Prevalence of Anti-Human Papillomavirus IgG Antibody among Students of a Private Tertiary Institution in Ado-Ekiti, Nigeria
Background: Human Papillomavirus (HPV) is an oncogenic sexually transmitted virus. It is the leading cause of cervical cancer, penile, vulva, vaginal and anal high-grade dysplasia. Infections are usually asymptomatic only to manifest after several years, implying that most adults with symptoms must have been infected at their young ages. The risky sexual behavior of subjects at ages 16-24 makes then vulnerable. Objectives: This study evaluates the prevalence of anti-human Papillomavirus IgG antibody among students of a tertiary institution in Ado-Ekiti, Nigeria. Methods: One hundred and fifty (150) blood samples were collected from consenting students (100 females and 50 males) age 16-24 in Ado-Ekiti. A structured questionnaire was administered concurrently. Sera were assayed using the anti-HPV-IgG antibody ELISA Kit (Melsin Medical Co. Limited). Data was analyzed using Epi-Info 7.2 Version Software and Excel. Ethical approval was obtained for the study. Results: Sixty eight (45%) of the total subjects were seropositive for anti-HPV-IgG antibody. Twenty six (52%) males and 42 (41%) females were seropositive. There was no significant difference (p>0.05) in seropositivity across the ages and among the gender. Fifty nine (60%) of sexually active subjects were seropositive for anti-HPV-IgG antibody (p˂0.05). Thirty five (97%) non-condom users were seropositive (p<0.05) while fifty four (75%) of subjects who have had unprotected sex at one point in their lives were seropositive (p< 0.05). Only three of the subjects had been vaccinated. Conclusion: The high rate of seropositivity to anti-HPV-IgG antibody in the population is a cardinal pointer to high rate of exposure to HPV and a likely exposure to the high-risk serotype.
Introduction
Human parpillomavirus (HPV) is a non-enveloped DNA
virus belonging to the papillomaviridae family which has over 170 types known for ability to infect man especially the mucosal areas of the anogenital region and upper digestive tract [1, 2, 3, 4, 5]. The virus is highly diverse, infecting mostly humans, mammals and bird [6]. Over 40 types are known to be transmitted via sexual contacts, infecting penile skin, vulva linings, cervix and rectum of both male and females [7, 8, 9, 10]. It ranks high among common sexually transmitted infections amounting to about 14 million new cases yearly. An estimated 50% of sexually active adults are said to have had a genital HPV and at least 75% of individuals globally will at least at one time or the other in a life time have a genital HPV infection, making genital HPV one of the most common sexually transmitted infection among adolescents and young women [5, 11, 12]. In Nigeria, the highest prevalence has been reported to be among female aged 15-23 years [13].
The virus is oncogenic causing anogenital and oropharyngeal cancers and hyperplasia. Globally, an estimated 2 million of all new cancer cases per annum are attributable to infections with the developing countries having a significantly high proportion of about 32.7% [14]. HPV attributable cancers are the second most common infection-related cancers globally only second to Helicobacter pylori [15]. Globally 630 million people are estimated to be infected compared with 40 million in the case of HIV. Some authors have unequivocally linked ≥95% of cervical cancer cases and about 88% of anal cancer with HPV infection. More recently, there have been records of HPV-relevant head and neck cancers [15, 16]. HPV infections often go asymptomatic and remain dormant for years gradually transforming cells of infection locations. Types 6, 11, 16 and 18 are the leading cause of infections. The genotypes are generally classified into the “high risk” and “low risk” groups. Infection with the high risk group is generally associated with the development of cervical cancer, mucosal anogenital and other head and neck cancers [7, 8]. While the low risk groups are more associated with benign or low grade cervical tissue changes as well as genital warts [10, 17, 18, 19].
Over the years, there has been a worrisome increasing trend of risky sexual behavior (RSB) among adolescence especially among those in tertiary institutions who are just beginning to gain liberty from their parent protection especially because they now stay away from home. They want to try new things like sex, and drugs and many get trapped in there. Risky Sexual behaviors has become a concern to the Center for disease control and is define as those practices that exposes an individual to unintended pregnancy and sexually transmitted diseases. These includes multiple sexual partners, anal sex, exposure of adolescence under 18 year to sex, having sex without condom or other contraceptives, sexual activities done under the influence of alcohol or other drugs, sexual violence and translational sex [20, 21]. Since HPV is one of most encountered sexually transmitted infections likely to be contracted within the early years of initiation to sex, it is worrisome that the world may be sitting on a time bomb of cancer epidemic which is of grave socioeconomic impact on the global community, thus the need to evaluate the actual extent of spread especially among tertiary institution students who are the future of the world.
To the best of our knowledge, no work has been done to assess the sero-prevalence of HPV infection among undergraduate students of Afe Babalola University, Ado- Ekiti, Ekiti State. Scarcity of information in this regard, therefore necessitates this study. The aim of this study is therefore to evaluate the prevalence of anti-human Papillomavirus IgG antibody among students of Afe Babalola University, Ado-Ekiti, Ekiti State, Nigeria.
Materials and Methods
Study Area and Population
This study was carried out among students in a higher institution of learning in Ado-Ekiti. This city is in Ekiti State, Latitude 70351 and 70381 north of the equator and Longitude 50101 and 50151 east of the Greenwich Meridian [22]. The University is a privately owned institution and operates a strict boarding enclosed system where students are hardly allowed to go out of school premises except at vacation. One hundred and fifty three (153) consenting students (103 females and 50 males) between ages 16-24 were randomly enrolled into this study (n = 150). Three female subjects with history of HPV vaccination were excluded from the study. Ethical approval was obtained from the research and ethics review committee of the institution under study. Participants were duly informed of the purpose of the study and written consent was obtained from each of them.
Questionnaire
A structured questionnaire was confidentially administered to obtain information on vaccination status, basic socio-demographic data and information on sexual behaviours such as use of condom, sexually activity and number of sex partners.
Sample Collection and Serological Analysis
Three millilitres (3ml) of venous blood sample was aseptically collected from each unvaccinated participant. The blood was allowed to clot and serum separated by centrifugation at 3000rpm and 25oC for 5 minutes in an Eppendorf tube. Serum samples were stored at -20℃ until ready for analysis. Analysis of serum samples were carried out at the Medical Laboratory of Afe Babalola University using ELISA technique for detection of human papillomavirus IgG antibodies. Pre-coated HPV ELISA kits were purchased from Melsin medical co. Limited (CAT NO; EKHU-0731; LOT NO; M20180428) and analysis was carried out in accordance with the manufacturer protocol and instructions. Briefly, reagents provided were allowed to attain room temperature for 15 minutes before use. The 40X wash buffer was diluted with distilled water using a ratio of 1:40 before use. The micro-titer plate template was set up with 1 well as blank, 2 wells as negative control and 2 wells as the positive control. Ten microlitres (10µl) of sera sample and 90µl sample diluent were dispensed into the respective wells except for the blank well, negative control well and positive control well. One hundred microlitres (100µl) of the negative and positive controls were dispensed into their wells respectively. The content was mixed by vibrating the plate gently. The microplate was covered with a sealing paper and incubated in a microplate incubator (MARVOTECH PLATE INCUBATOR, CHINA) at 37℃ for 60 minutes [23]. After incubation, the microplate was washed five times using wash buffer. 100 µl of Horseradish peroxidase enzyme (HRP) conjugate was added to each well except the blank; the microplate was covered with a sealing paper and also incubated in a microplate incubator at 37℃ for 15 minutes. After incubation, the microplate was washed five times with the diluted wash buffer in an automatic plate washer (MARVOTECH PLATE WASHER, China). Fifty microlitres (50µl) of substrate solution A and B were added to each well respectively and were mixed; the plate was covered and incubated at 37℃ for 15 minutes. Fifty microlitres (50µl) of stop solution was added to each well and mixed. The absorbance was read in an ELISA reader machine (MARVOTECH ELISA READER, China) at a wavelength of 450 nm.
Results
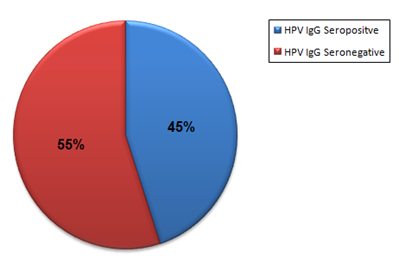
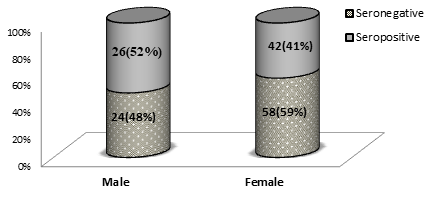
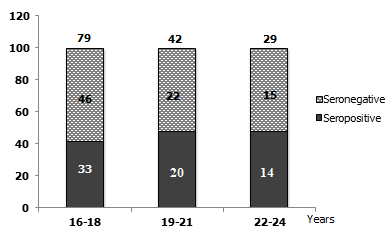
The percentage occurrence of anti-HPV-IgG antibody among the study participants is presented using a pie chart (Figure 1). Sixty eight (45%) out of the 150 participants examined were seropositive for anti-HPV-IgG antibody. Percentage occurrence of anti-HPV IgG antibody based on the gender distribution of the study participants is presented in Figure 2. Anti-HPV IgG antibody seropositivity was found to be higher among the male subjects (52%) than the females (41%), though not statistically significance (p=0.67) at 95 % confidence interval. Similarly, the percentage occurrence of anti-HPV IgG antibody based on the age range of the study participants (Figure 3) was not statistically significant (p=0.81). Seropositivity for anti-HPV IgG antibody was slightly higher among ages 19–21 years (48%) and 22-24 years (48%) than that observed among ages 16-18 years (42%).
Furthermore, a significant proportion (p<0.01) of the anti-HPV-IgG antibody seropositive subject (59/68) were sexually active, while a few individuals (9/68) claimed not to be sexually active but were seropositive (Table 1). Subject who practiced risky sexual behaviours such as having unprotected sex and multiple sex partners had higher and significant positivity rate (p<0.01) at 95% confidence interval. Sixty five precent (65%) of subject in this study was sexually active and 60% of these sexually active subjects were seropositive for anti-HPV-IgG antibody. Seventy percent (35/50) of male were sexually active while 63% (63/100) of females were sexually active. Of the entire population approached during sample collection, only three (3/153) indicated that they have been vaccinated against HPV, therefore were excluded from the study.
HPV Positive HPV Negative Total n 2 χ Odds ratio 95%CI p-Value Sexually active individuals Yes 59(39%) 39(26%) 98(65%) 150 24.1 6.93 57.74-72.91 0.001 No 9(6%) 43(29%) 52(35%) 7.03-11.45 Ever had unprotected sexual intercourse Yes 54(55%) 18(18%) 72(73%) 98 28.1 0.04 50.76-59.12 0.01 No 4(4%) 22(23%) 26(27%) 1.13-7.29 Have multiple sex partner Yes 36(37%) 6(6%) 42(43%) 98 5.07 3.15 30.47-40.33 0.02 No 22(22%) 34(35%) 56(57%) 17.97-28.11 Regularly use condom Yes 23(23%) 39(40%) 62(63%) 98 17.7 0.03 17.17-28.99 0.01 No 35(36%) 1(1%) 36(37%) 30.36-39.28
- Statistical Analysis
- Questionnaires were managed and analysed using the
- Epi-Info Version 7.2 Software. A chi-square and frequency distribution analysis and 95% confidence interval (95%CI) was determined.
Table 1: Percentage occurrence of anti-HPV IgG antibody based on the sexual behaviours of the study participants.
Discussion
In this present study, a high prevalence of anti-HPV-IgG antibody was observed among unvaccinated students of Afe Babalola University. It indicates that no less than 45% of the study population has possibly had an HPV infection at one point of their life or the other. A high frequency of HPV infection is a worrisome, indicating a possible rise in the incidence of cancer especially cervical and oropharyngeal cancers in the nearest future. The concern becomes more pressing when the sexual behaviors of the subjects are considered. First, the institution is strictly a boarding institution and the students get to relate and change friends over the duration of their stay. New and younger students also join the population yearly and also relate. Naïve young ones are also likely to learn risky sexual behaviors of older student as they relate with them. This presents a likelihood of a generational spread and a rising prevalence. These can be observed from the result as the younger students had a lower seroprevalence (though very marginal and not statistically significant) than the older students. This marginal difference may be attributed to the fact that this study was conducted at the latter part of the session when the new students had spent no less than six months in the school. It is possible that the prevalence could be lower at entry point.
The seroprevalence recorded in this present study is a little higher than that reported by Aminu et al., who reported a 33.3% for ages between 15-19 and 41.4% for ages 20- 24 [23]. In the present study, the subjects were apparently healthy, not having any cause to go to the clinic but in Aminu’s study, subjects were attending a clinic which may be a natural method of selecting sick persons especially in developing countries where people pay very little attention to routine medical checkup.
It was observed that a greater proportion of subjects were sexually active and as much as 73% of these sexually active individuals have had unprotected sex at one point or the other. A higher percentage of seropositive subjects were male students, likewise the higher percentage of those sexually active were male. This is also a great risk for the female students since the infected males are likely to act as vehicles for the spread of the virus. Liu et al., had earlier observed that it seems HPV infections is rapidly acquired more than a doubling rate within the first 5-10yrs of sexual activity; from 16.2% in 14-19years old female to 44.6% in 20-29 year old females [24, 25]. In the present study we have even a higher prevalence at ages between 16-19years. This may be attributed to the fact that more individuals seems to be accessing HPV vaccine (57.3%) in the US were the survey was carried out as against the less than 5% who were removed from the study because they have been vaccinated against HPV. This situation is likely to be compounded because there is available a couple of prophylactic vaccines against HPV, but people seem not to be accessing it and greater emphasis seems to be laid on vaccinating the female child against HPV compared to the male while we recorded higher prevalence among the males.
Limitation
The limitation of this study was that serotyping of the HPV to determine whether it was the high risk or low risk strains that were more prevalent in the population was not considered.
Conclusion
We recorded a high seroprevalence of anti-HPV IgG antibody among students in the higher institution. This is a signal of rise in risk of cervical and other oropharyngeal cancers and hyperplasia in the nearest feature. The risky sexual practice among these young students is likely to promote a geometric rise in the prevalence. They male seem to be more affected and are likely vehicles for the spread among the females.
What is Already known on this Topic
- The prevalence of anti-HPV IgG antibody among women presenting at reproductive health clinic of a hospital in Nigeria have been reported as 42.9%.
- It’s also known that seroprevalence varies with sociodemographic factors.
- Records are scanty on the prevalence of anti-HPV IgG antibody among tertiary institution students.
What this Study Adds
- The prevalence of anti-HPV IgG antibody among apparently healthy students of a private tertiary institution in Ado-Ekiti, Nigeria was observed to be 45%.
- Seropositivity was found to be higher among the male subjects (52%) than among the females (41%).
- Seropositivity to anti-HPV IgG antibody was significantly related to sexual behaviors.
Competing Interests
The authors declare that there is no competing interest.
Authors’ Contributions
All listed authors contributed significantly to this study and their contributions are as follows; Richard Yomi Akele conceptualized the study, developed the original proposal; participated in the sample analysis and wrote the initial draft of the manuscript. Chinyere Glory Amaechi obtained the ethical permission for the study, developed the questionnaire and administered it, collected the samples and participated in the laboratory analysis and entered data. Benard Oluwapelumi Oluboyo revised and corrected the initial proposal, revised and modified manuscript, participated in laboratory analysis. Janet Funmilayo Akinseye, Seyi Samson Enitan and Michael Olugbamila Dada made valuable contribution in the design of original concept and questionnaire. All authors modified and approved the final manuscript.
Acknowledgments
We acknowledge the cooperation of all the students who took part in the study.
References
-
Touzé A, de Sanjosé S, Coursaget P, Almirall MR, Palacio V, et al. (2001) Prevalence of Anti-Human Papillomavirus Type 16, 18, 31, and 58 Virus-Like Particles in Women in the General Population and in Prostitutes. J Clin Microbiol 39(12): 4344-4348.
-
Ma GX, Wang MQ, Ma XS, Shive SE, Tan Y, et al. (2013) Pathways of cervical cancer screening among Chinese women. Int J Womens Health 5: 351-359.
-
Frazer IH (2010) Measuring serum antibody to human papillomavirus following infection or vaccination. Gynecol Oncol 118(1): S8-S11.
-
Magaji SJ, Aminu M, Inabo HI, Oguntayo AO (2019) Spectrum of High Risk Human Papillomavirus Types in Women in Kaduna State, Nigeria. Ann Afr Med 18(1): 30- 35.
-
Richardson H, Kelsall G, Tellier P, Voyer H, Abrahamowicz M, et al. (2003) The Natural History of Type-specific Human Papillomavirus Infections in Female University Students. Cancer Epidemiol Biomarkers Prev 12(6): 485-490.
-
Bzhalava D, Guan P, Franceschi S, Dillner J, Clifford G, et al. (2013) A systematic review of the prevalence of mucosal and cutaneous human papillomavirus types. Virology 445(1-2): 224-231.
-
Bosch FX, Manos MM, Muñoz N, Sherman M, Jansen AM, et al. (1995) Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. International biological study on cervical cancer (IBSCC) Study Group. J Natl Cancer Inst 87(11): 796-802.
-
Chew GK, Cruickshank ME, Rooney PH, Miller ID, Parkin DE, et al. (2005) Human papillomavirus 16 infection in adenocarcinoma of the cervix. Br J Cancer 93(11): 1301- 1304.
-
Prati B, Marangoni B, Boccardo E (2018) Human papillomavirus and genome instability: from productive infection to cancer. Clinics 73: e539s.
-
Centers for Disease Control and Prevention (2018) Genital HPV Infection – CDC Fact Sheet 2012.
-
Di Giuseppe G, Abbate R, Liguori G, Albano L, Angelillo IF, et al. (2008) Human papillomavirus and vaccination: knowledge, attitudes, and behavioural intention in adolescents and young women in Italy. Br J Cancer 99(2): 225-229.
-
Trim K, Nagji N, Elit L, Roy K (2012) Parental Knowledge, Attitudes, and Behaviours towards Human Papillomavirus Vaccination for Their Children: A Systematic Review from 2001 to 2011. Obstet Gynecol Int 2012: 921236.
-
Ezenwa BN, Balogun MR, Okafor IP (2013) Mothers’ human papilloma virus knowledge and willingness to vaccinate their adolescent daughters in Lagos, Nigeria. Int J Womens Health 5: 371-377.
-
Plummer M, de Martel C, Vignat J, Ferlay J, Bray F, et al. (2016) Global burden of cancers attributable to infections in 2012: a synthetic analysis. Lancet Glob Health 4(9): e609-616.
-
Odutola M, Jedy-Agba EE, Dareng EO, Oga EA, Igbinoba F, et al. (2016) Burden of Cancers Attributable to Infectious Agents in Nigeria: 2012–2014. Front Oncol 6: 216.
-
Gillison ML, Chaturvedi AK, Anderson WF, Fakhry C (2015) Epidemiology of Human Papillomavirus–Positive Head and Neck Squamous Cell Carcinoma. J Clin Oncol 33(29): 3235-3242.
-
Palefsky JM (2010) Human Papillomavirus-Related Disease in Men: Not Just a Women’s Issue. J Adolesc Health 46: S12-19.
-
LaMontagne DS, Barge S, Le NT, Mugisha E, Penny ME, et al. (2011) Human papillomavirus vaccine delivery strategies that achieved high coverage in low- and middle-income countries. Bull World Health Organ 89(11): 821-830B.
-
Degarege A, Krupp K, Srinivas V, Ibrahimou B, Marlow LAV, et al. (2018) Determinants of attitudes and beliefs toward human papillomavirus infection, cervical cancer and human papillomavirus vaccine among parents of adolescent girls in Mysore, India. J Obstet Gynaecol Res 44(11): 2091-2100.
-
Madise N, Zulu E, Ciera J (2007) Is Poverty a Driver for Risky Sexual Behaviour? Evidence from National Surveys of Adolescents in Four African Countries. Afr J Reprod Health 11(3): 83-98.
-
Abels MD, Blignaut RJ (2011) Sexual-risk behaviour among sexually active first-year students at the University of the Western Cape, South Africa. Afr J AIDS Res 10(3): 255-261.
-
Adebayo WO, Jegede OA (2010) The Environmental Impact of Flooding on Transportation Land Use in Benin City, Nigeria. Afr Res Rev 4(1).
-
Aminu M, Gwafan J, Inabo H, Oguntayo A, Ella E, et al. (2014) Seroprevalence of human papillomavirus immunoglobulin G antibodies among women presenting at the reproductive health clinic of a university teaching hospital in Nigeria. Int J Womens Health 6: 479-487.
-
Liu G, Hariri S, Bradley H, Gottlieb SL, Leichliter JS, et al. (2015) Trends and patterns of sexual behaviors among adolescents and adults aged 14 to 59 years, United States. Sex Transm Dis 42(1): 20-26.
-
Zhu B, Liu Y, Zuo T, Cui X, Li M, et al. (2019) The prevalence, trends, and geographical distribution of human papillomavirus infection in China: The pooled analysis of 1.7 million women. Cancer Med 8(11): 5373- 5385.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions