Factors Contributing to COVID-19 Vaccine Hesitancy among Taxi Drivers in Juba City-South Sudan
Introduction: Over the past few decades, vaccine hesitancy emerged as a major public health problem leading to outbreaks of communicable infections. While the development of a vaccine against COVID-19 was eagerly awaited by most of the communities at the beginning of the pandemic, skeptical voices are now becoming louder, and rising evidence shows mixed patterns with a worldwide rather decreasing trend of acceptance. The reasons for vaccine refusal are complex and differ according to geographical and cultural context. Objective: To find out factors contributing to COVID-19 vaccine hesitancy among taxi drivers in Juba City-South Sudan. Methodology: This research was a descriptive cross-sectional study designs which used quantitative research method. The study was conducted between February-May 2022. It targeted all the taxi drivers offering taxi service in formal/designated taxi park. To ensure better representation, all the designated/formal taxi parks in the three (3) payams of Juba City (Juba, Kator and Munuki) were purposely selected for the study and the numbers of the respondents were assigned equally to the three (3) taxi park. Total sample size of 384 was used and about 128 taxi drivers were interviewed in each taxi park. The daily registration lists of the taxi in the taxi parks were used as a sampling frame. Drivers were selected at a random from the sample frame using simple random sampling technique until the required number was met. A Self-administered close ended questionnaire was used to collect the data and responses from the questionnaires were manually validated and entered in excel spread sheet version 2019. It was analyzed and presented inform of tables, graphs, and pie-charts. Results: About 116 (30%) of the drivers were above the age of 35 years. Majority of the participants 376 (98%) heard about COVID-19 vaccine. Of those who heard about the COVID-19 vaccine, 201 (28%) stated that they heard through social media. When asked on their readiness to receive the COVID-19 vaccine, majority of the respondent 256 (67%) specified that they would not accept to be vaccinated if COVID-19 vaccine was offered to them. Amongst those who refused to be vaccinated, majority of the respondent 180 (26%) reported that they were concern on the adverse effects of the vaccine. Conclusion: Vaccine hesitancy is a major threat to curving down the COVID-19 pandemic. This research findings showed that majority of the respondent heard about COVID-19 vaccine using social media. Furthermore, this research established that majority of the taxi drivers would not accept to be vaccinated when the COVID-19 vaccine was offered to them due to fears of adverse effects of the vaccine; others were concern of acquiring COVID-19 infection from the vaccine itself.
Introduction
Vaccination against SARS-CoV-2, is the most desired solution to end the pandemic [1]. Multiple candidate vaccines are being developed, and some have already been authorized and deployed for mass immunization [2]. Safe and effective vaccines provide a route out of this crisis, but the development of these vaccines, while necessary, is not sufficient. For vaccines to achieve their full potential, the public also needs to be willing to be vaccinated. Sources indicated that though mass vaccination programs have already been started globally, the effectiveness of vaccination program has been affected by a hesitancy to receive the vaccines in populations [3]. While the development of a vaccine against COVID-19 was eagerly awaited by most of the communities at the beginning of the pandemic, skeptical voices are now becoming louder, and rising evidence shows mixed patterns with a worldwide rather decreasing trend of acceptance [4].
The reasons for vaccine refusal are complex and differ according to geographical and cultural context. However, concern about vaccine safety continues to be an important driver of decreased vaccine uptake in most contexts [5]. This concern is fueled by misinformation and propagated through organized antivaccine groups, social media, and celebrity endorsements. Despite a wealth of scientific data supporting the safety of currently recommended vaccines, counteracting false information to convince vaccine hesitant populations continues to be challenging. While there will always be individuals with strongly held beliefs for whom well informed discussions about vaccine safety will have little impact, it has been repeatedly demonstrated that provider recommendation strongly influences decision making around vaccines [6].
Understanding factors contributing to COVID-19 vaccine hesitancy is critical in expanding the vaccine coverage to flatten the infection curve. The Ministry of Health, Government of South Sudan started with AstraZeneca in the first phase, then later brought in J&J vaccines. The hesitancy to receive the COVID-19 vaccine may pose critical challenges in the fight against the pandemic. Unfortunately, studies related to the COVID-19 vaccine hesitancy are limited in the context of South Sudan. It even becomes vilest when it comes to studies in COVID-19 vaccine hesitancy among public transporters like the taxi drivers. At the time of conducting this study, there was only one research on COVID-19 vaccine hesitancy among South Sudanese population conducted by Udoh K [7]. However, the study did not point out factors related to COVID-19 vaccine hesitancy. Nevertheless, no study has been conducted on factors contributing to COVID-19 vaccine hesitancy among taxi drivers yet, they are always exposed to the public given the nature of their job.
To address this gap, this research assesses the factors contributing to COVID-19 vaccine hesitancy on taxi drivers in Juba City, South Sudan. The findings from this study are expected to guide and inform Ministry of Health, Health partners, health experts, and media in tailoring successful COVID-19 immunization campaigns.
Aim/Broad Objective
To find out factors contributing to COVID-19 vaccine hesitancy among taxi drivers in Juba City-South Sudan
Specific Objectives
- To establish the general understanding of the taxi driver on COVID-19 Vaccine. This objective will find out whether the taxi driver heard about COVID-19 vaccine, source(s) of information for COVID-19 vaccine and the information they heard about COVID-19 vaccine.
- To find out taxi drivers’ willingness to receive the COVID-19 Vaccine. This will help unearth issues around COVID-19 vaccine readiness among taxi drivers.
- To understand the reasons of not getting vaccinated with the COVID-19 Vaccine. This objective will comprehend the facts behind refusal of taxi drivers to get vaccinated with COVID-19 vaccine.
Research Questions
- What is your general understanding on COVID-19 vaccine?
- Are you willing to receive COVID-19 vaccine?
- What are the reasons of not getting vaccinated with the COVID-19 vaccine?
Study Design
This research was a descriptive cross-sectional study designs which used quantitative research method. The study was conducted from February-May 2022.
Study Area
Juba City is located within Juba County of Central Equatorial State, South Sudan. It borders Terekeka County to the north and Kajo-Keji and Lainya Counties to the south. The counties of Lopa/Lafon, Torit, and Magwi in Eastern Equatorial State to the east, while the counties of Mundri East and Mundri West in Western Equatorial State to the west. The River Nile flows northwards through the county and capital city.
Juba City is directly under the administration of the Juba City Council. It comprised of three (3) Blocks namely Juba
Block, Kator Block and Munuki Block. The city is located at coordinates of 4° 51’ 33.7068’’ N and 31° 34’ 16.5’’ E. The elevation of Juba is 487.079, above sea level.
The area has a tropical wet and dry climate and as it lies near the equator, temperatures are hot year-round. However, little rain falls from November to March, which is also the time of the year with the hottest maximum temperatures, reaching 42 °C (100 °F) in February. From April to October, more than 100 millimeters of rain falls per month. The annual total precipitation is nearly 1,000 mm.
Study Population
The study population comprised of all taxi drivers in Juba City. Target Respondents The target respondents included all the taxi drivers offering taxi service in formal/designated taxi park.
Inclusion Criteria
All taxi drivers running taxi service using designated/ formal cars for ferrying passengers. Taxi drivers that have been carrying taxi service for the last 12 months. Taxi drivers offering taxi service in designated/formal taxi parks.
Exclusion Criteria
Taxi drivers offering taxi services not in designated/ formal taxi car Taxi drivers offering taxi services using “racksher” Taxi drivers who offered taxi service for less than 12 months. Taxi drivers carrying taxi services in non-designated/ informal taxi park.
Sample Size Determination
The sample size was determined using Kish Leslie formula. The confidence level was taken at 95%, Margin of error 5%, Population proportion was taken at 50% since it was unknown.
2
2 Z P(1-P) N= d
Where N: The desired sample size Z: Confidence level P: Proportion of population d: Margin of Error
Sampling Methods
To ensure better representation, all the designated/ formal taxi parks in the three (3) payams of Juba City (Juba, Kator and Munuki) were purposely selected for the study. These included Juba Taxi Park, Konyo-Konyo Taxi Park and Customs Taxi Park respectively.
The number of the respondent was assigned equally to the three (3) taxi park. That means, there were 128 taxi drivers that were interviewed in each taxi park.
The daily registration list of the taxies in the three (3) taxi parks were used as a sampling frame. Drivers were selected at a random from the sample frames using simple random sampling technique until the required number was met.
Data Collection Tools
A Self-administered close ended questionnaire was used to collect the data. Respondents that were not able to fill the questionnaire were assisted by the research assistants to complete the questionnaire.
Validity and Reliability Research assistants were trained prior to data collection and the questionnaires was pretested before the actual data collection exercise commenced. This helped the researcher to adjust and modify the questioners before the actual data collection exercise begun.
Ethical considerations
Clearance for conducting this research was sought from the ethical committee of research in the National Ministry of Health, Juba-South Sudan. Approval from the Juba City Council was sought.
Written Consent was gotten from the respondents prior to interviews. Any information obtained was handled with high degree of confidentiality as there was no mentioning of people’s names but using their signatures/fingerprint on the data collection tools. Any respondent who chose to decline before or during the process of interview was free to do so.
Data Processing and Analysis
Responses from the questionnaires were manually validated and entered in excel spread sheet version 2019. It was analyzed and presented inform of tables, graphs, and pie-charts.
Demographic Data (Table1)
Findings
This chapter confers on the findings, analysis and the discussion of this research.
| Variables | Categories | Frequency (F) | Percentage (%) |
|---|---|---|---|
| Age Group | <20 | 11 | 3 |
| 20-25 | 75 | 20 | |
| 26-30 | 93 | 24 | |
| 31-35 | 89 | 23 | |
| Above 35 | 116 | 30 | |
| Sex | Male | 381 | 99 |
| Female | 3 | 1 | |
| Religion | Muslim | 65 | 17 |
| Catholic | 131 | 34 | |
| Protestant | 160 | 42 | |
| Others | 28 | 7 | |
| Education Level | Basic Level (Primary) | 201 | 52 |
| Secondary | 127 | 33 | |
| Diploma | 39 | 10 | |
| Degree | 14 | 4 | |
| Master’s degree | 3 | 1 | |
| Marital Status | Married | 266 | 69 |
| Unmarried | 108 | 28 | |
| Divorced | 7 | 2 | |
| Widow/Widower | 3 | 1 | |
| Occupation | Driver | 382 | 99 |
| Conductor | 2 | 1 | |
| Others | 0 | 0 |
Table 1: ** Demographic Data.
(Source: Primary Data) Table 1: Demographic Data.
Majority 116 (30%) of the drivers were above the age of 35 years, followed by 93 (24%) at age group between 26- 30 years while age groups 31-35, 20-25 and less than 20 years were 89 (23%), 75 (20%) and 11 (3%) respectively. Most 381 (99%) of the respondent were male and 3 (1%) were female drivers. Close to half of the driver 160 (42%) were protestant, about 131 (34%) were catholic, 65 (17%) were Muslim and 28 (7%) were from other religion. More than half 201 (52%) of the drivers had primary (Basic) education, 127 (33%) had secondary level education, 39 (10%) had Diploma, 14 (4%) had basic degree and 3 (1%) were master’s degree holders. Over half of the drivers 266 (69%) were married, 108 (28%) were unmarried, 7 (2%) were divorced and 3 (1%) were widow/widower. Most of the respondent who were interviewed were drivers 382 (99%) while 2 (1%) were bus conductors/co-drivers.
General Understanding of the Taxi Driver on Covid-19 Vaccine
Drivers who heard about COVID-19 Vaccine (Figure 1)
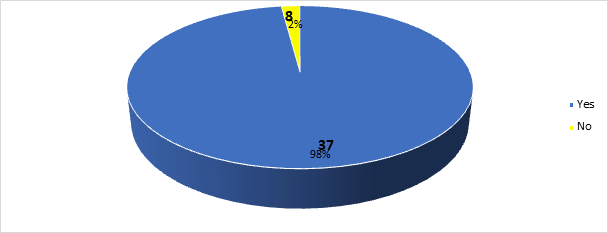
(Source: Primary Data) Figure 1: Drivers who heard about COVID-19 Vaccine (n=384).
Majority of the participants 376 (98%) heard about COVID-19 vaccine while 8 (2%) did not hear about the COVID-19 vaccine.
About 201 (28%) of the respondent stated that their source of information for COVID-19 vaccine was through social media followed social mobilizers 144 (20%), SMS 113 (16%), Radio 86 (12%), Community Leaders 67 (9%), News Papers (59 (8%) while Television (TV) 23 (3%) and other sources 18 (3%) were the least sources of information for COVID-19 vaccine.
Source (s) of Information for COVID-19 Vaccine (Figure 2)
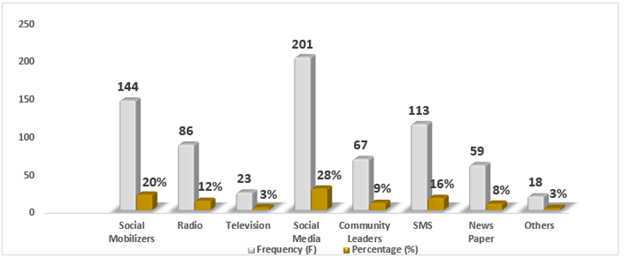
(Source: Primary Data) Figure 2: Source (s) of Information for COVID-19 Vaccine (n=711).
Information about COVID-19 Vaccine (Figure 3)
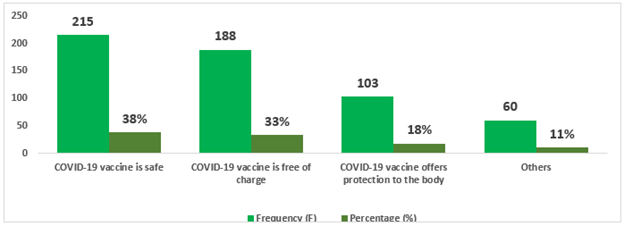
(Source: Primary Data) Figure 3: Information about COVID-19 Vaccine (n=566).
Less than half 215 (38%) participants responded that COVID-19 vaccine was safe, 188 (33%) indicated that COVID-19 vaccine was free of charge, 103 (18%) stated that
Eligibility to receive COVID-19 Vaccine (Figure 4)
COVID-19 vaccine offers protection to the body while 60 (11%) indicated other information about COVID-19 vaccine.
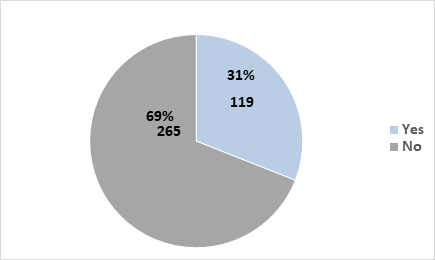
(Source: Primary Data) Figure 4: Eligibility to receive COVID-19 Vaccine (n=384).
More than half 265 (69%) of the respondent indicated that they were not eligible to receive COVID-19 Vaccine while 119 (31%) stated that they were eligible to receive COVID-19 vaccine.
Reasons for eligibility to receive COVID-19 Vaccine (Figure 5)
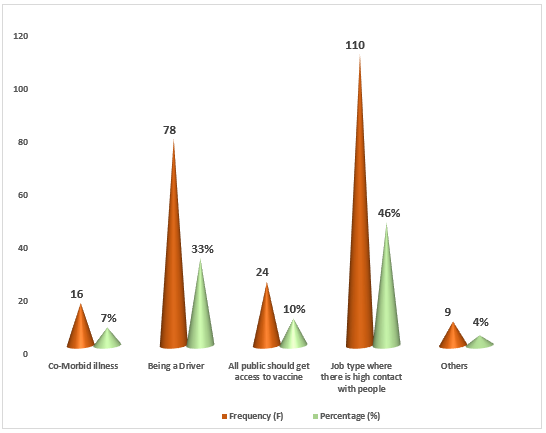
(Source: Primary Data) Figure 5: Reason (s) for eligibility to receive COVID-19 Vaccine (n=237).
Nearly half 110 (46%) of the respondent stated that they would receive COVID-19 vaccine because of the job type where there is high contact with people, about 78 (33%) indicated that they would take the COVID-19 vaccine because of being drivers while 24 (10%), 16 (7%) and 9 (4%) responded that they would receive COVID-19 vaccine because all public should get access to vaccine, co-morbid illness, and other reasons respectively.
Taxi Drivers’ Willingness to Receive the Covid-19 Vaccine
Willingness to be vaccinated if vaccine is offered (Figure 6)
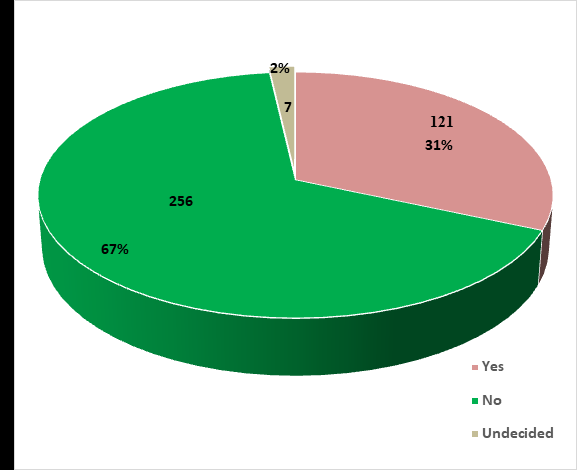
(Source: Primary Data) Figure 6: Willingness to be vaccinated if vaccine is offered (n=384).
Majority of the respondent 256 (67%) stated that they would not accept to be vaccinated if COVID-19 vaccine was offered to them while 121 (31%) indicated their willingness to receive the COVID-19 vaccine if offered. However, about 7 (2%) were undecided whether to or not to take the COVID-19 vaccine if offered.
Reasons of Not Getting Vaccinated With the Covid-19 Vaccine
Reason (s) of refusal to be vaccinated with COVID-19 Vaccine (Figure 7)
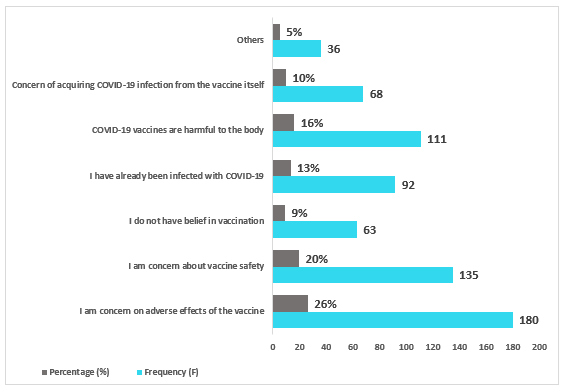
(Source: Primary Data) Figure 7: Reason (s) of refusal to be vaccinated with COVID-19 Vaccine (n=685).
Majority of the respondent 180 (26%) reported that they were concern on the adverse effects of the vaccine, some indicated that they were concern about vaccine safety 135 (20%), about 63 (9%) of the respondent reported that they do not have belief in the vaccination while 92 (13%) indicated that they had already been infected with COVID-19, COVID-19 vaccines are harmful to the body 111 (16%), concern of acquiring COVID-19 infection from the vaccine itself 68 (10%) and others 36 (5%).
Discussion
Demographic Data
Majority 116 (30%) of the respondent were above the age of 35 years, followed by 93 (24%) at age group between 26-30 years while age groups 31-35, 20-25 and less than 20 years were 89 (23%), 75 (20%) and 11 (3%) respectively. Most 381 (99%) of the respondent were male and 3 (1%) were female drivers. Close to half of the driver 160 (42%) were protestant, 131 (34%) were catholic, 65 (17%) were Muslim and 28 (7%) were from other religion. More than half 201 (52%) of the drivers had Basic (primary) education, 127 (33%) had secondary level education, 39 (10%) had Diploma, 14 (4%) had degree and 3 (1%) were master’s degree holders. Over half of the drivers 266 (69%) were married, 108 (28%) were unmarried, 7 (2%) were divorced and 3 (1%) were widow/widower. Most of the respondent who were interviewed were drivers 382 (99%) while 2 (1%) were bus conductors/co-drivers.
General Understanding of the Taxi Driver on Covid-19 Vaccine
Majority of the participants 376 (98%) heard about COVID-19 vaccine while 8 (2%) did not hear about the COVID-19 vaccine. These study findings disagreed with findings from a research conducted by Mesesle, (2021) in Ethiopia on awareness and attitude towards COVID-19 vaccination and associated factors. In their research report, less than half of the respondents 46.3% heard about COVID-19 vaccine while 53.7% did not hear about the COVID-19 vaccine. These research findings further varied from another study findings conducted by Mohamed NA, et al. [8] on Knowledge, acceptance, and perception on COVID-19 vaccine among Malaysians, in their study they found that 62.0% of the respondents had poor knowledge about COVID-19 vaccine and 38.0% had knowledge on COVID-19. Mahmud S, et al. [9], conducted a study on Knowledge, beliefs, attitudes and perceived risk about COVID-19 vaccine and determinants of COVID-19 vaccine acceptance in Bangladesh, in their findings, they indicated that about 43.75% did not heard about COVID-19 vaccine while 56.25% heard about the COVDI-19 Vaccine. These research findings were in treaty with the current findings of this study in which majority of the respondent heard about COVID-19 vaccine. The contrast and resemblance in the findings could be attributed to the level of public awareness on COVID-19 vaccine in those different countries at the time the studies were conducted. According to the researcher views, having appropriate and continuous knowledge and understanding on COVID-19 vaccine would be the only way to win peoples interest/hearts to take COVID-19 vaccine.
Of those who heard about the COVID-19 vaccine, 201 (28%) of the respondent stated that their sources of information for the COVID-19 vaccine were through social media followed by social mobilizers 144 (20%), SMS 113 (16%), Radio 86 (12%), Community Leaders 67 (9%), News Papers (59 (8%) while Television (TV) 23 (3%) and others 18 (3%) were the least sources of information for COVID-19 vaccine. These study findings were comparable to findings in a research conducted by Elgendy [10]. According to them, participants revealed that they received the information through social media 15.5%, other media 20.7%, Ministry of Health instructions 50% and Circle of acquaintances and friends 10%. Amongst those who heard about COVID-19 vaccine, when asked of the information they heard about the COVID-19 vaccine, less than half 215 (38%) participants reported that COVID-19 vaccine was safe, 188 (33%) indicated that COVID-19 vaccine was free of charge, 103 (18%) stated that COVID-19 vaccine offers protection to the body while 60 (11%) indicated other information about COVID-19 vaccine. When asked of their eligibility to receive the COVID-19 vaccine, more than half 265 (69%) of the respondent indicated that they were not eligible to receive COVID-19 Vaccine while 119 (31%) stated that they were eligible to receive COVID-19 vaccine. Of those who stated that they were eligible to receive the COVID-19 vaccine, nearly half 110 (46%) of the respondent specified that they would receive COVID-19 vaccine because of the job type where there is high contact with people, 78 (33%) indicated that they would take the COVID-19 vaccine because of being drivers while 24 (10%), 16 (7%) and 9 (4%) responded that they would receive COVID-19 vaccine because all public should get access to vaccine, co-morbid illness and others respectively. The researcher noted that the difference in understanding the level of eligibility to receive COVID-19 vaccine could be due to fallacy and lack of information on who to take the COVID-19 vaccine. Another contributing factor could have been the fact that when the COVID-19 vaccine had just been approved by the authorities for use, due to its scarcity and ability to afford the COVID-19 vaccines by the individual countries for all their populations, the first priority was given to the elderly, healthcare workers and those with underlying conditions e.g. diabetes, hypertension etc. these made people think that the vaccine was meant for those particular groups and not for the entire population.
Before people get to understand that the vaccine was for everyone, the first information had already been passed, digested, and being used by the population. Therefore, it would have been of greater help if everyone got clear information that COVID-19 vaccine was for everyone from the beginning. To set the “unseemly thoughts back to the dark,” there is immense need for collective efforts. These can only be done with the support from the Ministry of Health being at the vanguard.
Taxi Drivers’ Willingness to Receive the Covid-19 Vaccine
When asked on their willingness to receive the COVID-19 vaccine when it is offered to them, majority of the respondent 256 (67%) stated that they would not accept to be vaccinated if COVID-19 vaccine was offered to them while 121 (31%) indicated their willingness to receive the COVID-19 vaccine. However, about 7 (2%) were undecided whether to or not to take the COVID-19 vaccine if offered to them. These study findings were in contrast with research findings reported by Abebe [11], on understanding of COVID-19 Vaccine Knowledge, Attitude, Acceptance, and Determinates of COVID-19 Vaccine Acceptance among Adult Population in Ethiopia. According to them about 59 % were willing to receive the COVID-19 vaccine, about 22% respondents were out rightly not in support of the COVID-19 vaccine no matter the directive given by their governments while about 19 % were apathetic about the vaccine, although this group of people might later change their perspective to receive the vaccine or never. In a study conducted by Mahmud S, et al. [9] on Knowledge, beliefs, attitudes and perceived risk about COVID-19 vaccine and determinants of COVID-19 vaccine acceptance in Bangladesh, about 61.16% of the respondents were willing to accept/take the COVID-19 vaccine whereas 38.84% were not willing to receive the jab of COVID-19 vaccine. Among those who accepted, only 35.14% showed the willingness to take the COVID-19 vaccine immediately, while 64.86% would delay the vaccination until there were confirmed information about the vaccine’s efficacy and safety. These research findings as well deviated from the current study findings. Another Study on hesitation and refusal factors in individuals’ decision-making processes regarding Coronavirus Disease 2019 vaccination observed that 49% of the respondents were willing to be vaccinated, 23% not willing to be vaccinated and 28% were undecided [12]. These study findings were further incongruity with the current research findings in which majority of the respondent were not willing to receive COVID-19 vaccine. The oddness in these findings could still be ascribed to the level of public engagement and knowledge on COVID-19 vaccine. As highlighted earlier, at current, people still have vaccine hesitancy for vaccines that are used during routine immunization. This makes it nastiest when it comes to COVID-19 vaccines. The researcher, therefore, laments that for a successful vaccination to be conducted it is important to break the barriers to vaccination especially for the COVID-19 vaccine in which people have a lot of mistrust on vaccine product itself following the rapid production and disbursement to the market for use. That aside, to be able to win peoples interest to take vaccine especially the COVID-19 vaccine, it is important to have a “multi-stage approach”, an approach that targets every group of people implemented by various stakeholders. This strategy will help unearth the wrong believes about COVID-19 vaccine thus break vaccine hesitancy.
Reasons of not Getting Vaccinated with the Covid-19 Vaccine
Among those who refused to be vaccinated with COVID-19 vaccine, when asked of the reasons of refusal to be vaccinated when the vaccine was offered to them, majority of the respondent 180 (26%) reported that they were concern on the adverse effects of the vaccine, some indicated that they were concern about vaccine safety 135 (20%), about 63 (9%) of the respondent reported that they do not have belief in the vaccination, 92 (13%) indicated that they had already been infected with COVID-19, COVID-19 vaccines are harmful to the body 111 (16%), concern of acquiring COVID-19 infection from the vaccine itself 68 (10%) while 36 (5%) stated other reasons. These findings were like research conducted by Gbeasor Komlanvi FA, et al. [13] on Prevalence and factors associated with COVID-19 vaccine hesitancy in Togo. In their research they pointed out that of those who refused to be vaccinated, 59.8% were not confident in the vaccine and 40.2% were afraid of vaccine adverse effects. Not only that, but the current study findings were also related to a study done by Kollamparambil U [14], on COVID-19 vaccine intentions in South Africa: health communication strategy to address vaccine hesitancy, nearly a third (31%) reported being worried about side effects, 21% don’t believe the vaccine will be effective, 18% did not trust the vaccines or report being against vaccines in general, 14% reported being afraid or expressed feeling of being unsure of the vaccine safety. Cerda AA [12], studied hesitation and refusal factors in individuals’ decision-making processes regarding a Coronavirus Disease 2019 vaccination in Chile. In their findings, they noted that 40% of the participants indicated concerns about vaccine’s side effect and risks, lack of vaccine knowledge (24%), Will wait until there are others vaccinated 10%, fear of origin of the vaccine 8%, the vaccine probable cost 7% and lack of vaccine effectiveness 4%. These findings were in consistent with the findings of the current research. According to the researcher, the similitude in the findings could be attributed to lack or inadequate information on COVID-19 vaccine safety which was not clearly tailored to the communities based on their misconception/believes which could have helped to confiscate the fears about the COVID-19 vaccine. Secondly, there could have been insufficient community engagement and use of non-respectful people in the communities who increased the gap of community understanding on COVID-19 vaccine by creating or generating irrelevant information about COVID-19 vaccines. To address these gaps, use of credible and trusted local messenger would help expand the knowledge and understanding about COVID-19 vaccine consequently breaking vaccine hesitancy. Also setting up of a social and traditional media monitoring system to access key channels, communities, and conversations, including free monitoring and analytical tools would greatly be of importance to address some of the issues related to vaccine hesitancy.
Conclusion
Vaccine hesitancy is an important underlying and/ or direct public health threat to curbing the COVID-19 pandemic. The factors that lead to vaccine hesitancy or refusal are complex and a good understanding of local barriers to and concerns about vaccination is critical to develop tailored interventions. The findings of this research established that majority of the respondent heard about COVID-19 vaccine using social media. However, most of the respondents stated that they were not eligible to receive COVID-19 vaccine but among those who indicated that they were eligible to get the vaccine, majority itemized that they would receive the COVID-19 vaccine because of the job type where there is high contact with people, while co-morbid illnesses and being a driver were among other reasons to take the COVID-19 vaccine. Not only that, but this research also further recognized that majority of the taxi drivers would not accept to be vaccinated when the vaccine was offered to them due to fears of adverse effect of the vaccine, some indicated that they were concern about vaccine safety, others reported that they do not have belief in the vaccination while others indicated concern of acquiring COVID-19 infection from the vaccine itself among other reasons.
Acknowledgement
This research report is dedicated to my wife Mrs. Mary Sura, my dear father Mr Lukajo Felix, Mother Mrs. Tamara Muding, my brothers and their family members, my sisters and not forgetting my friends. It was all through your inspiration, guidance and support that made me reach this milestone. On a special note, I also want to thank my supervisor Dr. Beenish Nazir for her immense support in guiding me through the whole research process. Above all, I also want to give thanks to God Almighty for his protection and guidance through the whole academic period.
References
-
Lurie N, Saville M, Hatchett R, Halton J (2020) Developing Covid-19 Vaccines at Pandemic Speed. N Engl J Med 382(21): 1969-1973.
-
MacKenna B, Curtis HJ, Morton CE, Inglesby P, Walker AJ, et al. (2021) Trends, regional variation, and clinical characteristics of COVID-19 vaccine recipients: a retrospective cohort study in 23.4 million patients using OpenSAFELY.
-
Rozek LS, Jones P, Menon A, Hicken A, Apsley S, et al. (2021) Understanding Vaccine Hesitancy in the Context of COVID-19: The Role of Trust and Confidence in a Seventeen-Country Survey. Int J Public Health 66: 636255.
-
Salali GD, Uysal MS (2020) COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol Med 19: 1-3.
-
Larson HJ, Jarrett C, Eckersberger E, Smith DM, Paterson P, et al. (2014) Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature, 2007-2012. Vaccine 32(19): 2150-2159.
-
Smith LE, Amlot R, Weinman J, Yiend J, Rubin GJ, et al. (2017) A systematic review of factors affecting vaccine uptake in young children. Vaccine 35(45): 6059-6069.
-
Udoh K (2022) COVID-19 Vaccine Hesitancy in South Sudan; What Lessons Can be Learned From Angola’s Success Story? Am J Health Promot 36(3): 579-581.
-
Mohamed NA, Solehan HM, Mohd Rani MD, Ithnin M, Che Isahak CI, et al. (2021) Knowledge, acceptance and perception on COVID-19 vaccine among Malaysians: A web-based survey. PLoS One 16(8): e0256110.
-
Mahmud S, Mohsin M, Khan IA, Mian AU, Zaman MA, et al. (2021) Knowledge, beliefs, attitudes and perceived risk about COVID-19 vaccine and determinants of COVID-19 vaccine acceptance in Bangladesh. PLoS One 16(9): e0257096.
-
Elgendy MO, Abdelrahim MEA (2021) Public awareness about coronavirus vaccine, vaccine acceptance, and hesitancy. J Med Virol 93(12): 6535-6543.
-
Abebe H, Shitu S, Mose A (2021) Understanding of COVID-19 Vaccine Knowledge, Attitude, Acceptance, and Determinates of COVID-19 Vaccine Acceptance Among Adult Population in Ethiopia. Infect Drug Resist 14: 2015-2025.
-
Cerda AA, Garcia LY (2021) Hesitation and Refusal Factors in Individuals’ Decision-Making Processes Regarding a Coronavirus Disease 2019 Vaccination. Front Public Health 9: 626852.
-
Gbeasor-Komlanvi FA, Afanvi KA, Konu YR, Agbobli Y, Sadio AJ, et al. (2021) Prevalence and factors associated with COVID-19 vaccine hesitancy in health professionals in Togo, 2021. Public Health Pract (Oxf) 2: 100220.
-
Kollamparambil U, Oyenubi A, Nwosu C (2021) COVID19 vaccine intentions in South Africa: health communication strategy to address vaccine hesitancy. BMC Public Health 21(1): 2113.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions