What do we know about Music Interventions for Fibromyalgia?
Fibromyalgia (FM) is a complex chronic disease, characterized by a widespread chronic pain condition in pressure points located at specific muscle and tendon sites and frequently associated with a variety of dysfunctions such as persistent fatigue, sleep disorders, different types of headache, anxiety and mood disorders. To address clinical symptoms, various treatments have been proposed: pharmacological and non-pharmacological intervention based on an individualized treatment program. As for non-pharmacological intervention it is possible to find many researches evaluating music therapy or music interventions on FM patients. Therefore, the aim of this review was to observe the findings of the available music therapy interventions in FM and to portrait a state-of-the-art on the subject. To identify suitable publications, an online search of PubMed database was conducted with the following keywords: “Music therapyâ€, “Musicâ€, “Music intervention†and “Fibromyalgiaâ€. We therefore selected only the experimental studies containing music therapy for FM patients. Amongst the twelve analyzed studies the majority of them have successfully applied music therapy, showing a positive improvement of quality of life and pain reduction. Moreover, as far as instruments uniformity between the studies is concerned, measurement of pain is fairly uniform; on the contrary, we detect heterogeneity concerning other measures. Furthermore, future studies, including in the intervention protocol a music preference questionnaire, are needed to personalize the participants experience and increase adherence to the intervention. For future research, we highlight the relevance of a defined music therapy protocol, also in the form of passive listening, possibly in agreement with the World Federation of Music Therapy guidelines on music therapy interventions.
Introduction
Fibromyalgia Syndrome
Fibromyalgia [FM] or fibromyalgia syndrome, is a complex chronic disease, characterized by a widespread chronic pain condition in pressure points located at specific muscle and tendon sites, called tender points, and frequently associated with a variety of dysfunctions such as persistent fatigue, sleep disorders, different types of headache, anxiety and mood disorders [1].
Although the etiopathogenesis of FM is still unclear, the most accredited hypothesis concerns the mechanism of pain centralization; in fact, many studies have define it as a central sensitization disease that mainly affects the neurocircuits involved in the perception, transmission and processing of afferent pain stimuli [2].
Due to the painful condition in which FM patients live, both cognitive and psychological components interacting and influencing the experience of pain must be considered of primary importance. There are several cognitive variables that play an important role in the perception and management of pain, such as self-efficacy, catastrophizing and rumination [3, 4, 5]. Furthermore, the behavioral response to pain in FM patients appears to be influenced by the general knowledge of their state of health, in particular by incorrect beliefs regarding the origin of the FM pain and its chronicity and inevitability [6].
Anxiety disorders and depression are the most frequently observed psychiatric comorbidities among these patients [7]. FM also appears to be a risk factor for the development of a distress related condition [8].
Despite the difficulties in identifying both a correct etiopathogenesis of the disease and a decisive intervention, the optimal FM treatment strategy should consider an interdisciplinary and multi-professional approach aimed at improving the quality of life, severely compromised in most of these patients [9]. For example, a recent study has shown how patient education, such as information about the nature, possible causes and contributing factors of the disease, represents an effective treatment in FM. Moreover, it is demonstrated that psycho-education in combination with empowering programs provides a positive impact on patients’ quality of life [4]. Furthermore, the recent literature has highlighted that the most indicated therapeutic approaches should be based on an individualized treatment program which includes different types of pharmacological and non-pharmacological interventions [10].
Definition and Conceptualization of Music Therapy Interventions
In regards to non-pharmacological intervention, many researchers have identified the following interventions as effective integrative interventions in FM patients: psychotherapy, mindfulness, acceptance and commitment therapy (ACT), and art therapy.
In particular, art therapy seems to have a positive impact on the quality of life in the clinical population considered. Art therapy uses the potential that each person possesses to creatively elaborate all those sensations that cannot be brought out in words in everyday contexts. The artistic component of therapy include visual art forms such as painting, acting, dancing or listening music. In this context, Baptista [11] and colleagues suggested that the practice of art therapy might be considered as an effective therapeutic strategy in the treatment of FM in order to reduce the intensity level of perceived pain and decrease the levels of depression, consequently improving patients’ quality of life.
In regard to music therapy, the American Music Therapy Association (AMTA) has highlighted the importance of this intervention and stated what follows: music therapy is “the clinical and evidence-based use of music interventions within a therapeutic relationship to accomplish individualized goals by a credentialed professional who has completed an approved music therapy program” [12].
Moreover, the World Federation of Music Therapy (WFMT) recognized five different music therapy application models, which refers to different psychological directions:
- Benenzonian Music Therapy: is an active music therapy technique, characterized by free improvisation and based mainly on the observation of how the patient is able to express himself in a non-verbal and non- directive way through the free use of musical instruments. For this type of approach, it is crucial to identify in the first place the so-called ISO, or sound identity, which represents the sound experience of each individual, of an intermediary object and an integrating object [13].
- Creative music therapy: is an active music therapy technique that allows the enhancement of the expressiveness and communication of the subjects. It has been showed that this intervention may promote significant reduction in pathological behavior [14].
- Analytical Music Therapy: is an intervention characterized by an introspective analysis of the patient with the aim to alleviate internal conflicts and promoting inner growth [15].
- Cognitive and behavioral music therapy: is an intervention which combines cognitive behavioral therapy with the application of active and passive- receptive music therapy techniques.
- The GIM (Guided Imagery and Music): is a type of receptive approach that uses relaxation techniques and music. Its aim is to explore the potential of imagination to induce emotional and affective responses [16].
The use of music therapy can have different effects, which may depend on the intrinsic characteristics of the intervention but also personal features such as age, culture, health conditions, musical attitude and life experiences [17]. Music therapy seems to be associated with a decreased stress level [18, 19], emotional regulation and a reduction of depressive symptoms [20, 21, 22], better sleep quality [23] and an “audio analgesia” effect, also called music-induced analgesia (MIA) [24, 25, 26].
The aim of this review was to observe the findings of the available music therapy interventions in FM and to portrait a state-of-the-art on the subject.
Music Therapy as a Non-Pharmacological Intervention for FM
Methods
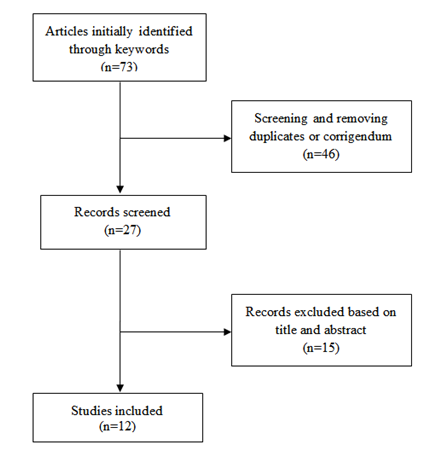
We searched the PubMed database with the following keywords: “Music therapy”, “Music”, “Music intervention” and “Fibromyalgia”. We selected only the experimental studies containing the music therapy intervention in FM patients and English or Italian articles published in the last 10 years. The exclusion criteria were: reviews, theoretical studies and meta-analysis. Our search yielded a total of 73 hits. During the selection phase (Figure 1), duplicates were removed (46) and we screened 27 records. Of these, 15 were excluded after titles and abstracts reading leaving a total of 12 full-text articles assessed for eligibility. At the end of our research we selected those 12 articles, shown in Table I, that we analysed for our review. In figure 1 is presented the selection phase of the studies.
| Authors | Title | Year | No. | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alparslan, et al. | Effects of music on pain in patients with fibromyalgia | 2016 | 27 | ||||||||
| Braun Janzen, et al. | A parallel randomized controlled trial examining the effects of rhythmic sensory stimulation on fibromyalgia symptoms | 2019 | 28 | ||||||||
| Espí-López, et al. | Effect of low-impact aerobic exercise combined with music therapy on patients with fibromyalgia. A pilot study | 2016 | 29 | ||||||||
| Garza-Villarreal, et al. | Music reduces pain and increases functional mobility in fibromyalgia | 2014 | 30 | ||||||||
| Garza-Villarreal, et al. | Music reduces pain and increases resting state fMRI BOLD signal amplitude in the left angular gyrus in fibromyalgia patients | 2015 | 31 | ||||||||
| Guétin, et al. | The Effects of Music Intervention in the Management of Chronic Pain | 2012 | 32 | ||||||||
| Linnemann, et al. | The effects of music listening on pain and stress in the daily life of patients with fibromyalgia syndrome | 2015 | 19 | ||||||||
| Mercadíe, et al. | Effects of Listening to Music versus Environmental Sounds in Passive and Active Situations on Levels of Pain and Fatigue in Fibromyalgia | 2015 | 33 | ||||||||
| Onieva-Zafra, et al. | Effect of Music as Nursing Intervention for People Diagnosed with Fibromyalgia | 2013 | 34 | ||||||||
| Picard, et al. | Music as a sleep aid in fibromyalgia | 2014 | 35 | ||||||||
| Torres | Randomized Trial of a Group Music and Imagery Method (GrpMI) for Women with Fibromyalgia | 2018 | 36 | ||||||||
| Weber, et al. | Effects of Music in Combination with Vibration in Acupuncture Points on the Treatment of Fibromyalgia | 2015 | 37 |
Table 1: Studies examined in this review.
Results
Study Designs, Experimental Measures and Sample Sizes
Of the above mentioned selected articles, six studies are randomized controlled trials (RCT) [27, 28, 32, 34, 36, 37], three studies have a pretest-posttest design [30, 31, 33] and there are both two pilot studies [29, 35] and an assessment study [19]. In regard of measurements, all the studies take into consideration different domains both of a psychological and a medical nature. In particular, pain severity and perception are measured with the Visual Analog Scale (VAS) [27, 32, 33, 34], the Fibromyalgia Impact Questionnaire (FIQ) [28, 29, 35, 36, 37], the Verbal Rating Scale (VRS) [30, 31], the Face Pain Scale (FPS) [29], the Brief Pain Inventory - Short Form [28] and the Mc Gill Pain Questionnaire (MPQ) [19, 34, 36]. Two studies measure the tendency of catastrophizing pain with the Pain Catastrophizing Scale (PCS) [30, 31]. Most of the studies include anxiety and depression measures such as the Beck Depression Inventory (BDI) [29, 34], the Hospital Anxiety and Depression scale (HADS) [32], the Center for Epidemiologic Studies Depression Questionnaire and its revised version (CES-D) (CESD-R) [30, 31], the Patient Health Questionnaire (PHQ) [34, 28], the State-Trait Depression Questionnaire (ST/DEP) [36] and the State-Trait Anxiety Inventory (STAI) [36]. Overall, health measures are represented by general health and wellbeing scales such as the Psychological Wellbeing Scale (PWS) [36], the Health Assessment (HAQ) [37] and the Quality of Life Enjoyment and Satisfaction – Short Form [28], while participant’s perceived benefit is measured with the Adapted Glasgow Benefit Inventory (GBI) [28] and the Patient Global Impression of change (PGI-C) [28, 35]. Music preference is observed a priori and a posteriori in two studies, either through participant’s choice on a listening device [8] or with the Music Preference Questionnaire (MPQ) [19].
Regarding sample size, the mean number of participants for our selected studies (only experimental group condition) is 33,83 included in a range that goes from a minimum of 20 to a maximum of 90.
Regarding Music Component
All the included studies have showed a musical component at an experimental level, with rather important differences as regards the number of sessions applied, the experimental setting and the duration of music reproduction, while the differences decrease when the type of music selected is observed. In particular, the number of sessions applied vary from 1 to 60 and the experimental setting consisted in individual sessions at home with a given device [19, 27, 28, 32, 33, 34, 35] or an experimental controlled setting [29, 30, 31, 36, 37]. The duration of the music reproduction varied from a minimum of 5 to a maximum of 120 minutes per session. In regard to music type choice, most of the studies include either classical music [33, 34, 37], relaxation music [27, 32] or highly pleasant, slow paced, self-chosen music [19, 30, 31]. Eventually, some studies include a standard music or noises selection [29, 34, 35, 36].
Results Overview: RCT, Pre-Post, Assessment and Pilot Studies
RCT
Alparlsan and colleagues conducted a RCT study with the aim to evaluate the effects of music therapy on pain perception in FM patients [27]. The findings suggest that this intervention was effective in reducing pain perception in FM patients compare to the control group, which results were similar to the experimental group but not significant. Similarly, Guétin, et al. [32] combined two different types of music interventions on FM patients using a new technique, to assess its effect on chronic pain and on other variables such as anxiety, depression, the consumption of analgesics and other kind of medications. The results showed a significant positive impact of music listening on pain levels and on all the variables mentioned above, indicating a prolonged effect of pain reduction up to 1 month after the end of the intervention. Similar findings were detected by Onieva-Zafra [34] which observed a pain reduction after music listening session, performed at least once a day for approximately two weeks. Janzen, et al. [28] investigated the effects of gamma-frequency rhythmic sensory stimulation. Patients underwent two different types of treatment: a vibrotactile stimulation and a random and intermittent complex wave gamma-range vibrotactile stimulation. The results showed a reduced interference of pain in patients’ functioning (for example in general activity or walking ability) and also improved depression levels and sleep quality. The authors also highlight that no significant difference was found between the two treatment parameters’ groups, which in fact were based on a similar mechanism of action. Using a different type of music stimulation (Group Music and Imagery intervention; GrpMI), Torres and colleagues [36] combined psychological and artistic interventions for FM patients. Participants would attend lessons were relaxation exercises, music listening, verbal sections and creative drawing were required. The whole process was constantly monitored with observational techniques, allowing the instructor to adapt and personalize the experience. Findings of this study after the experimental sessions were of a reduced pain influence in patients functional capacity and health, pain perception, anxiety and depression. These benefits persisted after three months from the end of the intervention with reported significant improvement across all variables (except of the state anxiety and state depression measures). In another study, Weber and colleagues [37] analyzed the effect of music listening and vibration (mechanical sound wave and classical/relaxation music) on acupuncture points in patients with FM with the aim of determining whether these interventions relieved the pain and improved patients’ daily functions. The results of this research showed that all the groups exhibited a significant improvement, suggesting a remarkable placebo effect. Moreover, a significant difference in improvements between the “complete” group (music and vibration) and the others was revealed through the intragroup comparison, in particular for the FM impact on daily life and on general health.
Pretest-Posttest
Mercadíe and colleagues [33] focused their research on the emotional impact of music on subjective pain perception, giving all participants a listening device with the possibility of choosing a passive or active type of listening and two different types of sounds, both music and environmental sounds. The results of this study confirm a pain and fatigue reduction at the end of the treatment. Moreover, both music and environmental sounds produced similar pain reduction effect suggesting that it may exhibit the same therapeutic effect through the distraction process. Garza-Villareal and colleagues [30] presented to their patients both self-chosen, relaxing and familiar music and a control auditory condition with the aim of determining whether this kind of therapy could be of any benefit on symptoms and/or on functional mobility in FM patients. The results suggest that music therapy is an effective intervention in pain reduction and it may promote functional mobility. Additionally, improved functional mobility seems to be influenced by MIA. In this regard, Garza-Villareal and colleagues [31] have evaluated the neural correlates of MIA in FM patients. The experiment required the application of resting state functional magnetic resonance imaging (rsfMRI) before and after music or pink noise listening. Results of this study confirm the positive effects of music therapy in pain reduction. caused by music listening in FM patients, which seem to be related to an increased amplitude of the low frequency BOLD (blood oxygen level-dependent) signal fluctuations in the left angular gyrus (lAnG) and to a top- down regulation of the pain modulatory network by the default mode network (DMN).
Assessment and Pilot Studies
Several studies have found that interventions based on music therapy may induce general improvement in FM symptoms, particularly on sleep quality [28]. In regard to it, Picard and colleagues [35] tried to identify the effect of music on sleep. After four weeks of treatment, the results showed a significant improvement of sleep quality, improved general health and a reduction of symptoms associated to FM. Linnemann and colleagues [19] investigated whether the pain level can be reduced by mere music listening, and if this improvement could be explained by biological stress-responsive systems’ action, through salivary cortisol analysis. Similarly to a previous examined study [28], Linnemann found a more significant positive effect on perceived control over pain than on the perceived pain severity itself. Furthermore, the authors hypothesized that both the activation and relaxation component activated by music can induce an increased control over pain. Espí-López and colleagues [29] have investigated the effect combining therapeutic aerobic exercise with music therapy on depression, quality of life, general discomfort and balance variations. The results showed that low impact aerobic exercise in combination with music therapy proved a better beneficial therapeutic effect on FM symptoms when compared with the other conditions, while no intervention wasn’t beneficial.
Discussion and Conclusion
The main purpose of this review was to observe the main findings of the available music therapy interventions in FM while. The majority of the analyzed studies have investigated different components of pain, quality of life and the impact of symptomatology on everyday life. Almost all studies have reported significant improvements on these domains.
In particular, with regard to the pain component, several authors have observed that in FM the pain can be measured both on a state scale (perceived pain) and on its perceived control. Most of the studies reported an ameliorated pain perception [27, 30, 32, 33, 34, 35, 36] while others an improvement in the perceived control of pain [19, 28].
The measurement of pain is fairly uniform in different studies, since we detected the use of widely validated measures in clinical practice, comparable to each other.
However, we observed a heterogeneity regarding the other measures (quality of life, quality of sleep, general health assessment etc.) that could lead to a hindrance in the comparison between the different studies’ results. For this reason and for future reviews and meta-analysis, it would certainly be interesting to increase the homogeneity of the instrumentation used to measure the psycho-physiological variables. Moreover, regarding music selection, we observed that only one research [19] presented a music preference questionnaire to the FM patients’ sample in the pre-test phase, which we consider a fundamental aspect of the music intervention therapeutic effect. Future studies, including in the intervention protocol also this kind of measurement are needed to personalize the participants experience and increase adherence to the intervention [38, 39, 40, 41, 42, 43, 44].
Regarding the choice of music selection, some reflections are necessary. The first observation is that the type of music intervention used in the selected works does not contain indications about belonging to a certain type of music therapy, as exposed in the introduction of our work [45, 46, 47, 48, 49, 50, 51, 52]. The fact that the aforementioned music therapy has not yet been clearly defined certainly represents a problem for its application, but, at the same time, our impression is that these studies use music as an instrument, mentioning the therapeutic component not in the selection process of the musical pieces but only in the effects discussions. Moreover, most of the selected studies used music through self-administration without the facilitation of an experienced music therapy instructor, and a type of passive intervention such as simply listening was offered. From this analysis, for future research, we highlight the relevance of a defined music therapy protocol, also in the form of passive listening, possibly in agreement with the World Federation of Music Therapy guidelines on music therapy interventions [53, 54, 55].
Furthermore, the effectiveness of an intervention with music certainly contains several variables that are difficult to isolate; in fact, the different authors wondered if the effect of the intervention could be due to a relaxation or activation response, distraction, stress releasing, emotion regulation or neural networks. All hypotheses would seem plausible and not necessarily mutually exclusive, but further research is needed to clarify the different contribution of the variables at issue [56, 57].
Lastly, all the studies agreed with the positive effects of music intervention, and highlight its easy-to-use aspect, inexpensiveness and the lack of evidence regarding harmful side effects which represent, together with the other efficacy proofs, a valid motivation to continue research in this direction.
References
-
Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Häuser W, et al. (2011) Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. The Journal of rheumatology 38(6): 1113-1122.
-
Cagnie B, Coppieters I, Denecker S, Six J, Danneels L, et al. (2014) Central sensitization in fibromyalgia? A systematic review on structural and functional brain MRI. In: Seminars in arthritis and rheumatism WB Saunders 44(1): 68-75.
-
Mannerkorpi K, Svantesson U, Broberg C (2006) Relationships between performance-based tests and patients' ratings of activity limitations, self-efficacy, and pain in fibromyalgia. Archives of physical medicine rehabilitation 87(2): 259-264.
-
Conversano C, Laura M, Rebecca C, Mirabelli V, Angelo G (2018) Catastrophizing and Fibromyalgia: A Mini- Review. J Transl Neurosci 3(3): 7.
-
Ricci A, Bonini S, Continanza M, Turano MT, Puliti EM, et al. (2016) Worry and anger rumination in fibromyalgia syndrome. Reumatismo 68(4): 195-198.
-
Galvez-Sánchez CM, Reyes del Paso GA, Duschek S (2018) Cognitive impairments in fibromyalgia syndrome: associations with positive and negative affect, alexithymia, pain catastrophizing and self- esteem. Frontiers in psychology 9: 377.
-
Berger A, Dukes E, Martin S, Edelsberg J, Oster G (2007) Characteristics and healthcare costs of patients with fibromyalgia syndrome. Int J Clin Pract 61(9): 1498-1508.
-
Ramiro FDS, Lombardi Júnior I, Silva RCBD, Montesano FT, Oliveira NRCD, et al. (2014) Investigation of stress, anxiety and depression in women with fibromyalgia: a comparative study. Revista brasileira de reumatologia 54(1): 27- 32.
-
Macfarlane GJ, Kronisch C, Dean LE, Atzeni F, Häuser W, et al. (2017) EULAR revised recommendations for the management of fibromyalgia Ann. Rheum. Dis 76(2): 318-328. [INLINE_TABLE:6:0]
-
Baptista A, Jones A, Cardoso F (2013) Assessment of art therapy program for women with fibromyalgia: Randomized, controlled, blinded study. Annals of the Rheumatic Diseases 71(S3): 271.
-
American Music Therapy Association (AMTA) (2017) 2017 AMTA member survey and workforce analysis: A descriptive, statistical profile of the AMTA membership and the music therapy community.
-
Benenzon RO (1983) Manuale di musicoterapia. Borla Editore.
-
Nordoff P, Robbins C (1977) Creative music therapy. New York: Samuel Day Publishing.
-
Priestley M (1994) Essays on analytical music therapy. Barcelona Publishers.
-
Goldberg FS (2013) The Bonny method of guided imagery and music. In: Art & Science of Music Therapy. Routledge, pp: 134-150.
-
Kemper KJ, Danhauer SC (2005) Music as therapy. South Med J 98(3): 282-288.
-
Koelsch S, Boehlig A, Hohenadel M, Nitsche I, Bauer K, et al. (2016) The impact of acute stress on hormones and cytokines, and how their recovery is affected by music-evoked positive mood. Scientific Reports 6: 20038.
-
Linnemann A, Kappert MB, Fischer S, Doerr JM, Strahler J (2015) The effects of music listening on pain and stress in the daily life of patients with fibromyalgia syndrome. Frontiers in human neuroscience 9: 434.
-
Gebhardt S, Dammann I, Loescher K, Wehmeier P, Vedder H, et al. (2018) The effects of music therapy on the interaction of the self and emotions - An interim analysis. Complementary Therapies in Medicine 41: 61-66.
-
Bo H, Ma L, Li H (2017) Music-evoked emotion classification using EEG correlation-based information. 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), 3348-3351.
-
Sutoo D, Akiyama K (2004) Music improves dopaminergic neurotransmission: demonstration based on the effect of music on blood pressure regulation. Brain Res 1016(2): 255-262. _23._ Trahan T, Durrant SJ, Müllensiefen D, Williamson VJ (2018) The music that helps people sleep and the reasons they believe it works: A mixed methods analysis of online survey reports. PLoS ONE 13 (11): e0206531.
-
Finnerty R (2018) Music Therapy as an Intervention for Pain Perception.
-
Korhan EA, Uyar M, Eyigör C Gülendam HY, Çelik S (2013) The effects of music therapy on pain in patients with neuropathic pain. American Society for Pain Management Nursing 15(1): 306-314.
-
Garza-Villarreal EA, Pando V, Parsons C, Vuust P (2017) Music-induced analgesia in chronic pain conditions: a systematic review and meta- analysis. Pain Physician 20(7): 597-610.
-
Alparslan GB, Babadağ B, Özkaraman A, Yıldız P, Musmul A, et al. (2016) Effects of music on pain in patients with fibromyalgia. Clinical rheumatology 35(5): 1317-1321.
-
Janzen TB, Paneduro D, Picard L, Gordon A, Bartel LR (2019) A parallel randomized controlled trial examining the effects of rhythmic sensory stimulation on fibromyalgia symptoms. Plos one 14(3): e0212021.
-
Espí-López GV, Inglés M, Ruescas-Nicolau MA, Moreno-Segura N (2016) Effect of low-impact aerobic exercise combined with music therapy on patients with fibromyalgia. A pilot study. Complementary therapies in medicine 28: 1-7.
-
Garza-Villarreal EA, Wilson AD, Vase L, Brattico E, Barrios FA, et al. (2014) Music reduces pain and increases functional mobility in fibromyalgia. Frontiers in psychology 5: 90.
-
Garza-Villarreal EA, Jiang Z, Vuust P, Alcauter S, Vase L, et al. (2015) Music reduces pain and increases resting state fMRI BOLD signal amplitude in the left angular gyrus in fibromyalgia patients. Frontiers in psychology 6: 1051.
-
Guétin S, Giniès P, Siou DKA, Picot MC, Pommié C, et al. (2012) The effects of music intervention in the management of chronic pain: a single-blind, randomized, controlled trial. The Clinical journal of pain 28(4): 329-337.
-
Mercadíe L, Mick G, Guétin S, Bigand E (2015) Effects of Listening to music versus environmental sounds in passive and active situations on levels of pain and fatigue in Fibromyalgia. Pain Management Nursing 16(5): 664-671. [INLINE_TABLE:7:0]
-
Picard LM, Bartel LR, Gordon AS, Cepo D, Wu Q, et al. (2014) Music as a sleep aid in fibromyalgia. Pain Research and Management 19(2): 97-101.
-
Torres E, Pedersen IN, Pérez-Fernández JI (2018) Randomized Trial of a Group Music and Imagery Method (GrpMI) for Women with Fibromyalgia. Journal of music therapy 55(2): 186- 220.
-
Weber A, Werneck L, Paiva E, Gans P (2015) Effects of music in combination with vibration in acupuncture points on the treatment of fibromyalgia. The Journal of Alternative and Complementary Medicine 21(2): 77-82.
-
Bennett R (2005) The Fibromyalgia Impact Questionnaire (FIQ): A review of its development, current version, operating characteristics and uses. Clin Exp Rheumatol 23(5): S154-162.
-
Buela-Casal G, Agudelo D, Spielberger CD (2008) Adaptación española del inventario de depresión estado rasgo (IDER). Madrid: TEA. Spanish adaptation: State/Trait Depression Questionnaire (ST/DEP).
-
Burkhardt CS, Clark SR, Bennet RM (1991) The fibromyalgia impact questionnaire: development and validation. J Rheumatol 18(5): 728-733.
-
Cleeland CS, Ryan KM (1994) Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore 23(2): 129-138.
-
Cork R, Isaac I, Elsharydah A, Saleemi S, Zavisca F, et al. (2004) A comparison of the verbal rating scale and the visual analog scale for pain assessment. Internet J Anesthesiol 8(1): 3.
-
Endicott J, Nee J, Harrison W, Blumenthal R (1993) Quality of Life Enjoyment and Satisfaction Questionnaire: a new measure. Psychopharmacol. Bull 29(2): 321-326.
-
Gould D (2001) Visual Analogue Scale (VAS). Journal of Clinical Nursing 10: 697-706.
-
Guy W (1976) ECDEU Assessment Manual for Psychopharmacology: Revised. ECDEU Assessment Manual. Washington, DC: US Government Printing Office.
-
Kim EJ, Buschmann MT (2006) Reliability and validity of the Faces Pain Scale with older adults. Int J Nurs Stud 43(4): 447-456.
-
Kroenke K, Spitzer RL (2002) The PHQ-9: A New Depression Diagnostic and Severity Measure. Psychiatr. Ann. SLACK Incorporated 32(9): 509-515.
-
Melzack R (1975) The McGill Pain Questionnaire: major properties and scoring methods. Pain 1(3): 277-299.
-
Ortega MR, Hernández ALS, Kegel JGM (2003) Actualización de la escala de depression del dentro de estudios epidemiológicos (CES-D). Estudio piloto en una muestra geriatric mexicana. Salud Ment 26(1): 59-68.
-
Pincus T, Summey JA, Salvatore AS, Wallston KA, Hummon NP (1983) Assessment of patient satisfaction in activities of daily living using a modified Stanford Assessment Questionnaire. Arthritis Rheum 26(11): 1346-1353.
-
Robinson K, Gatehouse S, Browning GG (1996) Measuring patient benefit from otorhinolaryngological surgery and therapy. Ann. Otol. Rhinol. Laryngol. SAGE Publications Sage CA: Los Angeles, CA 105: 415-422.
-
Sanchez-Canovas J (2007) EBP Escala de bienestar psicológico. Manual 2nd (Edn.), Madrid, Spain: TEA.
-
Smarr KL, Keefer AL (2011) Measures of depression and depressive symptoms: beck depression inventory-II(BDI II), center for epidemiologic studies depression scale(CES-D), geriatric depression scale (GDS), hospital anxiety and depression scale (HADS), and patient health questionnaire-9 (PHQ-9). Arthritis Care Res 63: S454-S466.
-
Spielberger CD, Gorsuch RL, Lushene RE (1970) STAI manual for the state trait anxiety inventory. Palo Alto, CA: Consulting Psychologists Press.
-
Suija K, Rajala U, Jokelainen J, Liukkonen T, Härkönen P, et al. (2012) Validation of the Whooley questions and the Beck Depression Inventory in older adults. Scand J Prim Health Care 30(4): 259-264.
-
Sullivan MJL, Bishop SR, Pivik J (1995) The pain catastrophizing scale: development and validation. Psychol Assess 7(4): 524-532.
-
Zigmond AS, Snaith RP (1983) The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica 67(6): 361-370.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis