Post-Traumatic Stress Disorder; What is Behind the Invisible Wounds??!!!
Post-traumatic stress disorder (PTSD) is the mental disorder that is encountered in sufferers who experienced or witnessed any kind of distressing events involving life threatening situations or extreme physical harm. Unfortunately, such a disorder significantly hurts the spirit, soul, mind, emotions, memories, and physiological body functions. It is a complicated condition that can be under-reported, missed, or undiagnosed, accordingly, raising public awareness about its etiology, manifestations, and prompt ways to deal with is crucial for its early diagnosis and proper intervention that will improve the quality of life of its sufferers dramatically. As not all wounds are visible and those invisible wounds are very difficult to treat and unlikely to disappear, it is important to collaborate efforts to understand and respect the suffering of PTSD victims and support them to bypass such a drastic disorder.
Introduction
Post-traumatic stress disorder (PTSD) is the mental disorder that is encountered in sufferers who experienced or witnessed any kind of distressing events involving life threatening situations (the threat of impending death) or extreme physical harm. It presents with vivid intrusive memories of the distressing event they experienced with hypervigilance and hyper-reactivity to propable threats associated with night mares, anxiety, mood swings, emotional numbness or dysphoria, anger, and aggression [1].
Affected individuals usually complain of intense anxiety and extreme fear even in the absence of danger as it could strike at any time and find it difficult to function normally in daily life tasks; socially, academically, and occupationally. It appears as if their normal stress response is imprisoned in a permanent override. Unfortunately, such a disorder significantly hurts the spirit, soul, mind, emotions, memories, and physiological body functions [2].
Historical Overview
PTSD has been long recognized as Hippocrates documented the battle trauma and combat flashbacks in a way that is nearly identical to the up to date diagnostic criteria of PTSD. Later, during the first world war, it was known as “shell shock”. It was then officially defined as a protective mental health condition from future experience of danger. On the other hand, Rape Trauma Disorder was then defined as a PTSD variant [1].
In 1980 version of the Diagnostic and Statistical Manual of Mental Disorders; DSM III [3], the PTSD term was introduced. Post Traumatic Stress Disorder Awareness Day was declared on the 27th of June, 2010 by USA Senate’s formal acknowledgment, then the whole month of June has been designated to be the awareness month of such a distressing disorder in 2014 after the suicide of an US National Guard Member who spent only 2 hours of duty in Iraq [2].
Epidemiology of Post-Traumatic Stress Disorder
PTSD is a complicated condition that can be under- reported, missed, or undiagnosed. About 5.2 million adults are expected to suffer from it yearly. As any other multifactorial disorder, its prevalence usually ranges between 2% and 9% and expected to increase in national or natural disasters as wars, floods, and earthquakes. Females are more likely to develop it with a female to male ratio of 2:1. No age is immune, children can experience it as well as adults [1, 2, 4].
PTSD is considered acute when symptoms starts as early as weeks up to 3 months, chronic if symptoms continue for 3 months or longer, and delayed if symptoms develop 6 months or more after exposure to the distressing event [1].
Etiology of PTSD
PTSD is a multifactorial disorder that develops due to interaction between the genetic make-up of an individual and his surrounding environmental factors; such interaction is under control of epigenetic mechanisms [4, 5, 6].
Many environmental triggers have been identified to precipitate PTSD as sexual assault, physical violence, military combat, natural disasters, violent accidents, harrassement and bullying, and loss of beloved ones. It could occur after a single extremely distressing incident or a series of incidents over a period of time. Risk of developing PTSD is magnified with multiplicity of triggers, prolonged or recurrent exposure to danger, premorbid physical or mental impairment, poor social support, and low economic status [1, 2, 4, 7].
Pathophysiology of PTSD
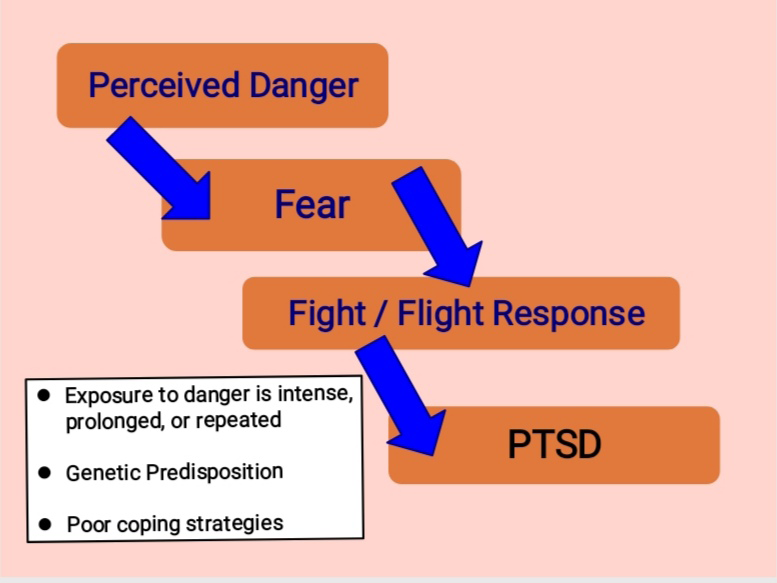
When perceive danger, humans feel fear that will trigger split second physical and mental body reactions to avoid or defend danger (flight or fight response) [8]. In cases of intense fear due to exposure to extreme, prolonged, and or repeated dangerous events, PTSD will develop in genetically predisposed individuals with poor coping strategies and defensive mechanisms (Figure 1).
Many brain regions are involved in the pathophysiology of PTSD that include parietal lobes, amygdala, hippocampus, and corpus callosum. Parietal lobes integrate information between different areas, amygdala evaluates the incoming emotional information for significance and gets activated on exposure to trauma triggers while hippocampus creates a cognitive map to categorize that experience. On the other hand, corpus callosum integrates emotional and cognitive input of exposure to such distressing events [8].
Those with reduced hippocampal volume and serum cortisol level as well as FKBP5, SERT, DAT, and GR gene polymorphism were found to be genetically predisposed to PTSD. Also, they showed changes in the global methylation patterns. Accordingly, some potential biomarkers are considered in diagnosis and prognosis of PTSD as circulating cortisol levels, glucocorticoid receptor expression, and GABA plasma levels [5, 6].
PTSD has many neurological, immunological, and hormonal effects. It is associated with memory alterations with decreased neurogenesis in the hippocampus and prefrontal cortenx with increased neurogenesis in the amygdala. On the other hand, enhanced inflammation has been recorded with reduced T cells, increased NK cells, IL- 6, TNF-alpha, and CRP in chronic cases of PTSD. Meanwhile, dysregulated hypothalamic pituitary adrenal axis with reduced cortisol levels and altered glucocorticoid receptor sensitivity have been reported [5, 6, 8].
Conclusion
It is not easy for our minds to forget what our eyes have seen or our soles experienced. Not all wounds are visible and those invisible wounds are very difficult to treat and unlikely to disappear. If we experience pain; this is life but feeling the suffering of others is humanity. It is our role to raise the public awareness about such distressing disorder to help sufferers to be understood, respected, and supported. If someone is unable to do so, at least he should avoid hurting others or add to their suffering.
References
-
Post-traumatic stress disorder. https:// www.nimh.nih. gov/health/topics/post-traumatic-stress-disorder-ptsd. Last reviewed May, 2022.
-
National Post-traumatic stress disorder awareness day. https:// nationaltoday.com/national-ptsd-awareness- day; last update on January, 2023.
-
Psychiatrists practice. https://psychiatry.org/ psychiatrists/practice/dsm/about-dsm/history-of-the- dsm. Last reviewed January, 2023.
-
Zaky EA (2015) Nature, nurture, and human behavior; an endless debate. J Child Adolesc Behav 3(6): 107.
-
Hunter RG (2012) Epigenetic effects of stress and corticosteroids in the brain. Front Cell Neurosci 6: 18.
-
Zaky EA (2017) Percussions of epigenetics on mood disorders; is it really a Charm or just a propaganda??!!!. Clin Depression 3(3): 126.
-
Zaky EA (2017) Violence and our children. J Psychiatry 20(5): 44.
-
Stahl SM (2013) Stahl’s essential psychopharmacology: neuroscientific basis and practical applications. J Can Acad Child Adolesc Psychiatry 19(3): 230.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis