Continuous Low-Grade Transmission of Dengue Virus in Winter Months-A Cause of Endemicity in Tropical Countries
Dengue is one of the most important mosquito borne viral diseases affecting patients in the monsoon and post monsoon period. The present study was carried out to determine the seropositivity and seasonal variation of dengue infection in West Bengal. A total of 7655 samples were tested for Dengue IgM during the period November 2012 to October 2018 with 1899 samples being tested positive. The most affected age group was 21-30 years. The monsoon and the postmonsoon period saw a peak in the number of cases especially in the months of September, October and November with ongoing low-grade transmission during the winter months.
Introduction
Dengue, an acute arboviral infection transmitted by mosquitoes has recently caused large epidemics. Entities of major global concern include dengue fever with its associated dengue hemorrhagic fever (DHF) and shock syndrome (DSS) and India reports high incidence [1]. The first epidemic of clinical dengue-like illness was recorded in Madras in 1780 and the first virologically proved epidemic of Dengue Fever in India occurred in Calcutta Continuous Low-Grade Transmission of Dengue Virus in Winter Months-A Cause of Endemicity in Tropical Countries and Eastern Coast of India in 1963-1964. Since then the disease has been reported often in many states of India in epidemic proportions, causing huge morbidity and mortality [2, 3, 4, 5, 6, 7, 8].
Dengue fever is caused by dengue virus, a single stranded positive sense RNA virus in the genus Flavivirus, belonging to family Flaviviridae [9]. Dengue fever was believed to be caused by four different serotypes that share an antigenic relationship (DENV-1, DENV-2, DENV- 3 and DENV-4). The fifth variant DENV-5 has been isolated in October 2013 which follows the sylvatic cycle unlike the other four serotypes which follow the human cycle [10]. Principle vectors of transmission for Dengue infection are arthropods of the Aedes genre, especially Virol Immunol J
Aedes aegypti and Aedes albopictus. Maximum transmission of dengue is seen in the months of rainfall due to increased breeding of the vectors in water collections like pots, old tyres, un-used open cans etc [11].
Dengue was primarily a disease of the tropical countries. Following World War II, spread has been noted in temperate countries as well. Environmental factors including weather variables like temperature, rainfall, and relative humidity play a significant role in its transmission. Societal factors such as dense urbanization and increased transportation coupled with decrease in mosquito control efforts, lack of adequate sanitation and improper water storages have also contributed to the spread of dengue during the latter part of 20th century [12, 13].
The present study was carried out to determine the epidemiological determinants and seasonal variation in dengue infection which could help in predicting epidemics and rendering adequate control measures.
Aims and Objectives
- To study the demographic profile of dengue patients.
- To study the seasonal trend of dengue infection.
- To find out whether there is continuous circulation of Dengue virus in winter months and its impact on epidemiology.
Materials and methods
Study Type
The study is a descriptive cross-sectional study.
Study Area
The study was done in Department of Microbiology, Medical College, Kolkata which is a tertiary care hospital in West Bengal.
Study Population
Patients from Kolkata and adjoining districts of West Bengal, of different age groups and both genders who came to Medical College & Hospital, Kolkata with a history of fever and were clinically suspected to be suffering from dengue were included in the study. Sample size was not determined a priori since the study enrolled all patients who had febrile illness clinically suspected to be dengue and were referred to Department of Microbiology for laboratory confirmation.
Study Period
- Samples were collected from November 2012 to October 2018.
- Patients with fever for more than or equal to 5 days were tested for Dengue IgM antibody by MAC ELISA technique.
- Result analysis was done from November 2018 to January 2019.
Subject Selection Criteria
Inclusion Criteria
Blood samples from all patients with fever, joint pain with or without rash for duration of equal to or more than 5 days to less than 4 weeks, clinically diagnosed as dengue coming to Department of Microbiology for IgM screening were included in this study.
Exclusion Criteria
The following patients were excluded from the study:
- All cases of joint pain for a duration of more than 4 weeks or fever more than 4 weeks
- Those having a history of chronic joint pain
- Those with serologically confirmed diagnosis of Chikungunya, Rheumatoid Arthritis and Systemic Lupus Erythematosis.
- Patients unwilling to give consent or blood.
Patient Details
Relevant history of suffering from fever, headache, nausea, rashes etc. were taken, and clinical examination of the patients were performed.
Investigations such as haemoglobin (Hb), the total and the differential leucocyte counts (TLC and DLC), platelet count, haematocrit (Hct), liver function tests (LFT), Urea, Creatinine, Chest X-Ray and Ultrasonography of abdomen were done in all the patients.
Other relevant investigations were performed according to the clinical conditions of the patients.
Collection of Blood
With aseptic precautions blood was collected from clinically suspected cases and serum was separated by centrifugation. It was stored at -20°C until further testing.
Enzyme Linked Immuno Sorbent Assay (Elisa)
The serum samples of patients were tested for Dengue IgM antibody with history of fever for equal to or more than 5 days and less than 4 weeks using commercial kits as per availability. The commercial kits included NIV Dengue IgM Capture ELISA manufactured by National Institute of Virology (NIV) & InBios Dengue IgM ELISA manufactured by Inbios Diagnostics. Manufacturer’s instructions were followed strictly while performing the ELISA. Values were calculated and results were interpreted as per manufacturer’s guidelines.
Data Analysis
For statistical analysis data were enrolled into a Microsoft Excel spreadsheet and then analyzed by Epi Info 7 and Graph Pad Prism version 5. Rate of positivity was estimated by analyzing data for the results of Dengue IgM by ELISA tests and any variations in disease reporting by gender, age, season and the trend of the infection in the 6 year period were assessed.
Data were summarized as mean and standard deviation for numerical variables and counted and percentages for categorical variables were enumerated. The unpaired proportions were compared by Chi-square test. The p-value was calculated wherever required and value ≤0.05 was considered to be statistically significant.
Results
In our study between November 2012 and October 2018, a total of 7655 samples from suspected Dengue cases were received in the Department of Microbiology, Medical College, Kolkata. These samples were received from both the in-patient and out-patient departments of the hospital. Out of these 7655 clinically suspected cases for dengue, 1899 cases were positive for Dengue IgM (24.8%) (Tables 1 & 2), (Figures 1-3).
Males (55.91%) were affected more than the females (44.09%). The seropositivity rate was also slightly higher in the males (26.23%) than the females (22.99%).
| Gender | Positive | Negative | Total | Positivity Rate | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | 1123 (59.14%) | 3157 | 4280 (55.91%) | 26.23% | |||||||||
| Female | 776 (40.86%) | 2599 | 3375 (44.09%) | 22.99% | |||||||||
| Total | 1899 (100%) | 5756 | 7655 (100%) | 24.80% |
Table 1: Age wise distribution of Dengue samples.
Positive
Negative
| Years | Positive | Negative | Suspected | Prevalence | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0-10 yr | 304 | 1393 | 1697 | 17.91% | ||||||||
| 11-20 yr | 442 | 1147 | 1589 | 27.81% | ||||||||
| 21-30 yr | 503 | 1189 | 1692 | 29.72% | ||||||||
| 31-40 yr | 307 | 793 | 1100 | 27.90% | ||||||||
| 41-50 yr | 169 | 531 | 700 | 24.14% | ||||||||
| above 50 yr | 174 | 703 | 877 | 19.84% | ||||||||
| Total | 1899 | 5756 | 7655 |
Table 2: Age wise distribution of Dengue samples.
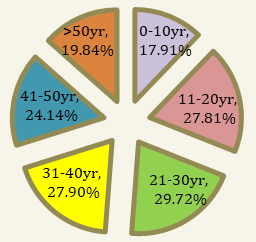
0 Table 2 and Figure 3 show the age wise distribution of Dengue suspected cases and Dengue positive cases. The age group between 21-30 yrs was the most affected with a percentage of positivity of 29.72% followed by age groups of 31-40 yrs (27.90%) and 11-20 yrs (27.81%). Age group of 0-10 yrs was the least affected.
The sprout in the number of Dengue cases started from the month of August about one month after the monsoon arrival in this part of the world and the number of suspected cases and positive cases increased every successive month.
Significant number of cases occurred during early winter. Percentage of positivity during the month of November was 33.01% which is only second highest after the month of October (34.51%).
The month of February has the lowest number of positive cases, which signifies a break in Dengue transmission. February 2012 recorded no positive cases. However other years recorded few positive cases.
| Months 2012 to 2018 | Total | Positive | Percentage | ||||
|---|---|---|---|---|---|---|---|
| Nov | 1466 | 484 | 33.01% | ||||
| Dec | 564 | 114 | 20.21% | ||||
| Jan | 247 | 29 | 11.74% | ||||
| Feb | 217 | 21 | 0.09% |
Table 3: The trend of Dengue cases per year from Nov 12 to Oct 18.
Year wise the year between Nov15 to Oct16 recorded highest positive rate 36.61% (681 cases were positive out of 1860 suspected). However subsequent years between Nov16- Oct17 and Nov17- Oct18, showed a gradual decline in the rate of positivity of 21.83% and 17.52% respectively. The decline may signify development of herd immunity among the population, although few positive cases continue to occur in winter months. The reduction in the positive cases of Dengue in the winter has been found to be statistically significant (P value of 0.0450).
| Susoected | Positive | Prevalence rate per year | |||||||
|---|---|---|---|---|---|---|---|---|---|
| nov12- oct13 | 388 | 106 | 27.31% | ||||||
| nov13- oct14 | 325 | 61 | 18.76% | ||||||
| nov14- oct15 | 592 | 174 | 29.39% | ||||||
| nov15- oct16 | 1860 | 681 | 36.61% | ||||||
| nov16- oct17 | 2088 | 456 | 21.83% | ||||||
| nov17- oct18 | 2402 | 421 | 17.52% | ||||||
| 7655 | 1899 |
Table 4: The trend of Dengue cases per year from Nov 12 to Oct 18.
Positivity rate per year
nov17- oct18 nov16- oct17 nov15- oct16 nov14- oct15 nov13- oct14 nov12- oct13
0 10 20 30 40 Positivity rate per year Figure 7: The trend of Dengue cases per year from Nov12 to Oct18.
Discussion
The number of Dengue cases are steadily increasing every year [14].
In the present study out of 7655 clinically suspected cases, 1899 cases (24.8%) were found to be positive for Dengue infection by IgM ELISA. The results were congruent with studies by Deshkar ST, et al. [15], Sathish JV, et al. [16], Biradar A, et al. [17], Pruthvi D, et al. [18], Garg A, et al. [19]. Few studies have reported lower prevalence rate ranging from 3- 14% and some have reported a higher prevalence ranging from 28-66% [20, 21, 22, 23, 24]. The difference in seroprevalence could be due to differences in study periods, differences in geographical areas and differences in climatic conditions.
In the present study, male preponderance was seen (55.91%). The seropositivity was also slightly more in the males (26.23%) as compared to females (22.99%) which is similar to other studies such as Deshkar, ST et al. [15], Sathish JV, et al. [16], Garg A, et al. [21], Neralwar, et al. [25] and Mehta KD, et al. [26].
The present study found maximum clinically suspected cases in the age group of 0-10 years (1697 cases) similar to the findings of other studies. However, rate of positivity was highest in the age group 21- 30 years (29.72%) followed by 31- 40 years (27.9%) and 11-
20 years (27.81%) similar to the findings of studies by Girish BRJ, et al. [27], Prakash B, et al. [28], Ukey PM, et al. [29], Kumar A, et al. [30], Gupta E, et al. [31]. Few studies have reported paediatric age group as the most affected age group [15, 16, 17, 18, 19, 32, 33].
A seasonal trend of Dengue summed up for 6 years showed the number of cases started to increase from the monsoon months and maximum cases being reported in September, October and November but most number of positive cases occurred in October. The findings are similar to studies by Dishakar ST et al. Aug-Nov (Maharashtra) 16, Garg A Sept- Oct (Bidar)22, Gupta E October (Delhi) [34], Mandal SK Oct-Nov (Northeast) [35] Singh J September (Lucknow) and Kumar A (Udupi) [30, 36]. The reason for such peak could be due to collection of rain water and inadequate sanitation and drainage systems helping in the proliferation of the vectors. Certain studies showed highest number of cases being reported in the monsoon months by Satish JV, et al. [37], Kauser MM, et al. [38] in Central India, Madhumati R, et al. [39] at Bangalore and Chakravati A, et al. [40] in Myanmar.
The trend of Dengue cases per year from Nov12 to Oct18 shows most cases being reported in the year Nov15- Oct16 (positivity rate 36.61%; 681 cases were positive out of 1860 suspected), followed by Nov14- Oct15 (positivity rate 29.39%; 174 cases were positive out of 592 suspected). However it was noted that though clinically suspected cases were being reported more in the subsequent years, the positivity rate has declined; Nov16- Oct17 (positivity rate 21.83% with suspected cases being 2088) and Nov17- Oct18 (positivity rate 17.52% with suspected cases being 2402). Also the positivity rate in Nov16-Oct17 and Nov17-Oct18 was much less than Nov15-Oct16 which could be due to development of herd immunity in general population as well as more testing for Dengue as there is easy availability of Dengue virus testing procedures.
In our study dengue positive cases occurred throughout the year. During the winter months between November and February in the 6 year period, it has been observed that positive cases of Dengue were reported which signifies continuous transmission of Dengue virus during the winter months which is consistent with other studies.15, 16, 22 This possibly signifies that the over- wintering phenomenon which is seen in temperate countries does not occur in tropical countries like India. The trans-ovarian transmission of the Dengue virus as a mechanism of overwintering and subsequent re- introduction of Dengue virus by the vectors Aedes aegypti and Aedes albopticus is probably not important where there is continuous transmission is occurring.
| Transmission months | Positive Cases | Negative Cases | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Rainy Season | 1170 | 2967 | 4137 | ||||||||
| Winter Season | 648 | 1846 | 2494 | ||||||||
| Total | 1818 | 4813 | 6631 |
Table 5: Comparison of the difference between transmission of Dengue infection in rainy season and winter season. Chi-square test
Table 5: Comparison of the difference between transmission of Dengue infection in rainy season and winter season. Chi-square test - 4.018 with 1° of freedom P value - 0.0450 All four serotypes were in co-circulation during the period of August to December 2016 as per study conducted by Barik G, et al. [41] in our hospital. Possibly all four serotypes remain in circulation even after that. However the DENV-1, DENV-3 and DENV-4 infection were less common beyond 30 years of age and prevalence of
Conclusion
Dengue has been a substantial cause of febrile illness in Kolkata. The most affected age group is 21-30 years and a male preponderance has been observed. Peak in the number of cases has been observed in the months of September, October and November which could be due to collection of rain water and improper drainage systems. Also, although in low levels, a continuous transmission of Dengue infection has been observed in the winter months. Community awareness, confirmatory diagnosis and management and vector control measures is the need of the hour to decrease the magnitude of Dengue illness.
References
-
Knipe DM, Howley PM, Lamb RA, Griffin DE, Martin MA, et al. (2012) Fields Virology 1(4): 991-1125.
-
Sarkar JK, Chatterjee SN, Chakravarty SK (1964) Haemorrhagic fever in Calcutta: some epidemiological observations. Indian J Med Res 52: 651-659.
-
Chatterjee SN, Chakravarti SK, Mitra AC, Sarkar JK (1965) Virological investigation of cases with neurological complications during the outbreak of haemorrhagic fever in Calcutta. J Indian Med Assoc 45(6): 314-316.
-
Carey DE, Myers RM, Reuben R, Rodrigues FM (1966) Studies on dengue in Vellore, South India. Am J Trop Med Hyg 15(4): 580-587.
-
Balaya S, Paul SD, D'Lima LV, Pavri KM (1969) Investigations on an outbreak of dengue in Delhi in 1967. Indian Journal of Medical Research 57(4): 767- 774.
-
Rodrigues FM, Patankar MR, Banerjee K, Bhatt PN, Goverdhan MK, et al. (1972) Etiology of the 1965 epidemic of febrile illness in Nagpur city, Maharashtra State, India. Bulletin World Health Organization 46(2): 173-179.
-
Padbidri VS, Dandawate CN, Goverdhan MK, Bhat UK, Rodrigues FM, et al. (1973) An investigation of the aetiology of the 1971 outbreak of febrile illness in Jaipur city, India. Indian Journal of Medical Research 61(12): 1737-1743.
-
Karamchandani PV (1937) Study of 100 cases of dengue fever in Madras Penitentiary. Indian Med Gazette 72(9): 532-534.
-
WHO (2009) Library Cataloguing in Publication Data Dengue Guidelines for diagnosis, treatment and control, pp: 58-105.
-
Mustafa MS, Rastogi V, Jain S, Gupta V (2015) Discovery of fifth serotype of dengue virus (DENV-5): a new public health dilemma in dengue control. Medical Journal armed forces of India 71(1): 67-70.
-
Mandell G, Bennett J, Dolin R (2010) Mandells, Doughlas and Bennett’s Principle and practice of Infectious diseases, 7th (Edn.), Churchill Livingstone Elsevier, Philadelphia 2: 2133-2156.
-
Wongkoon S, Jaroensutasinee M, Jaroensutasinee K (2011) Climatic variability and dengue virus transmission in Chiang Rai, Thailand. Biomedica 27: 5-13.
-
Bi P, Zhang Y, Parton KA (2007) Weather variables and Japanese encephalitis in the metropolitan area of Jinan city, China. J Infect 55(6): 551-556.
-
Shepard DS, Halasa YA, Tyagi BK, Adhish SV, Nandan D, et al. (2014) Economic and disease burden of dengue illness in India. Am J Trop Med Hyg 91(6): 1235-1242.
-
Deshkar ST, Raut SS, Khadse RK (2017) Dengue infection in central India: A 5 years study at a tertiary care hospital.Int J Res Med Sci 5(6): 2483-2489.
-
Sathish JV, Wadekar Mita D, Pooja C (2017) Dengue NS1 Antigen for Early Detection of Dengue Infection. Int J Curr Microbiol App Sci 6(10): 2054-2058.
-
Biradar A, Kauser Y, Itagi I, Jamadar NA (2016) Dengue infection: Its prevalence with seasonal variations. Indian J Microbiol Res 3(2): 89-92.
-
Pruthvi D, Shashikala P, Shenoy V (2012) Evaluation of platelet count in dengue fever along with seasonal variation of dengue infection. J Blood Disorders Transf 3(4): 1-4.
-
Garg A, Garg J, Rao YK, Upadhyay GC and Sakhuja S (2011) Prevalence of dengue among clinically suspected febrile episodes at a teaching hospital in North India. Journal of Infectious Diseases and Immunity 3(5): 85-89.
-
Wadekar MD, Naik TB, Upadhya AK, Swarooparani NB (2016) Prevalence of Malaria, Enteric fever, Dengue and Rickettsial diseases in fever cases at tertiary care hospital. International journal of microbiology research 8(1): 720-722.
-
Garg A, Gangane R, Asharani S, Sharanabasava (2015) Seroprevalence of Dengue in North Karnataka. JMSCR 3(6): 6192-6198.
-
Arunasree B, Uma P, Rajsekhar B (2015) Epidemiology of dengue fever in Srikakulam District, Andhra Pradesh. Journal of Evolution of Medical and Dental Sciences 4(27): 4599-4604.
-
Mehta KD, Gelotar PS, Vachhani SC, Makwana N, SinhaM (2014) Profile of dengue infection in Jamnagar city and district, West India. WHO South- East Asia Journal of Public Health 3(1): 72-74.
-
Jayasimha VL, Thippeswamy MTR, Yogesh Babu KV, Vinodkumar CS, Niranjan HP, et al. (2012) Dengue: Seroprevalence, Comparison of rapid test with ELISA. National Journal of Basic Medical Sciences 3(1): 57-60
-
Neralwar A, Banjare B, Barapatre R (2015) Detection of NS1 antigen, IgM antibody for the diagnosis of Dengue infection in patients with acute febrile illness. Int J Res Med Sci 3(10): 2826-2830.
-
Arunasree B, Uma P, Rajsekhar B (2015) Epidemiology of dengue fever in Srikakulam District, Andhra Pradesh. Journal of Evolution of Medical and Dental Sciences 4(27): 4599-4604.
-
Mehta KD, Gelotar PS, Vachhani SC, Makwana N, SinhaM (2014) Profile of dengue infection in Jamnagar city and district, West India. WHO South- East Asia Journal of Public Health 3(1): 72-74.
-
Girish BRJ, Madhuri KR (2016) A clinicomicrobiological study of dengue fever cases at Sri Siddhartha Medical College & Hospital, Tumkur. Indian J Microbiol Res 3(2): 209-212.
-
Prakash B, Darshan D (2015) Catching dengue early: clinical features and laboratory markers of Dengue virus infection. JAPI 63(5): 38-41.
-
Ukey PM, Bondade SA, Paunipagar PV, Powar RM, Akulwar SL (2010) Study of seroprevalence of dengue fever in central India. Indian Journal of Community Medicine 35(4): 517-519.
-
Kumar A, Rao CR, Pandit V, Shetty S, Bammigatti C, et al. (2010) Clinical manifestations and trend of dengue cases admitted in a tertiary care hospital, Udupi district, Karnataka. Indian J Community Med 35(3): 386-390.
-
Gupta E, Dar L, Narang P, Srivastava VK, Broor S (2005) Serodiagnosis of dengue during an outbreak at a tertiary care hospital in Delhi. Indian J Med Res 121(1): 36-38.
-
Shah GS, Islam S, Das BK (2006) Clinical and laboratory profile of dengue infection in children. Kathmandu University Med J 4(1): 40-44.
-
Anderson KB, Chunsutiwwat S, Nisalak A, Mameen P, Libarty DH, et al. (2007) Burden of symptomatic dengue infection in children at primary school in Thailand: a prospective study. Lancet 369: 1452-1459
-
Gupta E, Dar L, Kapoor G, Broor S (2006) The changing epidemiology of dengue in Delhi, India. Virol J 3: 92.
-
Mandal SK, Ganguly J, Sil K, Chatterjee S, Chatterjee K, et al. (2013) Clinical profiles of Dengue fever in a teaching hospital of Eastern India. Nat J Med Res 3(2): 173-176.
-
Singh J, Dinkar A, Atam V, Himanshu D, Gupta KK, et al. (2017) Awareness and outcome of changing trends in clinical profile of Dengue fever: A retrospective analysis of Dengue epidemic from January to December 2014 at a tertiary care hospital. Journal of the association of physicians of India 65(5): 42-46.
-
Sathish JV, Trupti BN, Krishna VM, Begum A, Biradar (2018) Dengue Infection - prevalence and seasonal variation among patients attending a tertiary care hospital at Chamarajanagar, Karnataka. Indian Journal of Microbiology Research, April-June 5(2): 275-279.
-
Kauser MM, Kalavathi GP, Radadiya M, Karthik M, Afreen A, et al. (2014) A study of clinical and laboratory profile of Dengue fever in tertiary care hospital in Central Karnataka, India. GJMR-B 14(5).
-
Madhumati R, Kavya ST, Amrutha A, et al. (2014) Demographic profile of Dengue infections in Bangalore: An Observational Study. Internat J Clin Cases Invest 5: 6-14.
-
Chakravarti A, Kumaria R (2005) Eco-epidemiological analysis of dengue infection during an outbreak of dengue fever, India. Virol J 2: 32.
-
Barik G, Dey M, Sengupta M, Chatterjee RP, Sarkar S, et al. (2017) Co-Circulation of All Dengue Serotypes among Patients Attending a Tertiary Ca re Hospital in Kolkata. Virol & Imm J 2(9): 1-7.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions