Which Strategies Facilitate Word Retrieval in Non-Fluent Progressive Aphasia? A Single Case Study
Non-fluent progressive aphasia (nfPPA) is the less studied variant of Primary Progressive Aphasia (PPA). Anomia treatments available in the literature seem to use a wide range of cueing paradigms, regardless the subtype of PPA. In this case study, we compare a semantic strategy with a phonological strategy on a confrontation naming task, in order to determine which one better compensate the anomia deficits in a patient with nfPPA. As hypothesized, the phonological strategy prompted better naming scores than the semantic strategy, likely because anomia in nfPPA is phonological based. Also, the patient revealed better word retrieval for objects and food, compared to animals. We suggest that successful treatments directed to PPA population should address the basis of the naming deficit by selecting learning strategies according to the impaired network.
Introduction
Primary progressive aphasia is the language variant of the neurocognitive disorders caused by frontotemporal lobar degeneration [1]. Patients diagnosed with PPA experience a progressive dissolution of language functions in the context of relatively preserved cognitive, memory and social skills for the first two years [2].
International consensus was established regarding the criteria used to diagnose the three subtypes of PPA – semantic variant (svPPA), agrammatic/non-fluent variant (nfPPA) and logopenic variant (lvPPA) [2]. They differ on the speech and language profile, and the pattern of brain atrophy on imaging tests. The semantic variant is characterized by impaired single-word comprehension and word retrieval. The discourse is considered fluent, which means the rate, grammatical content and oral motor abilities are maintained. These patients also present intact syntactic comprehension.
Individuals with non-fluent progressive aphasia present with slow speaking rate and effortful speech marked by agrammatism. Impaired comprehension of syntactically complex sentences is another feature of this variant. Patients exhibit phonemic and phonetic articulatory errors associated with apraxia of speech (AOS) [2, 3].
The logopenic progressive aphasia is diagnosed when the speech rate is slower compared to healthy adults, there are word-finding pauses and syntactic comprehension is largely impaired for complex structures. Sentence repetition is also compromised, as opposed to object knowledge that is relatively spared [2, 4].
Learning Mechanisms Applied to Anomia Treatment in PPA
The literature available to date shows that learning mechanisms used to treat naming deficits in PPA are broad enough to generate an effect that is transversal to all variants of the syndrome [5, 6]. However, the underlying cause of anomia differs across the variants [7] and therefore the learning mechanisms should be tailored to the features of each variant so that a bigger effect size could be accomplished. A scarce number of studies have planned the anomia treatment considering the variant presented by the participants [8, 9, 10]. More often the sample of the studies includes patients diagnosed with different variants of PPA [11, 12, 13], or even different diagnosis, such as progressive aphasia and aphasia resulting from stroke [14, 15]. In this case, the risk might be that the therapy addresses one’s deficits more successfully than the others.
Several learning strategies have been implemented in experimental studies targeting naming skills in PPA. The learning mechanisms can be grouped in the following clusters: i) simple repeated practice; ii) hierarchical cueing method; iii) spaced word retrieval; iv) semantic elaboration of concepts; v) mnemonic generation; vi) errorless vs. errorful learning paradigm; and vii) active vs. passive learning paradigm.
Simple repeated practice was reported in the study of Graham, Patterson, Pratt, & Hodges [16]. A former surgeon diagnosed with svPPA trained forgotten vocabulary through the repetition of lists of words and pictorial encyclopedias that contained labelled pictures, every day, for two weeks. Repeated rehearsal improved name production however, it failed to encourage the access to semantic information related to the trained items. The results of the study suggest that repeated rehearsal might be an option for non-fluent and logopenic variants, but not for semantic variant.
Hierarchical cueing method implements increasing or decreasing cues to prompt picture naming, depending on the study. The cues can be semantic, phonological and/or orthographic-based. An example of this approach is the Lexical Retrieval Cascade Treatment [12], used in two cases, one with the logopenic variant and another with the semantic variant. A sequence of carefully planned tasks engaged and strengthened the patients’ residual language skills, by facilitating the access to the central components of language processing. Increasing cues were provided in the following order: semantic self-cue > orthographic self-cue > phonemic self-cue > oral reading > repetition > semantic plausibility judgements > recall. The two patients showed beneficial effects mirrored by the ability to name the therapy assigned nouns. Following the same line, a model-oriented naming therapy delivered to a case of semantic progressive aphasia failed to reveal significant differences between naming performances on the set with semantic cues, compared to the set with phonological cues [17]. The cueing hierarchy for the phonological set predicted the addition of as many cues as the patient needed to name the target word: number of syllables > first sound > first syllable in the case of multisyllable words or sounds in case of single-syllable words > repetition. The cueing hierarchy for the semantic set comprised four levels: superordinate term > concept definition > semantic closure phrase > listening to the target word.
Spaced word retrieval strategy consists of confrontation naming of the same pictures with increasing time recall intervals, as well as producing the attribute related to each item. Bier and colleagues compared spaced word retrieval with simple word repetition and found no leverage of the first over the second [8]. Both strategies resulted in word relearning for the participant diagnosed with semantic progressive aphasia.
Mnemonic generation was used in the study of Dewar, Patterson, Wilson, & Graham [18], where a subject with svPPA was given photographs of famous people in the United Kingdom and required to name them, one at a time. Each photograph was presented accompanied by the corresponding written word and a semantic fact that were incorporated into a mnemonic. The mnemonic learning mechanism was associated with vanishing cues and expanded rehearsal techniques. After five sessions, the patient was able to recall the target words with a slight reliance on the cues. He also performed much better on category fluency tasks.
Semantic elaboration of concepts is the approach used in the Semantic Feature Analysis (SFA) implemented with a participant that suffered from severe non-fluent progressive aphasia [15]. The participant was required to name pictures representing objects and actions and was prompted with semantic information when he could not find the target word at the first attempt. Subsequent prompts were generated if needed, but after three attempts, the researcher produced the word and asked the patient to repeat. The participant benefited from this treatment, as he correctly named 14 nouns and verbs in a total of 15 after nine sessions. He also showed network expansion and recruited semantic processing areas to name the trained words, as seen in the fMRI performed pre- and post-treatment. The authors suggest that SFA seems to enable brain plasticity changes in degenerative- based anomia, through functional reactivation and reorganization.
A comparison between errorless vs. errorful and active vs. passive learning was conducted by Jokel & Anderson [19]. The participants with semantic variant responded better to errorless learning than errorful. No differences were found between active and passive learning, regarding their role in restoring lexical representations.
Ever since, the evidence pointed to the fact that errorless learning induced more gains than errorful learning, other authors used errorless strategy to treat anomia in PPA [20, 21, 22].
Clinic pathological characteristics of nfvPPA
Neurodegenerative-based aphasia derives from a wide range of pathologies. Among the most typical are frontotemporal lobar degeneration (FTLD), Alzheimer’s disease (AD) and other tauopathies (e.g., corticobasal degeneration, Pick’s disease). The literature shows that up to 30% of nfvPPA cases present AD etiology and approximately 20% of nfvPPA present FTLD etiology. Grossman estimated that the prevalence of nfvPPA due to FTLD is 0.5-3.0 per 100,000 and incidence is 0.4-0.7 per 100,000.
The hallmark of nfvPPA is effortful and halting speech output due to agrammatism along with word-finding pauses [23]. The speech is predominantly marked by grammatical and speech sound errors. While healthy adults typically produce 140 words per minute, these patients generate an average of 45 words per minute [24]. Apraxia of speech is commonly a co-occurring disorder [25]. Impaired syntactic comprehensions is not present at the onset but emerge with the disease progression, as well as, reduced sentence complexity [2]. In these patients, prosody is also affected, as rhythm and melody change. Other clinical features include surface dyslexia and surface dysgraphia. The phonological and syntax dissolution gradually worsens until patients become mute [26] and dependent on assisted communication [27]. Content word comprehension and object knowledge are considered spared.
Researchers have pointed out variable pathology underlying nfvPPA [26]. Progressive nonfluent aphasia might be associated with tau-positive pathology [28]; dementia with Pick bodies pathology [29]; AD pathology [30, 31]; FTLD-U pathology [32]; FTLD-TDP pathology [33]; dementia with Lewy bodies [31]; progressive supranuclear palsy and corticobasal degeneration [34].
When it comes to the PPA management, the most studied variant is the semantic one. There are substantially less studies that investigated the effects of anomia treatment and learning mechanisms in nfPPA. Thus, the aim this study is to determine the learning strategy that offers more gains in patients diagnosed with nfvPPA. Based on the supporting evidence from the literature, we hypothesize that an individual with non- fluent progressive aphasia will respond better to a phonological cueing approach than a semantic one.
Methods
This single-case study was conducted in a subject diagnosed with nfvPPA, following the consensus criteria established by Gorno-Tempini and colleagues and DSM-5 [1, 2]. The individual was required to speak European- Portuguese, be monolingual and literate. Exclusion criteria were inability to complete a comprehensive language evaluation and take cognitive-enhancing medication. The patient signed an informed consent to participate in this study, which was approved by the Ethics Committee of the Nursing School of Coimbra – Health Sciences Research Unit (UICISA:E), Portugal (reference P351-06/2016).
We first present the case history, then describe the patient’s performance on language and neuropsychological assessment, and finally report the procedures adopted in this study.
Case report
FP is a 60-year-old, right-handed, active Accountant who owes a business with his wife. He is a native speaker of European-Portuguese with a bachelor’s degree.
There was a 2-year history of speech and language deterioration when FP was first diagnosed with nfvPPA associated with apraxia of speech and ideomotor apraxia of the superior limbs, in January of 2017. The Neurologist reported increasing language impairment characterized by non-fluent speech, inconsistent semantic and phonologic errors, and major difficulties in tasks that involve reading and writing. Soft depression symptoms were identified as a comorbidity.
By the time he entered the study, he was completely independent on his daily living. He used to drive by himself, go to work every day, carry out his personal hygiene, shop for groceries at the supermarket, manage the family budget and ride the bike to exercise as suggested by the doctor. As the speech became less fluent and paraphasic, some adjustments were made in his job setting. For example, he kept working at the computer and doing the paperwork but someone else would handle the communication with the clients.
Baseline assessment
A comprehensive evaluation was conducted by a speech-language pathologist (SLP) blind to the experiment, to establish the patient’s neurocognitive and language profile. FP scored 23 (Maximum score=30) at the Mini Mental State Examination (MMSE) [35], showing an initial cognitive impairment. He failed on tasks of orientation to time, word recall, confrontation naming, and sentence writing. A picture description task [36] used to analyze spontaneous speech revealed a non-fluent discourse marked by phonemic, phonologic and semantic paraphasias, word finding pauses, effortful articulation and stereotyped expressions. The application of the Lisbon Aphasia Examination Battery (BAAL) [37, 38] showed impaired object naming and repetition, surface dyslexia and dysgraphia, relatively preserved comprehension of oral commands, and intact object recognition. The patient achieved a 39% percentage of correct answers at the Snodgrass and Vanderwart naming test [39], which showed impaired picture naming. The performance on neurocognitive and language tasks can be found in Table 1.
| Score achieved/Total | |
|---|---|
| Task (test) | |
| score | |
| Language Production | |
| Spontaneous speech | Non-fluent, anomic, paraphasic, effortfull |
| Picture description (BAAL) | Informative |
| Automatic discourse (BAAL) | Impaired |
| Picture naming (Snodgrass & Vand. Test) | 86/219 |
| Object naming (BAAL) | 7/16 |
| Word repetition (BAAL) | 18/30 |
| Number repetition (BAAL) | 3/14 |
| Sentence repetition (BAAL) | 5/14 |
| Language Comprehension | |
| Object identification (BAAL) | 16/16 |
| Comprehension of simple commands (BAAL) | 14.5/16 |
| Token test (BAAL) | 15/21 |
| Reading | |
| Letter recognition (BAAL) | 6/10 |
| Letter reading (BAAL) | 0/10 |
| Letter pairing (BAAL) | 10/10 |
| Object/word matching (BAAL) | 12/16 |
| Word reading (BAAL) | 7/16 |
| Word recognition (BAAL) | 15/16 |
| Text comprehension (BAAL) | 5/6 |
| Spelling | |
| Writing letters to dictation (BAAL) | 1/5 |
| Writing words to dictation (BAAL) | 1/5 |
| Writing sentences to dictation (BAAL) | 0/2 |
| Leter copying (BAAL) | 5/5 |
| Word copying (BAAL) | 3/5 |
| Sentence copying (BAAL) | 0/2 |
| Spontaneous writing (BAAL) | Impaired |
| Cognitive screening (MMSE) | 23/30 |
| Other | |
| Motor speech programming (BAAL) | 4/14 |
| Upper limbs motor programming (BAAL) | 11/22 |
| Visual perception and construction (BAAL) | Impaired |
Table 1: Results of pre-experimental neuro language testing.
Procedures
The main purpose of this study was to assess the best strategy for word retrieval in non-fluent progressive aphasia. Therefore, two lists of words were built, one to test naming accuracy after semantic cueing (responsive naming) and the other to assess naming response towards phonologic cueing (first syllable). Each list consisted of 33 items balanced for semantic category. Initially, picture naming was evaluated three times in different days and only the words FP failed to name at least two times in the absence of cues were included in the experimental corpus. The words chosen were objects, food, and animals. Different words took part of each list in order to avoid a repetition effect (Appendix 1). The target items were displayed in the center of a computer screen using a power point presentation. A written cue – semantic or phonological – was placed underneath each colored photograph representing the target words. An example of a semantic cue for the word ‘popcorn’ would be: “I watch a movie and eat [popcorn]”. The phonological cue for the word ‘penguin’ would be “pen-“. FP was required to look at the picture, listen to the cue and then name the target word within 30 seconds. One point was given for each correct answer and zero points were given for each incorrect answer or no response. When the patient produced more than one attempt to name the target word, only the first attempt was considered.
We considered a pre-test, the task in which the patient was required to name a list of words in the absence of cues and post-test, the task in which FP had to name the same list of words with the help of either semantic or phonological cues.
Statistical Analysis of Behavioral Data
Comparison between the pre-test and post-test trials were conducted using the McNemar test (naming score). A p-value of 0.05 was considered. The comparison of naming performance across the three semantic categories was calculated by the mean of naming score achieved in each category at post-test.
Result
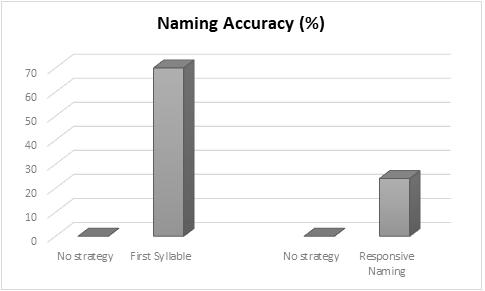
A McNemar Test revealed significant differences for naming performance after semantic and phonological strategies (p<0.05). The participant responded better to the phonological strategy (n=23/33 correct answers) than the semantic one (n=8/33 correct answers). The percentage of accuracy corresponded to 70% when the first syllable was provided and 24% when the semantic context of the target word was provided. During the testing session, the participant also took less time to retrieve the words associated with the phonological cue when compared to the words associated with the semantic cue.
Regardless the strategy implemented, FP revealed better naming score for objects (M=0.65), then food (M= 0.56) and at last animals (M=0.18).
The hypothesis stated at the introduction section was confirmed by the results of the statistical analysis.
Discussion
This study aimed to test the response of a patient with nfvPPA to two different strategies used to facilitate word retrieval. The findings support our hypothesis that the phonological strategy would be associated with a better naming performance.
The results are supported by a study where two participants with nfvPPA were exposed to a computer- based program designed to treat anomia – MossTalk Words [9]. The cued naming module was used to prompt single word production. The authors of the study tailored a cueing hierarchy system consisting of written initial letter, written entire word, and oral repetition. The subjects showed a significant increase of naming accuracy for trained items.
Another study used the semantic feature analysis (SFA) therapy to improve naming performance on a patient with nfPPA [15]. The patient was required to name a picture presented visually and when he could not retrieve the target word, semantic features were provided by the SLP. When the participant reached the three failed attempts to name the target word, the word was produced orally by the SLP and the patient was asked to repeat. The therapy not only allowed word relearning but also triggered the activation of semantic processing areas and network expansion.
SFA approach was built on the fundamentals of the spreading activation theory [40]. This theory stands that the activation of semantic characteristics of a target word leads to the activation of the word’s semantic network, which consequently results in the activation of the corresponding phonological knowledge and word production. On the light of the spreading activation theory, the stimulation of the semantic areas has an effect that is transversal to all language processing levels, among which we can include phonological processing and oral- motor planning. According to the results of this case- report, we suggest that despite the activation of semantic rote improves a large scope of language domains, if the damage is phonological-rooted, the anomia treatment should use a phonological hierarchical cueing paradigm, so that the effect is greater and immediate. The findings of our study pointed out that the phonological strategy is more powerful than the semantic one, when anomia is caused by a phonological processing impairment.
Naming deficits are the primary feature of all PPA variants and the underlying cause can be semantic in the case of svPPA or phonological in the case of lvPPA and nfvPPA. The key for successful management of anomia is to address its basis by selecting the learning strategies according to the impaired network.
This study poses some limitations that should be addressed. As a case study, the results are not representative of all individuals diagnosed with non- fluent progressive aphasia. We used different lists of words to test the semantic and phonological cueing strategies, which might or might not have introduced some bias in the results. However, the decision was taken in order to prevent the patient from memorizing the words. Even if the trials were carried out at different time points, there was a possibility that the participant could remember the list used to test the semantic strategy and showed an outstanding performance at the same list used to test the phonological strategy.
Future studies should investigate the learning paradigms that better serve each one of the PPA variants, considering the deficits associated with each variant and the pathological correlates. A valuable information like this could assist the health professionals planning anomia treatment in clinical settings.
References
-
American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th (Edn.), Washington: American Psychiatric Association.
-
Gorno-Tempini M, Hillis A, Weintraub S, Kertesz A, Mendez M, et al. (2011) Classification of primary progressive aphasia and its variants. Neurology 76(11): 1006-1014.
-
Josephs K, Duffy J (2008) Apraxia of speech and non- fluent aphasia: A new clinical marker for corticobasal degeneration and progressive supranuclear palsy. Current Opinion in Neurology 21(6): 688-692.
-
Gorno-Tempini M, Brambati S, Ginex V, Ogar J, Dronkers N, et al. (2008) The logopenic/phonological variant of primary progressive aphasia. Neurology 71(16): 1227-1234.
-
Cadório I, Lousada M, Martins P, Figueiredo D (2017) Generalization and maintenance of treatment gains in primary progressive aphasia (PPA): A systematic review. International Journal of Language and Communication Disorders 52(5): 543-560.
-
Croot K, Nickels L, Laurence F, Manning M (2009) Impairment- and activity/participation-directed interventions in progressive language impairment: Clinical and theoretical issues. Aphasiology 23(2): 125-160.
-
Henry M, Wilson S, Babiak M, Mandelli M, Beeson P, et al. (2016) Phonological processing in primary progressive aphasia. Journal of Cognitive Neuroscience 28(2): 210-222.
-
Bier N, Macoir J, Gagnon L, Linden M, Louveaux S, et al. (2009) Known, lost, and recovered: Efficacy of formal-semantic therapy and spaced retrieval method in a case of semantic dementia. Aphasiology 23(2): 210-235.
-
Jokel R, Cupit J, Rochon E, Leonard C (2009) Relearning lost vocabulary in nonfluent progressive aphasia with MossTalk Words. Aphasiology 23(2): 175-191.
-
Robinson S, Druks J, Hodges J, Garrard P (2009) The treatment of object naming, definition, and object use in semantic dementia: The effectiveness of errorless learning. Aphasiology, 23(6): 749-775.
-
Croot K, Taylor C, Abel S, Jones K, Krein L, et al. (2014) Measuring gains in connected speech following treatment for word retrieval: A study with two participants with primary progressive aphasia. Aphasiology 29(11): 1265-1288.
-
Henry M, Rising K, DeMarco A, Miller B, Gorno- Tempini M, et al. (2013) Examining the value of lexical retrieval treatment in primary progressive aphasia: Two positive cases. Brain Language 127(2): 145-156.
-
Newhart M, Davis C, Kannan V, Heidler-Gary J, Cloutman L, et al. (2009) Therapy for naming deficits in two variants of primary progressive aphasia. Aphasiology 23(7-8): 823-834.
-
Henry M, Beeson P, Rapcsak S (2008) Treatment for lexical retrieval in progressive aphasia. Aphasiology 22(7-8): 826-838.
-
Marcotte K, Ansaldo A (2010) The neural correlates of semantic feature analysis in chronic aphasia: Discordant patterns according to the etiology. Seminars in Speech and Language, 31(1): 52-63.
-
Graham K, Patterson K, Pratt K, Hodges J (2001) Can repeated exposure to “forgotten” vocabulary help alleviate word-finding difficulties in semantic dementia? An illustrative case study. Neuropsychological Rehabilitation 11(3-4): 429-454.
-
Dressel K, Huber W, Frings L, Kümmerer D, Saur D, et al. (2010) Model-oriented naming therapy in semantic dementia: A single-case fMRI study. Aphasiology 24(12): 1537-1558.
-
Dewar BK, Patterson K, Wilson B, Graham K (2009) Re-acquisition of person knowledge in semantic memory disorders. Neuropsychological Rehabilitation 19(3): 383-421.
-
Jokel R, Anderson ND (2012) Quest for the best: Effects of errorless and active encoding on word re- learning in semantic dementia. Neuropsychological Rehabilitation 22(2): 187-214.
-
Frattali C, Kang, Y (2004) An errorless learning approach to treating dysnomia in frontotemporal dementia. Journal of Medical Speech - Language Pathology 12(3): 11-24.
-
Jokel R, Rochon E, Anderson N (2010) Errorless learning of computer-generated words in a patient with semantic dementia. Neuropsychological Rehabilitation 20(1): 16-41.
-
Savage S, Ballard K, Piguet O, Hodges J (2013) Bringing words back to mind - Improving word production in semantic dementia. Cortex 49(7): 1823-1832.
-
Gunawardena D, Ash S, McMillan C, Avants B, Gee J, et al. (2010) Why are patients with progressive nonfluent aphasia nonfluent? Neurology 75(7): 588- 594.
-
Grossman M, Powers J, Ash S, McMillan C, Burkholder L, et al. (2013) Disruption of large-scale neural networks in non-fluent/agrammatic variant primary progressive aphasia associated with frontotemporal degeneration pathology. Brain and Language 127(2): 106-120.
-
Jung Y, Duffy J, Josephs K (2013) Primary progressive aphasia and apraxia of speech. Seminars in Neurology 33(4): 342-347.
-
Fried-Oken M, Rowland C, Gibbons C (2010) Providing augmentative and alternative communication treatment to persons with progressive nonfluent aphasia. Perspectives on Neurophysiology and Neurogenic Speech and Language Disorders 20(1): 21-25.
-
Grossman M (2010) Primary progressive aphasia: Clinicopathological correlations. Nature Reviews Neurology 6(2): 88-97.
-
Josephs K, Duffy J, Strand E, Whitwell J, Layton K, et al. (2006) Clinicopathological and imaging correlates of progressive aphasia and apraxia of speech. Brain 129(6): 1385-1398.
-
Yokota O, Tsuchiya K, Arai T, Yagishita S, Matsubara O, et al. (2009) Clinic pathological characterization of Pick’s disease versus front temporal lobar degeneration with ubiquitin/TDP-43-positive inclusions. Acta Neuropathologica 117(4): 429-444.
-
Grossman M, Xie S, Libon D, Wang X, Massimo L, et al. (2008) Longitudinal decline in autopsy-defined frontotemporal lobar degeneration. Neurology 70(22): 2036-2045.
-
Kertesz A, McMonagle P, Blair M, Davidson W, Munoz D (2005) The evolution and pathology of frontotemporal dementia. Brain 128(9): 1996-2005.
-
Knopman D, Boeve B, Parisi J, Dickson D, Smith G, et al. (2005) Antemortem diagnosis of frontotemporal lobar degeneration. Ann. Neurology 57(4): 480-488.
-
Snowden J, Neary D, Mann D (2007) Frontotemporal lobar degeneration: clinical and pathological relationships. Acta Neuropathologica 114(1): 31-38.
-
Josephs K, Peterson R, Knopman D, Boeve B, Whitwell J, et al. (2006) Clinicopathologic analysis of frontotemporal and corticobasal degenerations and PSP. Neurology 66(1): 41-48.
-
Folstein M, Folstein S, McHugh P (1975) Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research 12(3): 189-198.
-
Goodglass H, Kaplan E (1972) Assessment of Aphasia and Related Disorders. Philadelphia: Lea and Febinger.
-
Damásio A (1973) Neurologia da linguagem. PhD Thesis presented to the Lisbon Faculty of Medicine.
-
Castro-Caldas A (1973) Diagnóstico e evolução das afasias de causa vascular. PhD Thesis presented to the Lisbon Faculty of Medicine
-
Ventura (2003) Normas para figuras do corpus de Snodgrass e Vanderwart (1980). Laboratório de Psicologia 1(1): 5-19.
-
Collins A, Loftus E (1975) A spreading activation theory of semantic processing. Psychological Review 82(6): 407-428.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis