First and Preliminary Data about Sars-CoV-2 Serology among Asymptomatic Workers in Central African Republic
Context and Objectives: The pandemic induced by Sars-CoV-2 has disrupted the organization of work while its extent is not known in CAR. The objective of this study was to estimate the Sars-CoV-2 seroprevalence in the workplace in the Central African Republic. Methods: This is a cross-sectional study that took place at the Department of Occupational Medicine in Bangui. Asymptomatic workers who request to the Occupational Physician a medical certificate and consented were included in the study. A standard sheet was used to collect socio-demographic, professional and biological data. The serology of Sars-CoV-2 was based on 2 rapid immunochromatographic tests for detection of IgM and IgG separately: Covid-19 IgM / IgG Rapid Test (Cypress Diagnostics, Belgium) and Standard Q Covid-19 IgM / IgG Duo (SD Biosensor, Korea). Results: The seroprevalence of Sars-CoV-2 was 18.6% (CI [14.7-22.6]) including 1% positivity of IgM only, 1.0% of positivity of both IgM and IgG and 16.6% of positivity IgG only. Women (p = 0.001), young workers (
Introduction
Two months after its occurrence in China in December 2019, the disease due to the 2nd Conoravirus responsible for the Severe Acute Respiratory Syndrome (SARS-COV-2, Coronavirus Disease 2019 or Covid-19) has spread throughout the world [1]. It is the 3rd disease caused by a coronavirus to shake the whole world, after Severe Acute Respiratory Syndrome (SARS) in 2002-2003 and Middle East Respiratory Syndrome (MERS) in 2012-2013. Covid-19 is causing a pandemic, declared a “public health emergency of international concern” by the World Health Organization [2]. As of December 23, 2021, there are 276.5 million confirmed cases of covid-19 worldwide, including 5.4 million deaths and a total of 8.7 billion doses of vaccine administered [3]. This disease has deeply affected families, societies and economies and the world of work, which is reorganized each time a worker, is found to be carrying the virus. However, it also unleashed the fastest and broadest response in history, marked by unprecedented scientific mobilization and a commitment to global solidarity.
Despite this international mobilization, the pandemic still presents many challenges, including that of diagnosis. Indeed, even if there is not yet a reference method for the detection of SARS-CoV-2, molecular methods such as RT-PCR are methods of choice for the diagnosis of Covid-19 [4, 5, 6]. It is expensive and gives the result in 24 hours. An alternative is the antigenic detection of the virus [4, 7]. But these 2 methods taken together cannot assess the extent of the disease, given the overwhelming majority of asymptomatic cases. The advent of the vaccine means that there are now 2 categories of people who may have anti-Sars-CoV-2 antibodies in their blood. Only serology can identify all categories of people who have had contact with the virus in any way and regardless of the body’s reaction.
This diagnostic challenge of estimating the extent of Covid-19 in the population is a crucial problem in the Central African Republic. It is a country with limited resources of approximately 5 million people which notified its first case of Covid-19 on March 14, 2020. From that date until December 24, 2021, 11,961 cases of Covid-19 have been confirmed, including 101 cumulative deaths [8]. Vaccination, initially planned for vulnerable people, is gradually being extended to the entire population and 453,282 doses of vaccine were administered as of December 15, 2021 [8]. Only 2 central laboratories located in Bangui routinely perform RT-PCR for the diagnosis of SARS-CoV-2, despite the availability of around twenty Genexpert® devices (Cepheid, Sunnyvlae, USA) in laboratories in the provinces, of which only 7 have been trained in performing the Covid-19 RT- PCR test. These laboratories are experiencing difficulties in supplying Genexpert® cartridge (Cepheid, Sunnyvlae, USA). Thus the existence of this technical platform in Bangui as in the provinces does not allow us to know the extent of the Covid-19 in the CAR. A study carried out with rapid diagnostic tests on sera from Central African Republic patients, collected before the year 2019 showed a significant proportion of probable false reactivity and suggests that a combination of tests could reduce the risk of false reactivity. The lack of human resources in health area and ignorance of the role of Labor medicine mean that many companies in the CAR do not have an occupational health safety structure and even less a Covid-19 screening system, as would have been the screening procedure for a Covid-19 infection in a structured African workplace [9]. The present investigation aims to determine the Sars-CoV-2 seroprevalence among workers requesting medical certificates from the Department of Occupational Medicine in Bangui.
Methods
This is a cross-sectional study that took place at the Department of Occupational Medicine (DOM). DOM is a public service responsible for promoting occupational health and safety through the prevention of occupational accidents and diseases. All workers in the public and private sectors are oriented towards DOM, requiring a medical opinion on occupational health and safety or a medical certificate. Included in the study was any asymptomatic worker requesting DOM for the issuance of a medical certificate, who had given informed and signed consent to participate in the study. The data were collected using a standardized sheet providing information on socio-demographic, occupational and immuno-microbiological variables (results of the SARS- CoV-2 serology). The data were collected by the occupational physician responsible for issuing the medical certificate; the tests were carried out by a Biomedical Analysis Engineer under the supervision of the Hospital Biologist, virologist who validated the results in 2 copies, one of which was given to the participant. Every worker who showed a positive result regardless of the class of immunoglobulin detected was isolated for 8 days at home and treated free of charge according to the national Covid-19 treatment protocol.
SARS-CoV-2 serology was based on 2 immunochromatographic tests allowing the qualitative detection of IgM and IgG separately on 2 different bands. The Covid-19 IgM/IgG Rapid Test (Cypress Diagnostics, Belgium)
is a test that has received the CE mark [10]; it detects antibodies specific for SARS-CoV-2 membrane antigens using a single cassette containing 2 strips impregnated with conjugates coupled to colloidal gold [11]. The Standard Q Covid-19 IgM / IgG Duo test (SD Biosensor, Korea), for its part, detects the same antibodies using 2 different cassettes, one for IgM and another for IgG [12]. This test has a sensitivity and specificity of 91.7% for IgM and 79.2% for IgG at 7 days after disease onset. These diagnostic performances are 100% for both IgM and IgG 9 days after the onset of the disease [13, 14]. In both cases, the deposition of capillary whole blood was followed by that of the migration buffer [13, 12]. The analyses were carried out according to the instructions of the manufacturers of the 2 tests used.
Workers who tested positive for SARS-CoV-2 were those in whom anti-Sars-CoV-2 (IgG and / or IgM) antibodies were detected in the blood. Recent exposure (between 3 and 6 days) to Sars-CoV-2 corresponded to the presence of IgM alone while long-standing exposure (> 8 days) resulted in the presence of IgG [15, 16]. The study protocol was approved by the Ethics and Scientific Committee of the Faculty of Health Sciences and the Pasteur Institute of Bangui, representing the National Ethics Committee of the CAR. The results were entered and analyzed using Epi-Info software, version 7 (WHO, Geneva & CDC, Atlanta). The proportions were estimated with a 95% confidence interval (95%CI). The difference was considered significant when the intervals of the 2 groups were not overlapping. Fisher’s exact test was used, with online software (https://biostatgv.sentiweb. fr/?module=tests/fisher), to compare the proportions of categories of qualitative variables with a significance level of 5%.
Results
During the study period, SARS-CoV-2 serology was offered to 105 workers, of whom 97, or 92.4% (8/107) gave their consent to participate in the study; the proportion of refusals was therefore 7.6%. There is no socio-demographic difference between the 8 who refused to participate in the study and the 97 who consented. Fifty (50) participants were men (52.0%), for a sex ratio (M / F) of 1.1. The average age of the workers was 34.3 years with extremes of 18 and 67 years; the most represented age group was under 40 with 76.3%. Eighty (82.5%) workers resided in Bangui and 81, or 83.5%, stated that they comply with the barrier measures against Sars-CoV-2 transmission (Table 1).
| Number | Percentage (%) | |
|---|---|---|
| Sex | ||
| Male | 50 | 50.0 |
| Female | 47 | 48.0 |
| Age (years) | ||
| <40 | 74 | 76.3 |
| 40-59 | 20 | 20.6 |
| ≥60 | 3 | 3.1 |
| Vaccinated | ||
| Yes | 43 | 44.3 |
| No | 54 | 55.7 |
| Origin | ||
| Bangui City | 80 | 82.5 |
| Suburb | 17 | 17.5 |
| Compliance with barrier measures | ||
| Yes | 81 | 83.5 |
| No | 16 | 16.5 |
Table 1: Socio-demographic characteristics of workers.
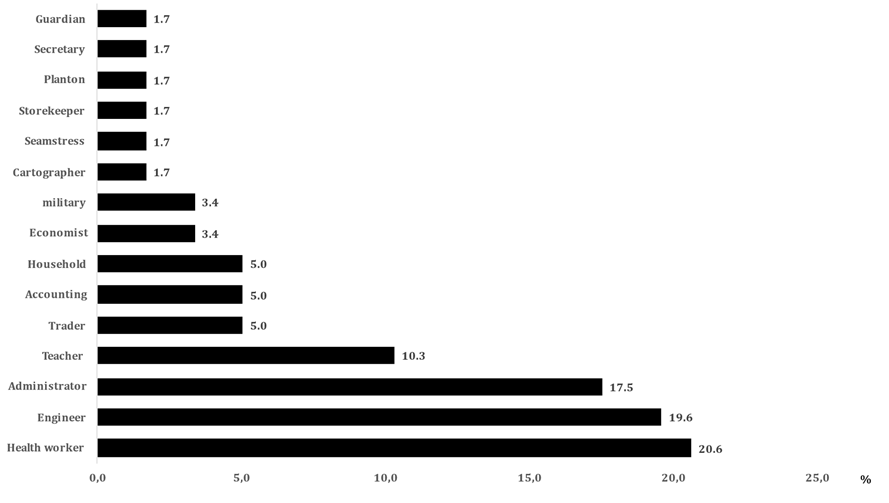
Regarding the profession, 4 socio-professional groups were the most represented with a cumulative frequency of 68.0%: health workers, engineers, administrators and teachers with a respective frequency of 20.6%, 19.6%, 17.5% and 10.3% (Figure 1).
The 2 tests used gave the same results in the same workers: 18 workers (18.6%; CI [14.7-22.6]) had a positive Sars-CoV-2 serology, including 1 with only IgM positivity (1.0%), 1 other (1.0%) a positivity of the 2 classes of Antibodies (IgM and IgG) and 16 with a positivity of IgG only (16.6%). The distribution of Sars-CoV-2 serology results according to the different characteristics showed that the women were more predominantly seropositive (p = 0.001); positive serology was more observed in young people (<40 years; p = 0.01); no difference was observed between vaccinated and unvaccinated. Compliance with barrier measures was significantly associated with a high prevalence of anti-Sars-CoV-2 antibodies (0.005). The inhabitants of Bangui were more seropositive than those of the suburbs (p = 0.05); positive serology was significantly more observed among theoretically highly exposed professions (health professionals, teachers and traders) than workers in other sectors of activity (p = 0.0003).
Discussion
We report here the first data relating to Sars-CoV-2 seroprevalence among workers in Bangui. The sex ratio (M / F) was 1.1; the average age of workers of 34.3 years; 44.3% were vaccinated against Sar-CoV-2, 82.5% of workers requesting medical certificates resided in Bangui and 83.5% claimed to respect the barrier measures against Sars-CoV-2 transmission (Table 1). The Sars-CoV-2 seroprevalence was 18.6% of which 2.0% carried IgM. Female sex (p = 0.001), young age (<40 years; p = 0.01), residence in Bangui (0.05), compliance with barrier measures, (0.005) and healthcare workers, teachers and traders were significantly (p = 0.0003) more associated with Sars-CoV-2 seropositivity (Table 2).
Sars-CoV-2 infection has caused great upheaval in the world of work. With the advent of the Sars-CoV-2 vaccine, it is becoming crucial to identify the professions most at risk in order to offer them vaccination as a priority. If the RT-PCR and the antigenic tests make it possible to detect the carriage of the virus, which is a very transient event, the serology makes it possible to identify the carriers of antibodies, whether they are vaccinated or not. They had contact with Sars-CoV-2 by any way. However, the study used rapid tests less efficient than the reference serological technique, the virus neutralization test, reserved for high- security reference laboratories (biosafety level 3). The risk of infection can be mitigated in this technique by using viral pseudo-particles carrying the spike protein of Sars-CoV-2 [17, 18]. But the limited resources of our country do not allow us to use such a technique because of their expensive costs. Our laboratories no longer use rapid tests to make the diagnosis. This limitation was compensated by using 2 tests to minimize the lack of reliability of each of the 2. The Standard Q Covid-19 IgM / IgG Duo test (SD Biosensor, Korea) has already shown good performance [13, 14]; it would confirm or not the performance of the Covid-19 IgM / IgG Rapid Test (Cypress Diagnostics, Belgium), both being used in the country without prior evaluation. The 2 tests used gave the same results in the same workers, indicated that the biological methodology is valid. Some information was obtained by interview and it is not possible to verify its veracity. So this is the real limitation of the study.
- Workers
- Sars-CoV-2 serology p-
- Characteristics
- Positive
- Négative
- Value
- Sex
- Male
- 5
- 54
- 0.001
- Female
- 13
- 25
- Age (years)
- <40
- 15
- 49
- 0.01
- 40-59
- 2
- 30
- ≥60
- 1
- 0
- Vaccinated
- Yes
- 10
- 40
- NS
- No
- 8
- 39
- Origin
- Bangui
- 12
- 68
- 0.05
- Suburb
- 6
- 11
- Compliance with barrier measures
- Oui
- 11
- 70
- 0.005
- Non
- 7
- 9
- Occupation
- Theoretically very exposed*
- 13
- 22
- 0.0003
- Theoretically less exposed#
- 5
- 57
Table 2: Percentage distribution of positive and negative serologies among workers according to their socio-demographic and
*The theoretically highly exposed professions are those which, in their activities, are in regular contact with many other people. These are healthcare workers, teachers and traders. They are grouped here with a total number of 35 workers.
#The theoretically low-exposure professions include the other socio-professional categories with a total nomber of 62 workers.
Despite this limitation, the seroprevalence of Sars-CoV-2 in our study was 18.6%. This seroprevalence is relatively comparable to the average of the seroprevalences of African countries which is 22.0% (15.0% -30.0%), obtained by Chisale in a metanalysis and review [19] and the average of the Sars-CoV-2 séroprevalence in West Africa. The Sars- CoV-2 seroprevalence in our serie is higher than the averages of the seroprevalences of the countries of East Africa on the one hand and those of North Africa on the other hand. Although our study was carried out during the vaccination campaign for healthcare workers, the elderly and those with co-morbidities, the Sars-CoV-2 seroprevalence observed is low compared to the average seroprevalence of studies carried out in Central Africa which is 41.0% (14.0-72.0%) [19]. The seroprevalence of Central African countries taken individually was 36.2% in Libreville in Gabon [20], 40.8% to 41.2% in Bukavu in Democratic Republic of Congo [16, 21]; 29.2% in urban districts in Cameroon [22] and 17.6% in Brazzaville in Congo [23]. The Sars-CoV-2 seroprevalence of our series is very close to that obtained by Batchi-Bouyou in Brazzaville in Congo, which used a methodology similar to ours. Its study was carried out in the general population and our study on asymptomatic workers in search of a medical certificate. Despite this difference, our two Sars-CoV-2 seroprevalences are very close: 17.6% in Brazzaville [23] and 18.6% in Bangui. On the other hand, the studies carried out in Central Africa which showed Sars-CoV-2 seroprevalences higher than ours, used study populations which seem to be more at risk of Covid-19: the patients coming to carry out the laboratory examinations in Gabon [20] , healthcare workers in the DRC [21], travelers and workers seeking medical certificates in the DRC [16], except the study made by Nwosu in Cameroon in the general population [22] . These studies show that the Sars-CoV-2 seroprevalence is higher in Central Africa [16, 20, 21, 22] particularly and that it increases over time with the duration of circulation of Sars-CoV-2 in a population [19].
Our study identified 4 main factors associated with a positive Sars-CoV-2 serology: age under 40 years (p = 0.01), female sex (p = 0.01), residence in the city (Bangui) (p = 0.005) and professions in regular contact with the population (p = 0.0003). The association between young age and a positive Sars-CoV-2 serology has also been noted by other authors [19, 24]. This association would be linked to the fact that the high media coverage of the Covid-19 pandemic which, as a general rule, is benign among young people, the relatively low morbidity and mortality of Covid-19 in the CAR, the lack of objectivity in the behavior of some responsible for the fight against Covid-19 and false information conveyed by social networks have largely contributed to the non-application of preventive measures of Covid-19 by young people. At the start of the epidemic in CAR in March 2020, health authorities claimed that masks were only for the sick. Hence the difficulty of acceptability of the mask in young people. This could explain the fact that young people (<40 years old) were more Sars-CoV-2 seropositive than those over 40 years old. Along with age, female gender was also associated with positive Sars-CoV-2 serology (p = 0.001). This female predominance has been observed in a meta-analysis on African studies [19] while some studies have found a high Sars-CoV-2 seroprevalence among men [25]. However, a pooled analysis of meta‐analyzes carried out with a global representation of the data, showed that the difference is not statistically significant [26]. Relative gender differences are also confirmed by the absence of a gender factor in the WHO and Africa CDC reports [7, 27].
Living in an urban area was also associated with positive Sars-CoV-2 serology (p = 0.005). This result confirms those obtained in the State of Niger in Nigeria [28]. This more pronounced attack in urban areas should be linked to the density of the population with frequent meetings of people in closed environments, in particular for professional reasons. This also should explain the high prevalence (p = 0.0003) of anti-Sars-CoV-2 antibodies among people whose work requires meeting others (teachers, healthcare professionals, traders), noted in our study. This observation has already been reported by numerous studies, in particular those carried out in Central Africa [19, 21]. On the other hand, another study in the DRC showed that few healthcare workers had anti-Sars-CoV-2 antibodies than other workers [16]. On the one hand, the more frequent attack of healthcare professionals by Sars-CoV-2 is linked to their activities which consist of caring for the sick. During the Covid-19 period, most of the activities of healthcare professionals come down to taking care of patients with Covid-19. Overwork and fatigue are factors favoring accidents, especially in the workplace, would explain the high Sars-CoV-2 seroprevalence among healthcare professionals. On the other hand, however, healthcare workers familiar with the virus and the disease would be the people who theoretically would protect themselves better against transmission of the virus. In the specific Central African Republic context, protective equipments (in particular masks) were not provided to healthcare professionals until one of them tested positive for Sars-CoV-2 by PCR when he was attending a meeting, while presenting a symptomatology very suggestive of Covid-19. In all cases, these data suggest an active screening strategy for Sars-CoV-2 in the occupational groups most at risk [29].
Conclusion
The Sars-CoV-2 seroprevalence in the workplace in CAR is 18.6%. This Sars-CoV-2 seroprevalence remains low despite the introduction of vaccination against Sars-CoV-2 which is gradually spreading in CAR with 44.3% of workers vaccinated. The Sars-CoV-2 seroprevalence is significantly higher among healthcare professionals, teachers and traders. These workers are therefore among the most exposed occupations in the CAR which must be the subject of close surveillance or even priority vaccination. Further studies should be carried out to understand the acceptability of vaccination and the kinetics of antibodies following vaccination in CAR.
References
-
Davenne E, Giot JB, Huynen P (2020) Coronavirus et COVID-19 : le point sur une pandémie galopante. Rev Med Liege 75(4): 218-225.
-
Samhouri D, Barry J, Mahrous H, Mahgoub F, El Gohary P, et al. (2021) COVID-19 threat perception: public health emergency of international concern versus pandemic. Wkly Epidemiol Rec 27: 20-24.
-
WHO (2021) WHO Coronavirus (COVID-19) Dashboard.
-
Safiabadi Tali SH, LeBlanc JJ, Sadiq Z, Oyewunmi OD, Camargo C, et al. (2021) Tools and Techniques for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS- CoV-2)/COVID-19 Detection. Clin Microbiol Rev 34(3): e00228-20.
-
Carter LJ, Garner LV, Smoot JW, Li Y, Zhou Q, et al. (2020) Assay techniques and test development for COVID-19 diagnosis. ACS Cent Sci 6(5): 591-605.
-
Corman VM, Landt O, Kaiser M, Molenkamp R, Meijer A, et al. (2020) Detection of 2019 novel coronavirus (2019- nCoV) by real-time RT-PCR. Euro Surveill 25: 2000045.
-
WHO (2020) Strategic response plan for the World Health Oragnisiation African Region. World Health Organization. African regional website 2020: 1-10.
-
WHO (2021) Central African Republic WHO Coronavirus (Covid-19) Dashbord.
-
Ndiaye M, Diatta AER (2020) Procédure de dépistage d’une infection à Covid-19 en milieu de travail structuré Africain. Arch des Mal Prof et de l’Environnement 81(4): 337-340.
-
Federal Agency for Medicines and Health Products of Begium (2021) List of recommended SARS-CoV-2 antibody and antigen tests.
-
Cypress Diagnostics (2020) Covid-19 IgM/IgG Rapid Test (product insert).
-
SD Biosensor Laboratories (2020) STANDARD Q_ COVID-19 IgM IgG Duo (product insert).
-
Zainol Rashid Z, Othman SN, Abdul Samat MN, Ali UK, Wong KK, et al. (2020) Diagnostic performance of COVID-19 serology assays. Malays J Pathol 42(1): 13-21.
-
Department Health and Human Services of USA (2021) Serology Test Evaluation Report for “STANDARD Q COVID-19 IgM/IgG Duo” from SD BIOSENSOR, Inc. 12p.
-
Lee HK, Lee BH, Seok SH, Baek MW, Lee HY, et al. (2010) Production of specific antibodies against SARS-coronavirus nucleocapsid protein without cross reactivity with human coronaviruses 229E and OC43. J Vet Sci 11(2): 165-167.
-
Bianga Katchunga P, Murhula A, Akilimali P, Zaluka JC, Karhikalembu C, et al. (2021) Séroprévalence des anticorps anti SARS‐Cov‐2 parmi les voyageurs et travailleurs dépistés à la clinique Saint Luc de Bukavu, à l´Est de la République Démocratique du Congo, de mai en août 2020. Pan Afr Med 38:93.
-
Hantz S (2020) Diagnostic biologique de l’infection à Sars-CoV-2 : stratégies et interprétation des résultats. RFL 526 : 48-56.
-
Grangeot-Keros L (2020) Intérêt et limites de la sérologie covid-19 chez l’homme. Bull. Acad Vét France pp : 89-91.
-
Chisale MRO, Ramazanu S, Mwale SE, Kumwenda P, Chipeta M, et al. (2021) Seroprevalence of anti‐SARS‐ CoV‐2 antibodies in Africa: A systematic review and meta‐analysis. Rev Med Virol 6: e2271.
-
Mveang Nzoghe A, Leboueny M, Kuissi Kamgaing E, Maloupazoa Siawaya AC, Bongho EC, et al. (2021) Circulating anti‐SARSCoV‐2 nucleocapsid (N)‐protein antibodies and anti‐SARS‐CoV‐2 spike (S)‐protein antibodies in an African setting: herd immunity, not there yet. BMC Res Notes 14(1): 152.
-
Mukwege D, Byabene AK, Akonkwa EM, Dahma H, Dauby N, et al. (2021) High SARS-CoV-2 Seroprevalence in Healthcare Workers in Bukavu, Eastern Democratic Republic of Congo. Am J Trop Med Hyg 104(4): 1526- 1530.
-
Nwosu K, Fokam J, Wanda F, Mama L, Orel E, et al. (2021) SARS-CoV-2 antibody seroprevalence and associated risk factors in an urban district in Cameroon. Nat Commun 12(1): 5851.
-
Batchi-Bouyou AL, Lobaloba Ingoba L, Ndounga M, Vouvoungui JC, Mfoutou Mapanguy CC, et al. (2021) High SARS-CoV-2 IgG/IGM seroprevalence in asymptomatic Congolese in Brazzaville, the Republic of Congo. Int J Infect Dis 106: 3-7.
-
Olayanju O, Bamidele O, Edem F, Eseile B, Amoo A, et al. (2021) SARS‐CoV‐2 seropositivity in asymptomatic frontline health workers in Ibadan, Nigeria. Am J Trop Med Hyg 104(1): 91-94.
-
Lai CC, Wang JH, Hsueh PR (2020) Population‐based seroprevalence surveys of anti‐SARS‐CoV‐2 antibody: an up‐to‐date review. Int J Infect Dis 101: 314-322.
-
Rostami A, Sepidarkish M, Leeflang MMG, Riahi SM, Nourollahpour Shiadeh M, et al. (2020) SARS‐CoV‐2 seroprevalence worldwide: a systematic review and meta-analysis. Clin Microbiol Infect 27(3): 331-340.
-
Africa CDC (2021) Outbreak Brief # 57: coronavirus disease 2019 (Covid‐19) pandemic.
-
Majiya H, Aliyu-Paiko M, Balogu VT, Musa DA, Salihu IM, et al. (2020) Seroprevalence of SARS-CoV-2 in Niger State: A Pilot Cross Sectional Study. Preprint 6: 1-23.
-
Campbell JR, Uppal A, Oxlade O, Fregonese F, Bastos ML, et al. (2020) Active Screening in Groups at Increased Risk of SARS-CoV-2 in Canada: Costs and Human Resources Needed. CMAJ 192(40): E1146-E1155.
-
World Health Organization (2020) Antigen-detection in the diagnosis of SARS-CoV-2 infection using rapid immunoassays interim guidance, 11 September 2020. World Health Organization, Geneva, Switzerland.
-
Thabet L, Mhalla S, Naija H, Jaoua MA, Hannachi N, et al. (2020) Diagnostic virologique de l’infection par le Sars- CoV-2. Tunis Med 98(4): 304-308.
-
Ministry of Health and Population of the Central African Republic (2021) SITREP Epidemiological situation as of December 23, 2021Ministry of Health and Population, Bangui, Central African Republic, pp:1.
-
Mboumba Bouassa RS, Péré H, Tonen-Wolyec S, Longo JD, Moussa S, et al. (2020) Unexpected high frequency of unspecific reactivities by testing pre‐epidemic blood specimens from Europe and Africa with SARS‐CoV‐2 IgG– IgM antibody rapid tests points to IgM. as the Achilles heel. J Med Virol 93(4): 2196-2203.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions