Supporting Father Involvement to Promote Co-Parent, Parent and Child Outcomes in a Canadian Context
<p>This study describes a western Canadian implementation of Supporting Father Involvement (SFI), a California, U.S. evidenced-based intervention designed to promote couple and co-parenting relationships and father engagement. Unlike the more ethnically diverse, lower income California families, Alberta families were mostly Caucasian and middle class. Evidence from SFI Alberta showed positive changes in father involvement and reduced parenting stress, parental conflict, and both avoidant and violent problem-solving strategies. In addition, couple relationship quality and children’s hyperactive and withdrawn behaviors remained stable (though they worsened in a previous control group study).Given the program’s success among these families, SFI appears to be a useful and appropriate intervention with the Albertan families. These findings add to a growing body of evidence showing the importance of strengthening father involvement through a focus on co-parenting and couple relationships, in order to obtain positive results for parents and children.</p>
Introduction
After a long history of recognizing the valuable role mothers play in children’s development, attention to the role fathers play has gathered momentum from researchers concerned about couples’ and families’ stress levels and vulner abilities, and their effects on child well- being. An abundance of evidence shows associations between fathers’ positive relationships with their children and child developmental outcomes. A sampling of studies across child age groups and ethnic/cultural groups shows positive involvement related to enhanced cognitive and educational [1, 2, 3, 4], behavioral and emotional [5, 6, 7], and social [8, 9, 10] adaptation across cultures and family structures[11, 12, 13]. Physiologically-oriented studies using fMRI studies of the brain and/or hormonal research [14] point to similar associations. However, it is also evident that father involvement does not exist as separate and independent from couple or co-parenting relationships. From the outset of parenting, paternal involvement is heavily influenced by the mother’s attitude toward his involvement [15, 16]. Her attitude towards him as a parent is affected by her valuation of the prior or present couple relationship .The parents’ relationship quality is related to fathers’ assumption of direct child care responsibilities, his satisfaction in his paternal role, and his competence as a parent Similarly, in the presence of relationship conflict, it is more difficult for fathers to be involved and have positive relationships with their children [17]. Like mothers, fathers are less likely to be warm and firm with their children when the parental relationship is conflictual [18, 19]. On the other hand, positive co-parenting that includes reduced conflict supports positive parenting styles and quality parent– child relationships for both parents [20], but especially fathers [21]. These connections between couple and co-parenting relationships with father involvement suggest that a fertile direction for strengthening family relationships would be to focus interventions simultaneously on the relationship between parents and on paternal involvement in parenting Yet, fathers continue to be notably absent from prevention and social service programs, and researchers do not collect adequate data from or about them [22, 23, 24]. Federally funded responsible fatherhood programs in the U.S. have achieved only minor success [25]. In contrast, programs that focused on the synchronicity between involving fathers and working with the parents’ relationship have obtained more promising results [26, 27]. A review of international studies on father engagement [28] offers strong support for including both parents in interventions in order to attain stronger parenting quality and child outcomes than interventions that focus on only one parent, typically the mother. This review showed, too, that few intervention studies include fathers. Thus, we are just beginning to understand how family-strengthening interventions that are inclusive of fathers and focus on inter parental relationships fare across national as well as cultural contexts Investigations are needed to determine whether interventions developed in one country or for one population are successful in other contexts. This study addresses this gap utilizing an evidence- based father involvement and co-parenting program from the U.S. implemented and evaluated with a middle class western Canadian sample. The California-based, U.S. Supporting Father Involvement (SFI) program was tested in three phases with over 800 couples in both randomized control and benchmark comparison trials. The program proved successful across ethnic and geographic boundaries. Based on the results of these initial studies [29, 30], the Palix (previously Norlien) Foundation funded several sites in Alberta to learn whether SFI could achieve positive results in Canada. This study describes changes from pre- to post-intervention for 136couples who participated in the program. The question addressed in this paper is whether couples participating in the Alberta SFI program would report positive changes in the domains of co-parenting, parenting, and child outcomes similar to those already reported in lower income, ethnically diverse populations in the U.S. In other words, would the intervention translate to a new national and cultural context? The Supporting Father Involvement (SFI) program was launched in 2003 by the California Department of Social Services, Office of Child Abuse Prevention, as the first co- parenting focused, father involvement program evaluated with a longitudinal randomized clinical trial (RCT) research methodology [29]. The intervention was based on an ecological [31] model and a family systems approach [32, 33] that articulated five key family domains (individual well-being and mental health; parenting quality and stress; co-parenting/couple communication, problem solving, and satisfaction; three generational transmission of parenting attitudes and behaviors; and balance between stress and social support outside of the family). Risk and protective factors in each of these domains are associated with fathers’ level of positive involvement in intact families [34] as well as in divorced families [35]. SFI was conceptualized as a preventive intervention for community and high risk samples, intended to increase partnership parenting and father involvement before the characteristic downturn of partner satisfaction after becoming parents [36, 37] initiates a spiral of negative family dynamics. The drop in relationship satisfaction and cooperation has been shown to increase conflicts, stress, and parental gate keeping, resulting in poorer parenting, fathers’ withdrawal or absence, and negative child outcomes [38, 39, 40, 41, 42].
Intervention
The SFI intervention begins with a couple interview that introduces the five domains parents will be working on in the intervention groups and establishes a collaborative approach to motivating change in attitudes and behaviors [43]. Families then participate in either a 32-hour fathers group or 32-hour couples group that are nearly identical in content and focus, with the only change being activities directed at the couple/co-parent pair directly or through the available paternal participant. Both curricula are conducted by clinically trained male- female pairs of Group Leaders, and an SFI Case Managergets involved with each family to help with referrals to other services as needed during the family’s time in the project. Onsite childcare and family meals before the group comprise two final aspects of the program. The curriculum, adapted by Drs. Kline Pruett and Ebling from previous iterations of the intervention model [32, 44], focuses on strengthening couple (if applicable), co-parenting, and parent-child relationships. Sixteen
sessions each focus on one of the five domains. Each week begins with a time for open check-ins with participants, where homework completion is reviewed and participants inform the group about any successes, difficult times, or other issues that arose during the week. The check-in is followed by a short didactic session, then activities designed to draw out the key lessons for that session and give participants an opportunity to expand their understanding and practice skills related to that lesson. Leaders’ questions, exercises, and games encourage parents to discuss how they are feeling about themselves and their relationship (“who does what in the family?”), their attitudes about parenting (e.g., defining and role playing different parenting styles), how they communicate and exploring how they can do so more effectively (e.g., ‘‘How well do you know your partner?’’ activity), three generational family patterns (e.g., which family rituals they wish to repeat or avoid in their current family), and how to access supports for dealing with life stresses (e.g., discussing which services they could access for specific types of problems or questions).Although each meeting focuses on one domain, the interconnectedness between domains is emphasized and exemplified. The sessions end with a homework assignment to try something different at home based on discussions from the session. In both fathers’ and couples’ groups, two of the 16 meetings are conducted separately for fathers and mothers (fathers meet with the male co-leader and focus on the relationship with their children; mothers meet with the female co-leader and focus on the process of engaging fathers and sharing family tasks with them). In addition, the mothers are invited to the first meeting of the fathers’ groups in order to increase the probability that their partners will participate and stay the course with encouragement. The curricular activities are hands-on and fairly active, with alternatives generally offered that allow more or less discussion versus active movement and are responsive to literacy levels of the group. The curriculum allows for Group Leaders’ flexibility in implementing activities and discussion, using various formats (large group, small group, couples/pairs, individuals, gendersplits) as determined to be most useful for the particular group participants.
SFI Evidence-base
The California study included randomized control trials that analyzed differences between the two interventions (fathers and couples) described as well as a 3-hour informational session that functioned as the low dose control group. The first SFI study phase included 279 Mexican American and European American low-income couples residing in 4 California counties with a youngest child ranging in age from 0-7 (average 2.5 years). Participants were all biological parents of the youngest child. This first clinical trial SFI study demonstrated that the intervention was associated with long-term benefits for each parent in terms of their parenting (including father involvement), the couple relationship, and the child for complete details and results and [45]. Results held across Hispanic and Caucasian, married and unmarried, and higher and lower socioeconomic status families. The intervention was also effective regardless of parental levels of depression, conflict, and couple satisfaction when entering the program. The number and range of positive outcomes, combined with careful program methodology and assessment, led SFI to be designated as an evidence- based practice by the California Evidence-Based Clearinghouse. Following the positive results of the first SFI study, the same research team sought to establish whether the outcomes could be replicated with a more diverse participant population. A second SFI trial [30] was conducted in the original four California sites with the addition of a new site comprised of an African American family sample. Other variations in this study (referred to as Study 2) involved extending the age range of the youngest child from 0-7 to 0-11, and including any father figures (step parent, siblings, grandparents). As in Study 1, the youngest child (and mean age) entering Study 2 was a toddler. The most significant change in the design of Study 2 included dropping the control group and RCT design. Because results from the first study showed that participants in the control group experienced no positive and many negative changes in their relationships as couples or in their children’s behavior [29], ethical concerns drove the decision to eliminate the control group. The sites also were allowed to choose whether to implement fathers or couples groups, and given the findings of Study 1 that revealed better outcomes for the couples groups, the choice to run couples groups predominated. In the initial study, fathers groups produced positive changes in individual and parental domains but did not affect the couple domain, and the Group Leaders reported that families – especially mothers – preferred the couples group option and participants more deeply explored issues when both parents were involved. Couples group attendance averaged 10% higher than fathers group attendance, as well. SFI researchers chose to use a “benchmarking” strategy [46] by comparing the results from Study 2, which offered the same curriculum and program to a more inclusive population, with the already-published data from the original RCT study [29]. The researchers conceptualized Study 2 as an opportunity to gather practice-based evidence through a community-based application of the SFI approach. In the second study, 236 low-income parents participated in an SFI couples group. This time participant couples in all three ethnic groups (European American, Mexican American, African American) showed positive changes in measures of parent-child relationships, couple relationship quality, and children’s problem behaviors. This study added a couple communication variable that is also a child abuse risk factor: violent means of problem solving, which also decreased significantly on average among participants. In addition to individual- and family- level effects, systems-level results indicated that both studies 1 and 2 showed organizational changes in the community agencies responsible for implementing SFI in terms of increased father friendliness and family focus that more fully included men as well as women [47]. These changes were sustained for 18-months beyond the Baseline assessment, which occurred prior to the intervention. Study 2 demonstrated that repeating the SFI intervention with a more diverse sample (inclusion of African American families and non-biological father figures) produced positive results comparable to or better than those obtained in Study 1, increasing confidence in the utility of SFI [30]. The results of both studies support the combined focus on couple relationships, fatherhood, and parenting to draw upon the strengths of each to produce positive outcomes for the entire family.
SFI in Alberta Canada
In 2011, the Norlien (now called Palix) Foundation brought SFI to Canada and implemented the full program at three family resource centers, but adopted a scaled back evaluation component. SFI Alberta focused on offering prevention program components that maximize the chance of obtaining similar results [48], including sufficient funding, coordination with other agencies, provider skill proficiency, training, and technical assistance. The SFI Alberta program entailed the same 32- hour couples group intervention with clinically trained co-leaders, case management, and attempts to enhance father friendliness in the social service agencies in which SFI was embedded. The Canada sample was assessed with a longitudinal design prior to the intervention (Baseline) and again one-year later.
The purpose of the current study is to examine the program’s utility with the Alberta sample. The program was implemented in Alberta after all Canadian SFI staff were trained by the original program developers and California program staff for all positions (group leaders, case managers, and project directors). In addition, SFI Alberta followed a model of weekly consultative phone calls with the developers in the first years and bi-weekly calls thereafter, and twice yearly day-long training and consultations in orderto support fidelity to the program model. Procedures for screening, recruitment, and data collection were similarly kept the same as California procedures and monitored on an ongoing basis. The Data Manager from the original SFI had regular contact with the Alberta staff and oversaw data collection and analysis, further maximizing data collection fidelity. All of these precautions aimed at demonstrating the program’s utility for the Canadian sample with reasonable replicability.
Methods
Procedures
SFI Alberta parent participants were recruited widely to participate in family centers in two regional sites, Cochrane and Leth bridge. Community outreach extended to agencies, newspapers, and outreach at family-oriented events. Inclusion criteria for SFI Alberta were: (a)both partners agreed to participate with their youngest child, who was identified as the “target child” for purposes of this study, and (b) the parents were raising the child together regardless of marital and cohabitation status. Participant families were excluded from the program if (a) either co-parent suffered from a severe mental illness or drug or alcohol abuse problem that interfered with daily functioning at work or in caring for the children, or (b) the family had a current open child or spousal protection case with child protective services or an instance within the past year of spousal violence or child abuse. Parents who expressed interest in program participation were screened for inclusion, then interviewed separately and together to orient parents to the topics of the intervention and to familiarize parents with Group Leaders before group participation. Parents filled out questionnaires at the time they joined the study (Baseline) and 1 year later. Note that the participants do not constitute a high risk sample; they did voluntarily seek support and positive change in their relationships as parents and partners.
Participants
In total, 164couples (data from 167fathers and 164mothers) have participated up to the time of the present report. Most of the parents at Baseline were 25- 43 years old (86% of the fathers, 91% of the mothers), married (82%), living together as a couple (97%), and born in Canada (90% of the fathers, 91% of the mothers). A majority of mothers (94%) and fathers (93%) are Caucasian/European. The other participants identified as First Nations/Inuit/Metis (4% of fathers and 2% of mothers); Asian or Pacific Islander (2% of fathers and 3% of mothers), and other (unspecified) lineage (1% of fathers). Most of the Albertans were high school graduates (87% of the fathers, 92% of the mothers).About 19% of the fathers and 22% of the mother completed college. The average and median combined family income fell in theC$60,000-70,000 (SD=C$27,000) a year range, and the modal reported income was “C$90,000or more a year.”On the other end of the economic spectrum, 5% of fathers and 4% of mothers reported that they receive federal financial assistance. During the time of data collection, the exchange rate between US and Canadian dollars was 1:1 and fluctuated little. The higher income was due in large part to a parent working in the Alberta oil industry in high-paying jobs, but parent participants also reported they experienced stressful work conditions. Target (youngest) children were newborn to ten years old (average, 2.5years old; SD=2.0, median and mode both 2.0); the average was comparable across the two sites.
Data Collection
Once families agreed to participate, Case Managers provided them with questionnaires, which they filled out at the Family Resource Centers. Of the families who agreed to participate, 11 never returned to the Family Resource Center and so did not fill out Baseline questionnaires. From the 331 Baseline participants (again, 167 fathers and 164 mothers), information is available for 212 of them (about two-thirds of the sample) at the 1-year follow-up. Of the remainder, 69 participants have not yet received follow-up assessments and 50 participants dropped out of the program and did not complete the follow-up. Of those who started groups, 91% completed the 16-week meetings and 83% completed the post-intervention questionnaires as of this writing. The modal number of sessions attended was 14 (mean=11.5 sessions, SD=4.7).
Measures
Parental well-being
Center for Epidemiological Studies–Depression [49]: The CES-D scale is a 20-item self-reported instrument on which participants report the frequency of common Depressive Symptoms over the past week. Each item is scored from 0 (rarely or none of the time, less than one day) to 3 (all of the time, 5–7 days) for a total score ranging from 0-60. Four positively stated items (item 4, I felt that I was just as good as other people; item 8, I felt hopeful about the future; item 12, I was happy; item 16, I enjoyed life) are reverse-coded when calculating the total score. The cut-off value of ≥16 has been widely used to define clinically meaningful depressive symptoms [50].
Parenting
(a) Who Does What? [51]: Who Does What? is an 11-item
questionnaire administered to both parents to assess Fathers’ Involvement in the care of their youngest child (e.g., feeding, playing with the child, getting up with the child at night), using a 1-9 scale in which 1 = she does it all, 5 = we do it about equally, and 9 = he does it all. We calculated means across responses to the 11 items for the analysis; a mean close to 5 suggests a more balanced workload of child-related tasks. Average inter correlation for the items was r =.50 (p<.001) between parents. Because the items represent distinctly different realms of involvement, and because we did not expect that a parent who plays most with the child will necessarily be the one who gets up at night, we did not expect high scale reliabilities. (b) Parenting Stress Index [52]: A 16-item revised version [52] of the standardized PSI measures Parental Stress associated with parenting the youngest (target) child. Mean subscale scores of Parental Distress, Parent-Child Dysfunctional Interaction, and Difficult Child were obtained and averaged to create a mean Parenting Stress score. Parents indicated on a 1-5 scale the extent of their agreement (1=Strongly Agree) to disagreement (5=Strongly Disagree) with statements describing themselves as stressed, their child as difficult to manage, and a lack of fit between what they expected and the child they have. Therefore the mean scores range from 1 to 5; a mean of about 2.5 would suggest clinically significant levels of stress. The scale has been validated by comparing parents who do and do not have known childrearing stressors (developmental delay, oppositional defiance, or difficult temperaments). Scale reliabilities for the Alberta sample ranged from α=.58 to .83 for fathers and α=.56 to .84 for mothers.
Couple Satisfaction
The Quality of Marriage Index [53] is a six-item questionnaire with one 10-point global estimate of each partner’s relationship satisfaction. Couple Relationship
Quality ranging from 1=Unhappy to 10=Perfectly Happy, and five specific questions (e.g., My relationship with my partner is very stable; My relationship with my partner is strong; and I really feel like part of a team with my partner) rated on 7-point scales ranging from 1=Very Strongly Disagree to 7=Very Strongly Agree (α =.94for fathers and for mothers). The QMI has high overlap with longer, traditional measures of marital quality [54].
Co-parenting Quality
The Couple Communication Questionnaire [55] is a 27- item measure of the amount of conflict between partners, specific areas of conflict, and the strategies employed by the couple in dealing with conflict. We used three subscales (score range in parentheses): (a) overall Frequency of Conflict (0-78) for 13 items, (b) Avoidant Problem-solving (0-4) (“We ignore the problem”; “We avoid talking but continue to feel uneasy” and (c) Violent Problem-solving (0-14).Items for this latter variable included “I yell at or insult my partner”; “I throw something”; and “I push, grab or shove my partner.” Because this measure is designed in a checklist format, we report scores as sums, not means. Internal consistency in this sample for the three subscales ranged from α =.66 to .84 for mothers and α =.60 to .86for fathers.
Child
Child Adaptive Behavior Inventory [56]. Each parent filled out a 25-item adaptation of the 106-iteminventory.
Each item on the CABI was rated by both parents on a 4- point scale ranging from 1 (not at all like this child) to 4 (very much like this child). We report scores as means. Item scores were composited based on a factor analysis of the scale: (a) Aggression (11 items): “Has a hot temper”, “Argues; quarrels”, or “Gets into fights with other children”(b) Hyperactivity (6 items): “Has trouble concentrating on what he/she’s doing”, “Is restless, can’t sit still”, or “Is nervous or high strung”, (c) Social Isolation (8 items): “Isolates him/herself from the peer group”, “Withdraws; prefers solitary activities”, or “Usually plays or works alone” and (d) Child Leadership (4 items).We excluded Child Leadership from the study since the average age of the children was 2 years. Internal consistency values for each of the 3 subscales were strong: α =.89 (fathers) and α =.90 (mothers) for aggression; α =.76 (fathers) and α =.79 (mothers) for hyperactivity; and α =.80 (fathers and mothers) for social isolation.
Results
Table 1 presents the means and standard deviations at Baseline (Pre-intervention) and Follow-up (12 months later) for each of the measures used in the study. We determined possible intervention effects via a 2 x 2 repeated measures MANOVA using time (Baseline, Follow-up) and sex (Father, Mother) as within-subject.
| Father | Mother | |||
|---|---|---|---|---|
| Baseline Mean (SD) | Follow-up Mean (SD) | Baseline Mean (SD) | Follow-up Mean (SD) | |
| Measure | ||||
| Individual Well-Being (CES-D) | 11.7 (7.4) | 13.0 (8.7) | 15.0 (10.0) | 13.8 (10.1) |
| Parenting Stress (PSI) | 2.3 (0.7) | 2.2 (0.7) | 2.4 (0.7) | 2.3 (0.7) |
| Parent-Child Dysfunctional (PSI) | 1.8 (0.6) | 1.7 (0.5) | 1.8 (0.6) | 1.7 (0.5) |
| Father Involvement (Who Does What?) | 3.8 (1.1) | 4.0 (1.1) | 3.4 (1.1) | 3.6 (1.2) |
| Couple Quality of Partnership (QMI) | 5.5 (1.3) | 5.5 (1.4) | 5.3 (1.4) | 5.3 (1.6) |
| Overall Conflict (CCOMM) | 25.8 (12.9) | 23.5 (12.8) | 27.2 (13.6) | 24.7 (14.7) |
| Avoidant Problem Solving (CCOMM) 1.4 (1.3) | 1.4(1.3) | 1.2 (1.3) | 1.5 (1.4) | 1.2 (1.3) |
| Violent Problem Solving (CCOMM) | 1.6 (1.7) | 0.9 (1.2) | 1.6 (1.6) | 1.1 (1.3) |
| Child Aggression (CABI) | 2.0 (0.6) | 2.2 (0.5) | 2.0 (0.7) | 2.1 (0.5) |
| Child Hyperactive (CABI) | 2.2 (0.7) | 2.3 (0.6) | 2.2 (0.7) | 2.2 (0.8) |
Table 1: Comparison between Baseline and Follow-up means in the Alberta Study.
| F | df¹ | 95% CI | partial eta squared | |
|---|---|---|---|---|
| Parent Well-Being (CES-D) | .00 (NS) | 105 | [-1.3, 1.2] | 0 |
| Parent Well-Being Sex Difference | 5.5* | 105 | [0.3, 3.8] | 0.05 |
| Parenting Stress (PSI) | 6.1* | 101 | [-0.2, -.02] | 0.06 |
| Parent-Child Dysfunctional Interaction (PSI) | 8.2*** | 101 | [-0.2, -.03] | 0.05 |
| Father Involvement (Who Does What?) | 4.3* | 102 | [.01, 0.4] | 0.04 |
| Who Does What Sex Difference | 30.0**** | 102 | [0.3, 0.5] | 0.23 |
| Couple: Quality of Partnership (QMI) | 0.1 (NS) | 105 | [-0.2, 0.2] | 0 |
| Overall Conflict (CCOMM) | 6.5* | 105 | [-4.2, -.05] | 0.06 |
| Avoidant Problem Solving (CCOMM) | 7.6* | 105 | [.08, 0.5] | 0.07 |
| Violent Problem Solving (CCOMM) | 28.1**** | 105 | [-0.8, -0.4] | 0.21 |
| Child Aggression (CABI) | 6.0* | 98 | [.02, 0.2] | 0.06 |
| Child Hyperactive (CABI) | 1.6 (NS) | 97 | [-0.2, .05] | 0.02 |
| Child Shy, Withdrawn (CABI) | 1.8 (NS) | 98 | [-0.2, .03] | 0.02 |
Table 2: Comparison between Baseline and Follow-up means in the Alberta Study.
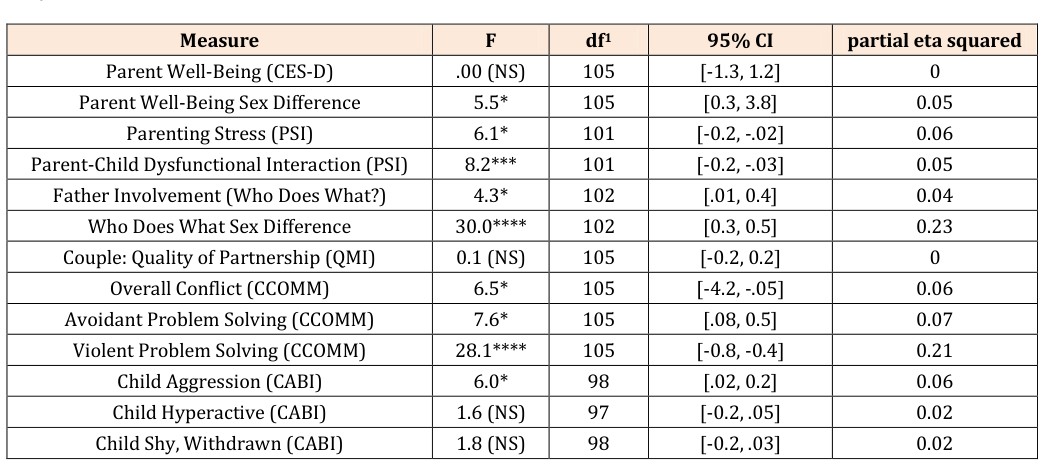
Data collected from Alberta participants at the follow- up assessment illustrated positive results in the domains of couple and co-parenting relationships, parenting, and child adaptation. For couple relationship quality, given the decline in relationship satisfaction for parents of young children in almost all longitudinal studies [36, 37], stability of couple relationship quality as measured by the Quality of Marriage Index is understood as a positive outcome for Alberta couples (F (1, 105) =0.1, n.s.). Co- parenting improved following the group intervention on the following variables assessed: violent problem-solving behaviors (yelling, throwing things, hitting) declined significantly (F (1, 105) =28.1, p<0.001) as did avoidant problem solving strategies (F (1, 105)=7.6, p<.05). Moreover, couples reported less overall conflict (F (1, 105)=6.5, p<.05). In sum, following the intervention these couples reported more adaptive ways of dealing with their disputes. In the parenting domain, both parents’ reports of father involvement increased significantly (F (1, 102) =4.3, p<.05). However, there was a significant sex difference in parents’ characterization of fathers’ involvement; fathers said they did more child care than mothers said they did (F (1, 102) =30.0, p<.001). Couples also reported significant declines in parenting stress (F (1, 101) =6.1, p<0.05) over the year and they characterized their relationships with their children as less dysfunctional (F (1, 101)=8.2, p<.005). In terms of child outcomes, no change occurred in parents’ characterizations of their children as hyperactive (F(1,
97)=.1.6, n.s.) or socially isolated (F(1,98)=1.8, n.s.), whereas negative changes occurred in previous analyses of families who did not receive the intervention [45, 30]. Not all changes were positive or stable. No significant changes were obtained in parents’ depression after the intervention. However, a sex difference emerged showing that mothers became less depressed, while fathers became more so. The difference between genders was significant (F (1, 105)=5.5, p<.05) and the interaction between gender and time showed that parents moved closer together in their levels of depressive symptoms after the intervention (F (1, 105)=3.9, p<.05). Parents also reported increases in their children’s aggressive behaviors (F (1, 98=6.0, p<.05).
Differences between Program Stayers and Dropouts
We used a general linear model to assess any differences between the families that dropped out of the program prior to completing the follow-up assessments. For the most part, the data that came from demographic reports showed no differences between families that completed the program and families that did not, with regard to participants’ age, living arrangements, whether they were born in Canada, or whether they receive financial assistance. There were no differences in terms of their measures of parenting stress, parent-child dysfunctional interaction, father involvement, quality of partnership, and any responses to the couple communication or the child behavior questions. However, some differences emerged. Couples were more likely to complete the follow-up if they were married rather than unmarried (fathers F(1, 161) =5.8, mothers F(1, 161) =4.3, both p<.05), if they had attended at least some college (fathers F(1, 160) =3.6, p =.06, ns; mothers F(1, 160) =6.2, p<.05), and if they had higher incomes (fathers F(1, 160) =9.0, mothers F(1, 160) =7.9, both p<.01). Participants were less likely to complete the follow-up if they identified their ethnicity as First Nations, Metis, or Inuit (fathers F(1, 160) =7.8, mothers F(1, 160) =7.5, both p<.01). Fathers who were more depressed at baseline also were less likely to complete the program (F(1, 161) =4.0,p<.05).
Discussion
This study presents findings from an Alberta, Canada evaluation of Supporting Father Involvement (SFI), a program that aims to enhance father involvement and parenting through strengthening parents’ couple and co- parenting relationships, with the ultimate goal of preventing or reducing behavioral problems among their children. The study was designed as a prevention program to enhance all family members’ well-being while attending to family systems dynamics in couple, co- parenting, and parenting domains. Results obtained with the sample of 106 primarily Caucasian, higher income families from Alberta showed that, on average 12 months after the families entered the study, SFI participants remained stable or changed positively on nine of the 11 measures assessed: increased father involvement, declines in parenting stress, improved co-parenting through less conflict, improved couple communications in less avoidant and violent problem solving, reduced dysfunction in parent-child relationships, and stability in couple relationship satisfaction and children’s hyperactivity and social isolation. On the other hand, parental depression did not change. Only one measure – the parents’ reports of children’s aggression – worsened after the intervention. Seven of the 11 measures also were assessed in rigorous evaluation designs of low income, ethnically diverse California participants numbering over 800 families [45, 30], and the changes in content and direction were remarkably similar. The stability, rather than reduction, of parental depression, especially among the mothers’ whose baseline scores approached clinical levels, was not altogether surprising, since changes in the couple relationship do not necessarily parallel changes in depression [57]. It is concerning, however, as depression tends to be associated with parenting stress [58], which can be related to poorer couple relationships and negative parenting strategies [57]. Since couple relationships improved and stress decreased in the current study, it is possible that couple and co-parenting relationships that changed positively over time will eventually spillover to lessen the mothers’ personal distress. The mothers’ distress may also wane with time as their youngest child (average two years) develops, since toddlerhood is a difficult life stage in general for many parents due to the increase in toddlers’ relentless push for autonomy and accompanying non-compliance [59], as well as decreased time and energy for couple relationships [32]. The increased aggression from children would be expectable as children age, as shown by a previous control group study of SFI participants [45]. The increased aggression in this sample is puzzling, especially since the children did not develop other behavior problems shown to manifest without intervention. The finding could be a byproduct of the maternal depressive symptoms, since such symptoms have been found to be related to parental tendencies to make negative attributions about children’s behavior [57]. But this doesn’t explain why child aggression would increase, but not the other behaviors measured. Only additional follow- up will illuminate whether it is a temporary increase or one associated with other types of behavioral change, as well. It is also evident that those who stayed in the program had greater economic and educational resources, although they were not less distressed as couples or parents than the participants who did not complete the follow-up. Despite the presence of a case manager, those with less of these resources and more depressed fathers, were less likely to provide follow-up information, and to stay the course of the program. This points to an area for further focus and improvement in the future, as a concerted effort is made to retain and learn from these participants, especially fathers, what makes it difficult to stay, and hopefully, to develop knowledge, skills, and support to enhance their family life. Since there were no differences in program efficacy among ethnic, income and educational groups in the California sample [45], and since 91% of those who started the SFI program in Alberta finished the group and85% of them completed the follow-up survey, the relevant question is not whether the program is effective for these different groups, but how to engage these lower resourced families up front so they choose to avail themselves of the program. This difficulty in recruiting Canadian fathers in their real life settings has been noted elsewhere [60], and this study shows progress but also that there is more work to do in improving our collective success in this regard. Patterns from this study of Albertan families show gains in domains paralleling those in the California studies of the same program. Parental depression did not change significantly in the Albertan sample and was not reported in the California studies to date. However, positive changes in the parenting and co-parenting variables (father involvement and parenting stress, conflict, parent ratings of dysfunctional parent-child relationships, and avoidant and violent problem solving) occurred alongside stability in couple satisfaction and some child domains, even when control groups from the California RCT showed that without intervention, couples’ well-being and child behaviors worsened over 1-1/2 years. The Canadian couples’ relationship satisfaction did, in fact, hold steady and their communication improved. In relation to child outcomes, although three measures of child behavior problems (aggression, hyperactivity, social isolation)worsened over time in the comparison sample in the California study, the Albertan sample showed no change occurring in hyperactive or social isolation behaviors. Parents did rate their child as more aggressive, much like the children whose parent did not participate in the SFI intervention. Overall, then, findings are very similar to previous SFI studies. As in the California replication study [30], we cannot interpret the results of the current study as being due to the intervention without a control or comparison group. We are optimistic, however, that the results echo previous ones obtained through an RCT and its benchmark comparison study. The benchmark study indicates that without intervention, quality of couple satisfaction decreases and child problem behaviors increase. In the California replication study, the fact that couple relationship satisfaction and three measures of child problem behavior remained stable over time lends support to the inference that this pattern reflects the positive impact of working in the SFI groups on family relationship issues over 16 weeks. The fact that this pattern is repeated again in the current Alberta study after SFI group participation supports the possibility that the positive effects are due to participation in the intervention program. The finding regarding the stability of couple relationship satisfaction over a year in the current Canadian study is noteworthy. The consistent pattern of positive findings for nearly 1,000 families across all three studies (two U.S. and 1 Albertan) supports the proposition that the findings could be attributable to participating in the SFI couples group intervention with a case management component.
These effects, while small, are notable as outcomes. Equally of note, is the success of SFI implementation in another setting and culture. SFI program developers required a high degree of implementation fidelity in Canada: an intensive training of all staff (including new staff after turnover), monthly phone consultations with each staffing group (Group Leaders, Case Managers, Program Directors), twice yearly day long meetings attended by all staff at all sites, and feedback from processes observed over the course of evaluation. Positive results produced in the current study suggest that the Alberta SFI program demonstrates the program’s potential robustness in adapting to the culture and circumstances of the Alberta participants through scale up of core intervention and implementation components [61] of SFI. The Alberta study stands as a quasi- experimental dissemination of the SFI approach. Across the California and Alberta studies, the common denominator for the core intervention components involved the effective implementation of the five-domain ecological conceptual framework [32, 33] and a “couples relationship” approach [26, 62, 63] that focuses on co- parenting communication in achieving positive outcomes. In addition to increasing father involvement and reducing parents’ ineffective and problematic (avoidant and violent) problem solving strategies, SFI strengthens co- parenting through more effective problem-solving and reduced conflict. These outcomes, placed alongside reviews and meta-analyses of intervention studies that include fathers and focus on the couple and co-parenting as well as parenting [28, 64], strengthen credibility for the power of co-parenting and couples’ focused interventions to affect parenting and children, with value-added changes in family subsystems known to impact family functioning over the life course Stable aspects of the intervention common in all three SFI studies were the use of two clinically experienced group leaders (one male, one female), case management for each family, a meal prior to each session, and childcare while the parents met in groups. The structure of each group session (open-ended, didactic, and activity-based) also remained constant. The fact that all three SFI trials used staff from agencies embedded within local communities also adheres to a key component of the replication model. As the SFI program continues to evolve and undergo adaptation over time, the program will build upon the existing model by synthesizing evidence from these disseminations to inform potential changes to make the intervention increasingly effective and have even greater impact on families [65].
Limitations
A primary limitation of the present study is that the Alberta participants comprised a sample of convenience rather than a representative sample of families from the Albertan communities. The participants were men and women who were parents of young children and willing to take part in an intervention to increase fathers’ involvement in family life. Another limitation is that the assessment reported here relied on parent report, with all of the shortcomings thereof. In addition, a self-selection bias is highly likely since only two-thirds of those who intended to participate and filled out baseline information completed the follow-up data, although some of that data are yet to be collected from the most recent waves of data collection and parent participation. The current study does not speak to SFI’s appropriateness across more diverse populations in Canada. We could not test for differences between ethnic groups, due to the high proportion of Caucasian European participants in the present sample of parents. The three intervention sites in Alberta did span geographic areas consisting of one urban site, one large town/rural mixed site, and one small urban/rural mixed site. Further implementation and investigation will be needed to conclude that the SFI intervention approach is equally successful among families of different geographic and ethnic origins and economic resources. Such replications are currently underway in Canada, the U.S. and the U.K.
Future Research
Although the current study demonstrated positive changes in the quality of the couple relationship, it was not able to isolate effects on the couple’s intimate relationship from effects on co-parenting quality with existing measures from previous SFI studies. Interviews conducted with each parent to capture qualitative impacts of the intervention according to parents’ perceptions of their intimate relationships and co-parenting dynamics could be illuminating in broadening and deepening what is understood from the quantitative measures. The design of the current study does not provide data regarding the mechanisms by which the intervention produces positive effects. Extracting the couple relationship versus co-parenting [66] will enable researchers to better understand how these processes work in families with high and low relationship satisfaction and/or those cohabitating and in a long-term relationship versus those who are not. Using data supported by the benchmark study and similar interventions with middle-class couples [32, 67]. Cowan P et al. [30] proposed that the SFI provides an environment in which couples could find “support in exploring the connections among the key domains of family life while working on their own relationship challenges” (p. 29). In turn, this process helps parenting couples to find ways of reducing the risks and increasing the protective factors that affect their own and their children’s adaptation. The expectation –and findings – shows that strengthening the relationship between parents is associated with a) positive outcomes in father involvement and b) positive co-parenting communication, c) stability in couple relationships and d) stability in children’s behaviors. Future analyses using path modeling and observational data are underway to learn more about the interconnections among these relationships.
Practice Implications
A central practice implication from the current study is that the SFI model of intervention offers a process as well as content that could potentially be disseminated on a larger scale by embedding it within existing service delivery systems with locally-trained family service providers. Outside of the initial California studies cited above, the program has been implemented with Head Start programs, ex-incarcerated offenders, and teens involved in a second-pregnancy prevention program (none yet evaluated). The SFI model can contribute to integration of service delivery by substituting for or adding to the parenting classes that are currently being offered in agencies in order to widen the parenting focus to include couple and co-parenting relationships. The SFI approach may further increase cost effectiveness for agencies by working with groups of couples at a time, preventing future family distress from escalating, and thus reducing the programmatic costs associated with it. SFI provides a community-based, non-stigmatizing approach that is more likely to be accepted by parents than one which is parent-training specific and singling out parental inadequacies when they are often already feeling overwhelmed and incompetent. The father-inclusive model of SFI suggests that fathers can offer valuable support to mothers and together, they can adopt a team approach that can enhance both parents’ mental health, maternal parenting [68] and child adjustment [69]. The current study supports the notion that it is a feasible and worthy goal to enhance children’s development and well- being through including fathers, as well as mothers, in programs that offer help in managing their relationship challenges with one another. Our experience in conducting and evaluating the Supporting Father Involvement intervention program leads us to recommend harnessing the power of both parents, and focusing on the relationship between them, to produce a greater impact on the entire family [70, 71, 72, 73].
References
-
Kim MI, JangYA (2007) The effect of father’s child rearing behavior and child rearing involvement perceived by children on children’s self-esteem and school adjustment. Korean Journal of Community Living Science 18(3): 379-390.
-
McWayne C, Downer JT, Campos R, Harris RD (2013) Father involvement during early childhood and its association with children's early learning: A meta- analysis. Early Education & Development 24(6): 898- 922.
-
Tamis‐LeMonda CS, Shannon JD, Cabrera NJ, Lamb ME (2004) Fathers and mothers at play with their 2‐and 3‐year‐olds: contributions to language and cognitive development. Child dev 75(6): 1806-1820.
-
Yogman MW, Kindlon D, Earls F (1995) Father involvement and cognitive/behavioral outcomes of preterm infants. J Am Acad Child Adolesc Psychiatry 34(1): 58-66.
-
Langley C (2016) Father knows best: Paternal presence and sexual debut in African-American adolescents living in poverty. Family Process 55(1): 155-170.
-
Pougnet E, Serbin LA, Stack DM, Schwartzman AE (2011) Fathers' influence on children's cognitive and behavioural functioning: A longitudinal study of Canadian families. Canadian Journal of Behavioural Science/Revue canadienne des sciences du comportement 43(3): 173-182.
-
Sarkadi A, Kristiansson R, Oberklaid F, Bremberg S (2008) Fathers' involvement and children's developmental outcomes: A systematic review of longitudinal studies. Acta paediatr 97(2): 153-158.
-
DavidsonAJ, Updegraff KA, McHale SM (2011) Parent/peer relationship patterns among Mexican- origin adolescents. Int J Behav Dev 35(3): 260-270.
-
Katoh K, Ishii-Kuntz M, Makino K, Tsuchiya M (2002) The impact of paternal involvement and maternal childcare anxiety on sociability of three-year-olds: Two cohort comparisons. Japanese Journal of Developmental Psychology 13(1): 30-41.
-
McDowell DJ, Parke RD( 2009) Parental correlates of children’s peer relations: An empirical test of a tripartite model. Developmental Psychology 45(1): 224-235.
-
Lamb ME (2010) The role of the father in child development. Hoboken, NJ: Wiley.
-
Peters HE, Day RD, Peterson GW, Steinmetz S (2014) Fatherhood: Research, interventions, and policies. Routledge.
-
Pruett KD (2000) Father need: How fathers parent differently than mothers and why it matters to children and families. New York: Free Press.
-
Weisman O, Zagoory-Sharon O, Feldman R (2012) Oxytocin administration to parent enhances infant physiological and behavioral readiness for social engagement. Biological psychiatry 72(12): 982-989.
-
Schoppe-Sullivan SJ, Brown GL, Cannon EA, Mangelsdorf SC, Sokolowski M (2008) Maternal gatekeeping, coparenting quality, and fathering behavior in families with infants. J Fam Psycho 22(3): 389-398.
-
Zvara BJ, Schoppe‐Sullivan SJ, Dush CK (2013) Fathers' involvement in child health care: associations with prenatal involvement, parents' beliefs, and maternal Gate keeping. Family Relations 62(4): 649-661.
-
Doherty WJ, Kouneski EF, Erickson MF (1998) Responsible fathering: An overview and conceptual framework. Journal of Marriage and Family 60(2): 277-292.
-
Hanington L, Heron J, Stein A, Ramchandani P (2012) Parental depression and child outcomes – is marital conflict the missing link? Child Care, Health and Dev 38(4): 520-529.
-
McHale J (2007) Charting the bumpy road of co parenthood: Understanding the challenges of family life. Washington, DC: Zero to Three.
-
Zemp M, Cummings EM, Bodenmann G, (2016) The significance of parental conflict for children: Rationale for couple-focused programs in family therapy. European Psychologist 21(2): 99-108.
-
Feinberg ME, Kan ML (2008) Establishing family foundations: intervention effects on coparenting, parent/infant well-being, and parent-child relations. J Fam Psychol 22(2): 253-263.
-
Brandon M, Bailey S, Belderson P, Gardner R, Sidebotham P, et al. (2009) Understanding Serious Case Reviews and their Impact: A Biennial Analysis of Serious Case Reviews 2005-2007. Research Report No DCSF-RR129, University of East Anglia.
-
Smith TK, Duggan A, Bair‐Merritt MH, Cox G (2012) Systematic review of fathers' involvement in programmes for the primary prevention of child maltreatment. Child Abuse Review 21(4): 237-254.
-
Maxwell N, Scourfield J, Holland S, Featherstone B, Lee J (2012) The benefits and challenges of training child protection social workers in father engagement. Child Abuse Review 21(4): 299-310.
-
Cowan CP, Cowan, PA, Knox V (2010) Marriage and fatherhood programs. Future Child 20(2): 205-230.
-
Caldwell CH, De Loney EH, Mincy RB, Klempin S, Brooks CL, et al. (2011) Strengthening bonds between nonresident African American fathers and sons as a way to reduce or prevent youth risky behaviors. In: Haen C (Ed.) Engaging boys in treatment: Creative approaches to the therapy process New York 265- 291.
-
Fagan J (2008) Randomized study of a prebirth coparenting intervention with adolescent and young fathers. Family Relations 57(3): 309-323.
-
Panter‐Brick C, Burgess A, Eggerman M, McAllister F, Pruett K, et al. (2014). Practitioner review: engaging fathers–recommendations for a game change in parenting interventions based on a systematic review of the global evidence. J Child Psychol Psychiatry 55(11): 1187-1212.
-
Cowan PA, Cowan CP, Pruett M, Pruett K, Wong JJ (2009) Promoting fathers' engagement with children: Preventive interventions for low-income families. Journal of Marriage and Family 71(3): 663- 679.
-
Cowan PA, Cowan CP, Pruett M, Pruett K, Gillette P (2014) Evaluating a couples group to enhance father involvement in low-income families using a benchmark comparison. Family Relations 63(3): 356- 370.
-
Bronfenbrenner U (1979) The ecology of human development: Experiments by nature and design, MA: Harvard University Press, Cambridge.
-
Cowan CP, Cowan PA (2000) When partners become parents: The big life change for couples. Mahwah, NJ: Erlbaum.
-
Heinicke CM (2002) The transition to parenting. Handbook of parenting 3: 363-388.
-
Cookston JT (1999) Parental supervision and family structure: Effects on adolescent problem behaviors. Journal of Divorce and Remarriage 32(1/2): 107–122.
-
Maccoby EE, Depner CE, Mnookin RH(1990) Coparenting in the second year after divorce. Journal of Marriage and the Family 52(1): 141-155.
-
Twenge JM, Campbell WK, Foster CA (2003) Parenthood and marital satisfaction: A meta-analytic review. Journal of Marriage and Family 65(3): 574- 583.
-
Hirschberger G, Srivastava S, Marsh P, Cowan CP, Cowan PA (2009) Attachment, marital satisfaction, and divorce during the first fifteen years of parenthood. Personal Relationships 16(3): 401-420.
-
Coley RL (2001) In visible men: Emerging research on low-income, unmarried, and minority fathers. Am Psychol 56(9): 743-753.
-
Ganong L, Coleman M, Chapman A (2016) Gate keeping after separation and divorce. In: Drozd L, Saini M, Olesen N (Eds.) Parenting Plan Evaluations: Applied Research for the Family Court 2nd (Edn) University Press New York: Oxford 308-345.
-
Kuczynski KJ, Lindahl KM, Malik NM, Laurenceau JP (2006) Marital conflict, maternal and paternal parenting, and child adjustment: a test of mediation and moderation J Fam Psychol 20(2): 199-208.
-
Sandler I, Miles J, Cookston J, Braver S (2008) Effects of father and mother parenting on children's mental health in high‐and low‐conflict divorces. Family Court Review 46(2): 282-296.
-
Sturge-Apple ML, Davies PT, Winter MA, Cummings EM, Schermerhorn A (2008) Interparental conflict and children's school adjustment: The explanatory role of children's internal representations of interparental and parent-child relationships. Devl Psychol 44(6): 1678-1690.
-
Miller W R, Rollnick S (2009) Ten things that motivational interviewing is not. Behav Cogn Psychother 37(2): 129-140.
-
Cowan PA, Cowan CP, Ablow JC, Johnson VK, Measelle JR (2005) The family context of parenting in children's adaptation to elementary school. Monographs in parenting series. Mahwah, NJ: Lawrence Erlbaum Associates.
-
Pruett MK, Cowan CP, Cowan PA, Pruett KD (2009) Lessons learned from the supporting father involvement study: A cross-cultural preventive intervention for low-income families with young children. Journal of Social Service Research 35(2): 163-179.
-
Hunsley J, Lee CM (2007) Professional Psychology: Research and Practice 38(1): 21-33.
-
Vann N, Nelson-Hooks J (2000) Father-friendliness organizational self-assessment and planning tool 8: 2007.
-
Durlak JA, DuPre EP (2008) Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. American Journal of Community Psychology 41(3/4): 327-350.
-
Radloff LS (1977) The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological Measurement 1(3): 385-401.
-
Weisman O, Zagoory-Sharon O, Feldman R (2012) Oxytocin administration to parent enhances infant physiological and behavioral readiness for social engagement. Biological psychiatry 72(12): 982-989.
-
Cowan CP, Cowan PA (1990a) Who Does What? In: Touliatos JF, Perlmutter BF, Straus MA (Eds.) Handbook of Family Measurement Techniques Thousand Oaks: Sage Publications 447-448.
-
Abidin RR (1997) Parenting Stress Index: A measure of the parent-child system Zalaquett, In: Carlos P, Wood Richard John (1997) Evaluating stress: A book of resources. Lanham, MD: Scarecrow Education 277- 291
-
Norton R (1983) Measuring marital quality: A critical look at the dependent variable. Journal of Marriage and the Family 45(1): 141-151.
-
Heyman RE, Sayers SL, Bellack AS (1994) Global marital satisfaction versus marital adjustment: An empirical comparison of three measures. Journal of Family Psychology 8(4): 432-446.
-
Cowan CP, Cowan PA (1990b) Couple Communication Questionnaire. Institute of Human Development, Berkeley.
-
Cowan, PA, Cowan CP, Heming G (1995) Manual for the Child Adaptive Behavior Inventory (CABI). Unpublished manuscript, University of California, Berkeley.
-
Chester CE, Blandon AY (2016) Dual trajectories of maternal parenting stress and marital intimacy during toddlerhood. Personal Relationships 23(2): 265-279.
-
Crnic KA, Booth CL (1991) Mothers’ and fathers’ perceptions of daily hassles of parenting across early childhood. Journal of Marriage and Family 53(4): 1042-1050.
-
Kuczynski L, Kochanska G (1990) Development of children’s noncompliance strategies from toddlerhood to age 5. Developmental Psychology 26(3): 398-408.
-
Devault A, Gaudet J, Bolte C, St-Denis M (2005) A survey and description of projects that support and promote fathering in Canada: Still work to do to reach fathers in their real-life settings. Can J Commun Ment Health 24(1): 5-17.
-
Fixsen DL, Naoom SF, Blase K, Friedman RM, Wallace F (2005) Implementation research: A synthesis of the literature. National Implementation Research Network, University of South Florida, Louis de la Parte Florida Mental Health Institute.
-
Coley Rebekah L, Lindsay P, Chase-Lansdale (1999) Stability and change in paternal involvement among urban African American fathers. Journal of Family Psychology13 (3): 416-435.
-
Rienks SL, Wadsworth M E, Markman HJ, Einhorn L, Etter E (2011) Father involvement in urban low- income fathers: Baseline associations and changes resulting from preventive intervention. Family Relations 60(2): 191-204.
-
Teubert, D, Pinquart M (2010) The association between coparenting and child adjustment: A meta- analysis. Parenting: Science and Practice 10(4): 286- 307.
-
Schorr LB, Farrow F (2012) Expanding the universe: Doing better by knowing more. Working Strategies 15(2): 4.
-
Feinberg M E, Jones DE, Kan ML,Gosling MC (2010) Effects of family foundations on parents and children: 3.5 years after baseline. J Fam Psychol 24(5): 532- 542.
-
Cowan CP, Cowan PA, Heming G (2005) Two variations of a preventive intervention for couples: Effects on parents and children during the transition to elementary school. In: Cowan PA, Cowan C, Ablow JC, Johnson V, Measelle JR (Eds.) The family context of parenting in children's adaptation to elementary school : Lawrence Erlbaum Associates Mahwah, NJ 277-312.
-
Don BP, Biehle SN, Mickelson KD (2013) Feeling like part of a team Perceived parenting agreement among first-time parents. Journal of Social and Personal Relationships 30(8): 1121-1137.
-
Palkovitz R, Fagan J, Hull J (2013) Coparenting and Children’s Well-being. In: Cabrera NJ & Tamis- LeMonda CS (Eds.) Handbook of father involvement: Multidisciplinary perspectives: 202- 220 New York.
-
MacDonald K, Parke RD (1984) Bridging the gap: Parent-child play interaction and peer interactive competence. Child Development 55(4): 1265-1277.
-
Pruett M K, Williams TY, Insabella G, Little TD (2003) Family and legal indicators of child adjustment to divorce among families with young children. J Fam Psychol 17(2): 169.
-
Pruett MK, Cowan PA, Cowan CP, Pruett KD (2009) Fathers as resources in families involved in the child welfare system. Protecting Children 24(2): 54-65.
-
Weissman M, Sholomaskas D, Pottenger M, Prusoff B, Locke B (1977) Asssessing depressive symptoms in five psychiatric populations: A validation study. Am J Epidemiol 106(3): 203-214.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis