.
-
Kim BJ, Kuo B (2019) Gastroparesis and Functional Dyspepsia: A Blurring Distinction of Pathophysiology and Treatment. Journal of Neurogastroenterology and Motility 25(1): 27-35.
-
Pittayanon R, Yuan Y, Bollegala NP, Khanna R, Lacy BE, et al. (2019) Prokinetics for Functional Dyspepsia: A Systematic Review and Meta-Analysis of Randomized Control Trials. Am J Gastroenterol 114(2): 233-243.
-
Quach DT, Ha QV, Nguyen CT, Le QD, Nguyen DT, et al. (2022) Overlap of Gastroesophageal Reflux Disease and Functional Dyspepsia and Yield of Esophagogastroduodenoscopy in Patients Clinically Fulfilling the Rome IV Criteria for Functional Dyspepsia. Front Med (Lausanne) 9: 910929.
-
Nguyen TKT, Cheng TM (2014) Vietnam’s Health Care System Emphasizes Prevention and Pursues Universal Coverage. Health Affairs 33(11): 2057-2063.
-
Sullivan SD, Mauskopf JA, Augustovski F, Jaime Caro J, Lee KM, et al. (2014) Budget Impact Analysis-Principles of Good Practice: Report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value in Health 17(1): 5-14.
-
Bank W (2022) Population Ages 15-64, Total - Vietnam. World Bank Group.
-
Li XB, Liu WZ, Ge ZZ, Zhang DR, Zhao YJ, et al. (2005) Analysis of Clinical Characteristics of Dyspeptic Symptoms in Shanghai Patients. Chin J Dig Dis 6(2): 62- 67.
-
Kwan AC, Bao T, Chakkaphak S, Chang FY, Ke M, et al. (2003) Validation of Rome II Criteria for Functional Gastrointestinal Disorders by Factor Analysis of Symptoms in Asian Patient Sample. J Gastroenterol Hepatol 18(7): 796-802.
-
Kawamura A, Adachi K, Takashima T, Murao M, Katsube T, et al. (2001) Prevalence of Functional Dyspepsia and its Relationship with Helicobacter Pylori Infection in a Japanese Population. J Gastroenterol Hepatol 16(4): 384-388.
-
Kim J, Lee K, Kim JH, Hahm K, Cho S (2004) Functional Gastrointestinal Disorders in Patients Referred to Specialist Gastroenterologists in a Tertiary Hospital. J Neurogastroenterol Motil 10(2): 111-117.
-
Ji SW, Park HJ, Choi JP, Lee TH, Lee DY (2003) Validation of Rome II Criteria for Functional Gastrointestinal Disorders in Korean Patients. Korean J Gastroenterol 41(3): 183-189.
-
Noh YW, Jung HK, Kim SE, Jung SA (2010) Overlap of Erosive and Non-erosive Reflux Diseases with Functional Gastrointestinal Disorders According to Rome III Criteria. J Neurogastroenterol Motil 16(2): 148-156.
-
Mahadeva S, Chia YC, Vinothini A, Mohazmi M, Goh KL (2008) Cost-Effectiveness of and Satisfaction with a Helicobacter Pylori “Test and Treat” Strategy Compared with Prompt Endoscopy in Young Asians with Dyspepsia. Gut 57(9): 1214-1220.
-
Wai CT, Yeoh KG, Ho KY, Kang JY, Lim SG (2002) Diagnostic Yield of Upper Endoscopy in Asian Patients Presenting with Dyspepsia. Gastrointest Endosc 56(4): 548-551.
-
Teo HS, Huong DL (2020) Improving Efficiency in the Health Sector.
-
(2022) Ministry of Health. Drug Price Lookup.
-
Chuah KH, Cheong SY, Lim SZ, Mahadeva S (2022) Functional Dyspepsia Leads to More Healthcare Utilization in Secondary Care Compared with Other Functional Gastrointestinal Disorders. J Dig Dis 23(2): 111-117.
-
Quach DT, Ho QD, Vu KV, Vu KT, Tran HV, et al. (2020) Improving Efficacy of Endoscopic Diagnosis of Early Gastric Cancer: Gaps to Overcome from the Real-World Practice in Vietnam. Biomed Res Int.
- Measuring What Matters: Data Gaps, Certificate of Need Reform, and Pediatric Psychiatric Inpatient Capacity in North Carolina
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal