Anti-Hypertensive Medication Adherence and Associated Factors among Adult Hypertensive Patients at Dilla University Referral Hospital, South Ethiopia
Background: Hypertension is a global public health challenge that contributes to the burden of hypertensive heart disease, stroke, renal failure, premature morbidity, and mortality. The availability of effective antihypertensive medications didn’t bring expected outcomes in terms of adherence for antihypertensive medication. Objective: The aim of this study was to assess antihypertensive medication adherence and associated factors among adult hypertensive patients at Dilla university referral hospital, Southern Ethiopia, 2021. Methods: A hospital-based cross-sectional study was conducted, at Dilla University Referral Hospital from June 10, 2021, to July 10, 2021, and 205 study participants were selected from the study population using a systematic random sampling procedure. Patients in the study were interviewed while their medical records were reviewed using a data abstraction sheet. Adherence was assessed using an eight-item Morisky Medication adherence scale (MMAS-8); a MMAS-8 score of less than 6 was considered non-adherence, and a MMAS-8 score greater than or equal to 6 was considered adherence. Factors associated with adherence were identified using binary and multivariate logistic regression analyses. The crude odds ratio and adjusted odds ratio with a 95% confidence interval were calculated using SPSS version 20. Variables with a P-value <0.05 in the multivariable analysis were assumed to be statistically significant factors. Results: 205 respondents were interviewed, with a response rate of 100%. More than half (57.6%) of the study participants were male. 65.3% (58.784–71.816) of the study participants were found to be adherent to their medication. Longer Duration of diagnosis of hypertension (AOR =0.280, 95% CI = 0.025–0.836), participants who can’t read and write (AOR = 0.40, 95% CI = 0.00-0840), and traditional drug users (AOR =0.15, 95% CI =0.003-0.489) were inversely significant associated with antihypertensive medication adherence. Conclusion: An adhesion level of 65.3% was found to be suboptimal. Traditional drug users, being uneducated and the duration of the diagnosis of hypertension were adversely influencing medication adherence. Therefore, routine health education and awareness creation are strongly recommended
Introduction
Hypertension is known as the “silent killer” since it frequently has no warning signs or symptoms, and many people are unaware they have it [1]. Most individuals find out they have it by coincidence when they are hospitalized for an unrelated disease or are exposed to pre-employment or pre-operative medical testing. Although the specific causes of high blood pressure are unknown, a multitude of variables and situations have a part in its development [2]. Medication adherence or compliance is defined as “the act of adhering to the provider’s advice regarding the timing, dosage, and frequency of medication adherence” [3].
As there is no cure for hypertension, patients are expected to take medications for the rest of their lives. Hypertension medication treatment necessitates that patients take their medication exactly as prescribed [4]. Adherence to pharmacological therapy and adaptation to necessary lifestyle adjustments has been found to be particularly effective in hypertension control, with the following benefits for individuals, healthcare systems, and society at large: it improves quality of life and reduces complications and mortality. It is also a cost-cutting approach because it lowers the possibility of complications [5].
Non-communicable diseases (NCDs) are the leading causes of death globally, killing more people each year than all other causes combined [1]. According to World Health Organization reports from 2015 and 2016, NCDs were responsible for 40 million deaths and more than 70% of global mortality, respectively. More than 40% of these deaths could have been avoided by increasing antihypertensive medication adherence, and in low and middle-income countries it account for 80% of NCD deaths [6, 7, 8]. The prevalence of hypertension has increased dramatically in Sub-Saharan Africa over the last two to three decades. The number of adults with hypertension in Sub-Saharan Africa was estimated to be around 80 million in 2000, with a projected increase to 150 million by 2025. Hypertension is one of the most common risk factors for cardiovascular disease in Sub-Saharan Africa (CVD). If nothing is done, by 2020, hypertension would be responsible for three-quarters of all fatalities in Africa [7].
In 2011, the Southern Nations, Nationalities, and Peoples
Region (SNNPR) had a hypertension prevalence of roughly 10% [8].
Adherence is the extent to which a person’s behavior- taking medication, following a diet, and/or executing lifestyle changes corresponds with agreed recommendations from a health care provider [9, 10].
Therefor this study was sought to identify the prevalence and associated factors among adult hypertensive patients at Dilla General Hospital.
Methods and Materials
Study Area
The research was carried out at Dilla University Referral Hospital, which is located in Dilla town, the administrative center of the Gedeo zone in Ethiopia’s Southern Ethiopia. DURH is a teaching and referral hospital with a catchment population of approximately 5 million people. It primarily serves patients from the Gedeo zone, as well as some areas of the Sidama region and west Guji zone. Internal medicine, surgery, obstetrics and gynecology, and pediatrics are all available at the hospital. It also has a psychiatry ward, an orthopedics ward, ophthalmology, dermatology, and other services.
Study Period
Study was conducted from June 10, 2021 to July 10, 2021.
Study Design
Institution based cross-sectional study design was conducted.
Source Population
All hypertensive patients who were attending for treatment follow up at chronic illness clinic at Dilla University Referral Hospital.
Study Population
All adult hypertensive patients, who were on antihypertensive medications and on, follow up at Dilla University Referral Hospital.
Eligibility Criteria
Inclusion Criteria: All adult hypertensive patients who were aged 18-years and above, who were on antihypertensive medications and on follow up at Dilla University Referral Hospital for at least six months before study period.
Exclusion criteria: All hypertensive patients who were critically ill and unable to respond during the data collection period.
Sample Size Determination
Sample size was determined by using single population proportion formula final sample size for this study was 205 [11, 12, 13]. Sampling Technique Systematic random sampling technique was conducted. Study Variables Dependent variable: Antihypertensive medication adherence (Yes/No). Independent variables
- Socio-demographic factors: (age, sex, educational status, occupation, marital status, family support and residence).
- Clinical factors: (Duration of diagnosis of HTN, duration of treatment, comorbidity, number of drugs, dosage frequency, number of pills taken per day, side effects of drug and cost of medication).
- Patient related factors: (Family history of hypertension, forgetfulness, negligence, traditional drug use and knowledge about hypertension).
- Health care related factors: (Patient provider relationship, distance of hospital from home and availability of quality service).
Data Collection Tools and Procedure
Face-to-face interview with a pretested structured questionnaire was conducted to collect the socio- demographics, drug related factors, health care related factors, and patient related characteristics. Face to face interview was employed using two trained clinical nurses, who work at other departments of hospital. Data on co- morbidities, Antihypertensive medication(s) and three isolated BP measurements was extracted from medical records of patients using a pretested data abstraction format. An eight item Morisky’s Medication Adherence Scale was employed to assess the study participant’s medication adherence. It is a self-report questionnaire with a total of 8 items. Items from 1 through 7 are dichotomous based on “Yes” or “No” response. Concerning scoring of these items each ‘No” response was rated as ‘‘1” and each ‘‘Yes” was rated as ‘‘0” except for item 5, in which case, a ‘Yes’ response was rated as ‘‘1” and a ‘‘No” was rated as ‘‘0”. The last item (item8) had a 5-point Liker response choice. The choices were never, once in a while, sometimes, usually, and all of the time. The score for each choice respectively were 1, 0.75, 0.50, 0.25, and 0. The total score of all the 8 items ranges from 0 to 8 points and it can be categorized into three levels of adherence (the cut –off points): ‘high adherence’ (score = 8), ‘medium adherence’ (score of 6 to <8 ), and ‘low adherence’ (score < 6) [10, 14].
Data Quality Control
To maintain validity of data collection tool, structured questionnaire was developed in English and translated to local languages (Amharic and Gedeoffa) and back translated to English. During data collection supervision was carried out by principal investigator. To assure data quality, pretest was conducted; data collectors were recruited; training and orientation was given to data collectors. Completed questionnaires were checked every day after data collection for completeness, clarity and consistency. Any error identified during data entry was corrected after revision of the original completed questionnaire.
Data Processing and Analysis
Data was checked manually for completeness and then coded. Data was entered, cleaned and recorded to analyze using SPSS version 20. Descriptive statistics was used using frequency, percentage, mean and standard deviation. Binary logistic regression statistical modeling was used to identify associated factors. In Bivariable logistic regression, those variables with a p-value <0.25 were candidates for multivariable logistic regression. The association between dependent and independent variables was assessed, and its strength, direction, and significance were presented using odds ratios and 95% confidence intervals. Finally, the result was presented by text, graph, and table.
Operational Definitions
- Hypertension: According to the WHO, hypertension is defined as “a persistent raised systolic or diastolic blood pressure equal to or more than 140/90 mmHg in adults aged 18 years and over” [15].
- Adherence: Is defined as “the extent to which a person’s behavior- taking medication, following a diet, and/or executing lifestyle changes corresponds with agreed recommendations from a health care provider” and adherence was considered when the patient’s MMAS-8 score is ≥ 6 but Any form of deviation from adherence like losing one appointment, missing doses and when MMAS-8 score was less than 6 was considered non- adherence [9, 10, 16].
- Controlled BP: defined as the achievement of an average three BP readings <140/90 mmHg for age <60 years and <150/90 mmHg for age ≥60 years in individuals being treated for HTN [9, 17].
- Uncontrolled BP: average three BP readings >= 140/90 mmHg for age <60 years and >= 150/90 mmHg for age ≥60 years in individuals being treated for HTN [9, 18].
- Knowledge about Hypertension: Assessed using six-item questions and computing the mean value. Respondents who scored above the mean for the knowledge questions were classified as having good knowledge; otherwise, they did not [12, 19].
• Patient Provider Relationship: Participants who score above the mean for questions prepared on patient provider relationships in the treatment and care of hypertension patients have a good patient-provider relationship; otherwise, they do not [13, 20].
Ethical Consideration
Ethical clearance was obtained from the Research and Ethics Committee Dilla University, college of medicine and health sciences and official letter was obtained from school of medicine prior to data collection. Verbal and written consent was obtained for willingness of patients to participate. The patient’s privacy was maintained by conducting the interview in a private place and they were informed that there won’t be any incentive or harm for their participation in this study. Finally, participant identity was kept anonymous throughout the data collection and analysis process.
Results
Socio-Demographic Characteristics
In this study a total of 205 participants were interview and making a response rate of 100 %. More than half, 118(57.6%) of study participants were male. Regarding age group, majority of the respondents, 75 (36.6%) were between the age group of 55 and 64 years and 8 (3.9%) of the respondents were between age group of 18-334. Greater than three-fourth, 156(76.1%) of the participants were married, while 18 (8.8%) of the respondents were divorced. Concerning educational status, 68(33.2%) of respondents were completed college/university education level, while 36 (17.6 %) of participants can’t read and write. More than half, 135 (65.9%) of respondents had family support. Majority of participants, 193 (94.2%) were residing urban area (Table 1).
| Variables Category | Frequency | Percentages (%) | |
|---|---|---|---|
| Age | 18-34 | 8 | 3.9 |
| 35-44 | 33 | 16.1 | |
| 45-54 | 59 | 28.8 | |
| 55-64 | 75 | 36.6 | |
| 65 and above | 30 | 14.6 | |
| Sex | Male | 118 | 57.6 |
| Female | 87 | 42.4 | |
| Marital status | Single | 13 | 6.3 |
| Married | 156 | 76.1 | |
| Divorced | 18 | 8.8 | |
| widowed | 18 | 8.8 | |
| Educational status | Can’t read and write | 36 | 17.6 |
| Primary school | 44 | 21.5 | |
| Secondary school | 57 | 27.8 | |
| College/university | 68 | 33.2 | |
| Family support | Yes | 135 | 65.9 |
| No | 70 | 34.1 | |
| Residence | Rural | 12 | 5.8 |
| Urban | 193 | 94.2 |
Table 1: Frequency and percentage distribution of socio demographic characteristics of adult hypertensive patients on chronic fol
Comorbidities of Adult Hypertensive Patients
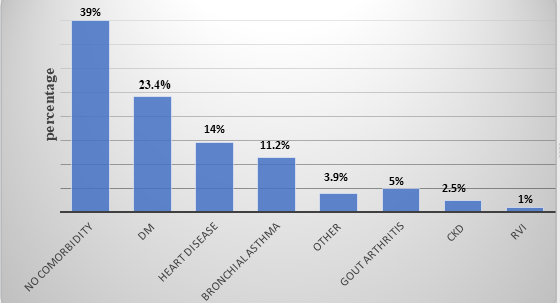
Comorbidity has been noted as a potential barrier to proper adherence to antihypertensive medications. More than half of 80(39%) patients have not history of comorbidities. The most common comorbid conditions were diabetes mellitus (48patients,23.2%), Heart disease (29patients,14%), Bronchial asthma (23 patients,11.2%), Gout arthritis (10 patients,5%),CKD (5 patients,2.5%), RVI (2patients,1%), Others (8 patients, 3.9%) (Figure 1).
Knowledge and Patient Related Characteristics
Regarding family history of hypertension, 55(26.8%) of the respondents had family history of hypertension, while the rest hadn’t. Majority of participants, 165(80.5%) of them had follow up visit once every month, while 26 (12.7%) of them visit once in two or more months and 14(6.8%) of them once in less than one month. From total of study participants who had irregular follow up due to patient related factors,91 (44.4 %) of them were due to forgetfulness while 12(5.9%) were due to negligence. From study subjects, 28(13.7%) of them uses traditional drugs to treat hypertension, whereas the rest not. 19(9.3%) of the respondents use ‘Shiferaw’ as traditional drug to treat hypertension while 9 (4.4%) use other.
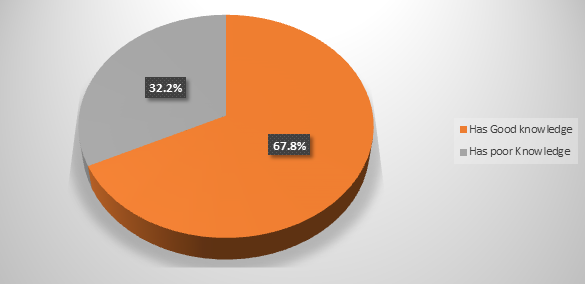
Concerning knowledge about hypertension and its treatment, 139(67.8%) of respondents know the term hypertension, and 141(68.8%) of participants reported hypertension as extremely sever disease, whereas 17(8.3%) of subjects reported it as less sever disease. From the study participants, 164(80%) of them know the normal level of BP, of this all of them reported 120/80 mmgh as normal level of BP. Among the study subjects 145(70.7%) of them know increase in body weight is a risk factor for hypertension, whereas 133(64.9%) of them reported uncontrolled hypertension can leads to stroke. 191(93.25) of respondents know lowering high blood pressure has impact to improve health, whereas only 3(1.5%) said it can’t improve health, while 189(92.2%) of participants reported people with hypertension need to take their medication though they exercise well, whereas the rest reported it as unnecessary. Accordingly, 139 (67.8%) of the respondents scored above mean for the six-item knowledge about hypertension and its treatment questions and labeled as having good knowledge, whereas, 66(32.2%) of participants scored mean and below mean and labeled as having poor knowledge (Figure 2).
Health Care Related and Relationship Characteristics
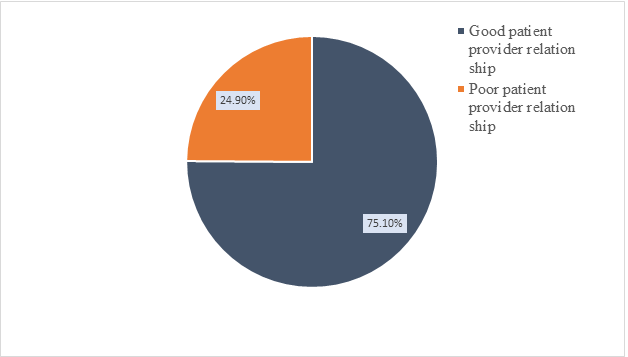
Regarding time it takes to travel from home to hospital, for 28(13.7%) of the participants it takes one hour and more on a single trip to reach to the hospital, while for 102(49.8%) of respondents, it takes greater than thirty minutes but less than one hour and 75(36.6%) of study subjects reported it take thirty minutes and less time to arrive at hospital. Concerning waiting time to get treatment after arrival to the hospital, 138(67.3%) of the respondents wait for one to two hours duration, while 36(17.6%) of the study subjects reported they wait for three and more hours and 31 (15.1%) of participants reported they wait for less than an hour.153 (74.6%) of participants reported their physicians devote their time to them. Three-fourth of the respondents, 155(75.6%) reported their physicians understand them. Majority of study participants, 196(95.6%) of them trust their physicians, similarly 196(95.6%) of respondents agree with their physicians about their treatment. Accordingly, 154 (75.1%) of the respondents scored above mean for the six-item patient provider relationship questions and labeled as having good patient provider relationship whereas the rest 51(24.9%) of respondents scored mean and below mean, therefore labeled as having poor patient provider relationship (Figure 3).
Medication Adherence Status of the Study Participants
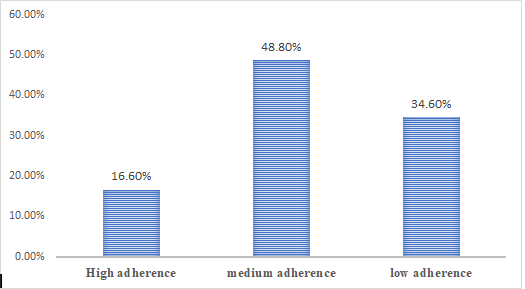
From the study participants, 134 (65.3%) of them were found adherent to their antihypertensive medications, of this 100 (48.8%) of respondents had medium adherence and 34 (16.6%) of them had high adherence. 71 (34.6%) of the study participants were found non-adherent to their medications (had low adherence). The level of adherence was determined by using an eight item Morisky’s Medication adherence scale (MMAS-8). Accordingly, respondents who scored eight Mills KT, et al. [14] on MMAS from the eight adherence related questions labeled as having high adherence, while those who scored six and above but less than eight (MMAS > 6 <8) were labeled as having medium adherence and respondents who scored below six (MMAS <6) were labeled as having low adherence (Figure 4).
Factors Associated with Antihypertensive Medication Adherence
The association of socio-demographic, clinical, patient related and health care related characteristics on adherence status was investigated by using both binary and multivariate logistic regression techniques. Accordingly, all variables were investigated in bivariate analysis. Variables like age, marital status, occupation, educational status, residence, presence or absence of family support, duration of diagnosis, duration of therapy, number of antihypertensive drugs, number of pills, dosage frequency, drug cost, drug side effects, perceived severity of hypertension, knowing normal BP level, trust on physicians, time taken to travel from home to hospital, waiting time at hospital to get treatment after arrival and traditional drug use to treat hypertension had p-value less than 0.25 and became candidate variables for multivariate analysis. The multivariate analysis showed, duration of diagnosis, educational status and traditional drug use were significantly associated with antihypertensive medication adherence (Table 3).
| Variable | Adherent status | ||||
|---|---|---|---|---|---|
| Adherent (%) | Non adherent (%) | COR (95%CI) | AOR (95%CI) | ||
| Age | 18-34 years | 6(75%) | 3(25%) | 1 | 1 |
| 35-44years | 30(85.7%) | 5(14.29%) | 3(0.560-16.071 ) | 0.32(0.023-2.60) | |
| 45-54years | 41(71.9%) | 16(28%) | 1.281(0.285-5.751) | 0.843(0.005-13.60) | |
| 55-64years | 43(58.9%) | 30(41%) | 0.717(0.166-3.093) | 2.933(0.90-9.50) | |
| >= 65 years | 14(40%) | 18(60%) | 0.389(0.082-1.836) | 3.2(0.76-6.87) | |
| Marital status | Single | 10(76.9%) | 3(23.1%) | 1 | 1 |
| Married | 109(69.8%) | 47(30.2%) | 0.696(0.183-2.643) | 3.21(0.7602-5.098) | |
| Divorced | 8 (44.5%) | 10(55,.5%) | 0.240(0.049-1.77) | 0.237(0.003-1.519) | |
| Widowed | 18(61.1%) | 11(38.9%) | 0.491(0.11-2.183) | 1.234(0.569-3.234) | |
| Educational status | Can’t read and write | 13(36.1%) | 23(63.8%) | 0.086(0.032-0.229) | 0.4(0.004-0.840)* |
| Primary school | 15 (34%) | 29(66%) | 0.079(0.031-0.202) | 0.50(0.001-0.194) * | |
| Secondary school | 47(82.4%) | 10(17.6%) | 0.717(0.269-1.908) | 0.06(0.001-1.974) | |
| College/university | 59(86.7%) | 9(13.3%) | 1 | 1 | |
| Family Support | Yes | 96(71.2%) | 39(28.8%) | 1 | 1 |
| No | 70(54.3%) | 32(45.7%) | 0.889(0.508-1.556) | 0.234(0.000-0.345) ** | |
| Duration of diagnosis | < 2 years | 17(65.3%) | 3(34.7%) | 1 | 1 |
| 2-4 years | 29(59.1%) | 10(40.9%) | 0.512(0.123-2.122) | 2.1(0.0156-4.587 | |
| 4-6 years | 39(68.4%) | 18(31.6%) | 0.382(0.099-1.473) | 1.25(0.1423-3.589) | |
| >= 6 years | 33(45.3%) | 40(54.7.%) | 0.146(0.39-0.540) | 0.28(0.025-0.836) | |
| Traditional drug use | Yes | 4(14.2%) | 24(85.8%) | 0.069(0.029-0.183) | 0.15(0.023-0.489) * |
| No | 130(73.4%) | 47(26.65%) | 1 | 1 | |
| Number of drugs | One type | 60(95.2%) | 3(4.8%) | 48(12.145-189.712) | 0.589(0.765-1.567) |
| Two types | 64(59.2%) | 44(40.8%) | 3.491(1.520-8.018) | 0.127(0.047-1.648) | |
| Three and above | 10(29.4%) | 24(70.6%) | 1 | 1 |
Table 3: Results of logistic regression analysis for factors associated with medication adherence among adult hypertensive patien
Discussion
In many developing nations, ensuring patient adherence to antihypertensive therapy in order to prevent consequences remains a serious public health concern. Poor adherence is the single most major cause of uncontrolled hypertension, severe consequences, and resource waste. Several variables influence a patient’s adherence to medicine [12, 15]. According to this study, 65.3 (58.78–71.82) percent of people take their antihypertensive medication. The result of this study was consistent with a study conducted in Gondar, Debrebirihan, North west Ethiopia, and Shashemene, which was 64.6%, 65.2%, and 63.5%, respectively [12]. Debrebrehan 63.5% Tigist Demisew SM, et al. [16], North west Ethiopia 65.2% Hareri A, et al. [17, 21] and Shashemene 63.5% of respondents were reported [11]. This might be due to similarities in the study settings, the economic status of participants, and the same criteria used for measuring medication adherence (MMAS-8). However, this study reports lower adherence than the study done at Black Lion Hospital in Addis Ababa (69.5%) Tibebu A, et al. [2, 22]. This might be due to better access to care and the provision of quality services in this facility. The findings of this study showed a higher adherence level than Adama’s (59.5%) and Jimma 52.9%) Fiseha G, et al. [19, 23]. This variation could be due to differences in subpopulation and measurement tool (Adama used MMAS4, while at this study setting MMAS 8 was used). Another possible reason could be the high sample size used at Jimma compared to this study area (380 vs. 210) and the high number of participants from rural areas at Jimma compared to the current setting (46% vs. 5.8%), which could be a factor in the low level of education and knowledge gaps regarding hypertension and its treatment. In this study, adherence level was lower than the findings of other studies done at Kenya Mueke AT [5, 24] (74%), South Africa Inkster ME, et al. [20, 25] (76%), and Egypt Youssef RM, et al. [21, 26] (77%). This difference could be due to Variations in the studied populations, better health care and access to health facilities in developed countries, and participants’ better knowledge of hypertension and its treatment in the mentioned countries than in the current study area.
Multivariate logistic regression revealed educational status, duration of therapy, and traditional drug use were factors significantly and inversely associated with antihypertensive medication adherence Akhter N [27, 28, 29, 30].
In this study, participants who can’t read and write (AOR = 0.4, 95% CI = 0.004-0.840) were 60% less likely to adhere to antihypertensive medication when compared to participants who completed college or university level. Similarly, respondents who had a primary school level of education (AOR = 0.50, 95% CI = 0.001-0.194) were 50% less likely to adhere than college or university graduates. The findings of this study were supported by the study report of Nejo, et al. [22, 31] where participants who can’t read and write were 95% less likely to be adherent than college completed and Central Ethiopia Daniel G, et al. [23, 32] which reported respondents who can’t read and write were 65 % less likely to be adherent than university graduates. Studies done at Ghana Agbor VN, et al. [4, 33], Nigeria Iloh GUP, et al. [24, 34] and Zambia [21, 35] showed similar findings. This could be due to low awareness about hypertension, its medications, and its treatment. Patients with a higher education level are expected to have better knowledge about disease and therapies and will thus be more compliant with treatments Roth GA [15, 36].
In this study, duration of diagnosis of hypertension had a significant association with antihypertensive medication adherence. Participants who were diagnosed with hypertension six or more years ago (AOR = 0.280, 95% CI = 0.025–0.836) were 72% less likely to adhere to antihypertensive medications when compared with those diagnosed less than two years ago. This finding was in line with studies done in northwestern Ethiopia Mekonnen HS, et al. [18] Southern Ethiopia Giday A, et al. [8] and Jimma Fiseha G, et al. [19] where respondents with diagnosis of hypertension more than 6 years back were 70%, 73% and 69 % less likely to be adherent to antihypertensive medications than their counter parts respectively. This could be due to patients who were diagnosed many years ago being ageing adults with multiple chronic conditions and polypharmacy, which may adversely affect medication adherence. Such patients are highly vulnerable to alteration in memory, Major depression, and dementia, and thus they could forget their doses. However, in a study done in China by Lee, et al. [25, 37]. Lower adherence was correlated with illness durations shorter than five years. These authors link the better adherence in patients who have lived with the disease longer to their better understanding of the illness, better relationship with the prescribing physician, and greater faith in their physician’s advice. This difference between the studies could be due to variations in socioeconomic settings and the quality of health care service provisions.
Other traditional drug use to treat hypertension is significantly associated with antihypertensive medication adherence. This study revealed that participants who used traditional drugs to treat hypertension (AOR = 0.15, 95% CI = 0.023–0.489) were 85% less likely to adhere to antihypertensive medications than their counterparts. This finding was supported by the report of the study done at Adama Terline DMD, et al. [26], where respondents who used traditional drugs to treat hypertension were 62% less likely to be adherent to medications than those who were diagnosed less than two years back. Similarly, study done China Lee
GKY, et al. [25] where hypertensive patients who did not use traditional drugs to treat hypertension were 5.6 times more likely to be adherent to their antihypertensive medications. Another study done among hypertensive patients in twelve low and middle-income Sub-Saharan countries showed similar findings; accordingly, the odds of adherence among hypertensive patients who used traditional drugs were three times more likely than their counterparts [27, 37].
Conclusion
More than half of study participants were found to be adherent to antihypertensive medications. However, it is found to be significantly lower when compared to expected WHO index of 80% medication adherence. Longer duration of diagnosis of hypertension, Traditional drug use to treat hypertension and being uneducated (can’t read and write) were factors adversely affecting medication adherence. Therefore, routine health education is strongly recommended.
Acknowledgments
We acknowledge Dilla University referral hospital for technical support and study participants for their willingness to participate.
Author’s Contributions
All authors contributed towards drafting manuscript, data analysis and revising the manuscript, gave final approval of the manuscript to be published, and they agreed to be accountable for the all aspects of the manuscript.
Compliances with Ethical Standard
All steps done during data interview were in accordance with ethical review board of Dilla University and Helsinki declaration. The study was approved by Ethical review board of Dilla University College of medicine and health science.
Funding
Non applicable
Disclosure
The authors declare that they have no any conflicts of interest.
Data Sharing Statement
On reasonable request, the corresponding author will provide the datasets used and analyzed during the current work.
References
-
Alwan A (2010) Global status report on noncommunicable diseases 20 Avenue Appia, 1211 Geneva, Switzerland.
-
Tibebu A, Mengistu D, Bulto NL (2017) Adherence to prescribed antihypertensive medications and associated factors for hypertensive patients attending chronic follow-up units of selected public hospitals in Addis Ababa, Ethiopia. Int J Health Sci 11(4): 47-52.
-
Vrijens B, Geest SD, Przemyslaw K, Demonceau J, Hughes DA, et al. (2012) A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol 73(5): 691-705.
-
Agbor VN, Takah NF, Aminde LN (2018) Prevalence and factors associated with medication adherence among patients with hypertension in sub-Saharan Africa: protocol for a systematic review and meta-analysis. BMJ 8(3).
-
Mueke AT (2013) Factors influencing adherence to hypertension medication. University of Nairobi Journal of hypertension 7(3): 47-60.
-
WHO (2015) Non communicable disease fact sheet.
-
Vijver SVD, Akinyi H, Oti S, Olajide A, Agyemang C, et al. (2013) Status report on hypertension in Africa— Consultative review for the 6th session of the African Union Conference of Ministers of Health on NCD’s. Pan Afr Med J 16(38).
-
Giday A, Tadesse B (2011) Prevalence and determinants of hypertension in rural and urban areas of southern Ethiopia. Ethiop Med J 49(2): 139-147.
-
Bundy JD, Li C, Stuchlik P, Bu X, Kelly TN, et al. (2017) Systolic Blood Pressure Reduction and Risk of Cardiovascular Disease and Mortality: A Systematic Review and Network Meta-analysis. JAMA Cardiol 2(7): 775-781.
-
Morisky DE, Ang A, Krousel-Wood M, Ward HJ (2008) Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens 10(5): 348-354.
-
Hasen G, Abdo A (2020) Medication Adherence and Associated Factors in Management of Hypertension in Shashemene Referral Hospital, Ethiopia. J Hypertens Management 6(2): 6-8.
-
Ambaw AD, Alemie G, Yohannes SM, Mengesha ZB (2012) Adherence to antihypertensive treatment and associated factors among patients on follow up at University of Gondar Hospital, Northwest Ethiopia. BMC Public Health 12(282).
-
Fatmah Jabr A Alsolami (2016) Factors Affecting Antihypertensive Medications Adherence among Hypertensive Patients Attending a General Hospital in Jeddah City, Saudi Arabia . Indian J Heal Sci 7(2): 65-76.
-
Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, et al. (2016) Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies from 90 Countries. Circulation 134(6): 441-450.
-
Roth GA (2018) Global, regional, and national age- sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet 392(10159): 1736-1788.
-
Tigist Demisew SM, kechalew T (2018) Adherence to Antihypertensive Treatment and Associated Factors among Hypertensive Patient on Follow Up in Debre Berhan Referral Hospital, North Shoa, Ethiopia. J Cardiovasc Dis Diagn 6(3).
-
Hareri A, Gedefaw M, Simeng B (2014) Assessment of prevalence and associated factors of adherence to anti- hypertensive agents among adults on follow up in Adama Referal hospital, East Shoa, Ethiopia-cross sectional study. Int J Curr Microbiol App Sci 3: 760-770.
-
Mekonnen HS, Gebrie MH, Eyasu KH, Gelagay AA (2017) Drug adherence for antihypertensive medications and its determinants among adult hypertensive patients attending in chronic clinics of referral hospitals in Northwest Ethiopia. BMC Pharmacology and Toxicology.
-
Fiseha G, Emishaw S, Mekonnen A, Alemshed F (2014) Compliance with antihypertensive treatment and associated factors among hypertensive patient on follow up in Jima University specialized hospital, Jimma, South West Ethiopia: A Quantitative Cross- Sectional Study. Journal of Hypertension.
-
Inkster ME, Donnan PT, MacDonald TM, Sullivan FM, Fahey T (2006) Adherence to antihypertensive medication and association with patient and practice factors. J Hum Hypertens 20(4): 295-297.
-
Youssef RM, Moubarak I (2002) Patterns and determinants of treatment compliance among hypertensive patients. East Mediterr Health J 8(4-5): 579-592.
-
Berisa HD, Defefo MG (2018) Non-Adherence Related Factors to Antihypertensive Medications Among Hypertensive Patients on Follow up at Nedjo General Hospital in West Ethiopia. The Open Public Health Journal 11: 62-71.
-
Daniel G, Berhane Y, Worku A (2020) Adherence to Antihypertensive Treatment and Associated Factors in Central Ethiopia. International Journal of Hypertension.
-
Iloh GUP, Ofoedu JN, Njoku PU, Amadi AN, Godswill-Uko EU (2013) Medication adherence and blood pressure control amongst adults with primary hypertension attending a tertiary hospital primary care clinic in Eastern Nigeria. African J Prim Heal Care Fam 5(1): 446.
-
Lee GKY, Wang HHX, Liu KQL, Cheung Y, Morisky DE, et al. (2013) Determinants of Medication Adherence to Antihypertensive Medications among a Chinese Population Using Morisky Medication Adherence Scale. PLoS One 8(4).
-
Terline DMD, Kane A, Kramoh KE, Toure IA, Mipinda JB, et al. (2019) factors associated with poor adherence to medication among hypertensive patients in twelve low and middle income countries. PLoS One 14(7).
-
Akhter N (2010) Self-management among patients with hypertension in Banagladesh. Journal of cardiovascular medicine 23(5).
-
Jameson F, Kasper, Hauser, Longo, Loscalzo (2018) Harisons principles of internal medicine 20th (Edn.), New York, USA.
-
Gosmanova EO, Kovesdy CP (2014) Adherence to antihypertensive medications: is prescribing the right pill enough?. Nephrol Dial Transpl 30(10): 1649-1656.
-
Yenesew A, Gashi F, Tatiparthi R (2015) Prevalence of non - adherance and its associated factors of hypertensive patients at Jimma University Specialized Hospital in Southwest Ethiopia. Indian J Heal Sci and Bio Med Research 8(1): 18-23.
-
Heydari H, Kamran A, Ahari S, Biria M, Malepour A (2014) Determinants of patient′s adherence to hypertension medications: Application of health belief model among rural patients. Ann Med Health Sci Res 4(6): 922-927.
-
Osamor PE, Owumi BE (2011) Factors associated with treatment compliance in hypertension in southwest Nigeria. J Heal Popul Nutr 29(6): 619-628.
-
Kimuyu BM (2006) Factors Associated with Adherence to Anti-Hypertensive Treatment. Nairobi university. African J Prim Heal Care Fam 2(3).
-
Chelkeba L, Dessie S, Med JR, Aug S (2013) Antihypertension medication adherence and associated factors at Dessie Hospital, North East Ethiopia, Ethiopia. Int J Res Med Sci 1(3): 191-197.
-
Khanam MA, Lindeboom W, Perez TL, Alam DS, Niessen L, et al. (2014) Adherence to treatment in rural Bangladesh findings from a population-based study. Glob Health Action.
-
Boas LCG, Foss MC, DeFreitas MCF, Pace AE (2012) Relationship among social support , treatment adherence and metabolic control of diabetes mellitus patients. BMJ 20(1): 52-58.
-
Bandura A (1989) Human agency in social cognitive theory. Am Psychol 44(9): 1175-1184.
- Measuring What Matters: Data Gaps, Certificate of Need Reform, and Pediatric Psychiatric Inpatient Capacity in North Carolina
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal