Global and Local Upsurge in Monkey pox Epidemic: Current Trends, Challenges and Future Prospects
Amidst global relaxation of the Coronavirus Disease 2019 (COVID-19) intervention measures and celebration of the unprecedented grounds conquered in the fight against the pandemic, the monkeypox virus (MPXV) has emerged and remerged in many countries taking over major headlines around the globe at the present. Since 1 January and as of 22 June 2022, 50 nations and territories in five WHO Regions (Africa, America, Eastern Mediterranean, Europe, and Western Pacific) have reported 3413 laboratory-confirmed cases; along with one fatality. The Nigeria Centre for Disease Control (NCDC) received notice of a possible monkeypox epidemic in Bayelsa State on September 22, 2017. Thereafter, from Bayelsa to Rivers, Ekiti, Akwa Ibom, Lagos, Ogun and Cross River, the scourge of Monkeypox has continue to escalate five (5) years after the disease was first reported in Nigeria. An aggregate of 716 suspected cases have been recorded from 25 states nationwide between September 2017 and June 26, 2022. There have been 288 (40.2 percent) confirmed cases from 25 states out of the 716 suspected cases. So far, nine (9) deaths in total (CFR=3.1%) have been reported in 6 states between September 2017 and June 2022. At the moment, the following challenges are preventing the country from containing the virus effectively: 1) Low patient use of healthcare facilities because of stigma, cost, and low fatality rate; 2) Underreporting of cases due to inadequate access to healthcare facilities; 3) Low sample collection rate in reporting states; 4) Poor infectious disease laboratories support in remote areas; 5) Corruption and lack of political will by current administration to fight the virus; 6) Weak monkeypox monitoring, possibly related to a limited health workforce and the COVID 19 pandemic response; 7) A lack of international cooperation, unity, and coordination in the pursuit of establishing global health equity; and 8) Lack of access to authorized and safe treatment and vaccine among other things. Despite these challenges, a monkeypox-free Nigeria is possible. To this end, a safe and effective immunization of the public, as with smallpox, polio and yellow fever, is the key to the future. Until, a safe and effective vaccine becomes readily available, control and prevention lies largely on non-pharmaceutical intervention measures.
Introduction
Monkey pox is an emerging and re-emerging viral zoonosis in different part of the globe with the potential of assuming a public health emergency of international concern – PHEIC [1, 2, 3]. The viral infection (with an incubation period of 7-14 days) is characterized with fever, chills, headaches, body pains, weakness, weariness, swollen lymph nodes (glands), and a rash. The rash appears after one to three days of fever, first appearing on the face and then spreading to other parts of the body, with the face and palms and soles being most commonly affected. Usually, it is a self-limiting condition that lasts between two and four weeks. Skin lesions featuring macules, papules, vesicles, pustules, and scabs are the distinguishing features of the infection [4, 5].
The Monkey pox virus (MPXV), the etiology of monkey pox is a 200 to 250 nm brick- shaped enveloped double- stranded DNA virus (genus – Orthopoxvirus and family - Poxviridae) with characteristic surface tubules and a dumbbell-shaped core component [6]. The virus shares an antigenic ancestor with the variola and vaccinia viruses and has a linear double-stranded DNA genome. There are two distinct genetic clades of the monkeypox virus: the Central African (Congo Basin) clade and the West African clade [7]. The former has historically caused more severe disease and was thought to be more transmissible than the latter. The geographical division between the two clades has so far been in Cameroon, the only country where both virus clades have been found [3, 8]. The MPXV has been found to be susceptible to several animal species. This includes non-human primates, rope squirrels, tree squirrels, dormice, Gambian pouched rats, and other species. Non-human primates like the monkey and other animals like rodents are the reservoir hosts and animal vectors of the virus [1].
Both animals to human transmission, as well as human to human transmission have been reported. The virus can spread from human to human as well as from animal to human (which is the initial [spillover] occurrence before the diagnosis of cases in humans). Direct contact with the blood, bodily fluids, skin, or mucosal lesions of infected animals (e.g., monkeys, squirrels, and rodents) can result in animal to human transmission. A bite, scratch, handling of infected bush meat, or consumption of improperly prepared or other products of infected bush meat can cause animal to human transmission. When a person comes into touch with the virus from an infected individual or via contaminated objects like clothing or bedding, human-to-human (person-to-person) transmission takes place. Consequently, there is a higher risk of infection for family members or healthcare professionals. The respiratory system, mucous membranes of the eyes, nose, and mouth, as well as any obvious or hidden breaks in the skin allows the virus to enter the body. Aerosols and droplets can cause human to human transmission during prolonged face-to-face or close contact. It is still unclear if infected people with no symptoms can transmit the MPXV, making it important for anyone attending gatherings to exert additional care [9].
Historically, MPXV was first isolated from an animal (Cynomolgus macaques) in 1958 and also in a nine months old baby in the Democratic Republic of Congo (DCR) in 1970 with most cases reported in the rainforest and rural areas [7, 10, 11]. West Africa and Central Africa Basin are the two clades where MPXV is endemic [4, 12]. Only a few cases were irregularly reported for several years since 1970. Then, in 2017, there was a sharp increase, with over 2800 suspected cases recorded in seven African nations (The Democratic Republic of the Congo, Nigeria, Cameroon, Liberia, Sierra Leone, Gabon, and Sudan) [13]. This increase persisted, reaching a peak in 2020 with more than 6300 suspected cases (however the number of probable cases then decreased to about 3200 in 2021), 95% of which were in the Democratic Republic of the Congo. Although the causes of these spikes are unknown, deforestation and human intrusion into the habitats of the monkeypox animal hosts may be responsible. The majority of cases, according to the World Health Organization [10], have involved people under the age of 16, with 1:10 mortality rate. The Nigeria Centre for Disease Control (NCDC) for the first time received notice of a possible monkeypox epidemic in Bayelsa State on September 22, 2017 [14]. From Bayelsa to Rivers, Ekiti, Akwa Ibom, Lagos, Ogun and Cross River, the scourge of Monkeypox has continue to bite seriously on the country [15], unfortunately the country appears not to be doing enough to stop or arrest this public health monster five (5) years after the disease was first reported in the country.
Amidst global relaxation of the COVID-19 intervention measures and celebration of the unprecedented grounds conquered in the fight against the pandemic, the MPXV have emerged and remerged in many countries taking over major headlines around the globe at the present. Since 1 January and as of 22 June 2022, 50 nations and territories in five WHO Regions have reported 3413 laboratory-confirmed cases, along with one fatality [10]. This current review takes a look at the global and local upsurge in monkeypox epidemic, with emphasis on current trends, challenges and future prospects.
Current Trends of Monkeypox Around the Globe
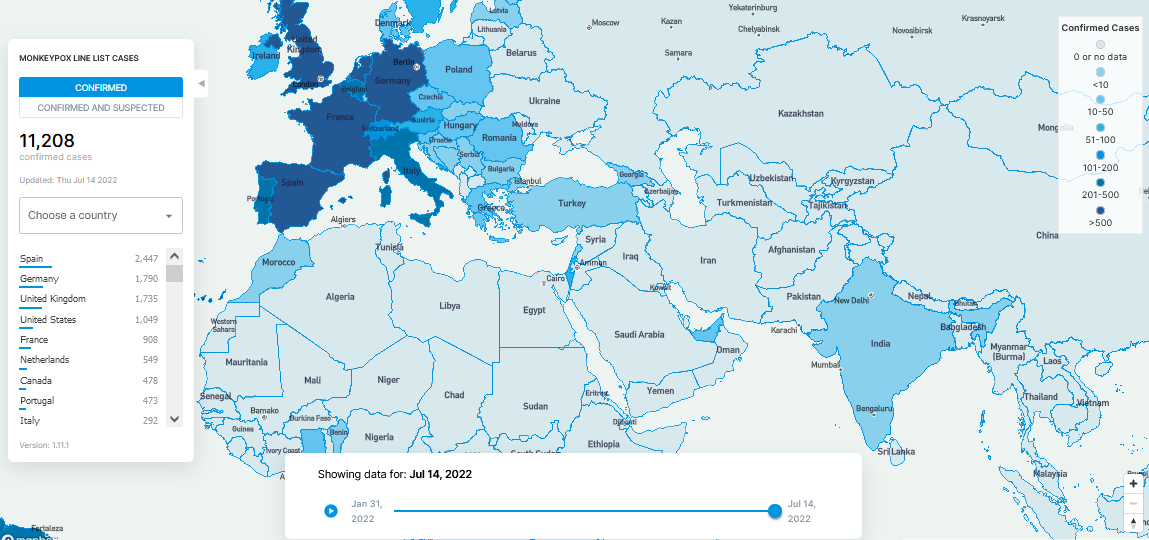
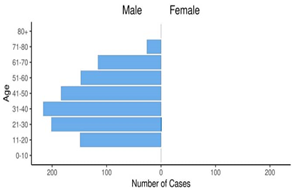
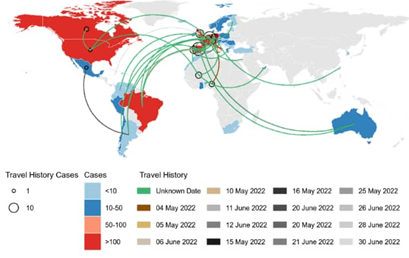
Since 1 January and as of 22 June 2022, 3413 laboratory confirmed MPXV cases and one death have been reported to the World Health Organization (WHO) from 50 countries/ territories in five WHO Regions (Table 1). The majority of laboratory confirmed cases (2933/3413; 86%) were reported from the WHO European Region. Other regions reporting cases include: the African Region (73/3413, 2%), Region of the Americas (381/3413, 11%), and Eastern Mediterranean Region (15/3413, <1%) and Western Pacific Region (11/3413, <1%). One death was reported in Nigeria in the second quarter of 2022 [10]. Between January 31, 2022 and July 14, 2022, a total of 11,208 MPXV cases have been confirmed globally. The top 5 most hit countries as indicated by Global Health (Figure 1) are Spain (2,447), Germany (1,790), United Kingdom (1,735), France (908) and Netherlands (549). Ninety-nine percent (99%) of global MPX cases were reported among males within the mean age of 40 years (Figure 2). At the moment, monkeypox is no longer Africa problem, but a global one due to travel history (Figure 3). For instance, in July 2021, more than 200 people in 27 US states were tracked for possible rare monkeypox infections. Health officials feared people may have come in contact with a Texas man, believed to be the 1st monkeypox case in the US since 2003. According to the Centers for Disease Control and Prevention (CDC), there are concerns that passengers on board two flights the man may have been exposed to the disease. He arrived in Atlanta, Georgia on [9 July 2021] on a flight from Lagos, Nigeria, and then traveled by air to Dallas, where he was taken to a hospital [16]. Despite being uncommon, the illness has occasionally struck the US. A 2003 outbreak that resulted in 47 confirmed or probable cases was connected to imported [West African] rats. In the context of the current monkeypox outbreak and spread around the globe, cases have been primarily identified among some gay, bisexual and other men who have sex with men including those who have reported recent sex with a new partner or multiple partners [17].
| WHO Region | Country/Area/Territory | Confirmed Cases |
|---|---|---|
| African Region | Benin | 3 |
| Cameroon | 3 | |
| Central African Republic | 8 | |
| Congo | 2 | |
| Democratic Republic of the Congo | 10 | |
| Ghana | 5 | |
| Nigeria | 41 (Including 1 death) | |
| South Africa | 1 | |
| Region of the Americas | Argentina | 3 |
| Brazil | 11 | |
| Canada | 210 | |
| Chile | 3 | |
| Mexico | 11 | |
| United States of America | 142 | |
| Venezuela (Bolivarian Republic of) | 1 | |
| Eastern Mediterranean | Lebanon | 1 |
| Morocco | 1 | |
| United Arab Emirates | 13 | |
| European Region | Austria | 12 |
| Belgium | 77 | |
| Czechia | 6 | |
| Denmark | 13 | |
| Finland | 4 | |
| Georgia | 277 | |
| Germany | 1 | |
| Greece | 521 | |
| Hungary | 1 | |
| Iceland | 3 | |
| Ireland | 7 | |
| Israel | 3 | |
| Italy | 24 | |
| Lativia | 13 | |
| Luxembourg | 85 | |
| Malta | 2 | |
| Netherlands | 167 | |
| Norway | 4 | |
| Poland | 7 | |
| Portugal | 317 | |
| Romania | 5 | |
| Serbia | 1 | |
| Western Pacific Region | Australia | 9 |
| Republic of Korea | 1 | |
| Singapore | 1 | |
| Cumulative | 50 countries/territories | 3413 |
Table 1: Confirmed cases of MPX by WHO region and country from 1 January to 22 June, 2022 [10].
Current Trends of Monkeypox in Africa
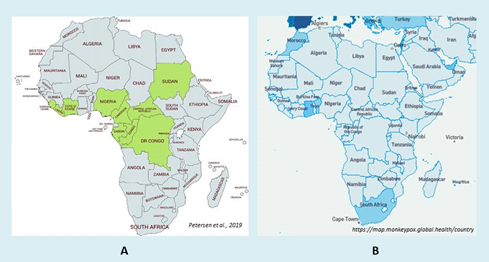
According to the African CDC, there have been 1715 instances of monkeypox reported from 8 endemic and 2 non- endemic African Union (AU) Member States (MS) since the start of 2022, with 1636 suspected cases and 79 confirmed deaths (CFR: 4.3 percent) [10]. This includes Benin (3 cases, 0 deaths), Cameroon (28, 2), Central African Republic (17, 2), Republic of Congo (7, 3), Democratic Republic of the Congo (1439, 67), Ghana (12, 0), Nigeria (162 suspected,
41 confirmed, 1 death) and South Africa (1, 0), according to World Health Organization data (numbers differ slightly from Africa CDC numbers). According to reports, two (2) of the three Benin cases had just visited Nigeria. The other instance, which had no known recent travel history, was found in the country’s north. So far, Africa has reported 12,141 cases and 363 fatalities (CFR 3%) of monkeypox during the COVID-19 pandemic period (February 2020 to 27 June 2022). Till date, the number of cases has remained on the rise on the continent (Figure 4) [10, 11, 18, 19, 20].
Coming to Nigeria, at the onset of the outbreak, 33 suspected cases in all were recorded in 2017 from 7 states. However, since then Nigeria has continued to report intermittent MPX occurrences after September, 2017 [21]. Prior to 2019, monkeypox cases in Nigeria were primarily reported in the south of the country. However, since 2020, the virus has spread to the country’s central, eastern, and northern regions (Figure 5 & 6) [14, 15]. According to the NCDC epidemiology report of week 25 [22], forty-two (42) new suspected cases were reported from 18 states, including Abia (1), Adamawa (2), Bayelsa (4), Benue (1), Cross River (2), Delta (2), Edo (1), FCT (3), Katsina (1), Kwara (1), Gombe (3), Lagos (5), Nasarawa (4), Ondo (2), Oyo (2), Plateau (4), Rivers (2) and Taraba (2). Out of 42 suspected cases, there were 21 new positive cases from 13 states: Abia (1), Adawama (1), Bayelsa (1), Edo (1), Cross River (2), Delta (2), FCT (2), Katsina (1), Lagos (2), Nasarawa (2), Plateau (2), Rivers (2), and Taraba (2). Furthermore, 204 suspected cases and 62 confirmed cases (44 male, 18 female) have been reported from 19 states between January 1 and June 26, 2022: Abia (1), Adamawa (6), Bayelsa (5), Cross River (4), Delta (5), Edo (4), FCT (4), Imo (2), Kano (2), Katsina (1), Lagos (10), Nasarawa (3), Niger (1), Ogun (1), Ondo (1), Oyo (1), Plateau (4), Rivers (5) and Taraba (2) (Table 2). Majority of the confirmed cases were reported among male patients (Figure 7) within the age range of 31-40 years (Table 3). Infection has been more prevalent towards the end of the year (August – December) since the onset of the outbreak in 2017, except in 2022 (April) (Figure 8).
![Figure 5: Map of Nigeria showing distribution of suspected MPX cases in 7 states in 2017 [14].](/fulltextimages/9008/fig_5.png)
![Figure 6: A map of Nigeria showing distribution of confirmed MPX cases in 25 States between September 2017 and June 26th, 2022 [22].](/fulltextimages/9008/fig_6.png)
![Figure 7: Age and gender distribution of confirmed MPX cases in Nigeria from September 2017 to June 26th, 2022 [22].](/fulltextimages/9008/fig_7.png)
![Figure 8: Line graph showing confirmed MPX cases in Nigeria from September 2017 to June 26th 2022, according to the incidence year [22].](/fulltextimages/9008/fig_8.png)
| State | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | Total |
|---|---|---|---|---|---|---|---|
| Rivers | 25 | 14 | 7 | 1 | 5 | 5 | 57 |
| Bayelsa | 19 | 11 | 7 | o | 6 | 5 | 48 |
| Lagos | 4 | 1 | 15 | 4 | 6 | 10 | 40 |
| Delta | 3 | 6 | 10 | 1 | 9 | 5 | 34 |
| Cross River | 9 | 3 | 1 | o | 1 | 4 | 18 |
| Imo | 5 | 2 | 1 | o | o | 2 | 10 |
| Akwa Ibom | 6 | o | 1 | o | o | o | 7 |
| Oyo | 1 | 3 | 2 | o | o | 1 | 7 |
| Edo | 4 | 1 | 1 | o | 4 | 4 | 14 |
| FCT | 5 | o | o | o | 1 | 4 | 10 |
| Enugu | 1 | 2 | 1 | o | o | o | 4 |
| Abia | 1 | 2 | o | o | o | 1 | 4 |
| Plateau | o | 2 | o | 1 | o | 4 | 7 |
| Nasarawa | 1 | 1 | o | o | o | 3 | 5 |
| Benue | 2 | o | o | o | o | o | 2 |
| Anambra | o | 1 | 1 | o | o | o | 2 |
| Ekiti | 2 | o | o | o | o | o | 2 |
| Ebonyi | o | o | o | 1 | o | o | 1 |
| Niger | o | o | o | o | 1 | 1 | 2 |
| Ogun | o | o | o | o | 1 | 1 | 2 |
| Adamawa | o | o | o | o | o | 6 | 6 |
| Kano | o | o | o | o | o | 2 | 2 |
| Ondo | o | o | o | o | o | 1 | 1 |
| Taraba | o | o | o | o | o | 2 | 2 |
| Katsina | o | o | o | o | o | 1 | 1 |
| Grand Total | 88 | 49 | 47 | 8 | 34 | 62 | 288 |
Table 2: Age distribution of MPX cases confirmed between September 2017 and June 26th, 2022 [22].
| Age Group | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | Total |
|---|---|---|---|---|---|---|---|
| 0-10 Years | 7 | 5 | 1 | o | 1 | 7 | 21 |
| 11-20 Years | 12 | 4 | 1 | 0 | 4 | 6 | 27 |
| 21-30 Years | 34 | 13 | 13 | 4 | 10 | 18 | 92 |
| 31-40 Years | 26 | 17 | 22 | 4 | 13 | 23 | 105 |
| 41-50 Years | 9 | 10 | 9 | 0 | 5 | 8 | 41 |
| 51-60 Years | 0 | 0 | 1 | 0 | 1 | 0 | 2 |
| Total | 88 | 49 | 47 | 8 | 34 | 62 | 288 |
Table 3: Age distribution of MPX cases confirmed between September 2017 and June 26th, 2022 [22].
states from the resurgence of monkeypox in September 2017 until June 26, 2022. Out of the 716 suspected cases, 288 (40.2 percent), have been confirmed, with the affected states being: Abia (4), Adamawa (6), Akwa Ibom (7), Anambra (2), Bayelsa (48), Benue (2), Delta (34), Cross River (18), Ebonyi (1), Edo (14), Ekiti (2), Enugu (4), FCT (10), Imo (10), Kano (2), Katsina (1), Lagos (40), Nasarawa (5), Niger (2), Ogun (2), Ondo (1), Oyo (7), Rivers (57), Plateau (7) and Taraba (2). Additionally, between September 2017 and June 26, 2022, a total of 9 deaths have been recorded (CFR= 3.1%) in 6 states: Cross River (1), Edo (2), FCT (1), Imo (1), Lagos (3), and Rivers (1). In response to a risk assessment of the local, national, and international monkeypox situation, a monkeypox National Emergency Operations Center (EOC) was activated on May 26th, 2022. The primary goal of founding the EOC was to better coordinate national planning and response efforts.
Challenges in the Control of Monkeypox
Some of the Identified Challenges Militating Against the Fight against MPX Include the Followings
- Low patient use of healthcare facilities because of stigma, expense, and low fatality rate
- Underreporting of cases due to inadequate access to healthcare facilities.
- Low sample collection rate in reporting states.
- Poor infectious disease laboratories support in remote areas.
- Corruption and lack of political will by current administration to fight the virus.
- Weak monkeypox monitoring, possibly related to a limited health workforce and the COVID-19 pandemic response.
- A lack of international cooperation, unity, and coordination in the pursuit of establishing global health equity.
- Lack of access to authorized and safe therapeutics and vaccine [4, 21, 23].
Monkeypox Therapeutics and Vaccines
Although supportive care is usually sufficient for the majority of monkeypox cases, which have moderate and self-limited disease, there are broad spectrum antivirals (such as tecovirimat, brincidofovir, and cidofovir) and vaccinia immune globulin intravenous (VIGIV) currently being used for the treatment and management of MPX cases. Antivirals should be taken into account in cases of severe illness, immunosuppressed individuals, children, pregnant and nursing women, complicated lesions, and when lesions develop close to the mouth, eyes, or genitalia [24]. Based on animal models and data regarding safety, pharmacokinetics, and pharmacodynamics in humans, the European Medicines Agency recently granted regulatory approval for tecorivimat for use in treating orthopovirus-associated illnesses, such as monkeypox. As a result, it is anticipated that information on its safety and effectiveness will soon be available in a credible, understandable and timely manner [2, 10].
Meanwhile, since smallpox was completely eradicated from the world in 1979, monkeypox has become the most common orthopoxvirus infection in humans. At the moment, the highly attenuated smallpox strain vaccine is being used and it has showed promise in humans, providing immunity for up to 6 weeks following vaccination. Although a new vaccine against smallpox and monkeypox has been approved, it is not yet widely available and accessible [11]. ACAM2000® (live, replication competent vaccinia virus) and JYNNEOSTM (live, replication-incompetent vaccinia virus) are the two vaccines that are now available for protection against MPXV. While ACAM2000® causes a significant cutaneous reaction at the site of injection, as well as progressive vaccinia and eczema vaccinatum in some people due to unchecked viral replication; JYNNEOSTM does not. Also, while ACAM2000® poses risk of accidental and auto-inoculation; JYNNEOSTM does not [25, 26]. To this end, the World Health Organization (WHO) has urged Member States to consider the current multi-nation monkeypox outbreak and call their national immunization technical advisory groups (NITAGs) in order to review the data and create recommendations for vaccine use that are appropriate to the national context. A healthcare expert and the prospective vaccinee should jointly weigh the risks and advantages of each smallpox or monkeypox vaccination on a case-by-case basis before choosing to receive it. Member States are urged to administer the monkeypox vaccine within the scope of cooperative clinical research, utilizing standardized design techniques and data gathering instruments for clinical and outcome information to speed up the emergence of evidence, especially regarding the safety and efficacy of vaccines [2, 10].
Future Prospects in the Control of Monkeypox
Globally, the World Health Organization (WHO) is keeping a close eye on the situation and is in favor of international cooperation and information sharing with partners and member states. Member States have activated the clinical and public health incident response to coordinate thorough case discovery, contact tracing, laboratory investigation, isolation, clinical management, and infection prevention and control measures. Genomic sequencing of the monkeypox virus deoxyribonucleic acid (DNA) found in the present outbreak is ongoing and preliminary results from polymerase chain reaction (PCR) tests show that the monkeypox virus genes detected belong to the West African clade [2, 10].
An impartial panel of specialists present at the meeting of the International Health Regulations Emergency Committee on the worldwide monkeypox outbreak on June 23, 2022, according to Science media Centre [25], recommended that monkeypox should not be declared a Public Health Emergency of International Concern (PHEIC) yet because the epidemic seems to be plateauing or there are downward trends in some (non-endemic) countries affected early in the international epidemic. The possibility of increasing stigmatization and the violation of impacted population groups’ human rights, such as their right to privacy, the prohibition of discrimination, and their right to good bodily and mental health, is more concerning because it would make response efforts more difficult. Meanwhile, some experts are in support of the opinion that the current monkeypox outbreak should be declared a PHEIC. This they believe would increase the drive for vaccine manufacture and purchase and may also help towards improving the flow of support into those African countries that are having a difficult time with endemic Monkeypox such as Democratic Republic of the Congo, which has seen monkeypox kill at least 58 people and infect over 1200 others since the start of the year.
Furthermore, some experts on the other hand opined that whether the monkeypox international epidemic is declared a PHEIC or not, this will not have a huge impact on the current epidemic as those non-epidemic countries with many cases are already taking steps to control the problem in their countries. While the WHO is yet to declare the monkeypox outbreak a PHEIC, more efforts are needed to fill in some existing gaps in knowledge, particularly in the areas of: transmission modes; full spectrum of clinical presentation; infectious period; reservoir species and potential for reverse zoonosis; the possibility of virus mutating; and access to vaccines and antivirals and their efficacy in humans [26, 27, 28].
Like other African countries, complete elimination of MPX in Nigeria is possible because we have all it takes in this country to control the disease with minimal assistance - but only, if we are intentional as a country and adopts some stringent measures including:
- Attitudinal changes among the Citizenry and the Government.
- Assume national ownership of MPX control and ensure cooperation among other African Countries.
- Develop a MPX control roadmap for the engagement of stakeholders and partners in the area of vaccine research and development.
- Research funding for indigenous monkey pox vaccine and treatment must become a priority at all levels.
- Provision of a well-functioning disease surveillance system which will aid early detection and response.
• Lastly, intensify public awareness campaigns on MPX among rural communities.
Conclusion
Like the country fought against Ebola some years back, it is very possible for Nigeria and other African countries to be free of MPX, but availability of effective and safe vaccine for the general public among other measures, is the key to the country’s future in the fight against this monster. But sad to say, to date Nigeria like other Africa countries is yet to produce her own MPX vaccine locally. To this end, African countries in general need to build local capacity for production of indigenous monkeypox vaccine. A path forward to future licensure of vaccines and therapeutics for MPX may rely on a traditional approval pathway involving multi-site efficacy trials in endemic regions of Africa and Nigeria in particular. Indeed, the apparent annual incidence of disease would support this route rather. While we gear concerted efforts in this direction, it is imperative that the MPX outbreak is quickly and effectively contained in all the affected states and other mapping areas. The Government and the general populace must be intentional in taking more proactive measures at all levels towards the total eradication of this public health threat before it becomes a pandemic just like the COVID-19.
Recommendations
- Creating public health awareness about the disease and educating the people especially in rural area should be encouraged.
- Availability of personal protective equipment (PPE) for health workers and enough laboratory kits for proper screening and diagnosis of patients should be implemented.
- It is very important that the general public have equal access to effective and safe MPX vaccines to stay protected. The vulnerable groups in particularly such as the contacts of cases and health workers should have access to Post-exposure prophylaxis (PEP) and Pre- exposure prophylaxis (PrEP), respectively.
- Enough isolation centers should be provided for MPX patients so as to reduce the spread of the virus.
- It is advisable to discourage behaviors like eating so- called “bush meats” that could increase contact with the MPXV.
- The Emergency Operations Center (EOC) should keep coordinating ongoing national response efforts while contributing to the international effort.
- Ensure that active case searches are conducted in facilities localities that have reported positive cases.
- NCDC should intensify ongoing plans to validate more MPX test kits. In addition, they should keep working with the Africa Centre for Disease Control (ACDC) to promote NRL’s regional training programs for African nations on the use of RT-PCR and MPX viral genomics to detect the monkeypox virus.
- Even though the modes of transmission for COVID-19 and MPX between people differ, some COVID-19 prevention strategies used in social settings, such as maintaining a physical distance and washing hands often, also work to prevent the spread of the MPXV and therefore should be encouraged.
- Until it is determined that they no longer pose a risk to the public health, anyone who is feeling ill, including those who have a fever and rash-like illness, or who is identified by jurisdictional health authorities as having MPX, should refrain from taking non-essential travel, including international. According to WHO interim guidance on surveillance, case investigation, and contact tracking, anyone who has experienced a rash-like illness while traveling or after returning home should contact a health care provider right away and provide details about all recent travel, immunization history, including whether they have received the smallpox vaccine or other vaccines (such as the measles-mumps-rubella vaccine or the varicella zoster vaccine, to support making a diagnosis), and information on close contacts.
Competing Interests
The authors have stated that there are no conflicting interests.
Funding
This compilation is a review article written by its authors and required no substantial funding to be stated.
References
-
Parker S, Nuara A, Buller RM, Schultz DA (2007) Human monkey pox; an emerging zoonotic disease. Future Microbiol 2(1): 17-34_._
-
Igiebor FA, Agbontaen OJ, Egharevba PA, Amengialue OO, Ehiaghe JI, et al. (2022) Monkeypox: Emerging and Re-emerging Treats in Nigeria. BIU Journal of Basic and Applied Sciences 7(1): 119-132.
-
World Health Organization (WHO) (2022) Monkeypox.
-
Sukanya K, Swami P (2018) A brief review on monkey pox virus. International Journal of Science and Research 7(1): 1480-1483.
-
Barnett A (2021) Eight symptoms of monkeypox to watch for as virus cases discovered in the UK.
-
Takele TH, Huaijie J, Guohua C, Fang Y, Xiang XH, et al. (2019) Methodological Review on Monkey pox virus: Replication and Gene Responsible for the development of infection and host immune response against the disease. Arch Microbiol Immunology 3(2): 003-019.
-
Osadebe L, Hughes CM, Shongo Lushima R, Kabamba J, Nguete B, et al. (2017) Enhancing case definitions for surveillance of human monkeypox in the Democratic Republic of Congo. PLoS Negl Trop Dis 11(9): e0005857.
-
Falendysz EA, Lopera JG, Doty JB, Nakazawa Y, Crill C, et al. (2017) Characterization of Monkeypox virus infection in African rope squirrels (Funisciurus sp.). PLoS Negl Trop Dis 11(8): e0005809.
-
Hutin YJ, Williams RJ, Malfait P, Pebody R, Loparev VN, et al. (2001) Outbreak of human monkeypox, Democratic Republic of Congo, 1996-1997. Emerg Infect Dis 7(3): 434-438.
-
World Health Organization (WHO) (2022) Multi-country monkeypox outbreak: situation update.
-
World Health Organization (WHO) (2022) WHO is supporting African countries to strengthen monkeypox surveillance and response actions.
-
Reynolds MG, Damon IK (2012) Outbreaks of human monkey pox after cessation of smallpox vaccination. Trends Microbiol 20(2): 80-87.
-
Yinka-Ogunleye A, Aruna O, Dalhat M, Ogoina D, McCollum A, et al. (2019) Outbreak of human monkeypox in Nigeria in 2017–2018: A clinical and epidemiological report. Lancet Infect Dis 19(8): 872-879.
-
Nigeria Centre for Disease Control (NCDC) (2017) Monkey pox Outbreak in Nigeria Situation Report (No. 001).
-
Nigeria Centre for Disease Control (NCDC) (2021) Update on Monkeypox (MPV) in Nigeria. Situation Report, Series Number 10 (EPI-Week 38).
-
Maryland Department of Health (2021) Travel- Associated Monkeypox virus infection confirmed in Maryland resident.
-
Bunge EM, Hoet B, Chen L, Lienert F, Weidenthaler H, et al. (2022) The changing epidemiology of human monkeypox—A potential threat? A systematic review. PLoS Negl Trop Dis 16(2): e0010141.
-
Africa Centre for Disease Control (African CDC) (2022) Monkey pox in Africa: 1,715 cases, 73 deaths in 2022 to date, according to African CDC.
-
(2022) Outbreak News Today Africa: Benin reports 3 monkeypox cases.
-
Petersen E, Kantele A, Koopmans M, Asogun D, Yinka-Ogunleye A, et al. (2019) Human Monkeypox Epidemiologic and Clinical Characteristics, Diagnosis, and Prevention. Infect Dis Clin North Am 33(4): 1027- 1043.
-
Kabuga AI, El Zowalaty ME (2019) A review of the monkeypox virus and a recent outbreak of skin rash disease in Nigeria. J Med Virol 91(4): 533-540.
-
Nigeria Centre for Disease Control (NCDC) (2022) Update on Monkey pox (MPV) in Nigeria Situation Report, Series Number 09 (EPI-Week 25).
-
Oladoye MJ (2021) Monkey pox: A Neglected Viral Zoonotic Disease. European journal of Medical and Educational Technologies 14(2): em2108.
-
Rizk JG, Lippi G, Henry BM, Forthal DN, Rizk Y, et al. (2022) Prevention and Treatment of Monkeypox. Drugs 82: 957-963.
-
Sciencemedia Centre (2022) Expert reaction to WHO Emergency Committee not recommending that the ongoing monkeypox outbreaks be declared a Public Health Emergency of International Concern (PHEIC).
-
UK Health Security Agency (2022) Recommendations for the use of pre and post exposure vaccination during a monkeypox incident.
-
Velavan TP, Meyer CG (2022) Monkeypox 2022 outbreak: An update. Trop Med Int Health 27(7): 604-605.
-
World Health Organization (2022) WHO consultation sets research priorities for monkeypox.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions