Semen Infection Associated Male Infertility and Role of Assisted Reproductive Techniques: A Review
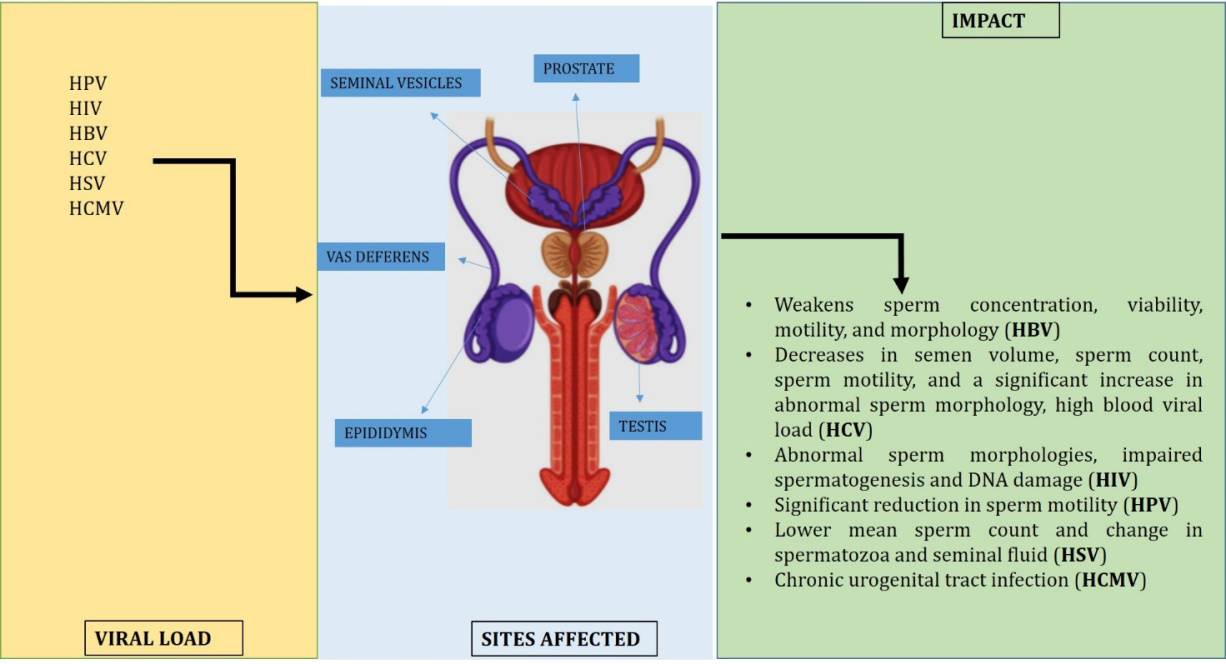
Recent research has revealed that pathogens in the semen and in the genital tract play a significant role in male infertility. The infection of viruses like Human Immunodeficiency Virus (HIV), Hepatitis B virus (HBV), Hepatitis C virus (HCV), Human Papilloma Virus (HPV), Herpes-Simplex Virus (HSV), and Human Cytomegalovirus (HCMV) may have a significant impact on male infertility. These infections may lead to temporary or permanent infertility, hormonal impairment, testicular malfunction, or abnormal spermatogenesis. This review is looking into the mechanism of viral infections and their effects on male fertility. The current review also focuses on defining the role of ARTs (Assisted Reproductive Techniques) in the occurrence and management of viral load of the male reproductive system.
Introduction
Healthy reproductive life is one of the most vital aspects of human health. Its management is also essential for the overall health of society. Multiple bio-social factors affect the reproductive performances of both males and females and lead to infertility. Infertility and associated problems distress one in seven couples, which account for approximately 8-12% of couples worldwide [1]. About 40–50% of all infertility cases are due to “male factor” infertility [2].
Many studies have supported that different factors reversibly or irreversibly influence male fertility [3]. These factors include varicocele, testicular failure, endocrine dysfunction, genital tract infection, testicular disturbances, testicular cancer, hormonal disturbances, retrograde ejaculation, prolonged exposure to heat, obesity, older age, smoking, alcohol, heavy metals, pesticides, oxidative stress, genetic factors, different environmental and nutritional factors. Recently, idiopathic cases, hypo-gonadal patients, and infertile men with other associated male factor infertility causes have significantly increased [4]. Research on male infertility has revealed that pathogens in the semen and in the genital tract play a significant role in altering fertility outcomes [5]. It is reported that genital tract infections significantly induce male infertility, and out of total male infertility, 15-20% is contributed to such conditions [6]. Depending upon the modes of infection, the pathogenesis may be in various forms. Infections in the urethra and male accessory reproductive glands also adversely affect males’ reproductive functions [7]. The infections may also lead to temporary or permanent infertility, hormonal impairment, testicular malfunction, or abnormal spermatogenesis [3].
The manifestation of the infections in the male is mostly asymptomatic and leads to poor sperm quality. In literature, it was reported that viral infection is one of the most common causes of chronic male infertility [8, 9]. The common viruses are the human immunodeficiency virus (HIV), Hepatitis B (HBV), and Hepatitis C (HCV) virus [8]. However, a review by Gorolla et al. suggested that apart from HIV, HBV, and HCV, other viruses like Human Papilloma Virus (HPV), Herpes- Simplex Virus (HSV), and Human Cytomegalovirus (HCMV)) may have a significant impact on male infertility [9]. Based on these facts, we are reviewing evidences for the effects of viral load on male infertility. The current review will look into the mode of different viral infections and their impact on male fertility. We are also reviewing the role of assisted reproductive techniques (ARTs) in the occurrence and management of the viral load of the male reproductive system.
Materials and Methods
A literature review was performed till June 2021 on semen infection, viral load and its mechanism of infection, and the role of assisted reproductive techniques. Original research articles, case reports, and review articles were considered for the current review purpose. PubMed, Medline, Scopus, Web of Science, Google Scholar, and other available online sources were searched using the keywords: semen infection and virus, HIV and sperm alteration, sperm viral infection and infertility, herpes virus, among infertile couples, semen infection, and ART. The titles, contents, and abstracts were thoroughly screened to find relevant articles which are eligible for this review. Furthermore, the cross- references cited in the literature were also searched to identify further important studies.
Viral Load and Male Fertility
Various pathogens (virus, bacteria, fungi and more) are found in human semen and may cause severe infection. The empirical evidence showed that reproductive micro biomes could significantly affect male’s and females’ reproductive function and performance [10]. Previous studies have also shown that urogenital infections are mostly asymptomatic. Their manifestation is increasingly difficult to detect [11, 12]. Most of these infections are sexually transmitted and may play a critical role in altering fertility outcomes. To facilitate male infertility, viral infections migrate via the urethra or enter the reproductive tract through the bloodstream (Figure 1). They affect the male reproductive tract cells by causing toxicity through immunological or local inflammatory reactions. The cells specific manifestation of the infections can occur, where HPV likely to infect epithelial cells, HSV to nerve cells and HIV and HCMV to WBC’s [13].
Hepatitis B Virus (HBV)
Hepatitis B, a circular, double-stranded DNA virus enclosed in an envelope consisting of three proteins known as L (large), M (Medium), and S (Small), all together results in the formation of HBsAg surface antigen (Australia antigen) [12]. HBV infection is found in both the somatic and germ cells [14]. As a result of semen infection, HBV passes through the blood-testis barrier and integrates itself into the male genome. HBV virus transmission occurs vertically and horizontally through parenteral, perinatal and sexual routes [15]. A link found between the pre-S1 domain in envelop protein L of HBV and the target cell identification suggests a possible HBV infection mechanism [16]. The impact of HBV on human sperm is adverse. HBV damage spermatozoa and weakens sperm concentration, viability, motility, and morphology [17]. A study in 151 male patients chronically infected with HBV reported that the combination of serum HBV DNA and HBeAg are useful predictors of HBV DNA’s presence in semen in HBV chronically infected men from infertile couples [18]. The probable cause of the reduction in sperm motility is the co-incubation of HBV and human sperm that induces a loss of sperm mitochondrial membrane [19]. All these causes may induce male infertility by damaging sperm quality and quantity.
Hepatitis C Virus (HCV)
HCV is a single-stranded positive-sense RNA virus of the Flaviviridae family and enveloped with a capsid [20]. Its transmission occurs mainly through blood and plasma derivatives by the parenteral route and sexual contact [21]. The HCV infection mechanism involves E1 and E2 HCV envelops glycoproteins that interact with their respective receptors and integrate into the sperm cell [22]. CD81 has been the most common out of many HCV receptors, which binds with the HCV E2 glycoprotein, and the hyper variable regions of the virus modulate this binding process. Many other receptors include LDL-R (low-density lipoprotein receptors), DC-SIGN, glycosaminoglycans (GAG), human scavenger receptors etc., have been reported [23]. This virus also has adversely affected sperm quality and quantity. A study observed substantial decreases in semen volume, sperm count, sperm motility, and a significant increase in abnormal sperm morphology compared to the non-infected [24]. Another study reported HCV-RNA in the semen of infectious males having high blood viral load [25].
Moretti, et al. reported the presence of HCV in semen affecting sperm morphology and motility. Moreover, the HCV semen infection increases sperm diploidy and reduces fertility index [26]. Still, there are fewer studies that give significantly concrete evidence about the HCV semen infection mechanism. However, the presence of HCV in semen is confirmed so that further studies may reveal more information.
Human Immunodeficiency Virus (HIV)
HIV is a double-stranded RNA virus of the Retroviridae family [27]. It can be transmitted from infected individuals through blood, sexual intercourse and perinatal transmission [28, 29]. HIV got two main strains; HIV-1 (common type) and HIV-2 (uncommon and less infectious type). HIV-1 proviral DNA has been detected in monocyte, lymphocyte, and macrophages cells of semen [5]. A study by Ceballos, et al. reported that leukocytes are the primary source of HIV- 1 infection [30]. There are multiple reproductive diseases associated with HIV-1 infection. During HIV-1 infection, chronic orchitis with progressive hypogonadism arises [31]. Low sperm concentration is associated with a high percentage of abnormal sperm morphologies, impaired spermatogenesis and DNA damage [32]. Pavili, et al. has also reported sperm abnormality and leukocytospermia among AIDS patients [33]. Cardona‐Maya et al. and Ceballos, et al. suggested that human spermatozoa may integrate with various HIV receptors such as glycoprotein ( gp120), mannose receptors, DC-SIGN, Gal-AAG, and heparan sulfate [8, 30]. Furthermore, Zea-Mazo, et al. reported that spermatozoon carrying HPV DNA has little chance of conception [12].
Human Papilloma Virus (HPV)
HPV, a double-stranded non‐enveloped DNA virus, is one of the most commonly found sexually transmitted infections globally [34]. The transmission is primarily through a sexual route, i.e., vaginal, anal, or oral sex with an infected person. This infection is asymptomatic. However, HPV can be detected in semen and a urethral swab of asymptomatic men [35]. Foresta, et al. reported the presence of HPV in the sperm head, which can be visualized after carrying out FISH (Fluorescence in situ hybridization) for infected males [36]. It can also be localized in exfoliated cells of sperm. Patients with HPV infection have a higher risk of infertility [37]. Jeršovienė, et al. reported that HPV infection was more frequent in men with abnormal sperm parameters [38]. Till now, more than 200 types of HPV have been reported, of which at least 12 are known as high-risk types [34]. Among couples undergoing IVF treatment, high-risk HPV-52 was the most common genotype. Previous studies have reported an association between HPV semen infection and decreased sperm motility [9, 39]. With the help of immunofluorescence and flow cytometry analyses of the sperm exposed to HPV16 capsid and the infected localized sperm, Foresta, et al. showed that syndecan-1 protein is expressed at the central part of the sperm head [40]. Foresta et al. also observed a significant reduction in sperm motility among HPV-infected patients [41].
Herpes-Simplex Virus (HSV)
HSV, a double-stranded DNA virus, is one of the most commonly found viruses coexisting with the human population for ages [42]. It is transmitted through the skin and mucosal contact during sexual intercourse [43]. In the HSV group, the two closely related variants HSV-1 and HSV-2, primarily located in the genitals, may significantly affect male fertility. The infection of these two HSV variants diminishes sperm count. It is reported that HSV DNA reduces sperm concentration and affects sperm motility [44]. Spear describes that HSV binds with Nectin-1 immunoglobulin and found various cell lines such as epithelial, endothelial, neurons, fibroblasts. This study also revealed the expression of Nectin-1 on spermatid [43]. A study found a significant association of HSV-2 with hematospermia and a lower mean seminal volume. They also reported that HSV-1 infection is associated with a lower mean sperm count [45]. This study has also revealed that HSV infection causes a change in spermatozoa and seminal fluid in the male partner, influencing fertility.
Human Cytomegalovirus (HCMV)
HCMV is a linear double-stranded DNA virus of the herpesvirus family, with a high prevalence rate. Its transmission occurs mainly through oral, respiratory, and sexual routes [9]. It stays lifelong inside the host’s body. Isaacson et al. found that, in adhesion and genetic expression of HCMV in the host cell, the role of epidermal growth factor receptor (EGFR) is critical [46]. Further, various cell integrins such as α2β1, αVβ3, and α6β1 bind with the N- terminal region of the HCMV fusion protein (gB) and facilitates entry of virus in the host cell [47]. Moreover, β2–microglobulin has also been described as a common receptor of HCMV, which helps cell adhesion and entry (Table 1).
| HIV | HBV | HCV | HPV | HCMV | HSV | |
|---|---|---|---|---|---|---|
| Genetic material | ds-RNA | ds-DNA | ss-RNA | ds-DNA | ds-DNA | ds-DNA |
| Mode of Transmission | Vertical and horizontal | Vertical and horizontal | Vertical and horizontal | Vertical | Vertical and horizontal | horizontal |
| Mechanism of infection | 1. It is detected in monocyte, lymphocyte, and macrophages cells of semen. | 1. It passes through the blood-testis barrier and integrates itself into the male genome. | 1. E1 and E2 HCV envelope glycoproteins interact with their respective receptors and integrate into the sperm cell | 1. HPV16 capsid affects sperm head and exfoliated cells of sperm. | 1. β2-microglobulin has also been described as a common receptor of HCMV, which helps cell adhesion and entry. | 1. HSV binds with Nectin-1 immunoglobulin and is also found in the various cell such as epithelial, endothelial, neurons, fibroblasts. |
| Mechanism of infection | 2. Leucocytes are considered the primary source of infection. | 1. It passes through the blood-testis barrier and integrates itself into the male genome. | 1. E1 and E2 HCV envelope glycoproteins interact with their respective receptors and integrate into the sperm cell | 1. HPV16 capsid affects sperm head and exfoliated cells of sperm. | 1. β2-microglobulin has also been described as a common receptor of HCMV, which helps cell adhesion and entry. | 1. HSV binds with Nectin-1 immunoglobulin and is also found in the various cell such as epithelial, endothelial, neurons, fibroblasts. |
| Impact | 1. Orchitis | 1.Damage spermatozoa | 1. Reduces semen volume, sperm count, sperm motility | 1. Affects sperm morphology and vitality. | 1. Negatively influences sperm parameters. | 1. Low sperm count. |
| Impact | 2. Leukospermia | 2.Reduces sperm motility | 2. Sperm diploidy and reduces fertility index | 2. Genital warts (penile and anal). | 2. Viral DNA integrates into spermatozoa | 2. Reduces sperm motility. |
| Impact | 3. Low testosterone level. | 3.Increases sperm apoptosis and necrosis | 2. Sperm diploidy and reduces fertility index | 3. It is affecting sperm motility and causing Asthenozoospermia. | 3. Germs cells get infected. | 3. The occurrence of ulcers. |
| Impact | 4. Impairment of sperm morphology and spermatogenesis | 4. Mutation due to HBV DNA integration into sperm. | 2. Sperm diploidy and reduces fertility index | 3. It is affecting sperm motility and causing Asthenozoospermia. | 3. Germs cells get infected. | 4. Prostatic and epididymal functions are disturbed. |
| Impact | 5. Sperm DNA damage | 4. Mutation due to HBV DNA integration into sperm. | 2. Sperm diploidy and reduces fertility index | 3. It is affecting sperm motility and causing Asthenozoospermia. | 3. Germs cells get infected. | 4. Prostatic and epididymal functions are disturbed. |
| Impact | 6. Hypogonadism | 4. Mutation due to HBV DNA integration into sperm. | 2. Sperm diploidy and reduces fertility index | 3. It is affecting sperm motility and causing Asthenozoospermia. | 3. Germs cells get infected. | 4. Prostatic and epididymal functions are disturbed. |
| Impact | 7. Erectile dysfunction | 4. Mutation due to HBV DNA integration into sperm. | 2. Sperm diploidy and reduces fertility index | 3. It is affecting sperm motility and causing Asthenozoospermia. | 3. Germs cells get infected. | 4. Prostatic and epididymal functions are disturbed. |
Table 1: Mechanism and impact of viruses on fertility parameters.
This molecule also increases virus infectivity by suppressing the expression of class 1 HLA [48]. However, sexual transmission of the HCMV virus is not frequent. Eggert-Kruse, et al. [49] reported its presence in the genital tract of sub fertile males. The appearance of the virus in semen suggests genital tract infection. Many studies have pointed out the significant role of HCMV in male infertility [49]. A high prevalence of HCMV infection was reported among infertile men than fertile men [50]. This study also pointed out the importance of HCMV infection in male infertility. Another survey by Naumenko, et al. reported the association of HCMV with chronic urogenital tract infection that may lead to permanent sterility in males [51].
Assisted Reproductive Techniques (ART) and viral load
In assisted reproductive techniques (ART), sexually trans- mitted diseases (instigated primarily by viruses) are a sig- nificant threat. Various preventive measures are necessary to minimize or remove the specimens’ viral load. Most of the literature reported concern regarding gamete banking and donation as it may result in cross-contamination during as- sisted reproductive techniques among patients [52].
HBV and ART
Berry, et al. suggests that Hepatitis B contamination may occur during artificial insemination [53]. The sperm- mediated HBV genes can replicate and express themselves in early embryonic cells [54]. A Chinese study reported that HBV infection in men is associated with poor sperm quality and worse ICSI and embryo transfer outcomes [55]. In such a case, for patients undergoing IVF or ICSI, HBV screening is a must. Seronegative partners must be vaccinated against HBV in couples that are discordant with HBV infection. Once the anti-hepatitis B surface antibody (HBsAb) of the vaccinated partner is positive, fertility treatments may be started. Once the female partner is vaccinated against HBV, modified sperm washing to minimize viral load is unnecessary [56].
HCV and ART
Devaux, et al. suggested that the possibility of HCV transmission during IVF cannot be ignored [57]. HCV-RNA can be found in non-sperm cells and seminal plasma but not in spermatozoa [58]. A study by the same author suggested that it is unnecessary to perform nested PCR to detect HCV RNA since routine technical means can eliminate the virus [59]. However, the possible presence of HCV in semen implies a potential risk of nosocomial contamination. Thus sperm washing should be performed for each semen sample of HCV patients before ART [58]. If any one of the partners is infected with HCV (HCV RNA positive), to reduce the infected partner’s viral load, treatment with tribavirin (ribavirin) and Pegasys (peginterferon alfa 2a) must be considered before fertility treatment [60].
HIV and ART
For HIV serodiscordant couples preparing for family planning, assisted reproduction techniques may be a better option to prevent vertical viral transmission. Nicopoullos, et al. demonstrated that the presence of HIV infection significantly impairs sperm parameters [61]. Reproductive assistance to HIV-discordant couples can make a significant impact on the prevention of viral transmission. Here the spermatozoa of HIV-positive males can be used for IVF or ICSI only after evaluating the semen quality. Before using, the semen is washed off through the gradient technique to reduce the viral load [62]. Anti-retroviral therapy decreases viral load in the semen and improves fertility outcomes [61].
HPV and ART
HPV can be detected in the placenta through ascending infection from the cervix and the sperm [63]. Clinical analysis by Spandorfer, et al. reported a significant reduction in pregnancy outcomes among the HPV-positive females undergoing IVF [64]. A retrospective study by Depuydt, et al. [65] reported a prevalence of 11% for HPV per IUI (Intrauterine Insemination) cycle. This study also reported a lower fertility rate among women with HPV infection [65]. Modified swim-up and heparinase III methods have been proposed to reduce the risk of HPV infection during ART. The method helps in removing the HPV DNA from semen without degrading quality [66]. Sperm wash may reduce the viral load on semen from HPV-infected men, as HPV remains suspended on semen and infected epithelial cells as a cell-free virus [56]. A recent study has suggested that hyaluronidase treatment can remove HPV virions bound to spermatozoa [67].
HSV and ART
A negative influence of HSV-infected male gametes is seen at the early stages of embryo development and decreases preg- nancy achievement frequency during assisted reproduction techniques (ART) [68]. Studies of in vitro incubation of se- men with HSV-2 showed no interaction between virus and sperm, but the virus remains in the seminal fluid [9]. In acute infection, the risk of HSV-2 contamination increases if sperm is collected from the testis, where it gets infected from blood and interstitial tissues [69]. Though in ART, the exact role of HSV is yet to be unveiled, the transmission of herpes simplex virus (HSV) may impair the success of assisted reproductive techniques.
HCMV and ART
In ART, the donors’ semen is screened to detect primary infection from HCMV because, during pregnancy, this infection may exhibit serious complications upon the fetus/neonate [70]. In infected males, sperm washing is done to reduce the viral load. However, in ICSI, complete removal of viral load is impossible [69]. Identification of HCMV via rapid antibody testing (a serological method) may be helpful in the prevention of HCMV transmission during ART [9]. Insemination with semen from a CMV- positive man is acceptable when the female partner is also CMV seropositive [49]. Despite the risk of superinfection, the neonate’s infection rate with CMV is around 1%, and such a newborn does not exhibit substantial abnormalities or illness [70].
For most of the above viruses, sperm washing is considered one of the best tools for eradicating viral loads during ARTs in male infertility cases. A study by Molina I, et al. [71] concluded that sperm washing and intracytoplasmic sperm injection (ICSI) are safe and effective options for reducing the risk of viral transmission among infertile couples. Another study by Garolla, et al. discussed the role of targeted sperm washing for each sperm infection. The screening of viral infection is strongly recommended to avoid viral transmission and improve ARTs or spontaneous fertility outcomes among male infertile patients [9]. Another triple gradient semen wash technique has been described as a highly reliable technique for removing viral load [72]. This study reported that triple gradient-based sperm selection, coupled with extensive centrifugation, is highly beneficial for HIV removal. This technique provides lower than reported post-wash positive tests while maintaining high pregnancy rates in assisted reproduction cycles. However, this study also suggested that despite extensive personnel training and the washing protocol’s effectiveness, a post-wash HIV test on semen is required to identify residual positive samples. Foresta, et al. studied the efficiency of three sperm washing protocols in removing human papillomavirus (HPV)-infected cells from semen samples of infertile patients. They evaluated the sperm parameters and the presence of HPV in semen samples before and after procedures of sperm selection. This study demonstrated that conventional sperm washing before sperm selection rarely eliminates HPV infection in sperm [40]. The evidence, as mentioned above, suggests that sperm washing is the best method in the present scenario; however, it is not effective in removing viral load in semen samples.
We still need comprehensive research to find an alternative approach to diagnose and treat male infertility even before ARTs administration.
Conclusion
The viruses are very ambiguous to physical and chemical factors and are mostly asymptomatic. Unlike other pathogens, viral infection causes an inflammatory response and leads to immune suppression. So, various viruses may cause multiple infections at one time [73]. Current literature shows that virus-mediated urogenital infections are mostly asymptomatic. Moreover, their manifestation is increasingly challenging to detect. Most of these infections are sexually transmitted and may play a critical role in altering fertility outcomes of all infertility cases; approximately 40–50% is due to “male factor” infertility. Even sperm washing, the best method present in the current scenario in ARTs is ineffective in removing viral load in semen samples. We need to find effective strategies to detect and remove the viral load from semen to endure male fertility.
Further, while dealing with male infertility, viral infections are strenuous to manage in the individual and community. It may be because of the lack of knowledge and awareness for male infertility in healthcare management. More than this, people’s social stigma for a male having fertility issues is also a severe problem. However, it was recently observed that males opt for infertility treatments, which is a very constructive sign. Before ARTs administration, to avoid any illness or defects in the embryo, viruses’ screening should be prioritized. This screening is also a must to prevent male infertility and viral transmission among partners. The healthcare experts’ recommendation will lead to timely diagnosis and intervention to prevent the viral load in semen so that the healthy sperm can contribute to the origin of a healthy new life.
References
-
Stojanov M, Baud D, Greub G, Vulliemoz N (2018) Male infertility: the intracellular bacterial hypothesis. New Microbes New Infect 26: 37-41.
-
Kumar N, Singh AK (2015) Trends of male factor infertility, an important cause of infertility: A review of literature. J Hum Reprod Sci 8(4): 191-196.
-
Naz M, Kamal M (2017) Classification, causes, diagnosis and treatment of male infertility: a review. Oriental Pharmacy and Experimental Medicine 17(2): 89-109.
-
Fallara G, Cazzaniga W, Boeri L, Capogrosso P, Candela L, et al. (2021) Male factor infertility trends throughout the last 10 years: Report from a tertiary‐referral academic andrology centre. Andrology 9(2): 610-617.
-
Gimenes F, Souza RP, Bento JC, Teixeira JJ, Maria-Engler SS, et al. (2014) Male infertility: a public health issue caused by sexually transmitted pathogens. Nat Rev Urol 11(12): 672-687.
-
Weidner W, Krause W, Ludwig M (1999) Relevance of male accessory gland infection for subsequent fertility with special focus on prostatitis. Hum Reprod Update 5(5): 421-432.
-
Marconi M, Pilatz A, Wagenlehner F, Diemer T, Weidner W, et al. (2009) Impact of infection on the secretory capacity of the male accessory glands. Int Braz J Urol 35(3): 299-309.
-
Cardona-Maya W, Velilla PA, Montoya CJ, Cadavid Á, Rugeles MT, et al. (2011) In vitro human immunodeficiency virus and sperm cell interaction mediated by the mannose receptor. J Reprod Immunol 92(1-2): 1-7.
-
Garolla A, Pizzol D, Bertoldo A, Menegazzo M, Barzon L, et al. (2013) Sperm viral infection and male infertility: focus on HBV, HCV, HIV, HPV, HSV, HCMV, and AAV. Journal of reproductive immunology 100(1): 20-29.
-
Rowe M, Veerus L, Trosvik P, Buckling A, Pizzari T, et al. (2020) The reproductive microbiome: an emerging driver of sexual selection, sexual conflict, mating systems, and reproductive isolation. Trends Ecol Evol 35(3): 220-234.
-
Solomon M, Henkel R (2017) Semen culture and the assessment of genitourinary tract infections. Indian J Urol 33(3): 188-193.
-
Zea-Mazo JW, Negrette-Mejía YA, Cardona-Maya W (2010) Virus of sexual transmission: semen and virus relationship. Actas Urol Esp 34(10): 845-853.
-
Kushwaha B, Gupta G (2017) Sexually transmitted infections and male infertility: Old enigma, New Insights. In: Singh R, et al. (Eds.), Male Infertility: Understanding, Causes and Treatment. Springer, Singapore, pp: 183-212.
-
Hu XL, Zhou XP, Qian YL, Wu GY, Ye YH, et al. (2011) The presence and expression of the hepatitis B virus in human oocytes and embryos. Hum Reprod 26(7): 1860- 1867.
-
Qian WP, Tan YQ, Chen Y, Peng Y, Li Z, et al. (2005) Rapid quantification of semen hepatitis B virus DNA by real-time polymerase chain reaction. World journal of gastroenterology 11(34): 5385-5389.
-
Le Seyec J, Chouteau P, Cannie I, Guguen-Guillouzo C, Gripon P, et al. (1999) Infection process of the hepatitis B virus depends on the presence of a defined sequence in the pre-S1 domain. J Virol 73(3): 2052-2057.
-
Oger P, Yazbeck C, Gervais A, Dorphin B, Gout C, et al. (2009) Adverse effects of hepatitis B virus on sperm motility and fertilisation ability during IVF. Reprod Biomed Online 23(2): 207-212.
-
Fei QJ, Yang XD, Ni WH, Pan CS, Huang XF, et al. (2015) Can hepatitis B virus DNA in semen be predicted by serum levels of hepatitis B virus DNA, HB eAg, and HB sAg in chronically infected men from infertile couples? Andrology 3(3): 506-511.
-
Zhou XL, Sun PN, Huang TH, Xie QD, Kang XJ, et al. (2009) Effects of hepatitis B virus S protein on human sperm function. Hum Reprod 24(7): 1575-1583.
-
Lamps LW, Kakar S (2016) Diagnostic pathology: hepatobiliary and pancreas. Elsevier, Philadelphia.
-
Genesca J, Esteban JI, Alter HJ (1991) Blood-borne non-A, non-B hepatitis: hepatitis C. Semin Liver Dis 11(2): 147- 164.
-
Bartosch B, Dubuisson J, Cosset FL (2003) Infectious hepatitis C virus pseudo-particles containing functional E1–E2 envelope protein complexes. J Exp Med 197(5): 633-642.
-
Roccasecca R, Ansuini H, Vitelli A, Meola A, Scarselli E, et al. (2003) Binding of the hepatitis C virus E2 glycoprotein to CD81 is strain specific and is modulated by a complex interplay between hypervariable regions 1 and 2. J Virol 77(3): 1856-1867.
-
Hofny ER, Ali ME, Taha EA, Nafeh HM, Sayed DS, et al. (2011) Semen and hormonal parameters in men with chronic hepatitis C infection. Fertil Steril 95(8): 2557- 2559.
-
Levy R, Bourlet T, Maertens A, Salle B, Lornage J, et al. (2002) Pregnancy after safe IVF with hepatitis C virus RNA-positive sperm: Case report. Hum Reprod 17(10): 2650-2653.
-
Moretti E, Federico MG, Giannerini V, Collodel G (2008) Sperm ultrastructure and meiotic segregation in a group of patients with chronic hepatitis B and C. Andrologia 40(3): 173-178.
-
Levy JA (1993) Pathogenesis of human immunodeficiency virus infection. Microbiol Rev 57(1): 183-289.
-
Galvin SR, Cohen MS (2004) The role of sexually transmitted diseases in HIV transmission. Nat Rev Microbiol 2(1): 33-42.
-
McGowan JP, Shah SS (2000) Prevention of perinatal HIV transmission during pregnancy. J Antimicrob Chemother 46(5): 657-668.
-
Ceballos A, Remes Lenicov F, Sabatté J, Rodríguez Rodrígues C, Cabrini M, et al. (2009) Spermatozoa capture HIV-1 through heparan sulfate and efficiently transmit the virus to dendritic cells. J Exp Med 206(12): 2717-2733.
-
Muciaccia B, Corallini S, Vicini E, Padula F, Gandini L, et al. (2007) HIV-1 viral DNA is present in ejaculated abnormal spermatozoa of seropositive subjects. Hum Reprod 22(11): 2868-2878.
-
Van Leeuwen E, Wit FW, Repping S, Eeftinck Schattenkerk JK, Reiss P, et al. (2008) Effects of antiretroviral therapy on semen quality. AIDS 22(5): 637-642.
-
Pavili L, Daudin M, Moinard N, Walschaerts M, Cuzin L, et al. (2010) Decrease of mitochondrial DNA level in sperm from patients infected with human immunodeficiency virus-1 linked to nucleoside analogue reverse transcriptase inhibitors. Fertil Steril 94(6): 2151-2156.
-
de Sanjosé S, Brotons M, Pavón MA (2018) The natural history of human papillomavirus infection. Best Pract Res Clin Obstet Gynaecol 47: 2-13.
-
Garolla A, Pizzol D, Bertoldo A, De Toni L, Barzon L, et al. (2013) Association, prevalence, and clearance of human papillomavirus and antisperm antibodies in infected semen samples from infertile patients. Fertil Steril 99(1): 125-131.
-
Foresta C, Noventa M, De Toni L, Gizzo S, Garolla A, et al. (2015) HPV‐DNA sperm infection and infertility: from a systematic literature review to a possible clinical management proposal. Andrology 3(2): 163-173.
-
Lyu Z, Feng X, Li N, Zhao W, Wei L, et al. (2017) Human papillomavirus in semen and the risk for male infertility: a systematic review and meta-analysis. BMC Infect Dis 17(1): 714.
-
Jeršovienė V, Gudlevičienė Ž, Rimienė J, Butkauskas D (2019) Human papillomavirus and infertility. Medicina 55(7): 377.
-
Lee CA, Huang CT, King A, Chan PJ (2002) Differential effects of human papillomavirus DNA types on p53 tumor-suppressor gene apoptosis in sperm. Gynecol Oncol 85(3): 511-516.
-
Foresta C, Pizzol D, Bertoldo A, Menegazzo M, Barzon L, et al. (2011) Semen washing procedures do not eliminate human papilloma virus sperm infection in infertile patients. Fertil Steril 96(5): 1077-1082.
-
Foresta C, Pizzol D, Moretti A, Barzon L, Palù G, et al. (2010) Clinical and prognostic significance of human papillomavirus DNA in the sperm or exfoliated cells of infertile patients and subjects with risk factors. Fertil Steril 94(5): 1723-1727.
-
Conrady CD, Jones H, Zheng M, Carr DJ (2011) A functional type I interferon pathway drives resistance to cornea herpes simplex virus type 1 infection by recruitment of leukocytes. J Biomed Res 25(2): 111-119.
-
Spear PG (2004) Herpes simplex virus: receptors and ligands for cell entry. Cell Microbiol 6(5): 401-410.
-
Monavari SH, Vaziri MS, Khalili M, Shamsi-Shahrabadi M, Keyvani H, et al. (2013) Asymptomatic seminal infection of herpes simplex virus: impact on male infertility. J Biomed Res 27(1): 56-61.
-
Kurscheidt FA, Damke E, Bento JC, Balani VA, Takeda KI, et al. (2018) Effects of herpes simplex virus infections on seminal parameters in male partners of infertile couples. Urology 113: 52-58.
-
Isaacson MK, Feire AL, Compton T (2007) Epidermal growth factor receptor is not required for human cytomegalovirus entry or signaling. J Virol 81(12): 6241- 6247.
-
Wrathall AE, Simmons HA, Van Soom A (2006) Evaluation of risks of viral transmission to recipients of bovine embryos arising from fertilisation with virus-infected semen. Theriogenology 65(2): 247-274.
-
Barnes PD, Grundy JE (1992) Down-regulation of the class I HLA heterodimer and β2-microglobulin on the surface of cells infected with cytomegalovirus. J Gen Virol 73 ( 9): 2395-2403.
-
Eggert-Kruse W, Reuland M, Johannsen W, Strowitzki T, Schlehofer JR, et al. (2009) Cytomegalovirus (CMV) infection—related to male and/or female infertility factors? Fertil Steril 91(1): 67-82.
-
Mohseni M, Mollaei HR, Arabzadeh SA, Mirshekari TR, Ghorbani P, et al. (2018) Frequency of cytomegalovirus in fertile and infertile men, referring to Afzalipour Hospital IVF Research Center, Kerman, IRAN: A case- control study. Int J Reprod Biomed 16(7): 443-446.
-
Naumenko V, Tyulenev Y, Kurilo L, Shileiko L, Sorokina T, et al. (2014) Detection and quantification of human herpes viruses types 4–6 in sperm samples of patients with fertility disorders and chronic inflammatory urogenital tract diseases. Andrology 2(5): 687-694.
-
Englert Y, Lesage B, Van Vooren JP, Liesnard C, Place I, et al. (2004) Medically assisted reproduction in the presence of chronic viral diseases. Hum Reprod Update 10(2): 149-162.
-
Berry WR, Gottesfeld RL, Alter HJ, Vierling JM (1987) Transmission of hepatitis B virus by artificial insemination. JAMA 257(8): 1079-1081.
-
Ali BA, Huang TH, Salem HH, Xie QD (2006) Expression of hepatitis B virus genes in early embryonic cells originated from hamster ova and human spermatozoa transfected with the complete viral genome. Asian J Androl 8(3): 273-279.
-
Zhou XP, Hu XL, Zhu YM, Qu F, Sun SJ, et al. (2011) Comparison of semen quality and outcome of assisted reproductive techniques in Chinese men with and without hepatitis B. Asian J Androl 13(3): 465-469.
-
Practice Committee of the American Society for Reproductive Medicine (2008) Guidelines for reducing the risk of viral transmission during fertility treatment. Fertil Steril 90(5): S156-S162.
-
Devaux A, Soula V, Sifer C, Branger M, Naouri M, et al. (2003) Hepatitis C virus detection in follicular fluid and culture media from HCV+ women, and viral risk during IVF procedures. Hum Reprod 18(11): 2342-2349.
-
Savasi V, Parrilla B, Ratti M, Oneta M, Clerici M, et al. (2010) Hepatitis C virus RNA detection in different semen fractions of HCV/HIV-1 co-infected men by nested PCR. Eur J Obstet Gynecol Reprod Biol 151(1): 52-55.
-
Savasi V, Oneta M, Parrilla B, Cetin I (2013) Should HCV discordant couples with a seropositive male partner be treated with assisted reproduction techniques (ART)? Eur J Obstet Gynecol Reprod Biol 167(2): 181-184.
-
Foster GR (2004) Past, present, and future hepatitis C treatments. Semin Liver Dis 24(2): 97-104.
-
Nicopoullos JD, Almeida PA, Ramsay JW, Gilling-Smith C (2004) The effect of human immunodeficiency virus on sperm parameters and the outcome of intrauterine insemination following sperm washing. Hum Reprod 19(10): 2289-2297.
-
Karamahmutoglu H, Erdem A, Erdem M, Mutlu MF, Bozkurt N, et al. (2014) The gradient technique improves success rates in intrauterine insemination cycles of unexplained subfertile couples when compared to swim up technique; a prospective randomised study. J Assist Reprod Genet 31(9): 1139-1145.
-
Weyn C, Thomas D, Jani J, Guizani M, Donner C, et al. (2011) Evidence of human papillomavirus in the placenta. J Infect Dis 203(3): 341-343.
-
Spandorfer SD, Bongiovanni AM, Fasioulotis S, Rosenwaks Z, Ledger WJ, et al. (2006) Prevalence of cervical human papillomavirus in women undergoing in vitro fertilisation and association with outcome. Fertil Steril 86(3): 765-767.
-
Depuydt CE, Jonckheere J, Berth M, Salembier GM, Vereecken AJ, et al. (2015) Serial type‐specific human papillomavirus (HPV) load measurement allows differentiation between regressing cervical lesions and serial virion productive transient infections. Cancer Med 4(8): 1294-1302.
-
Garolla A, Lenzi A, Palù G, Pizzol D, Bertoldo A, et al. (2012) Human papillomavirus sperm infection and assisted reproduction: a dangerous hazard with a possible safe solution. Hum Reprod 27(4): 967-973.
-
De Toni L, Cosci I, Carosso A, Barzon L, Engl B, et al. (2021) Hyaluronidase-based swim-up for semen selection in patients with human papillomavirus semen infection. Biol Reprod 104(1): 211-222.
-
Tsibizov AS, Abdulmedzhidova AG, Krasnopol’skaia KV, Gadzhieva ZS, Kushch AA, et al. (2011) Herpes simplex virus infection of human spermatozoa correlates with decreased frequency of blastocyst formation and frequency of embryo implantation during in vitro fertilisation. Ontogenez 42(6): 447-452.
-
Pallier C, Tebourbi L, Chopineau-Proust S, Schoevaert D, Nordmann P, et al. (2002) Herpesvirus, cytomegalovirus, human sperm and assisted fertilisation. Human Reproduction 17(5):1281-1287.
-
Centers for Disease Control and Prevention (2020) Cytomegalovirus (CMV) and Congenital CMV Infection.
-
Molina I, Carmen Del Gonzalvo M, Clavero A, Angel López-Ruz M, Mozas J, et al. (2014) Assisted reproductive technology and obstetric outcome in couples when the male partner has a chronic viral disease. Int J Fertil Steril 7(4): 291-300.
-
Zamora MJ, Obradors A, Woodward B, Vernaeve V, Vassena R, et al. (2016) Semen residual viral load and reproductive outcomes in HIV-infected men undergoing ICSI after extended semen preparation. Reprod Biomed Online 32(6): 584-590.
-
Baird A, Olarinde O, Talbot M (2007) Evaluation, using two assessment instruments, of the American and British national guidelines for the management of sexually transmissible and genital infections. Sex Health 4(4): 255-260.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions