Detection of HBV DNA among HBsAg Negative Patients
The persistence of Hepatitis B viral DNA (HBV DNA) in the blood or liver without the presence of detectable HBsAg is called Occult Hepatitis B infection (OBI)). This has become a threat when considering prevention of HBV transmission in our community. The purpose of this study was to determine prevalence as well as the HBV genotype(s) associated with OBI in Ibadan, Nigeria. HBsAg negative, using ELISA techniques, 219 blood samples were included for the study. Nested Polymerase Chain Reaction was used for the detection of HBV DNA in the samples. Data collected was processed using descriptive statistics and Chi square at p = 0.05. The number of male and female participants were 102 (46.6%) and 117 (53.4%) (P = 0.204) respectively. The participants have age range from 1 to 70 years with mean age of 32.1 years (SD =12.7) for females and 33.9years (SD = 12.4) for males. The clinical status of participants ranged from asymptomatic to those presented with acute hepatitis disease. Out of the 219 samples tested, one was positive for HBV DNA giving a prevalence of 0.5%. The positive sample was from a 30 years old female. We were unable to determine the genotype of the isolate due to poor sequence data. There is evidence of circulation of Occult Hepatitis B virus in our community as shown with prevalence of 0.5% OBI in this study. There is need for screening of blood units using Nucleic Acid Testing (NAT) technique to reduce the transmission of the virus through transfusion of infected blood and blood products. There is also need to increase awareness of HBV vaccination among the general population to forestall the danger OBI may pose.
Introduction
It is of public health importance to understand Hepatitis B virus (HBV) infection and to also put measure in place for necessary intervention. Literatures have shown that about 2 billion people have evidence of HBV serological indicators and 300 million have come down with chronic HBV infection worldwide [1]. The relationship between the host and viral factors are important in determining the outcome of every infection. The presence of Hepatitis B virus surface antigen (HBsAg) and the virus in the blood is termed Chronic HBV infection. The absence of viral DNA with reduction in disease manifestation usually accompanies removal of HBsAg in chronic hepatitis B patients [2]. There was report of Occult HBV infection in year 1970s. There was discussion to review information on OBI in 1998 by scientists from US and European. The level of HBV DNA in liver and serum remain low after disappearance of HBsAg in acute or chronic HBV infection. This occurrence is termed occult HBV infection which is interpreted as detection of HBV DNA in absence of HBsAg in the blood [2, 3, 4, 5]. OBI has been identified as one of the causative factors of HBV transmission despite public awareness of the disease prevention. This is due to its non-detection using routine surface antigen detection assays and this could leads to infection through blood transfusion or organ transplantation. There is possibility of reactivation of OBI and its eventual cause of acute hepatitis in immunocompromised individual or those receiving chemotherapy. OBI has been implicated for its potential to cause hepatocellular carcinoma by its ability to influence hepatic inflammation and fibrosis.
There is need to determine the prevalence of OBI infection using more sensitive assay like polymerase chain reaction to enhance prevention of the infection. Previous studies have focused on people like pregnant women or blood donor while there is little information on the general population. Hence, it is necessary to carried out study to detect OBI among HBsAg negative patients. Literature has established circulation of OBI in HBV endemic population like Nigeria. In his study, reported OBI prevalence of 7.1% among adult patients with viral hepatitis in Ibadan; observed prevalence of 17% among blood donors; in another study using HIV positive archived samples observe 11.2 % while reported prevalence of 14.6% among Nigerian patients on haemodialysis. These gave us little or no information about its prevalence in the general population [6, 7, 8, 9]. Hence, the need to investigate general population. There is also need to determine if a particular genotype of HBV is responsible for circulating occult OBI. This will help in epidemiology survey and control of the spread of the virus and also in vaccine production.
Materials and Methods
Study Area
This study was done in Ibadan among patients referred to the Department of Virology for HBV screening. The town serve as the capital city of Oyo State in Nigeria. It has population of about 3 million. This explains the reason is one of the most populous cities in Nigeria. It has the largest geographical area and hence it accommodates people from different parts of the country. Sampling from the city is a good representative of the country. Ibadan is located at South-eastern part of the State between Coordinates 10°23’
0”N, 12°5’ 0” E. The town cover an area of 3,080 sq. Km (square kilometres) and located at 119 km (74miles) of Lagos northeast and 120 km (75 miles) east of Nigeria away from Republic of Benin international border.
Sampling
Plasma samples previously collected and tested HBsAg negative and stored at -20oC were retrieved. Aliquot of each sample was dispensed into appropriately labeled cryovials and used for this study while the remaining samples were returned to -20oC.
HBV DNA Detection: Extraction of DNA was carried out on each of the 219 blood specimens with the aid of guanidium thiocyanate extraction method [10]. HBV-DNA was detected using a routine diagnostic PCR in the department of virology, University of Ibadan HBV laboratory. The primers used are: HBV S1F 5′-CTA GGA CCC CTG CTC GTG TT-3′ (Sense), HBV S1R 5′-CG AAC CAC TGA ACA AAT GGC ACT-3′ (Anti-sense), HBV SNF 5′-GTT GAC AAG AAT CCT CAC AAT ACC-3′ (Sense), HBV SNR 5′-GA GGC CCA CTC CCA TA-3′ (Anti-sense). PCR amplification was carried out using 25 μL solution consist of 12.5 μL type of Red load Taq (Jena Bioscience, Jena, Germany), 1.0 μL of each primers, HBV-SF as forward and HBV-SNR as reverse primers, DNA of 3.0 μL and RNase of 7.5 μL free water. Using an Applied Bio system Verity TM 9700 Thermal Cycler, amplification was done as follows: 94°C for 3 minutes leading to 45 cycles of 94°C which ran for 30 seconds, 55°C for 60 seconds and 72°C for 40 seconds. This was followed by 72°C for 7 minutes and held at 4°C till terminated. The reaction conditions for first and second round PCR were the same except that DNA product of first round was used as template for second round PCR. The products of PCR with band size of 409bp were separated on 2% agarose gels which were dye with cyber green and it was made visible with the use of UV. Positive and negative controls were included in the run to standardise the PCR reaction.
Statistical Analysis
Data obtained were entered into an Excel sheet and studied with the aid of statistical package for social sciences version 21 (Chicago, IL, USA). Analyses were carried out using descriptive statistics; the mean and standard deviations (SD) were determined. Both relationships and differences were also determined using Chi‑square test where applicable at a P < 0.05.
Results
A total of 219 samples which were already tested as HBsAg negative with the aid of Enzyme-Linked Immunosorbent Assay (ELISA) were retrieved from the Department of Virology, University of Ibadan were included for the study. The number of female was higher with 117 (53.4%) than that of male, 102 (46.6%) (Table 1; P = 0.204). The age range most represented was 20-29 years with 78 (35.6%) participants, followed by the interval of 30-39 years with 67 (30.6%) participants and the least was those ≥ 69 years with 5 (2.3%) participants (Table 1). The mean age was 33.9 years (SD = 12.4) for males and 32.1years (SD = 12.7) for females.
| Age (Years) | Gender | Total N (%) | |
|---|---|---|---|
| Male N (%) | Female N (%) | ||
| ≤19 | 7 (6.9) | 13 (11.1) | 20 (5.9) |
| 20-29 | 34 (33.3) | 44 (37.6) | 78 (35.6) |
| 30-39 | 38 (37.3) | 29 (24.8) | 67 (30.6) |
| 40-49 | 10 (9.8) | 17 (14.5) | 27 (12.3) |
| 50-59 | 9 (8.8) | 13 (11.1) | 22 (10.0) |
| ≥60 | 4 (4.0) | 1 (0.9) | 5 (2.3) |
| Total | 102 (46.6) | 117 (53.4) | 219 (100) |
Table 1: This Shows Distribution of the Population.
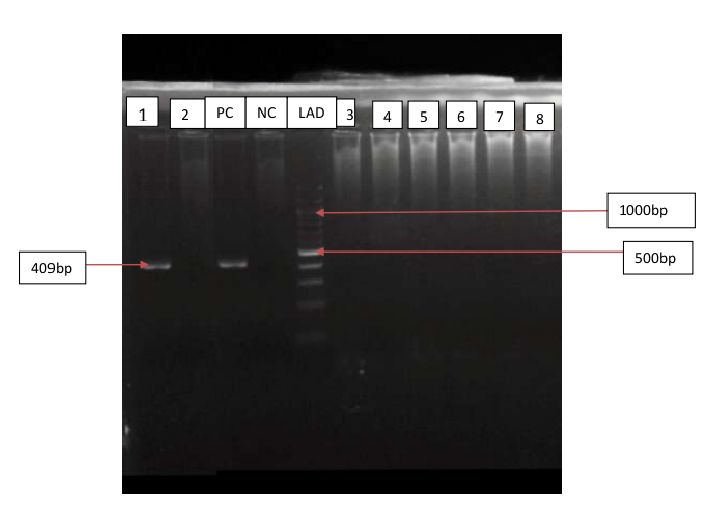
Figure 1 shows picture of gel from PCR product of amplification of HBV S-gene of HBsAg-negative samples with expected band size of 409bp. Out of the 219 samples tested only 1 (0.5%) was HBV DNA positive by nested PCR indicating OBI. The sample was from a female (0.8%) of 30 years old and none was positive for male (0%). Distribution of HBV DNA among the gender was not statistically significance ((Table 2); P = 0.352).
| Gender | Number Tested | HBV DNA Positive N (%) | HBV DNA Negative N (%) |
|---|---|---|---|
| Male | 102 | 0(0) | 102(100) |
| Female | 117 | 1(0.8) | 116(99.1) |
| Total | 219 | 1(0.5) | 218(99.5) |
Table 2: Statistical Distribution of HBV DNA among the Population by Gender.
P = 0.352, χ2 Table 2: Statistical Distribution of HBV DNA among the Population by Gender.
Figure 1 shows picture of gel from PCR product of amplification of HBV S-gene of HBsAg--positive samples with expected band size of 409bp. The HBsAg-positive samples show a detectable HBV DNA.
Discussion
The prevalence of Occult Hepatitis B infection (OBI) varies in different countries of the world depending on the level of HBV endemicity, HBV screening method adopted and primers used for Nucleic Acid Testing [7]. There is limited available data on prevalence of OBI in sub-Saharan Africa. A prevalence of 10% and 15% has been recorded in studies conducted among HIV infected patients in Ivory Coast and Sudan [11, 12]. Likewise, prevalence of 10.6% was recorded in research conducted in Northeast China among 359 HBsAg-negative populations [13]. OBI prevalence of 8% was reported by Nna E, et al. [14] among 100 blood donors in Abakaliki, Nigeria. Another study conducted in Nigeria by Oluyinka OO, et al. [7] observed prevalence of 17% among blood donors. Various study in Nigeria indicates HBV seroprevalence ranges from 9%-39% [15]. The prevalence above is higher than 0.5% as observed in this study. This could be as a result of differences in target population and/ or screening method adopted (nested PCR or automated real time PCR assays).
The OBI prevalence observed in this study is comparable to OBI prevalence of 0.5 % as observed by among 1026 blood donor samples in Egypt and also, 3% observed among an Italian migrant population. Other literatures show differences in the OBI prevalence as seeing from Taiwan, Laos, Australia and North Africa with OBI ranging from 0.1% to 15% [16, 17, 18, 19].
Prevalence of OBI in a study population different from blood donors in Nigeria such as Opaleye OO, et al. [8] using archived HIV positive samples in Ikole Ekiti obtained prevalence of 11.2%. OBI prevalence of 7.1% was reported among chronic hepatitis patients in Ibadan by Ola SO, et al. [6] while Igetei R, et al. [9] recorded 14.6% among Nigerians on haemodialysis. These are higher than OBI prevalence observed in this study. This could be as a result of population in which those studies were conducted. Literatures show that prevalence of OBI is higher among people who are more exposed to HBV infection (e.g. patients on haemodialysis), liver disease and also in HIV-positive individuals [20, 21].
OBI is observed when there is detectable HBV DNA in a blood sample with no observable presence of HBsAg [22]. There is need to adopt PCR for the detection of OBI to prevent its possible transmission during blood transfusion or other tissue transplant. Detection of HBV DNA in the study population (HBsAg negative samples), which was previously screened by ELISA technique, in this study support the earlier studies that PCR is more sensitive in detection of HBV when compare to ELISA techniques [23]. The use of PCR led to the detection of HBV DNA in one of the patients tested (0.5%, P = 0.352), initially diagnosed as HBsAg seronegative. This phenomenon (detection of HBV DNA without HBsAg) is termed OBI.
We could not screen for anti-HBc due to financial constrain. Presence of anti-HBc in the blood is a pointer to the presence of OBI. In some cases there is absence of anti- HBc in OBI patients. This is termed seronegative OBI (OBI without detectable anti-HBc and anti-HBs). The occurrence could be related to the finding of which shows 6 out of 8 (75%) of the OBI positive samples tested were negative to anti-HBc. In a study conducted by Oluyinka OO, et al. [7], 28% of OBI samples were negative for anti-HBc. Patients with detectable anti-HBc antibody usually tested positive for OBI. Though anti-HBc may be absent sometimes in some people Daef EA, et al. [24, 25, 26]. Hence, there is need to combine HBsAg, anti-HBc and OBI screening to prevent HBV circulation in our population.
We could not screen for HIV status of our samples due to limited fund. HIV has been recognised as one of the risk factors for OBI. This is due to common routes of transmission. HIV could influence the course of hepatitis B virus (HBV) infection and this effect reinforced outcome of morbidity and mortality. OBI prevalence in HIV positive patients ranges from 0% to 89% depending on the geographical area. Nunez et al. reported no detectable HBV-DNA among 85 HIV-positive injection drug users and in another study by, 0.8% OBI was found among French HIV-infected patients while 11.2 % OBI was reported among HIV positive population by found. Different studies from Brazil and Netherlands reported OBI prevalence of 5% in HIV positive patients [8, 27, 28, 29, 30, 31, 32, 33].
In this study, distribution of HBV DNA among the gender was not statistically significant (P = 0.352). Although, this may be due to limited number of OBI positive sample in this study but it is in concord with Minuk GY, et al. [34] who detected 8.1% OBI in North America community-based population and also observed that some factors could not be used to predict people living with OBI and the factor include: age, gender and liver biochemistry. The only HBV DNA carrier in this study was a female of 30 years. It is comparable with Oluyinka OO, et al. [7] who reported 44 out of 72 (61%) OBI carriers to be female and that the age group of 30–39 years formed the highest prevalence of OBI. This is a child bearing age and with many of the women receiving blood during delivery, it is easy to transfuse occult HBV infected blood in the process. Many of our blood banks do not screen blood using PCR techniques, which is effective in detecting occult HBV, before giving out blood unit. Hence, this could be one of the reasons behind rise in population of occult HBV female carrier.
We could not screen for hepatitis C virus (HCV) status of our samples due to limited fund. Literatures have shown HCV to be a risk factor for OBI. HCV-HBV co-infection could result in decrease replication process of both virus but with more observable effect in HBV. There is suppression of HBV gene expression and replication when HCV core protein attached to HBV-DNA. OBI may be encountered in HIV-HCV co-infected patients and may cause more severe liver disease and lower response to interferon [35, 36].
We could not sequence the OBI amplicons in this study due to low yield. Studies have shown that OBI of genotype E is mostly circulating in West Africa especially in Nigeria. In his study among blood donor, Oluyinka OO, et al. [7] observed higher prevalence of HBV genotype E among the isolated OBI. He also observed that Occult HBV-infected and HBsAg- positive population show no difference in their genotype.
Various studies including this one have shown evidence of circulation of OBI in Nigeria. Knowledge gathered from different literatures have revealed that OBI could occur as a result of mutation in the “a” determinant of HBsAg which leads to conformational changes and hence making the HBsAg undetectable by ELISA assays. This type of mutation is associated with HBV persistence despite HBIG prophylaxis. OBI can also be traced to treatment-associated mutations. This could be traced to the HBV polymerase double mutations which could result in amino acid changes in both HBV polymerase and the surface gene [37, 38, 39].
Conclusion
This study shows OBI prevalence of 0.5% consequentially indicating its circulation in the country. Increase in the circulation of OBI is usually observed in high endemic areas such as Nigeria. In addition to HBsAg and anti-HBc ELISA screening, there is need for urgent screening for OBI using nucleic acid testing (NAT) to prevent its further spread to susceptible individual. Hepatitis B is one of the highly contagious viral infections due to exposure to infected body fluids. Government needs to ensure that every citizen knows their HBV status. All government hospitals or blood donor centres should be equipped to carry out NAT and anti HBc before giving out blood. There should be an effective vaccination of individuals to prevent the spread of HBV infection.
Declaration of Conflict of Interest
There is no conflict of interest
Funding
The project was funded by me
References
-
Lavanchy D (2015) worldwide epidemiology of HBV infection, disease burden, and vaccine prevention. J Clin Virol 34(1): S1-3.
-
Hoofnagle JH, Seeff LB, Bales ZB, Zimmerman HJ (1978) Type B hepatitis after transfusion with blood containing antibody to hepatitis B core antigen. N Engl J Med 298(25): 1379-1383.
-
Tabor E, Hoofnagle JH, Smallwood LA, Drucker JA, Pineda-Tamondong GC, et al. (1979) Studies of donors who transmit post transfusion hepatitis. Transfusion 19(6): 725-731.
-
Grob P, Jilg W, Bornhak H, Gerken G, Gerlich W, et al. (2000) Serological pattern “anti-HBc alone”: report on a workshop. J Med Virol 62(4): 450-455.
-
Hu Z, Zhang Z, Kim JW, Huang Y, Liang TJ, et al. (2006) Altered proteolysis and global gene expression in hepatitis B virus X transgenic mouse liver. J Virol 80(3): 1405-1413.
-
Ola SO, Otegbayo JA, Odaibo GN, Olaleye DO, Olubuyide IO, et al. (2009) Occult HBV infection among a cohort of Nigerian adults. J Infect Dev Ctries 3(6): 442-446.
-
Oluyinka OO, Tong HV, Bui Tien S, Fagbami AH, Adekanle O, et al. (2015) Occult Hepatitis B Virus Infection in Nigerian Blood Donors and Hepatitis B Virus Transmission Risks. PLoS One 10(7): e0131912.
-
Opaleye OO, Oluremi AS, Atiba AB, Adewumi MO, Mabayoje OV, et al. (2014) Occult hepatitis B virus infection among HIV positive patients in Nigeria. J Trop Med 2014: 796121.
-
Igetei R, Awobusuyi JO, Wright OK, Olaleye DO (2015) Occult hepatitis B virus infection in Nigerian patients on haemodialysis. Tropical Journal of Nephrology 10(2).
-
Manzin A, Salvoni G, Bagnarelli P, Menzo S, Carloni G, et al. (1991) A single-step DNA extraction procedure for the detection of serum hepatitis B virus sequences by the polymerase chain reaction. J Virol Methods 32(2-3): 245-253.
-
N’Dri-Yoman T, Anglaret X, Messou E, Attia A, Polneau S, et al. (2010) Occult HBV infection in untreated HIV- infected adults in Cote d’Ivoire. Antivir Ther 15(7): 1029-1034.
-
Mudawi H, Hussein W, Mukhtar M, Yousif M, Nemeri O, et al. (2014) Overt and occult hepatitis B virus infection in adult Sudanese HIV patients. Int J Infect Dis 29: 65-70.
-
Fang Y, Shang QL, Liu JY, Li D, Xu WZ, et al. (2009) Prevalence of occult hepatitis B virus infection among hepatopathy patients and healthy people in China. J Infect 58(5): 383-388.
-
Nna E, Mbamalu C, Ekejindu I (2014) Occult hepatitis B viral infection among blood donors in South-Eastern Nigeria. Pathog Glob Health 108(5): 223-228.
-
Emechebe GO, Emodi IJ, Ikefuna AN, Ilechukwu GC, Igwe WC, et al. (2009) Hepatitis B virus infection in Nigeria—A review. Nigerian Medical Journal 50(1): 18-22.
-
Antar W, El-Shokry MH, Abd El Hamid WA, Helmy MF (2010) Significance of detecting anti-HBc among Egyptian male blood donors negative for HBsAg. Transfus Med 20(6): 409-413.
-
Tramuto F, Mazzucco W, Maida CM, Affronti A, Affronti M, et al. (2012) Serological pattern of hepatitis B, C, and HIV infections among immigrants in Sicily: epidemiological aspects and implication on public health. J Community Health 37(3): 547-553.
-
Li L, Chen PJ, Chen MH, Chak KF, Lin KS, et al. (2008) a pilot study for screening blood donors in Taiwan by nucleic acid amplification technology: detecting occult hepatitis B virus infections and closing the serologic window period for hepatitis C virus. Transfusion 48(6): 1198-1206.
-
Jutavijittum P, Andernach IE, Yousukh A, Samountry B, Samountry K, et al. (2014) Occult hepatitis B infections among blood donors in Lao PDR. Vox Sang 106(1): 31-
-
Maria LG, Conrado MF, Jose LL, Ingrid B (2015) Prevalence of occult hepatitis B virus infection. World J Gastroenterol 16: 12.
-
Hu LP, Liu DP, Chen QY, Harrison TJ, He X, et al. (2015) Occult HBV Infection May Be Transmitted through Close Contact and Manifest as an Overt Infection. PLoS One 10(10): e0138552.
-
Allain JP (2004) Occult hepatitis B virus infection. Transfus Clin Biol 11(1): 18-25.
-
Hairul Aini H, Omar AR, Hair-Bejo M, Aini I (2008) Comparison of Sybr Green I, ELISA and conventional agarose gel-based PCR in the detection of infectious bursal disease virus. Microbiol Res 163(5): 556-563.
-
Daef EA, Makhlouf NA, Ahmed EH, Mohamed AI, Abd El Aziz MH, et al. (2017) Serogical and Molecular Diagnosis of Occult Hepatitis B virus infection in hepatitis C Chronic Liver Diseases. Egypt J Immunol 24(1): 37-48.
-
Torbenson M, Thomas DL (2002) Occult hepatitis B. Lancet Infect Dis 2(8): 479-486.
-
Aghakhani A, Banifazl M, Kalantar E, Eslamifar A, Ahmadi F, et al. (2010) Occult hepatitis B virus infection in haemodialysis patients with isolated hepatitis B core antibody: a multicentre study. Ther Apher Dial 14(3): 349-353.
-
Hofer M, Joller-Jemelka HI, Grob PJ, Lüthy R, Opravil M, et al. (1998) Frequent chronic hepatitis B virus infection in HIV-infected patients positive for antibody to hepatitis B core antigen only. Swiss HIV Cohort Study. Eur J Clin Microbiol Infect Dis 17(1): 6-13.
-
Núñez M, Ríos P, Pérez-Olmeda M, Soriano V (2002) Lack of ‘occult’ hepatitis B virus infection in HIV-infected patients. AIDS 16(15): 2099-2101.
-
Filippini P, Coppola N, Pisapia R, Scolastico C, Marrocco C, et al. (2006) Impact of occult hepatitis B virus infection in HIV patients naive for antiretroviral therapy. AIDS 20(9): 1253-1260.
-
Lukhwareni A, Burnett RJ, Selabe SG, Mzileni MO, Mphahlele MJ, et al. (2009) Increased detection of HBV DNA in HBsAg-positive and HBsAg-negative South African HIV/AIDS patients enrolling for highly active antiretroviral therapy at a Tertiary Hospital. J Med Virol 81(3): 406-412.
-
Bloquel B, Jeulin H, Burty C, Letranchant L, Rabaud C, et al. (2010) Occult hepatitis B infection in patients infected with HIV: report of two cases of hepatitis B reactivation and prevalence in a hospital cohort. J Med Virol 82(2): 206-212.
-
Jardim RN, Gonçales NS, Pereira JS, Fais VC, Gonçales Junior FL, et al. (2008) Occult hepatitis B virus infection in immunocompromised patients. Braz J Infect Dis 12(4): 300-305.
-
Cohen Stuart JW, Velema M, Schuurman R, Boucher CA, Hoepelman AI, et al. (2009) Occult hepatitis B in persons infected with HIV is associated with low CD4 counts and resolves during antiretroviral therapy. J Med Virol 81(3): 441-445.
-
Minuk GY, Sun DF, Uhanova J, Zhang M, Caouette S, et al. (2005) Occult hepatitis B virus infection in a North American community-based population. J Hepatol 42(4): 480-485.
-
Jardi R, Rodriguez F, Buti M, Costa X, Cotrina M, et al. (2001) Role of hepatitis B, C, and D viruses in dual and triple infection: influence of viral genotypes and hepatitis B precore and basal core promoter mutations on viral replicative interference. Hepatology 34(2): 404-410.
-
Piroth L, Lafon ME, Binquet C, Bertillon P, Gervais A, et al. (2008) Occult hepatitis B in HIV-HCV coinfected patients. Scand J Infect Dis 40(10): 835-839.
-
Raimondo G, Allain JP, Brunetto MR, Buendia MA, Chen DS, et al. (2008) Statements from the Taormina expert meeting on occult hepatitis B virus infection. J Hepatol 49(4): 652-657.
-
Ghany MG, Ayola B, Villamil FG, Gish RG, Rojter S, et al. (1998) Hepatitis B virus S mutants in liver transplant recipients who were reinfected despite hepatitis B immune globulin prophylaxis. Hepatology 27(1): 213- 222.
-
Wakil SM, Kazim SN, Khan LA, Raisuddin S, Parvez MK, et al. (2002) Prevalence and profile of mutations associated with lamivudine therapy in Indian patients with chronic hepatitis B in the surface and polymerase genes of hepatitis B virus. J Med Virol 68(3): 311-318.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions