The Covid Calamity, the Human Life, and the Surviving Hope
Introduction - Ongoing Covid-19 Calamity: As a disease, COVID-19 is still in the pandemic phase because infections continue to increasingly occur world-wide and various population groups are still susceptible. It is likely that the SARS-CoV-2 will not be eradicated but become endemic and continue to circulate and cause infections in pockets of the global populations for years to come. It may evolve into more transmissible and virulent forms with novel mutations and variants, and associated factors may worsen the overall scenario with involvement of newer population groups and world regions. Mutations, Variants and Immune Escape: The unabated prevalence increases risk of mutations, as the virus has more chances to mutate. Further, in areas where the incidence rates are high, selection pressures favour the emergence of variants that evade neutralising antibodies. Furthermore, as population groups receive vaccination, immune pressure is conjectured to facilitate and speed up the emergence of such variants by selecting for escape mutants. In due course, these selected variants would replace previous versions of the virus propelling the pandemic or the endemic disease later on. Associated Uncertainties with SARS-CoV-2: There are various associated uncertainties with the SARS-CoV-2 virus and the disease it causes. Due to evolving genomic changes, the virus elicits erratic and labile immune response. Simultaneously, the host factors are highly variable and largely uncontrollable. Further, the control measures and available vaccines for COVID-19 may not reduce the prevalence of infections drastically for multiple reasons. These epidemiological drivers would lead to persistence of the virus and endemicity of the disease interspersed by periodic outbreaks and re-emergence. The Human Life during Covid-19 Pandemic: With COVID-19 becoming an endemic disease, the SARS-CoV-2 virus would be first encountered during childhood, typically causing mild manifestations or none. The population groups will develop some immunity through natural infection or vaccination and may not suffer with severe illness, except in those with comorbid conditions or immune-compromised states, and the disease course would depend on evolving variants, efficacy of vaccines, and nature of immunity to the virus. The herd immunity against SARS-CoV-2 may remain a myth and with individual immunity being labile and waning after 6-8 months, booster doses of updated vaccine will be required at regular intervals. Future Scenario and Search for Solutions: To mitigate the spread of SARS-CoV-2 virus, various countries have implementeda wide range of control measures from time to time and likely to resort to, in future as well. There is need for genotyping and genomic sequencing capability for quick and effective utilization of epidemiological data. Simultaneously, the large deployment of COVID-19 vaccines under way needs a rapid and effective global effort. The next-generation vaccines may stimulate T cells effectively, apart from generating antibodies against the virus, and there is possibility of designing a universal coronavirus vaccine or pan-virus vaccine for immunisation against multiple variants and strains. On the therapeutic side, use of probiotics as adjuvant therapy may Improve the prognosis and clinical outcomes in COVID-19.
The Resilient Virus and on-going Pandemic
Over hundreds of coronaviruses infect bats, pigs, camels, dogs and cats, and other animals. The seven types of coronaviruses infect humans; the first four human coronaviruses include HCoV-229E, HCoV-OC43, HCoV-NL63 and HCoV-HKU1, which cause mild to moderate upper- respiratory tract illnesses. Whereas other three aggressive human coronaviruses capable of causing serious morbidity and even mortality, have emerged during the last two decades and include SARS-CoV, MERS and now SARS-CoV-2. The influenza pandemic, which afflicted humanity in 1918 with fatality over 50 million people world-wide, is yardstick by which all other pandemics are compared [1].
The pandemic was caused by influenza a virus, which originated in birds. Since then, all the later influenza epidemics have been caused by descendants of the 1918 virus. Presently the influenza virus descendants circulate the globe and infect a significant number of people each year. The influenza epidemic occurs when a population group is naive to the virus and with the population groups developing immunity to the virus; it may become a seasonal disease. This is well exemplified by swine flu caused by influenza a virus subtype H1N1 in year 2009-10.
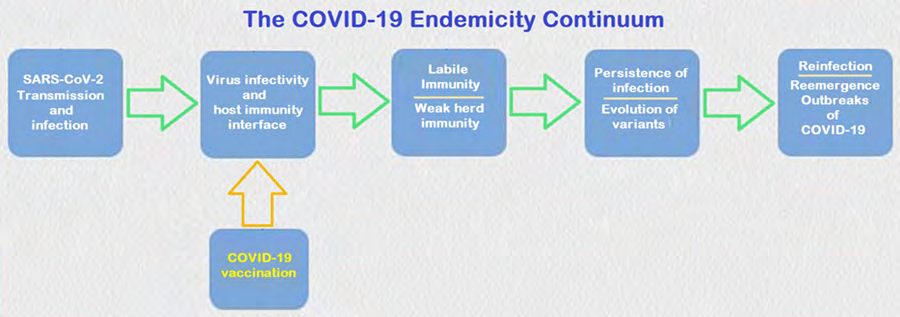
As a disease, COVID-19 is still in the pandemic phase because infections continue to increasingly occur world- wide and various population groups remain susceptible. It is expected the SARS-CoV-2 will not be eradicated but become endemic, continuing to circulate in pockets of the global population for years to come and causing outbreaks in regions where it had been earlier eliminated [2]. The optimistic view holds that the impact of COVID-19 on the humanity in terms of social isolation, morbidity, and mortality may lessen, as the population groups acquire some immunity through natural infection or from vaccination and the disease becomes endemic. Whereas the pessimistic view holds that with on-going evolution of new mutations and variants and other variables may worsen the scenario with involvement of newer population groups and world regions (Figure 1).
If vaccines are able to block transmission and effective against novel variants it may be possible to achieve herd immunity in regions where enough number of people are vaccinated. It has been shown that a vaccine that is 90% effective would need to reach at least 55% coverage to achieve temporary herd immunity with social distancing measures, face masking, and a large number of people working from home. The similar vaccine would need 67% coverage or even higher levels if the vaccine is less than 90% effective at blocking transmission or if there is increased transmission because of a new variant, to provide herd immunity if the control measures are not followed or lifted [3].
A large study has shown that levels of neutralising antibodies start to decline after around six to eight months following SARS-CoV-2 infection. If a new infection arises, the memory B cells can produce antibodies and T cells that can eliminate virus infected cells, but it is not established whether this immune memory can block the viral reinfection. It could take years or even decades to reach a state where enough of the population has sufficient immunity. Further, allowing the virus to spread unchecked to that point may result in millions of deaths world-wide, so the immunity through vaccination is the choice. In fact, there are various uncertainties associated with the virus, SARS-CoV-2 and the disease, COVID-19 it causes. The virus has a large genome and prone to mutations, yet simultaneously, it carries the nsp14 protein, which acts as a 3′-5′ exoribonuclease and has proofreading functions during the viral replication cycle. The immunity developed to the virus appears to be short-term and labile; lasting for 6-8
months at most and with evolving mutations and variants, the virus can potentially evade or escape immunity acquired following natural infection or by vaccination [4].
Mutations, Variants and Immune Escape
Mutations and Evolution of New Variants
The higher number of cases increases risk of mutations, as the virus has more chances to mutate. Further, in areas where the prevalence of the virus is high, selection pressures favour the emergence of variants that evade neutralising antibodies. Further, once a large population receives vaccination, immune pressure is conjectured to facilitate and speed up the emergence of such variants by selecting for escape mutants. Thus, in its gradual course, the disease will evolve into a phase of mutations and emerging variants. Further, the new variants are likely to have mutations in the parts shown to increase the ability of the virus to infect cells. SARS-CoV-2 may evolve to escape immunity, like the historical evolution of human coronavirus 229E [5]. In due course, these selected variants would replace previous versions of the virus propelling the pandemic or the endemic disease later on. Considering the inherent epidemiological features, COVID-19 may remain a serious endemic threat for years to come or even decades.
THE SARS-CoV-2 virus undergoes mutations in its genome, crucially affecting the S protein frequently targeted by antibodies. Compared to the current emerging variants, the earlier D614G mutation increased the transmission ability of the virus compared to the ancestral virus without the mutation. When the mutation slices out a section of the genome, the change is called a deletion. Various studies have shown that deletions tend to occur mostly at few distinct sites in the genomic region coding for S protein. McCarthy, et al have identified more over 1,000 samples with deletions in the genomic region [6].
An important variant of SARS-CoV-2 is B.1.1.7 lineage (The UK variant, VOC202012/01, 20I/501Y.V1). It carries a mutation in the RBD of the S protein at position 501, replacing asparagine (N) with tyrosine (Y), termed as N501Y, which appears to help the virus spread more easily. The mutation is also seen in SA variant and in Brazilian variant, P1. In addition, the variant has 69/70 deletion resulting in a conformational change in the S protein and P681H mutation near the S1/S2 furan cleavage site. The variant can potentially evade detection by viral diagnostic tests, has an enhanced transmissibility, and a probable heightened mortality risk. There has been found a new variant B1525 in the UK, which has genomic similarities to the B117 variant and contains a number of mutations including the E484K mutation to the S protein.
B.1.351 lineage (The SA variant, 20H/501Y.V2) carries several mutations in the spike protein, which include K417N, E484K, N501Y, but not the 69/70 deletion. It has E484K mutation, having an impact on neutralization by some polyclonal and monoclonal antibodies, leading to immune escape. The early results suggest that the T cells could be less vulnerable to the mutation as T-cell responses to COVID-19 vaccination or previous infection do not target the mutated regions. Thus, if T cells remain active against the 501Y.V2 variant they might protect against severe disease.
P.1 lineage (Brazil variant, 20J/501Y.V3) has 17 unique mutations and three mutations in the S protein RBD, including K417T, E484K, and N501Y, which may have an impact on transmissibility and antigenic profile affecting the potential of antibodies produced by a natural infection or vaccine and diminished susceptibility to therapeutic agents like monoclonal antibodies. The P2 variant occurs throughout Brazil, but unlike the P1 variant, it is not yet clear whether P2 leads to any change in the course of illness. The most widely disseminated SARS-CoV-2 Brazilian lineage B.1.1.33 that evolved from an ancestral clade, here designated B.1.1.33-like. The B.1.1.33-like lineage may have been introduced from Europe or may have arisen in Brazil in early February 2020 and a few weeks later gave origin to the lineage B.1.1.33 [7].
The Driving Factors for COVID-19 Endemicity
There are multiple associated uncertainties with the SARS-CoV-2 virus and the disease it causes. The virus is evolving through mutations and genomic changes, it elicits erratic and labile immune response, and various factors including the host factors are variable and to some extent uncontrollable, making it difficult to predict the course of the disease in the current scenario. Further, the control measures and available COVID-19 vaccines do not appear to reduce the prevalence as well as the severity of infections drastically as the result of appearance of viral variants which can evade immunity and lead to persistence of the virus resulting in periodic outbreaks and emergent epidemics [8].
In an endemic disease phase, the infections become relatively constant across years, with occasional flare- ups. It is being conjectured that SARS-CoV-2 may follow a similar course and with time, the COVID-19 may become a much less serious challenge and evolve into a seasonal disease interspersed with intermittent outbreaks. Over time COVID-19 may become a disease first encountered in early childhood, typically causing mild infection or none at all. But this optimistic turn of events is not being heralded so far.
There are certain epidemiological driving variables leading to persistence of the virus and endemicity of the disease interspersed by periodic outbreaks and re- emergence (Figure 2).
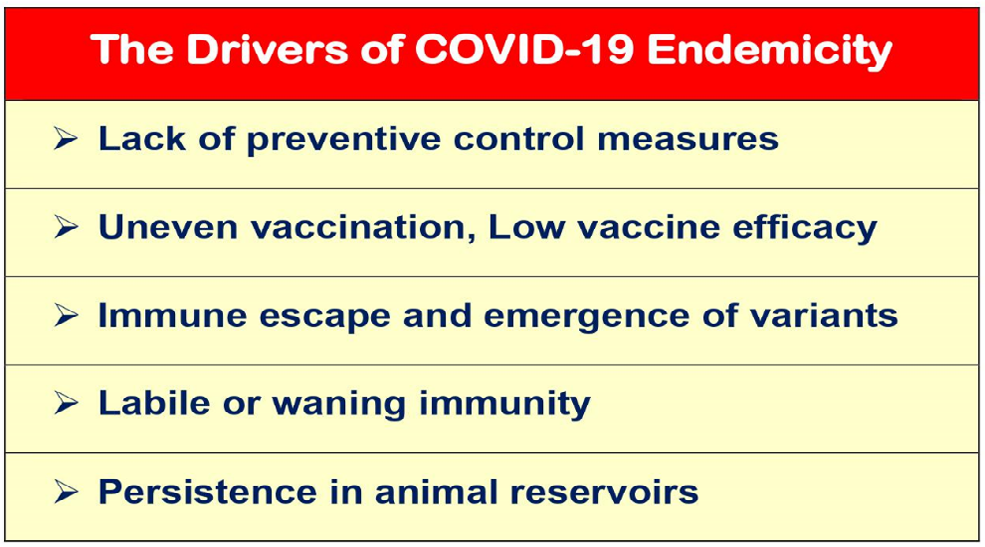
The evolutionary selection pressures on SARS-CoV-2 are not geographically specific. In fact, the virus is encountering similar selection pressures wherever it is transmitting and has relatively high prevalence. Thus, the selection for random mutations that can confer a fitness advantage for the virus can happen anywhere, and at any time. The speed and success of vaccination may impose another selection pressure on the evolution of the virus, leading to selection of new mutations and emergence of novel variants with ability to persist and propagate.
The immune escape is supposed to be a major driver for the virus’s continuing circulation. There is decreased neutralization of variants due to antigenic evolution of the viral S protein, especially in the receptor-binding domain (RBD). Immunity from past vaccination or infection should blunt the disease severity as with various endemic coronaviruses, but the accumulated mutations to SARS-CoV-2 may significantly erode neutralizing antibody immunity and the efficacy of SARS-CoV-2 vaccines. Further, if the vaccines do not stop some people from developing severe disease manifestations, the virus will continue to be a significant disease burden. A similar situation could emerge if a large number of people decline cOVID-19 vaccines.
The variants B.1.1.7, B.1.1.298, or B.1.429, continue to be potently neutralized despite the presence of mutations in RBD [9]. Other SARS-CoV-2 variants may escape vaccine- induced humoral immunity. The P.2 variant, which contains an E484K mutation within the RBD region, is capable of significantly reducing the neutralization potency of fully vaccinated individuals. Similarly, the P.1 strain, which has three RBD mutations, can more effectively escape neutralization. The B.1.351 variant exhibits remarkable resistance to neutralization, largely due to three mutations in RBD but with a measurable contribution from non-RBD mutations [10].
As documented, the efficacy of vaccines fades in the face of the 501Y.V2 variant. At least three vaccines, by Novara, Johnson & Johnson, and Oxford-AstraZeneca vaccines are less effective at protecting against mild COVID-19 in South Africa, where the 501Y.V2 variant dominates. For Oxford- AstraZeneca vaccine, the efficacy was reported to be only 22% effective against mild COVID-19 in a sample of 2,000 people in South Africa. The newly emerging and fast-spreading SARS- CoV-2 variants can also potentially reduce the protective effects of the mRNA COVID-19 vaccines by Pfizer-BioNTech and Moderna, Inc. [11]. As noted, within 3–14 weeks after the second dose, those inoculated developed several types of antibodies, including some that can block SARS-CoV-2 from infecting cells, but the antibodies were only one-third as effective at blocking the mutated variants.
There is another potential possibility of the SARS-CoV-2 virus establishing itself in animal reservoirs. The endemicity of the disease will be influenced by its persistence in animal population, as evidenced by the outbreaks in mink farms [12]. The SARS-CoV-2 virus has been shown to be able to pass to and fro between minks and handlers, similar to several other viruses related to diseases such as yellow fever, Ebola, and chikungunya, where the viruses persist in animal reservoirs and find chances to spill back.
The Associated Uncertainties with Covid-19
The Immune Response to Infection and Vaccines
The concern about the SARS-CoV-2 variants that are partially resistant to antibody defences has spurred a renewed interest in other immune responses that may protect against the viruses. In case of the SARS-CoV-2 variants, where the antibodies generated following vaccination may become less effective, the cellular immunity can help to maintain an enduring immunity. In particular, the T cells response is important and appears to target and destroy the virus- infected cells.
The immune system produces mainly two types of the T cells in response to the infecting viruses. There are killer T cells (CD8+ T cells), which detect and destroy the virus infected cells, and the helper T cells (or CD4+ T cells), which stimulate the production of antibodies against the virus and killer T cells. As apparent, the T cells do not prevent infection, because they come into action only following the viral infection but play a role in clearing the viral infection. In the projected scenario in case of COVID-19, if CD8+ T cells are able to remove the virus-infected cells before they spread further from the upper respiratory tract, there will be restricted transmission due to reduced harbouring and shedding of the visions. This may reduce the severity of disease manifestations from severe to mild, as well.
The T cells may be more resilient than antibodies to threats posed by evolving mutations and emerging variants. Following SARS-CoV-2 infection, there are generated T cells targeting at least 15-20 different fragments of viral proteins. In addition, the T cells can target viral proteins expressed inside infected cells, some of which are essentially stable. But the protein snippets used as targets can vary widely from person to person and there evolve a large variety of T cells acting against the virus, hindering the mutations and immune escape, unlike the situation for antibodies. The immune system through the T cells is able to recognize SARS- CoV-2 in multiple ways.
Various studies have reported a robust antiviral T cell response in adults recovered from COVID-19 [13]. The observed robust T cell response is against the S protein as well as other viral proteins. The circulating SARS-CoV-2− specific CD8⁺ and CD4⁺ T cells have been identified in ∼70% and 100% of COVID-19 convalescent patients, respectively and correlate with the anti-SARS-CoV-2 IgG and IgA titers. The M, S and N viral proteins account for 11-27% of the total CD4⁺ response, with additional responses to nsp3, nsp4, ORF3a and ORF8, among others [14]. There has been done a comprehensive analysis to establish the patterns of immune dominance of different SARS-CoV-2 antigens and virus- specific CD4+ and CD8+ T cells, and SARS-CoV-2 epitopes in COVID-19 cases [15]. Further, both natural infection with SARS-CoV-2 and immunization with COVID-19 vaccines induce protective immunity but the vaccine-induced immunity is more robust heterotypic immunity than natural infection to emerging SARS-CoV-2 variants of concern [16].
Viral Genomic and Phylogenetic Analyses
In general, the SARS-CoV-2 variants emerging in a range of geographical locations seem to share certain mutations. The non-synonymous substitutions affecting S protein are common and affect a number of SARS-CoV-2 lineages. The repeated evolution of a trait in independent populations provides strong evidence of adaptation. The coincidental rise and spread of variants on separate genetic backgrounds is remarkable and suggests some fitness advantage. As such the mutations may enable the virus to escape from neutralizing antibodies or enhance transmission through increased affinity for the ACE2 receptors or similar mechanisms.
The genomic surveillance in the US has detected a rapid rise of numerous clade 20G (lineage B.1.2) infections carrying a Q677P substitution in the S protein. The phylogenetic analyses have revealed evolution and spread of six distinct Q677H sub-lineages, from the samples collected between mid-august to late November 2020. There are four 677H clades from clade 20G (B.1.2), 20A (B.1.234), and 20B (B.1.1.220, and B.1.1.222), and a pair of clade 20G clusters in varying number of cases. There is rise of S: 677 polymorphic variants, with the mutations in proximity of the polybasic cleavage site at the S1/S2, which is consistent with its functional relevance during cell entry. The evolution of the trait may confer an advantage in viral transmission.
In a recent study, Hodcraft, et al. has reported seven new variants of the SARS-CoV-2 virus in the US. The researchers are tracking virus variants and some of them may be more easily transmissible and more virulent than the ancestral virus and can affect the efficacy of vaccines. The researchers have named a new variant, Robin (first spotted in October), accounting for 27.8% of sequenced viruses in Louisiana and 11.3% in Mexico between the start of December 2020 and mid-January 2021 [17]. The researchers have identified six other variants with a mutation at the same position in the S protein. Interestingly, the variants have been named after American birds, as Robin 1 and Robin 2, Pelican, Yellowhammer, Mockingbird, Bluebird, and Quail.
There is some proof that the vaccines spur antibody surge against a COVID variant, as well. One shot of either the Modern or the Pfizer vaccine provokes a strong immune response against an emerging variant of SARS-CoV-2, according to tests in people who have recovered from COVID-19 [18]. In the study, before inoculation, nine of the ten individuals had neutralizing antibodies against the original virus, although the levels generated were highly variable. Antibodies from only five people could neutralize B.1.351. Following a single shot of the vaccine, however, participants’ levels of neutralizing antibodies against both forms of the virus increased by approximately 1,000-fold.
Mapping of Viral Mutations with Immune Escape
The global surveillance of genomic changes in SARS- CoV-2 varies widely, with leading countries such as Australia, New Zealand, the United Kingdom, and Denmark sequencing viruses from 5-50% of all cases and lagging countries such as the United States, France, Spain, and Brazil sequencing less than 1% of all cases. The mapping of viral mutations and variants with Immune escape capability identifies mutations that can escape antibody binding. Many of the mutations that escape single antibodies are found to be circulating in the human population in various regions. Further, many escape mutations do not impair the RBD folding or ACE2 affinity and that some are already present at low levels among circulating viruses.
Therapeutically, the anti–SARS-CoV-2 antibodies against viruses can be rendered ineffective by mutations that are selected during treatment of infected patients or that spread globally to confer resistance on entire viral clades. Therefore, determining which SARS-CoV-2 mutations escape key antibodies is essential for assessing mutations observed during viral surveillance [19]. The mapping of variants with Immune escape capability has scope for developing novel therapeutic modalities to deal with the COVID-19 pandemic and can help in developing effective anti–SARS- CoV-2 antibodies to target the RBD region of S protein which mediates binding to the ACE2 receptors.
Evolving Scenario and Expected Course
The Projected Course for COVID-19 Pandemic
The prime scenario, which seems to be the most optimistic eventuality, is the virus persisting with COVID-19 becoming an endemic disease. The population groups will develop some immunity to through natural infection or vaccination and may not suffer with severe disease, except in those with comorbid conditions or immune-compromised states. As occurs with other four endemic coronaviruses, OC43, 229E, NL63 and HKU1, responsible for roughly 15% of respiratory infections, the SARS-CoV-2 virus may be first encountered in early childhood when it typically causes mild clinical manifestations or none.
The other likely scenarios would depend on the evolving variants and the pattern of immunity to SARS-CoV-2 in long run. A large study of people who have had COVID-19 suggests that their levels of neutralizing antibodies which help to block reinfection start to decline after around six to eight months [20]. But apart from the antibodies, those infected or vaccinated develop T cell response as well, which help in eliminating the virus-infected cells. They also develop memory B cells, which can produce antibodies in event of a new infection. But it is not established that the immune memory can block viral reinfection. The cases of reinfection are occasional but may become more likely with the evolving SARS-CoV-2 mutations and variants which can escape immunity. Further, immunity being labile, may wane entirely after 6-8 months or a year or two.
The SARS-CoV-2 infection has spread around the world and may seem like an endemic disease. But, In the endemic phase of the disease, the number of infections should become relatively constant across years, with occasional outbreaks. Because the disease continues to increase in prevalence worldwide, and with various population groups in world regions being still susceptible, technically COVID-19 is in a pandemic phase [12]. It is being conjectured that to reach the steady state of endemicity for COVID-19 it may take a few years or even a decade.
Natural Infection, Vaccination and Herd Immunity
Depending on the way human populations develop immunity to the virus, will determine the course of the disease. Allowing the potentially dangerous SARS-CoV-2 virus to spread unimpeded may be the fastest way to develop herd immunity but that would result in millions of deaths world- wide. Further, for the SARS-CoV-2 virus, herd immunity may be a myth as the immunity ensuing natural infection is not a lasting immunity and may not prove to be a defensive immunity. Hence, the goal is to ensure a protective immunity in the human population through COVID-19 vaccination.
The countries that have begun vaccinating their population for COVID-19 are likely to witness a reduction in the severe manifestations, as seen in Israel [21]. But how effectively the vaccines can reduce the transmission of the virus will depend on various factors. There are data from clinical trials to suggest that vaccination may prevent symptomatic disease as well as transmission from a person to other. On an optimistic note, if the vaccines can prevent transmission and remain effective against the new variants as well, it may be possible to eliminate the virus in regions where enough people are vaccinated to protect those who are not, contributing to herd immunity. It is being speculated that a vaccine that is 90% effective at blocking transmission will need to reach at least 55% of the population to achieve temporary herd immunity as long as some social distancing, work from home and masking are followed. For a vaccine less effective than 90%, vaccine coverage should be greater to blunt the SARS-CoV-2 circulation.
Conclusion: Protecting from Covid-19
Control Measures/Non-Pharmacological Interventions
Various governments across the world have implemented a wide range of control measures and non-pharmacological Interventions (NPI) to mitigate the spread of SARS-CoV-2 virus. It may be important to understand and assess their relative effectiveness. The measures have included closing all educational institutions, limiting gatherings to 10 people or less, and closing face-to-face businesses have been effective in reducing transmission considerably. It has been found that the additional effect of stay-at-home orders was comparatively small. The ultimate goal of the NPI or control measures including partial or more extensive lockdown is to reduce the spread, prevalence, morbidity, and excess mortality of COVID-19.
Closing the nonessential face-to-face businesses was only somewhat more effective than targeted closures, which affected businesses with high infection risk, such as bars, restaurants, and clubs. Closing both schools and universities was found to have a robust effect. Several measures were associated with a clear reduction in the effective Reproduction Rate, Rt. Further, there is evidence that the control measures are effective at mitigating and suppressing outbreaks of COVID-19 [22].
Advances in Vaccine Technology and Pan Virus Vaccine
With the raging COVID-19 pandemic, there is required rapid genotyping and genomic sequencing capability to be applied in real-time to the positive samples for quick and effective utilization of the data. The large and most rapid deployment of COVID-19 vaccines under way should be equitable and needs a global effort. Most COVID-19 vaccines, including the Pfizer-Biotech and Modern vaccines are able to decrease symptomatic infection in real world. The studies indicate that the mass vaccination campaigns are helpful in reducing the burden of symptomatic disease. Further, with vaccination, there is appreciable reduction in the rate of serious illness. Still there is a continuing risk that the virus mutations and novel variants may in various ways render the existing COVID-19 vaccines less effective.
Some COVID-19 vaccine developers are looking at ways to develop next-generation vaccines that stimulate T cells more effectively. The S protein-based vaccines carry the risk that the S protein is fairly variable and prone to mutating, leading to their reduced efficacy. Whereas the antibodies detect only the S protein which decorates surface of the virus, the T cells can target viral proteins expressed inside infected cells, some of which are very stable. This raises the possibility of designing vaccines against proteins that mutate less frequently than the S protein and incorporating targets from multiple proteins into one vaccine.
The recent technological advances in biomedical, computing, and engineering sciences have ushered in a new era in antigen and vaccine discovery. Simultaneously, the technology has potential to accelerate identification of common antigenic targets shared across coronaviruses. Databases of genetic sequences of various coronaviruses can be used to model the evolutionary emergence of the viruses. Further, the on-going efforts to decode the principles of immunity in aging populations can enhance the effectiveness of vaccines for elderly. There is a possibility of developing a universal coronavirus vaccine, which is scientifically feasible [23]. There has been suggested an effort to put resources for developing ‘pan-virus vaccines’ that can provide immunisation against multiple strains of a virus. This is specially required in the context of SARS-CoV-2, which is mutating and evolving to more transmissible and virulent forms.
Probiotics as Adjuvant Therapy for COVID-19
It is indicated from various studies that the use of probiotics as adjuvant therapy may Improve the prognosis and clinical outcomes in COVID-19. During the in course of infection process, there is modulation of virus infectivity by the commensal microbiota of the host. In the regulation of viral infection, commensal microbiota It may promote viral infectivity by facilitating genetic recombination of viruses and enhance their infectivity and other diverse mechanisms. But microbiota can also exert substantial inhibitory effects on viral infection. In addition to fostering the generation of immune regulatory Trig cells, the commensal microbiota has antiviral effect by suppressing the activation of effector immune cells and by inhibiting the production of various inflammatory cytokines that are pivotal for virus elimination. In addition, the beneficial probiotic bacteria are demonstrated to promote the host defence and to improve immune response [24].
The SARS-CoV-2 infected patients are often administered antibiotics and antivirals, which could also result in gut microbial symbiosis. The use of probiotics, and their metabolites SCFAs (short-chain fatty acids), may reinforce innate and adaptive immunity in SARS-CoV-2 patients. Further, the administration of probiotics may increase anti-inflammatory cytokines, decrease pro inflammatory cytokines, improve antiviral antibody production, and reduce the viral load. The probiotics administration may help in reducing SARS-CoV-2 dissemination in the respiratory tract and gut, reinforcing both anti-inflammatory responses and immune defences, and thus can be an effective adjuvant strategy against the clinical complications [25].
References
-
Taubenberger JK, Morens DM (2006) 1918 Influenza: the mother of all pandemics. Emerg Infect Dis 12(1): 15-22.
-
Torjesen I (2021) Covid-19 will become endemic but with decreased potency over time, scientists believe. BMJ 372: n494.
-
Hogan AB, Jewell BL, Smith SE, Vesga JF, Owatso OJ, et al. (2020) Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: a modelling study. Lancet Glob Health 8(9): 1132-1141.
-
Dan JM, Mateus J, Kato Y, Hastie KM, Yu ED, et al. (2021) Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 371(6529): eabf4063.
-
Eguia R, Crawford KHD, Stevens-Ayers T, Millevolte LK, Greninger AL, et al. (2021) A human coronavirus evolves antigenically to escape antibody immunity. Preprint at bioRxiv 17(4): e1009453.
-
McCarthy KR, Rennick LJ, Nambulli S, Robinson LR, Bain WG, et al. (2021) Recurrent deletions in the SARS- CoV-2 spike glycoprotein drive antibody escape. Science 371(6534): 1139-1142.
-
Resende PC, Delatorre D, Graf T, Mir D, Motta CF, et al. (2021) Evolutionary Dynamics and Dissemination Pattern of the SARS-CoV-2 Lineage B.1.1.33 During the Early Pandemic Phase in Brazil. Front Microbiol 11: 615280.
-
Phillips N (2021) The coronavirus is here to stay - here’s what that means. Nature 590(7846): 382-384.
-
Cele S, Gazy I, Jackson L, Hwa HS, Tegally H, et al. (2021) Escape of SARS-CoV-2 501Y.V2 variants from neutralization by convalescent plasma. Preprint at medRxiv Preprint.
-
Garcia Beltran WF, Lam EC, Denis K, Garcia ZH, Blake M, et al. (2021) Circulating SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity. MedRxiv.
-
Wang Z, Schmidt F, Weisblum Y, Muecksch F, Barnes CO, et al. (2021) mRNA vaccine-elicited antibodies to SARS- CoV-2 and circulating variants. bioRxiv Preprint.
-
Lavine JS, Bjornstad ON, Antia R (2021) Immunological characteristics govern the transition of COVID-19 to endemicity. Science 371(6530): 741-745.
-
Shrotri M, Van Schalkwyk MCI, Post N, Eddy D, Huntley C, et al. (2021) T cell response to SARS-CoV-2 infection in humans: A systematic review. Plos One 16(1): e0245532.
-
Grifoni A, Weiskopf D, Ramirez SI, Mateus J, Dan JM, et al. (2020) Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals. Cell 181(7): 1489-1501.
-
Tarke A, Sidney J, Kidd CK, Dan JM, Ramirez, SI, et al. (2020) Comprehensive analysis of T cell immunodominance and immunoprevalence of SARS-CoV-2 epitopes in COVID-19 cases. Cell Rep Med.
-
Skelly DT, Harding AC, Gilbert Jaramillo J (2021) Vaccine- induced immunity provides more robust heterotypic immunity than natural infection to emerging SARS- CoV-2 variants of concern.
-
Hodcroft EB, Domman DB, Oguntuyo K, Diest M, Densmore KH, et al. (2021) Emergence in late 2020 of multiple lineages of SARS-CoV-2 Spike protein variants affecting amino acid position 677. medRxiv Preprint.
-
Stamatatos L, Czartoski J, Wan YH, Homad LJ, Rubin V, et al. (2021) Antibodies elicited by SARS-CoV-2 infection and boosted by vaccination neutralize an emerging variant and SARS-CoV-1. medRxiv Preprint.
-
Starr TN, Greaney AJ, Addetia A, Hannon WW, Choudhary WC, et al. (2021) Prospective mapping of viral mutations that escape antibodies used to treat COVID-19. Science 371(6531): 850-854.
-
Ledford H (2021) How ‘killer’ T cells could boost COVID immunity in face of new variants. Nature 590(7846): 374-375.
-
Rossman H, Shilo S, Meir T, Gorfine M, Uri Shalit, et al. (2021) Patterns of COVID-19 pandemic dynamics following deployment of a broad national immunization program. medRixv Preprint.
-
Brauner JM, Mindermann S, Sharma M, Johnston D, Salvatier J, et al. (2021) Inferring the effectiveness of government interventions against COVID-19. Science 371(6531): 9338.
-
Koff WC, Berkley SF (2021) Editorial - A universal coronavirus vaccine. Science 371: 6531.
-
Nikhra V (2020) The Trans-zoonotic Virome interface: Measures to balance control and treat epidemics. Ann Biomed Sci Eng 4: 20-27.
-
Santacroce L, Inchingolo F, Topi S, Del Prete R, Cosola MD, et al. (2021) Potential beneficial role of probiotics on the outcome of COVID-19 patients: An evolving perspective. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 15(1): 295-301.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions