Hidden Violence in Romantic Relationships and Mental Health during Covid- 19 Era: An Exploration of Greek Counsellors’ Experiences in Private Practice
The purpose of this study was the in-depth exploration of therapists’ narratives who work with hidden abused receivers before and after pandemic years. More specifically, the objectives focused on highlighting thoughts and feelings regarding the phenomenon, therapeutic challenges, assessment, and overall treatment including Covid- 19 years when remote sessions were multiplied due to social distancing measures. Participants were 5 therapists from different psychotherapeutic approaches in Greece,working privately with clients who experience hidden abuse in their intimate relationships. The interviews were recorded and analysed using Interpretive Phenomenological Analysis (IPA). Retrieved from analysis, four themes appeared: Understanding Hidden Violence, Clients’ Therapeutic Journey, Competent Therapeutic Process and Working in Pandemic.
Literature Review
The current study will be focused on the phenomenon of hidden Intimate Partner Violence (IPV) a term specifically used to underline behaviours intending to harm emotional well-being [1]. Prior research entitled these behaviours as ‘concealed’, ‘unseen’ or ‘hidden’ because of their less visible by- products if compared with physical or sexual abuse [2]. Psychological Abuse forms are viewed as less harmful, more socially acceptable and received fewer clinical and empirical attention through the years [3, 4]. However, unseen violence is highly prevalent in mental health disorders [5, 6, 7].
A considerable body of research outlined numerous connections between IPV and mental health problems of its receivers [8, 9, 10, 11] emerging a general debate around if the definitionsof hidden violence should focus on the behaviour itself or its consequences for the victims [12]. Psychological abuse (PA) includes any emotional, mental, or verbal battering behaviour towards a person [13, 14]. All previous studies agreed that PA is more difficult to be identified because of its concealed nature to imply patterns of maladaptive interacting such as degradation, exploitation, and threats. On the other hand, controlling behaviours ,as the fourth form of IPV, include social isolation, stalking, exaggerated monitoring and restricting access to finances or employment. Economic Abuse (EA), especially, occurs when the abuser prevents the receiver to be economically independent [15, 16].
Whereas physical and sexual abuse can be recognised and reported from even a single isolated incident -because of its observed by-products-,PA, controlling behaviours and EA are constituted by multiple schemas of interacting and sometimes are camouflaged as forms of love and humour and not as degrading and offensive [17, 18, 19]. Because of its camouflaging nature, PA is interpreted as ‘unseen’ or ‘hidden’ by many researchers [20, 21].
To intervene on unseen abuse, one must be aware of its sub- categories [21]. Firstly, mental abuse provokes senses of worthlessness to receivers as it affects the mind. Emotional abuse targets victims’ ‘inner self’ via intimidating their feelings and personality characteristics. Emotional maltreatment includes rejection, withdrawal, and degrading others’ self- identity [22, 23]. Verbal abuse on the other hand, occurs when others’ language is used to deliver threats and insults achieving absence of self- esteem to the victims [24]. Those forms of abuse cause psychological and not physical and it is usually a predictor of more severe violent forms [25].
Even though disguised, studies prove that hidden violence isfrequentand itsconcealed effects are correlated with emotional and relational functioning [26]. In contrast to physical and sexual violence that can be more easily researched and recognized via standardized questionnaires, the existing literature proves professionals’ difficulties in recognizing unseen abuse due to their unawarenessof its warning signs and symptoms [27].
The literature review suggests that unseen violence in childhood can predict later adulthood eating disorders [28] whilst other authors recognized its high prevalence in depression and depressive symptomatology [29]. Moreover, PA and Economic Abuse are common in suicide ideation [30], psychosomatic symptomatology [31, 32] and post- natal depression [33].
However, even if the evidence on negative health and mental health impact is growing, the phenomenon remains ‘hidden’ in terms of conceptual clarity and difficulties in achieving representative sampling in research [22]. Limited researched or not, the disastrous effects of PA to mental health functioning highlight the necessity of examining its nature as people seem to seek psychotherapy for all the mental health burdens addressed, ignoring their abused condition [34]. For this reason, it is important to broaden the knowledge regarding the phenomenon in order to multiply therapy success and comprehensive prevention measures.
Theoretical Approaches
Approaching a theoretical explanation of the phenomenon, its concealed nature can be framed regarding low victimization acceptance. For instance, Poza, et al. [35] pinpointed that social shame, and its forthcoming emotional devastation preserves the situation due to ‘male- chauvinist culture’ and strict gender roles [35]. As a result, people, and especially women, tend to forgive or forget lower violence levels confusing them with acts of love and interest [36]. Furthermore, if the victimization exists and abused women attempt to leave their couples, literature argues that they are more at risk of lethal violence than others who do not [37].
Many studies explained the phenomenon in relation to the lack of emotional regulation and conflict- resolution skills, suggesting abusers’ greater need of regaining control in the relationship- a situation that can result in escalation of IPV [38]. Moreover, inhibition in disclosing abuse is represented as an ‘obligation’ of a good partner who enacts with enormous justifications over their experiences, as a set of ideology for a ‘functioning relationship’ [39]. Hidden IPV recognition underlines receivers activate decision on breaking up their relationship at early stages of psychological abuse. This determination is suggested as the most preventable measure against the escalation of the violence extent [23, 35].
On the other hand, the state of women’s inhibition of self-expression for the maintenance of the relationship is also represented in Jack’s theory of ‘Silencing the Self’ as an attempt to conceptualize women’s major depression in our society [40]. Jack’s model highlights how women conceive their role in intimate relationships and explain that self- silencing is a coping strategy to avoid confrontation [41]. As a result, the person, unconsciously or not, decides to silence their feelings and thoughts while serving themselves to their significant other’s needs. The experience of the ‘loss of self’ is emerged because of anger suppression and co-dependency [42, 44]. Considering co-dependency as a mediator of the existence and enduring unseen abuse, the literature defines the phenomenon as a ‘dysfunctional pattern of relating’ characterized by a lack of free self-expression and a desire to achieve sense of purpose only through relationships [45].
Although thoroughly represented, some studies pinpointed researchers’ reluctance to perceive women as abusers too [46, 47]. They argue that hidden violence has not only male- perpetrators [48]. Brush [48] posits attention on awareness over women’s aggression as an attempt to increase the quality of IPV interventions. Several authors have recognized interpersonal violence as a complex and dynamic dimension of human relating with multifaced forms and patterns [49, 50, 51]. For those authors, violence is not only gender- normed: it is rooted in social systems. For some authors, relationship itself is a bigger source of aggression than the gender [49]. In conclusion, social constructions on what is violent or not articulate the experience of unseen abuse receivers. Thus, research indicates that the interpretation of the reality is socially constructed and dependent on participants’ meaning making procedures [51]. According to this position, violence begins from the moment receiver can identify it and name it. This approach offers a different explanation regarding the concealed nature of non- physical violent forms.
Pandemic, Intimate Relationships and IPV
Vulnerability on IPV during the pandemic has been thoroughly described by the ecological model of WHO as an attempt to address all the elements associated with this complex phenomenon [73]. Indeed, forced cohabitation, isolation and fear of contagion- as forms of coercive control- were viewed as catalysts of violence [74]. Moreover, negative psychological effects of quarantines (high levels of stress, frustration, confusion and depression) combined with indirect Covid- 19 consequences (eg. Economic uncertainty) provoked extra burden to people, causing an increase in alcohol and psychotropic consumption [75, 76].
There exists an ambiguity regarding IPV’s representation on coronavirus outbreak [77]. Some authors suggested that perpetrators in lockdowns had fewer reasons to enact with physical aggression because psychological abuse in terms of control and power was more effective and in congruence with the government’s restricting measures [74]. Of course, augmentation of PA has devastating consequences on receivers’ self- identity and mental health [78, 79, 80]. Additionally, pre-existing mental health illnesses exacerbated in pandemic highlighting positive correlation between IPV and psychopathology . The reduction of more ‘seen’ abuse due to the nature of forced cohabitation does not imply a simultaneous reduction of ‘concealed’ forms of violence. Thus, the study will be concentrated on counsellors’ experiences while working with receivers of hidden abuse who searched for therapy due to extreme distress levels and not the unseen violence itself.
Post Covid- 19 Psychotherapy and Counselling
Psychotherapeutic process could not be unaffected by pandemic reality. Indeed, psychotherapists ordered to work remotely with old and new clients achieving competency and dealing with working challenges very quickly [81, 82]. Remote therapy includes video calls or/ and traditional telephones and smartphones. The expanded entrance of remote therapy [83] was convenient for many clients who were confident in using technology; yet, for several others proved difficult due to reasons of privacy or absence of internet access [84].
Challenges of remotely psychotherapeutic working were related to interpersonal signals and technical troubles. In a qualitative study, therapists expressed difficulties on limited ‘view’ of the clients, worries about confidentiality and isolated ways of practising the profession [81]. Several other therapists in the same study, expressed concerns regarding the lack of clients’ ‘embodied sense of self’, fatigue due to concentration required, difficulties in maintaining boundaries and issues in transmitting experiential interventions efficiently. Indeed, remote therapy can burden the dissociative tendency of a client and impede emotional engagement. Clients participating in tele- therapy sessions may underreport their symptomatology. As a result, physical remoteness may lead to aggravation of the avoidance patterns and thus, delay the process of change [85]. Emotional distancing and inability to handle non- verbal behaviour subtleties is a huge challenge for almost all therapists [86].
Therapists’ experiences over online working varied, as many of them, referred to opportunities in building professional confidence and working with non- geographically- near clients . The offering flexibility was underlined as a positive therapeutic factor that influenced therapeutic alliance in general [87, 88].
Crisis intervention was a priority for many counsellors in pandemic attempting to encourage exacerbated distress emerged from social isolation. Fears of contamination and uncertainty, grief, and career counselling due to coronavirus loses of loved- ones and unemployment were also targeted [89]. On the other hand, many quarantined couples experienced their dysfunctional patterns of relating and confronted with the reality of hidden violence in their home lives [90]. For instance, Sandler [91] underlined that during quarantines, abusers, in order to gain financial control over the victims, prevented them from going to work due to fear- of- contagion [91].
The study will be focused on therapist’s experiences in private settings with hidden abused receivers before, during and after social distancing era. The gained knowledge will enhance therapeutic competency whilst allow the individualized views of participants to be expressed regarding the phenomenon and their work with unseen abused receivers. Besides, enlightening the dark sight of unseen violence can be the most influential preventing measure against more fatal violent forms and mental health awareness [21].
Methods
This study will attempt to intensely scrutinize the lived experiences of the therapists by using Interpretive Phenomenological Analysis (IPA) [92, 93]. Using participants’ statements as a rich context, their lived experience will provide an in- depth conceptualisation of the phenomenon [94, 95]. The outcomes of this study will enrich or challenge existing theories of the phenomenon and not generate new knowledge [96, 97].
IPA was preferred for the study as it enhances a dynamic interaction amongst the participants (researchers and interviewees) [98]. All therapists were treated as co- researchers of the interpretation and meaning- making process. IPA’s creativity will enhance the discovery of therapists’ emotional and cognitive experiences related to hidden violence and will broaden the overall knowledge in the field with possible benefits to future therapeutic competency [99].
Sampling and Recruitment
Purposive and homogenous sampling was employed to guarantee that all participants’ relevant experiences was attuned in study’s objectives and aims [100]. Since the aims were related to deeper exploration over counsellors’ working experiences on the phenomenon of hidden violence, the sample was small (5 psychotherapists) with certain inclusion and exclusion criteria [101] (Table 1). Ethical approval was granted by University of Derby Ethics Committee [102].
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Private Working with a licenced Psychotherapeutic Approach | Experience gained from training programmes. |
| At least 5 years of professional experience with clients suffering from emotional and anxiety difficulties. | Absences of Psychotherapeutic Approach |
| Experience in remotely and online settings. |
Table 1: Inclusion and Exclusion Criteria.
Accordingly, experienced psychotherapists were voluntarily recruited via e-mails which included Information sheets of the study and Consent Forms. Most of the participants were women and their demographic characteristics are represented in Table 2. Of the 22 invited therapists, 5 participants agreed to be interviewed and thus, received a Debriefing Letter, right after their participation.
| Participants’ ID Number | Geographical area | Age | Gender | Psychotherapeutic Approach | Years of Experience in the Field |
|---|---|---|---|---|---|
| 1 | Thessaloniki | 32 | Female | Systemic & EMDR Therapist | 7 |
| 2 | Athens | 43 | Female | Integrative Therapist | 12 |
| 3 | Thessaloniki | 38 | Female | Gestalt Therapist | 6 |
| 4 | Thessaloniki | 44 | Male | Systemic/ Person Centred Therapist | 17 |
| 5 | Thessaloniki | 33 | Male | Integrative/ Systemic Therapist | 8 |
Table 2: Of the 22 invited therapists, 5 participants agreed to be interviewed and thus, received a Debriefing Letter, right afte
Data Collection
Semi-structured interviews with open questions were conducted in order to enhance participants’ narratives in a non- directive attitude [103]. Targeting to formulate the context and the flow of the conversation, a pilot interview was used as a follow- up [104]. All interviews’ duration was 40- 50 minutes approximately, an adequate time for an IPA study. Moreover, the interviews were conducted in Greek language and audiotaped. Afterwards, all data were transcripted and translated in English language. Audio recordings allow accuracy in data- process which, according to IPA’s framework, improves the quality of the forthcoming analysis [105].
Procedure
Data protection and confidentiality issues were prior communicated openly and therapists were able to sign a Consent Form for audiotape. All therapists acknowledged their rights in participation and after the interview they received a Debriefing Letter which targeted further protect and support of the interviewees. The interviews were handled on therapist’s private offices or via Skype- sessions.
Data Analysis
The present study’s data were collected, transcripted with verbatim system and then, analysed according to IPA principles. Theoretical orientation of IPA assumes that people interpret actively on their experiences as ‘self- interpreting’ beings [106, 107, 108]. Researchers’ active role in the analysis influenced the process of understanding therapists’ working experiences by moving back and forth to enhance interpretive activity [109]. IPA’s idiographic nature emphasized an in- depth exploration of the individuality before searching for generalizations [110].
Ethical Considerations
Primary data contained in this research, first and foremost ethical approved by the Research Ethics Committee of the University of Derby. Thus, all data are consistent with the Policy and Code of Practice in Research Ethics of the same university. Moreover, the researcher considered carefully the BPS Code of Human Research Ethics [111], the Ethical Guidelines for Researching Counselling and Psychotherapy of BACP [112] and the Data Protection Act, 1998.
Protection of Participants
A thorough Risk Assessment Form was completed before any attempt of contact with potential participants. Some questions or the interview’s context might cause psychological distress to some participants due to past traumatic memories in their personal or professional lives. Although the overall risk level was low, during every interview we were alert to remind participants’ right of withdrawal whenever needed. All interviewees had the right to be supported by a Counselling Centre.
Results
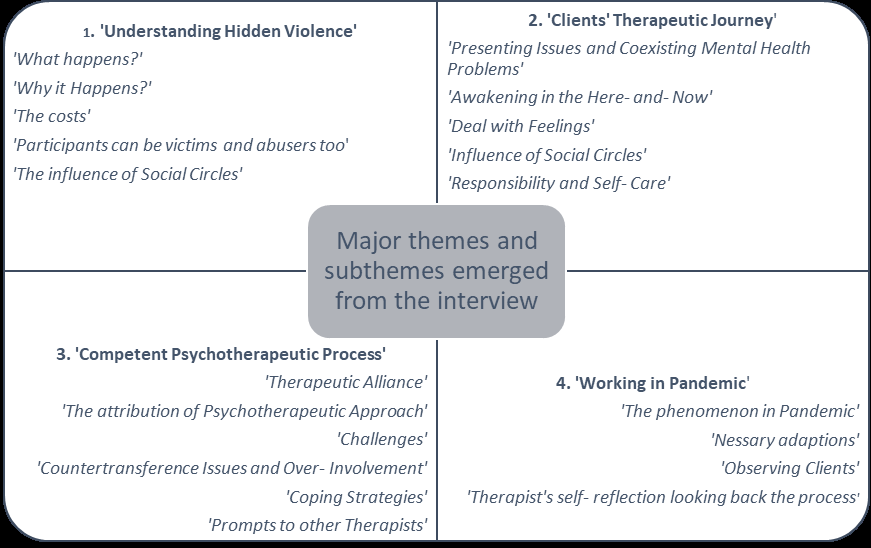
As shown in Figure 1, for major themes emerged from Interpretive Phenomenological Analysis of the primary data: i) ‘Understanding Hidden Violence, ii) ‘Client’s Therapeutic Journey’, iii) ‘Competent Psychotherapeutic Process’ and iv) ‘Working in Pandemic’.
Discussion
The study findings contributed to the literature gap on the phenomenon and more specifically on how therapists’ experiences with hidden abused clients view the therapeutic process and challenges with this population. Serious consideration was given to psychotherapeutic working with hidden abused clients during pandemic, when remote and online sessions were multiplied due to the social distancing era. Concerning all objectives of this study, 4 major themes (Figure 1) emerged.
Conclusions
Overall, the current study’s results proved substantial and consistent with the existing literature on hidden violent forms before, during and after the pandemic of Covid- 19 [124]. The analysis revealed further insight into therapists’ lived experiences with hidden abused receivers in terms of their psychotherapeutic working via in-vivo and remote sessions. Exploring therapists’ interpretations over therapeutic journey of hidden abuse clients, challenges and competency issues emerged, regarding the camouflaging nature of the phenomenon. The in- depth investigation of participants’ working experiences, can offer new therapeutic implications over psychological treatment [64]. Accepting its theoretical complexity whilst being mindful of professionals’ lived experience can contribute significantly to the field by shaping more immediate detection and prevention measures against concealed IPV [125]. Besides, as unseen IPV implies mental health difficulties and is viewed as a ‘predictor’ for more seen abused forms [126] the gained knowledge from the current study’s findings can be used for more spherical interventions.
Furthermore, the study’s results formulated a necessity for therapists to maintain a supervisory image of society rather than focusing only on individual psychopathologybecause some forms of abuse seem more socially acceptable than others [3, 127]. Findings underlined that psychotherapeutic sight will be insufficient if professionals ignore their triggering emotions and the impact of unseen abuse in their personal lives. Simultaneously, analysis has significant implications for the understanding of all secondary benefits of clients’ reluctance in distancing from their intimate abusers [128].
Limitations
Despite their huge significance, the limitations and weaknesses of the findings should be underlined [104]. Firstly, the current study followed a qualitative paradigm, which means that findings cannot be replicated as they encompass participants’ subjective interpretations which impede research validity and reliability [129]. In addition, the snowballing small sample size is not representative, and the results cannot be generalized [93]. Moreover, the analysis reflects upon retrospective experiences of therapists who worked psychotherapeutically with hidden abused receivers. They shared their views on the phenomenon and its population; views that may be biased by their attitudes. The researcher’s perspective during data analysis may be also reflected in the study as long astheir presence during data gathering may have affected participants’ responses [130, 131]. Although the aims of the research were focused on therapists working experiences, when answering general questions, some of them tended to express their general theoretical knowledge rather than their reflections on their lived experiences [132, 133, 134, 135, 136, 137, 138, 139, 140, 141, 142, 143, 144, 145, 146].
Recommendations for Practice and Further Research
It would be substantial if future research continues focusing on the topic of unseen violence via qualitative and quantitative methods in order to offer new insights and make the phenomenon more ‘seen’. Considerably, more work will need to be done to determine hidden violence experiences on people showing up in therapy rooms before and after the pandemic and future research can examine a wider range of therapists who work not only with heterosexual but also with homosexual couples; this can allow acquisition of a more spherical understanding towards therapists’ attitudes and competencies over unseen abuse. The quantitative methodology can guarantee more representative sampling formulating bigger clusters of different unseen abused forms [143].
For sure, the study findings fulfilled its objectives and aims and the in-depth analysis can be a helpful guide for new and older therapists to become more aware of hidden violence’s impact on everyday functioning. By acknowledging its high complexity, professionals can approach the psychological treatment of exact psychopathology with more sensitivity and integration. For example, combining methods in alleviating the symptomatology while simultaneously being ready to confront any defensive mechanism or secondary benefit of unseen abuse receiver can be significantly helpful. On the other hand, study findings highlighted the necessity of preserving therapists’ self-care against exaggerating emotional involvement, anticipation, and burnout. The current study has taken into serious consideration all therapeutic challenges and difficulties which will enrich the readers with some opportunities to explore coping strategies to overcome their professional stress [144, 145, 146, 147, 148, 149].
References
-
Yoon JE, Lawrence E (2013) Psychological victimization as a risk factor for the developmental curse of marriage. Journal of Family Psychology 27(1): 53-64.
-
Finzi dottan R, Gewirtz Meydan A (2020) Psychological abuse as a mediator between insecure attachment orientations and relationship satisfaction. Family Relations 70(2): 498-513.
-
Masci BS, Sandra F, Sanderson SDA (2017) Perceptions of psychological abuse versus physical abuse and their relationship with mental health outcomes. Violence and Victims 32(2); 362-376.
-
Arriaga XB, Schkeryantz EL (2015) Intimate relationships and personal distress: The invisible harm of psychological aggression. Personality andSocial Psychology Bulletin 41(10): 1332-1344.
-
Lawrence E, Yoon J, Langer A, Ro E (2009) Is psychological aggression as detrimental as physical aggression? the independent effects of psychological aggression on depression and anxiety symptoms. Violence and Victims 24(1); 20-35.
-
Straight ES, Harper FWK, Arias I (2003) The impact of partner psychological abuse on health behaviors and health status in college women. Journal of Interpersonal Violence 18(9): 1035-1054.
-
Follingstad DR, DeHart DD (2000) Defining psychological abuse of husbands toward wives: Contexts, behaviors, and typologies. Journal ofInterpersonal Violence 15(9): 891-920.
-
Campbell JC (2002) Health consequences of intimate partner violence. Lancet 359(9314): 1331-1336.
-
Iverson KM, Dardis CM, Pogoda TK (2017) Traumatic brain injury and PTSD symptoms as a consequence of intimate partner violence. Compr Psychiatry 74: 80-87.
-
Ellsberg M, Jansen HAFM, Heise L, Watts CH, Garcia Moreno C (2008) Intimate partner violence and women’s physical and mental health in the WHO multi-country study on women’s health and domestic violence: an observational study. Lancet 371(9619): 1165-1172.
-
Bacchus LJ, Ranganathan M, Watts C, Devries K (2018) Recent intimate partner violence against women and health: a systematic review and meta-analysis of cohort studies. BMJ Open 8(7): e019995.
-
Glaser D (2002) Emotional abuse and neglect (psychological maltreatment): A conceptual framework. Child Abuse & Neglect 26(6-7): 697-714.
-
Francis L, Pearson D (2021) The recognition of emotional abuse: adolescents’ responses to warning signs in romantic relationships. Journal of Interpersonal Violence 36(17-18): 8289-8313.
-
Murphy CM, Eckhardt CI (2005) Treating the abusive partner. In: Oguntayo R (Eds.), Spousal Violence in the Era of Covid-19 Lockdown : the Implication, pp: 51-60.
-
Pichon M, Treves-Kagan S, Stern E, Kyegombe N, Stöckl H, et al. (2020) A mixed-methods systematic review: Infidelity, romantic jealousy and intimate partner violence against women. International Journal of Environmental Research and Public Health 17(16): 1-35.
-
Giannouli V (2018) Elder abuse and consent capacity: Our collective nemesis. Social, psychological, and forensic perspectives on sexual abuse pp: 207-221.
-
Keashly L (2001) Interpersonal and systemic aspects of emotional abuse at work: The target’s perspective. Violence and Victims 16(3): 233-268.
-
Smullens S (2010) The codification and treatment of emotional abuse in structured group therapy. International Journal of Group Psychotherapy 60(1): 111-130.
-
Black MC, Basile KC, Breidling MJ, Smith SG, Walters ML, et al. (2011). National intimate partners and sexual violence survey: 2010 summary report. Retrieved from.
-
Romito P, Eastwood J (2008) A deafening silence: Hidden violence against women and children, A Deafening Silence: Hidden Violence against Women and Children. Great Britain: Policy Press.
-
Robinson JC (2018) The unseen forms of violence against women: Why psychological abuse must be treated as criminal offense. Appalachian Journal of Law 18(1): 75- 100.
-
Gibbs A, Dunkle K, Jewkes R (2018) Emotional and economic intimate partner violence as key drivers of depression and suicidal ideation: A cross-sectional study among young women in informal settlements in South Africa. PLoS ONE 13(4): e0194885.
-
Kelly JB, Johnson MP (2008) Differentiation Among Types of Intimate Partner Violence: Research Update and Implications for Interventions Family Court Review 46(3): 476-499.
-
Jewkes R (2010) Emotional abuse: a neglected dimension of partner violence. Lancet 376(9744): 851-852.
-
Schumacher JA, Leonard KE (2005) ‘Husbands’ and wives’ marital adjustment, verbal aggression, and physical aggression as longitudinal predictors of physical aggression in early marriage. Journal of Consulting and Clinical Psycholog 73(1): 28-37.
-
Karakurt G, Silver BA (2013) Emotional abuse in intimate relationships: The role of gender and age. Violence and Victims 28(5): 804-821.
-
Fraser J, Matthews B, Walsh KM, Chen L, Dunne MP (2010) Factors influencing child abuse and neglect recognition and reporting by nurses: A multivariate analysis. International Journal of Nursing Studies 47(2): 146-153.
-
Kent A, Waller G, Dagnan D (1999) A greater role of emotional than physical or sexual abuse in predicting unhealthy adult eating attitudes: The role of mediating variables. The International Journal of Eating Disorders 25(2): 159-167.
-
Estefn LF, Coulter ML, Vandeweerd C (2016) Depression in women who have left violent relationships: The unique impact of frequent emotional abuse. Violence against Women 22(11): 1397-1413.
-
StoÈckl H, Penhale B (2015) Intimate partner violence and its association with physical and mental health symptoms among older women in Germany. Journal of Interpersonal Violence 30(17): 3089 -111.
-
Ludermir AB, Lewis G, Valongueiro SA, de Araubjo TVB, Araya R (2010) Violence against women by their intimate partner during pregnancy and postnatal depression: a prospective cohort study. The Lancet 376(9744): 903- 910.
-
Alio AP, Daley EM, Nana PN, Duan J, Salihu HM (2009) Intimate partner violence and contraception use among women in Sub-Saharan Africa. International Journal of Gynecology& Obstetrics 107(1): 35-38.
-
Fulu E, Jewkes R, Roselli T, Garcia-Moreno C (2013) ‘Prevalence of and factors associated with male perpetration of intimate partner violence: findings from the UN Multi-country Cross-sectional Study on Men and Violence in Asia and the Pacific.’ The lancet global health 1(4): 187-207.
-
Leal J, Cunha C, Santos A, Salgado J (2020) Helping Clients Victimized by Intimate Partners Through Stages of Change: An Emotion Focused Approach. Journal of Contemporary Psychotherapy 51: 48-48.
-
Poza EDL, Jódar L, Barreda S (2016) Mathematical Modeling of Hidden Intimate Partner Violence in Spain: A Quantitative and Qualitative Approach. Abstract and Applied Analysis.
-
Galarza MLE, Tavora A (2008) Romantic love and the social subordination of women: reviews and proposals. Yearbook of Psychology 39(1): 59-73.
-
Stith S, McCollum E, Rosen K (2011) Couples Therapy for Domestic Violence: Finding Safe Solutions. American Psychological Association: Washington, DC, USA.
-
Guay S, Sader J, Boisvert JM, Beaudry M (2016) Typology of perceived causes of intimate partner violence perpetration in young adults. Violence Gend 3(4): 189- 195.
-
Ahmad F, Driver N, McNally MJ, Stewart DE (2009) Why doesn’t she seek help for partner abuse?” An exploratory study with South Asian immigrant women. Social Science and Medicine 69(4): 613-622.
-
Jack DC (1991) Silencing the Self: Women and Depression. Cambridge MA: Harvard University Press.
-
Emran A, Iqbal N, Dar IA (2020) Silencing the self’ and women’ s mental health problems : A narrative review. Asian Journal of Psychiatry 53: 102197.
-
Ussher J(2003) The ongoing silencing of women in families: an analysis and rethinking of premenstrual syndrome and therapy. J Fam Therapy 25(4): 388-405.
-
Maji S, Dixit S (2018) Self-silencing and women’s health: a review. Int. J. Soc. Psychiatry 65(1): 3-13.
-
Da Silva N, Verdejo T, Dillon F, Ertl M, De La Rosa M (2018) Marianismo Beliefs, Intimate Partner Violence, and Psychological Distress Among Recently Immigrated, Young Adult Latinas. J. Interpers. Violence 36(7).
-
Happ Z, Bodó-Varga Z, Bandi SA, Kiss, EC, Nagy L, et al. (2022) How codependency affects dyadic coping, relationship perception and life satisfaction. CurrPsychol 42: 15688-15695.
-
Archer J (2002) Sex differences in aggression between heterosexual partners:Ameta-analytic review. Psychological Bulletin 126(5): 651-680.
-
Frieze IH (2005) Female violence against intimate partners: An introduction. Psychology of Women Quarterly 29(3): 229-237.
-
Brush LD (2005) Philosophical and political issues in research on women’s violence and aggession. Sex Roles 52: 867-873.
-
Richardson DS (2005) The myth of female passivity: Thirty years of revelations about female aggression. Psychology of Women Quarterly 29(3): 238-247.
-
Frieze IH (2005) Hurting the one you love: Violence in relationships. Belmont, CA: Thomson Wadsworth.
-
Mchugh MC, Livingston NA, Ford A (2005) A postmodern approach to women’s use of violence: Developing multiple and complex conceptualizations. Psychology of Women Quarterly 29(3): 323-336.
-
Reisenhofer S, Taft A (2013) Women’s journey to safety - The Transtheoretical model in clinical practice when working with women experiencing Intimate Partner Violence: A scientific review and clinical guidance. Patient Education and Counseling 93(3): 536-548.
-
Grigsby N, Hartman BR (1997) The barriers model : An integrated strategy for intervention with battered women. Psychotherapy: Theory Research Practice Training 34(4): 485-497.
-
Bogat GA, Garcia AM, Levendosky AA (2013) Assessment and psychotherapy with women experiencing intimate partner violence: Integrating research and practice. Psychodynamic Psychiatry 41(2): 189-217.
-
Johnson DM, Johnson NL, Perez SK, Palmieri PA, Zlotnick C (2016) Comparison of adding treatment of PTSD during and after shelter stay to standard care in residents of battered women’s shelters: Results of a randomized clinical trial. J Trauma Stress 29(4): 365-373.
-
Evans M, Malpass A, Agnew-Davies R, Feder G (2018) Women’s experiences of a randomised controlled trial of a specialist psychological advocacy intervention following domestic violence: A nested qualitative study. PLoS ONE 13(11): e0193077.
-
Warshaw C, Sullivan CM, Rivera EA (2013) A systematic review of trauma-focused interventions for domestic violence survivors. Chicago: National Center on Domestic Violence, Trauma and Mental Health pp: 1-27.
-
Paivio SC, Jarry JL, Chagigiorgis H, Hall I, Ralston M (2010) Efficacy of two versions of emotion-focused therapy for resolving child abuse trauma. Psychotherapy Research 20(3): 353-366.
-
Timulak L, Keogh D (2020) Emotion-focused therapy: A transdiagnostic formulation. Journal of Contemporary Psychotherapy 50: 1-13.
-
Bliss MJ, Ogley-Oliver E, Jackson E, Harp S, Kaslow NJ (2008) African American women’s readiness to change abusive relationships. Journal of Family Violence 23(3): 161-171.
-
Elliott R, Watson JC, Goldman RN, Greenberg LS (2004) Learning emotion-focused therapy: The process- experiential approach to change. Washington, DC: American.
-
Tiwari A, Leung WC, Leung TW, Humphreys J, Parker B, et al. (2005) A randomised controlled trial of empowerment training for Chinese abused pregnant women in Hong Kong. British Journal of Obstetrics and Gynaecology 112(9): 1249-1256.
-
Chang JC, Cluss PA, Ranieri LA, Hawker L, Buranosky R, et al. (2005) Health care interventions for intimate partner violence: what women want. Women’s Health Issues 15(1): 21-30.
-
Hameed M, O’Doherty L, Gilchrist G, Tirado-Muñoz J, Taft A, et al. (2020) Psychological therapies for women who experience intimate partner violence. Cochrane Database of Systematic Reviews 7(7): CD013017.
-
Branson DC (2019) Vicarious trauma, themes in research, and terminology: A review of literature. Traumatology 25(1): 2-10.
-
Salston MD, Figley CR (2003) Secondary traumatic stress effects of working with survivors of criminal victimization. Journal of Traumatic Stress 16(2): 167- 174.
-
Boscarino JA, Figley CR, Adams RE (2004) Compassion fatigue following the September 11 terrorist attacks: A study of secondary trauma among New York City social workers. International Journal of Emergency Mental Health 6(2): 57-66.
-
Ghahramanlou M, Brodbeck C (2000) Predictors of secondary trauma in sexual assault trauma counselors. International Journal of Emergency Mental Health 2(4): 229-240.
-
Jenkins SR, Mitchell JL, Baird S, Whitfield SB, Meyer HL (2011) The counselor’s trauma as counseling motivation: Vulnerability or stress inoculation?’, Journal of Interpersonal Violence 26(12): 2392-2412.
-
Sutton L, Rowe S, Hammerton G, Billings J (2022) The contribution of organisational factors to vicarious trauma in mental health professionals: a systematic review and narrative synthesis. European Journal of Psychotraumatology 13(1): 2022278.
-
Coleman AM, Chouliara Z, Currie K (2021) Working in the field of complex psychological trauma: A framework for personal and professional growth, training, and supervision. Journal of interpersonal violence 36(5-6): 2791-2815.
-
Ortlepp K, Friedman M (2002) Prevalence and correlates of secondary traumatic stress in workplace lay counselors. Journal of Traumatic Stress 15(3): 213-222.
-
Krug EG, Dahlberg LL, Mercy JA, Zwi AB (2002) The World report on violence and health. Lancet 360(9339): 1083-1088.
-
Barbara G, Facchin F, Micci L, Rendiniello M, Giulini P, et al. (2020) Covid-19, lockdown, and intimate partner violence: Some data from an italian service and suggestions for future approaches. Journal of Women’s Health 29(10): 1239-1242.
-
Singh NK, Srivastava M, Pandey A (2020) Handbook of Mental Health Issues During COVID19 Pandemic.
-
Duncan TK, Weaver JL, Zakrison TL, Joseph BA, Campbell BT, et al. (2020) Domestic Violence and Safe Storage of Firearms in the COVID-19 Era. Annals of Surgery 272(2): e55 - e57.
-
Gelder NV, Peterman A, Potts A, O’Donnell M, Thompson K, et al. (2020) COVID-19: Reducing the risk of infection might increase the risk of intimate partner violence. EClinicalMedicine 21: 100348.
-
Almeida M, Shreshta AD, Stojanac D, Miller LJ (2020) The impact of COVID-19 pandemic on women’s mental health. Arch Womens Ment Health 23(6): 741-748.
-
Sediri S, Zgueb Y, Ouanes S, Ouali U, Bourgou S, et al. (2020) Women’s mental health: acute impact of COVID-19 pandemic on domestic violence. Arch Womens Ment Health 23(6): 749-756.
-
Tandon R (2021) COVID-19 and suicide: Just the facts key learnings and guidance for action. Asian J Psychiatry 60: 102695.
-
McBeath AG, Plock SD, Bager-Charleson S (2020) The challenges and experiences of psychotherapists working remotely during the coronavirus pandemic. Counselling and Psychotherapy Research 20(3): 394-405.
-
Shklarski L, Abrams A, Bakst E (2021) Navigating changes in the physical and psychological spaces of psychotherapists during Covid-19: When home becomes the office. Practice Innovations 6(1): 55-66.
-
Hilty DM, Ferrer DC, Parish MB, Johnston B, Callahan EJ, et al. (2013) The effectiveness of telemental health: A 2013 review. Telemed J E Health 19(6): 444-454.
-
Markowitz JC, Milrod B, Heckman TG, Bergman M, Amsalem D, et al. (2021) Psychotherapy at a Distance. The American Journal of Psychiatry 178(3): 240-246.
-
Prochaska JO, Norcross JC (2009) Systems of Psychotherapy: A Transtheoretical Analysis In: 6th (Edn.), Pacific Grove, CA: Brooks/ Cole.
-
Dores AR, Geraldo A, Carvalho IP, Barbosa F (2020) The use of new digital information and communication technologies in psychological counseling during the COVID-19 pandemic. International Journal of Environmental Research and Public Health 17(20): 1-24.
-
Brown S (2020) How are counsellors coping with Covid-19. Therapy Today Psychology and BehavioralSciences Collection 31(4): 16-20.
-
Békés V, Van Doorn KA (2020) Psychotherapists’ attitudes toward online therapy during the COVID-19 Pandemic. Journal of Psychotherapy Integration 30(2): 238-247.
-
Forte C (2020) Counseling in a time of covid-19 American Counseling Association Member Blogs framework. Child Abuse & Neglect 26: 697-714.
-
Mulqueen M (2020) When home is not where the heart is. Psychotherapy.net.
-
Sandler R (2020) Domestic violence hotline reports surge in coronavirus-related calls as shelter-in-place leads to isolation, abuse. Forbes.
-
Eatough V, Smith JA (2008) Interpretative phenomenological analysis, The Sage Handbook of Qualitative Research in Psychology 179: 194.
-
Flowers P, Larkin M, Smith JA (2009) Interpretative phenomenological analysis: Theory, method and research. London: Sage 6(4): 346-347.
-
Mcleod J (2011) Qualitative Research: In Counselling and Psychotherapy. 2nd (Edn.), London: Sage.
-
Silverman D, Marvasti A (2008) Doing Qualitative Research: A Comprehensive Guide. London: Sage.
-
Smith JA (2003) Qualitative psychology: A practical guide to research methods. London: Sage.
-
Larkin M, Thompson A (2012) Interpretative phenomenological analysis. In: Thompson A, Harper D (Eds.), Qualitative research methods in mental health and psychotherapy: a guide for students and practitioners pp: 99-116.
-
Jan P, John D, Ella M, Charles H (2011) Interpretative phenomenological analysis: A discussion and critique. Nurse researcher 18(3): 20-24.
-
Lund T (2005) The qualitative-quantitative distinction: Some comments. Scandinavian Journal of Educational Research 49(2): 115-132.
-
Langdridge D (2007) Phenomenological psychology: Theory, research and method. UK.
-
Levitt H (2015) Qualitative psychotherapy research: The journey so far and future directions. Psychotherapy 52(1): 31-37.
-
Research Ethics Committee of the University of Der by (2019) University Research Ethics Policy.
-
Ponterotto JG (2005) Qualitative research training in counselling psychology: A survey of directors of training. Teaching of Psychology 32(1): 60-62.
-
Creswell JW (2007) Qualitative Inquiry and Research Design. Choosing Among Five Approaches, 2nd (Edn.), London: Sage.
-
Willig C (2013) Introducing Qualitative Research in Psychology. 3rd (Edn.), Berkshire: Open University Press.
-
Gough E, Giannouli V (2020) A qualitative study exploring the experience of psychotherapists working with birth trauma. Health Psychology Research 8(3): 9178.
-
Rizou E, Giannouli V (2020) An exploration of the experience of trainee integrative psychotherapists on therapeutic alliance in the light of their attachment style. Health Psychology Research 8(3): 9177.
-
Taylor C (1985) Human agency and language. Cambridge University Press, New York, USA.
-
Smith JA, Osborn M (2003) Interpretative phenomenological analysis. In: Smith JA (Ed.), Qualitative psychology: A practical guide to research methods pp: 51-80.
-
Pietkiewicz I, Smith JA (2014) A practical guide to using Interpretative Phenomenological Analysis in Qualitative Research Psychology. Psychological Journal 20(1): 7-14.
-
The British Psychological Society (2018) Code of Ethics and Conduct. The British Psychological Society pp: 1-12.
-
BACP (2018) Ethical Framework for the Counselling Professions.
-
Pokharel B, Hegadoren K, Papathanassoglou E (2020) Factors influencing silencing of women who experience intimate partner violence: An integrative review. Aggression and Violent Behavior 52: 101422.
-
Stark E (2007) Coercive control: The entrapment of women in personal life. Oxford University Press New York, USA.
-
Gammeltoft TM (2016) Silence as a response to everyday violence: Understanding domination and distress through the lens of fantasy. Ethos 4(4): 427-447.
-
Hydén M (1999) The World of the Fearful: Battered Women´s Narratives of Leaving Abusive Husbands, Feminism & Psychology 9(4): 449-469.
-
Hydén M (2005) I must have been an idiot to let it go on: Agency and positioning in battered women’s narratives of leaving. Feminism and Psychology 15(2): 169-188.
-
Ulloa EC, Hammett JF, Guzman ML, Hokoda A (2015) Psychological growth in relation to intimate partner violence: A review. Aggression and Violent Behavior 25(Part A): 88-94.
-
Greenberg LS (2011) Emotion-focused therapy. American Psychological Association.
-
McClellan MJ, Florell D, Palmer J, Kidder C (2020) Clinician telehealth attitudes in a rural community mental health center setting. Journal of Rural Mental Health 44(1): 62-73.
-
Barker GG, Barker EE (2022) Online therapy: lessons learned from the COVID-19 health crisis. British Journal of Guidance and Counselling 50(1): 66-81.
-
Sánchez OR, Vale DB, Rodrigues L, Surita FG (2020) Violence against women during the COVID-19 pandemic: An integrative review. International Journal of Gynecology and Obstetrics 151(2): 180-187.
-
Piquero A.R, Jennings WG, Jemison E, Kaukinen C, Knaul FM (2021) Domestic violence during the COVID-19 pandemic - Evidence from a systematic review and meta- analysis. Journal of Criminal Justice 74: 101806.
-
Pfitzner N, Gibbon KT, True J (2020) Responding to the “Shadow Pandemic”: Practitioner views on the nature of and responses to violence against women in Victoria, Australia during the COVID-19 restrictions.
-
Fogarty A, Savopoulos P, Seymour M, Cox A, Williams K, et al. (2021) providing therapeutic services to women and children who have experienced intimate partner violence during the COVID-19 pandemic : Challenges and learnings. Child Abuse & Neglect 130(1): 105365.
-
Kyegombe n, Stern E, Buller AM (2022) we saw that jealousy can also bring violence: A qualitative exploration of the intersections between jealousy, infidelity and intimate partner violence in Rwanda and Uganda. Social Science & Medicine 292: 114593.
-
Jordan CE, Campbell R, Follingstad D (2010) Violence and women’s mental health: The impact of physical, sexual, and psychological aggression. Annual Review of Clinical Psychology 6: 607-628.
-
Haselschwerdt ML, Hardesty JL (2017) Managing secrecy and disclosure of domestic violence in affluent communities. Journal of Marriage and Family 79(2): 556-570.
-
Eatough, J, Smith A (2017) Qualitative research in Psychology. London: Sage
-
Braun V, Clarke V (2006) Using thematic analysis in psychology. Qualitative Research in Psychology 3 (2): 77-101.
-
Edwards R, Holland J (2013) what is qualitative interviewing? Bloomsbury pp:128.
-
Ansara DL, Hindin MJ (2011) Psychosocial consequences of intimate partner violence for women and men in Canada. J InterpersViolence 26(8): 1628- 645
-
BACP Good Practice in Action Resources
-
Beydoun HA, Beydoun MA, Kaufman JS, Lo B, Zonderman AB (2012) Intimate partner violence against adult women and its association with major depressive disorder, depressive symptoms and postpartum depression: a systematic review and meta-analysis. Soc Sci Med 75(6): 959-975.
-
Bond T (2015) Standards and Ethics for Counselling in Action. 4th (Edn.), pp: 325.
-
Bryman A (2012) Social Research Methods. 4th(Edn.), Oxford: University Press pp: 1-809.
-
Frieze IH (2005) Female violence against intimate partners: An introduction. Psychology of Women Quarterly 29(3): 229-237.
-
Golding JM (1999) Intimate partner violence as a risk factor for mental disorders: a meta-analysis. J Fam Violence 14(2): 99-132.
-
Greenberg LS (2014) The therapeutic relationship in emotion focused therapy.Psychotherapy 51(3): 350- 357.
-
Hegarty kl, Doherty LJO, Gunnet J,Pierce D, Taft AJ (2008) A brief counselling intervention by health professionals utilising the “readiness to change” concept for women experiencing intimate partner abuse: The weave project. Journal of Family Studies 14(2,3): 376- 388.
-
Indu PV, Vijayan B, Tharayil HM, Ayirolimeethal A, Vidyadharan V (2021) Domestic violence and psychological problems in married women during COVID-19 pandemic and lockdown: A community-based survey. Asian Journal of Psychiatry 64: 102812.
-
Kvale S (2007) Doing Interviews. London Sage.
-
Liendo NM (2009) Cross-cultural factors in disclosure of intimate partner violence: an integrated review. Journal of Advanced Nursing 65(1): 20-34.
-
Plichta SB (2004) Intimate partner violence and physical health consequences: policy and practice implications. J Interpers Violence 19(11): 1296-1323.
-
Ronen IH, Esther S (2020) Becoming Teletherapeutic: Harnessing Accelerated Experiential Dynamic Psychotherapy (AEDP) for Challenges of the Covid 19 Era. Journal of Contemporary Psychotherapy 50(4): 265- 273.
-
Simmons CA, Lindsey L, Delaney MJ, Whalley A, County S, et al. (2015) Real-World Barriers to Assessing and Treating Mental Health Problems With IPV Survivors: A Qualitative Study. Journal of Interpersonal Violence 30(12): 2067-2086.
-
Sorrentino AE, Iverson KM, Tuepker A, True G, Cusack, M, et al. (2021). Mental health care in the context of intimate partner violence: Survivor perspectives. Psychological Services 18(4): 512-522.
-
Sugg N (2015) Intimate partner violence: prevalence, health consequences, and intervention. Med Clin North Am 99(3): 629-649.
-
Tjaden P, Thoennes N (2000) Extent, nature and consequences of intimate partner violence: Findings from the National Violence Against Women Survey.’Washington, DC: National Institute of Justice and the Centers of Disease Controland Prevention.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis