TLR 1,3 Receptor Gene Polymorphism in Egyptian Patients with Behcets Disease
Behçet’s disease (BD) is a multisystem inflammatory disease characterized by recurrent orogenital ulcerations, ocular inflammations, and skin lesions. The ethology of the disease is currently unknown but evidences suggested that there is a strong genetic component mediating the chronicity of the disorder. The disease is characterized by infiltration of lymphocytes and neutrophils into the affected organs. APCs (Antigen Presenting Cells): It express receptor called (TLR) Toll like receptor which are one of PRR (pattern recognition receptor) and essential components of the innate immune system and they are a class of proteins play a key role in the innate immune system ,recognize structurally conserved molecules derived from microbes. This study aimed at investigating the possible associations between two SNPs (Single Nucleotide Polymorphisms) at TLR1 gene and TLR3 gene and BD in 87 Egyptian patients with BD and 87 healthy controls. Methodology: Blood samples were collected and DNA extraction done. Genotyping of TLR1 gene (1805 T/G), and TLR3 gene (1377 C/T) were performed using (PCR-RFLP) and we found In TLR1 gene (1805 T/G) • Patients with BD had significantly lower frequency of TT genotype and significantly higher frequency of TG , GG genotypes than healthy control • Patients with arthritis had significantly lower frequency of TT & TG, patients with activity had significantly lower frequency of GG genotype. • Patients with activity had significantly lower frequency of T allele, it might be protective allele and patients with arthritis had significantly lower frequency of G allele, it might be protective allele. In TLR3 gene (1377 C/T) • Patients with BD had significantly lower frequency of CC genotype and higher frequency of CT genotype than healthy control. • Patients with vascular involvement had significantly lower frequency of TT genotype. • BD patients with vascular involvement had significantly lower frequency of C allele than patients without involvement it might be protective allele. In conclusion, this preliminary study indicates that there are some genotypes in TLR1 gene (1805 T/G) ,and TLR3 gene (1377 C/T) over-represented , other less presented in BD indicating that they may play a role in BD susceptibility in Egyptian patients.
Introduction
Behçet’s disease (BD) is a chronic relapsing multisystem inflammatory disorder characterized by four major symptoms (oral aphthous ulcers, genital ulcers, skin lesions, and ocular lesions) and occasionally by five minor symptoms (arthritis, gastrointestinal ulcers, epididymitis, vascular lesions, and central nervous system) [1]. Patients with BD may manifest all or only some of these clinical features [2]. The disease is characterized by infiltration of lymphocytes and neutrophils into the affected organs. It is now well known that cytokines play critical roles in the pathogenesis of BD, because they mediate many of the effectors and regulatory functions of immune and inflammatory responses [3].
APCs (antigen presenting cells) express receptor called Toll like receptor (TLR) which are one of PRR (pattern recognition receptor) and essential components of the innate immune system as recognition of microbial antigens occurs via PRRs that are expressed by innate effector cells. Microbial recognition results in a rapid and efficient immne response against invading microorganisms [4].
Toll Like Receptor ( TLRS)
Toll-like receptors (TLRs) are a class of proteins that play a key role in the innate immune system. They are single, membrane-spanning, non- catalytic receptors usually expressed in sentinel cells such as macrophages and dendritic cells, that recognize structurally conserved molecules derived from microbes. Once these microbes have breached physical barriers such as the skin or intestinal tract mucosa, they are recognized by TLRs, which activate immune cell responses. The TLRs include TLR1, TLR2, TLR3, TLR4, TLR5, TLR6, TLR7, TLR8, TLR9, TLR10, TLR11, TLR12, and TLR13, though the latter two are not found in humans. They received their name from their similarity to the protein coded by the toll gene [5].
The family of TLRs is the major and most extensively studied class of PRRs, they are integral glycoproteins characterized by an extracellular or luminal li-gand-binding domain containing leucine-rich repeat (LRR) motifs and a cytoplasmic signalling Toll/interleukin-1 (IL-1) receptor homology (TIR) domain [3]. Ligand binding to TLRs through PAMP-TLR interaction induces receptor oligomerization, which subsequently triggers intracellular signal transduction. They recognize distinct PAMPs derived from various microbial pathogens, including viruses, bacteria, fungi and protozoa [6]. TLRs can be divided into subfamilies primarily recognizing related PAMPs; TLR1, TLR2, TLR4, and TLR6 recognize lipids, whereas TLR3, TLR7, TLR8, and TLR9 recognize nu-cleic acids. Moreover, it appears that TLRs can recognize PAMPs either through direct interaction or via an intermediate PAMP-binding molecule. Thus, TLR1/2, TLR3, and TLR9 directly bind to triacetylated lipopeptides, double-stranded RNA (dsRNA), and CpG DNA, respectively, whereas TLR4 recognizes lipopolysaccharide (LPS) through the accessory molecule MD2 [7]. Intriguingly, some TLRs are endowed with the capacity to recognize structurally and biochemically unrelated ligands, as exemplified by the ability of TLR4 to recognize such divergent structures as LPS, the fusion protein of respiratory syncytial virus (RSV), and cellular heat shock proteins (HSPs) [6].
The molecular basis of this phenomenon may be the ability of different regions of the extracellular portion of TLRs to bind their cognate ligands or the involvement of different PAMP-binding molecules, such as MD2. Further distinction between different PAMPs is accomplished through the formation of heterodimers between TLR2 and either TLR1 or TLR6. Another way of grouping TLRs is based on their cellular distribution. Certain TLRs (TLR1, 2, 4, 5, 6, and 10) are expressed at the cell surface and mainly recognize bacterial products unique to bacteria and not produced by the host, whereas others (TLR3, 7, 8, and 9) are located almost exclusively in intracellular compartments, including endosomes and lysosomes, and are specialized in recognition of nucleic acids, with self versus non self discrimination provided by the exclusive localization of the ligands rather than solely based on a unique molecular structure different from that of the host [4].
Aim of work
The aim of this study was to investigate the possible associations of two SNPs (Single Nucleotide Polymorphisms) at TLR1 gene (1805 T/G) & TLR3 gene (1377 C/T) with the susceptibility and clinical manifestations of Behçet’s disease in the Egyptian population.
Patients and Controls
Eighty seven patients with BD were recruited from Department of Rheumatology at El-Kasr El-Aini Hospital (70 men and 17 women) are included in this case control, study. They were diagnosed according to (ISG for Behcet’s Disease, 1990), Eighty seven age and gender matched healthy control subjects were included in the study. Patients who had other autoimmune disease or malignancy were excluded from the study. Informed consent was obtained from all subjects. The onset of the syndrome was defined as the time when the patient fulfilled the diagnostic criteria. Detailed clinical characteristics were recorded for each patient. At time of blood sampling, patients with two or more lesions in the previous 4 weeks (including oral ulcers, genital ulcers, skin lesions, uveitis, vascular, arthritis, gastrointestinal lesions, central nervous system lesions, and pulmonary involvement) were regarded to have active disease. Almost all patients, except seven cases, were on a treatment specifically for BD (including colchicine, prednisone, azathioprine, thalidomide, cyclosporine, cyclophosphamide, and methotrexate). Routine laboratory investigations were collected from the patients’ records.
Blood Sampling
Five ml of venous blood were withdrawn in (EDTA) sterile tubes and centrifuged at 1000 rpm for 10 minutes.
DNA Extraction
Genomic DNA was extracted from blood samples by using Wizard® Genomic DNA Purification Kit (promega, USA) according to the manufacturer’s instruction.
Red Blood Cell Lysis
Nuclei Lysis
Protein Precipitation DNA Precipitation and Rehydration: The DNA was stored at -20 °C for further application. Quality of DNA was tested using 1% agarose gel electrophoresis.
Genotyping
We investigated the association of the TLR gene polymorphisms on the susceptibility to BD, so we genotyped TLR1 1805 T/G , TLR3 1377 C/T using PCR- RFLP (Restriction Fragment Length Polymorphisms) in 87 Egyptian patients with BD and 87 healthy control, genotype were analysed and compared between patients and controls.
Genotyping of TLR1 (1805T/G) by PCR- RFLP
SNP was analysed by RFLP using two primers (Table 1). The reaction was done in one tube with 25 μl final reaction volume. PCR mixtures consisted 12.5 μl l of Dream Taq Green PCR Master Mix (2X) (Fermentas , USA), 2 μl of forward primer, 2 ul of reverse primer and 8 μl L of DNA , 0.5 μl distilled water All reactions were carried out in a Biometra thermal cycler (Biometra GmbH, Germany). PCR cycling conditions [8] consisted of 95°C for 5 min and 35 cycles of denaturing at 94°C for 30 s, annealing at 55°C for 30 s, and extension at 72°C for 30 s and a single final extension at 72°C for 7 min. The PCR product (280 bp) was digested by addition of AluI (the reaction was done by addition of 5 μl PCR product, 8.5 μl distilled water, 0.5 ul AluI enzyme, 1.5 μl buffer and incubation at 37 c (for 15 min (modified for 60 min for better band clearance), The PCR products were visualized by 4% agarose gel in 0.5X Tris-acetate-EDTA (TAE) buffer with ethidium bromide staining (10 mg/ml). The PCR products were determined relatively to the migration of a 100 bp step ladder (Ferments, USA)).
| forward primer: | 5- GGAAAGTTATAGAGGAACCCT-3 |
| reverse primer: | 5- CTTCACCCAGAAAGAATCGTGCC-3 |
Table 1: PCR Primers used to detect polymorphisms of the
Genotyping of TLR3 (1377 C/T) by PCR- RFLP
SNP was analysed in TLR3 (1377 C/T) by RFLP using two primer forward and reverse (Table 2). The reaction is down in one tube, the final volume for PCR reaction 25 μl; the PCR mixture consist of Master Mix (2X) 12.5 μl (ferments, USA), 2 μl of forward primer, 2 μl of reverse primer and 8μl of DNA, 0.5μl distilled water. PCR cycling conditions [9] consisted of 95°C for 5 min and 35 cycles of denaturing at 94°C for 45 s, annealing at 55°C for 45 s, and extension at 72°C for 30 s and a single final extension at 72°C for 7 min. The PCR product (337 bp) was digested by addition of TaqI ( the reaction was done by addition of 5 ul PCR product , 8.5 μl l distilled water , 0.5 μl TaqI enzyme , 1.5 μl buffer and incubation and incubation at 65°C for 15 min (modified for 60 min for better band clearance). The PCR products were visualized by 3% agarose gel electrophoresis in 0.5X Tris-Acetate EDTA (TAE) buffer with ethidium bromide staining. The relative size of PCR products were determined by comparison of migration of a 100 bp DNA molecular weight ladder (Fermentas, USA).
| Primer F (forward) | 5-CCAGGCATAAAAAGCAATATG - 3 |
| Primer R (reverse) | 5-GGACCAAGGCAAAGGAGTTC - 3 |
Table 2: PCR Primers used to Detect Polymorphisms of TLR3 (1377 C/T).
| Primer F (forward) | 5- CCAGGCATAAAAAGCAATATG - 3 |
| Primer R (reverse) | 5- GGACCAAGGCAAAGGAGTTC - 3 |
Table 3: PCR product of TLR1 1805 T/G and TLR3 1377 C/T.
Gel Electrophoresis
For electrophoresis analysis, 4 % agarose gel was made in 0.5x TAE buffer and 5 μl of ethidium bromide (10μg/ml) was added to 100 ml gel for DNA staining. Electrophoresis was done for 45 min at 90 V. PCR products were visualized by U.V. trans illuminator (UVP.USA) at 280, 337 [TLR 1,3(1805, 1377 respectively) (Table 3). The relative size of PCR products was determined by comparison of the migration of 100 bp DNA molecular weight ladder (Fermentas, USA).
Statistical Analysis
All statistical analyses were performed using the Statistical Package for Social Science (SPSS) version 23 (SPSS, USA), genotype and allele frequency in BD patients and control group were analysed. Results were considered significant at P < 0.05 (*), very significant at P < 0.01 (), and extremely significant at P < 0.001 (*).
Results
Patient’s Findings
Eighty seven patients with BD were recruited from the Department of Rheumatology at Kasr El-Aini Hospital (70 men and 17 women; mean age 37.01±10.41 years; range 18- 67 years). The mean disease duration from the onset time to study entry was (9.2 ±7.26 years; range 1-30 year (Table 4).
| Age (mean ± SD) | 37.01 ± 10 .41 |
|---|---|
| Disease Duration (mean ± SD | 9.2 ± 7.26 |
| Male/ Female | 70 / 17 |
| Clinical Involvement | |
| Oral Ulcers | 87 (100% ) |
| Genital Ulcers | 80 (91.95% ) |
| Ocular Involvement | 55 (63.2%) |
| Skin Lesion | 47 (54% ) |
| Vascular | 25 (28.7%) |
| Neuro | 19 (21.8%) |
| Arthritis | 27 (31 %) |
| GIT | 5 (5.7 %) |
| Chest | 6 (6.9 %) |
| Active patient | 37 (42.5%) |
| Laboratory Investigations | |
| ESR mmHg/hr (mean ± SD) | 30.21 ± 25.12 |
| Hemoglobin gm% (mean ± SD) | 12.95 ± 1.45 |
| WBC 1000/mm3 (mean ± SD) | 7.97 ± 3.35 |
| Neutrophils 1000/mm3 (mean ± SD) | 59.21 ± 11.25 |
| PLT 1000mm3 (mean ± SD) | 235.9± 69.9 |
| Disease Duration (mean ± SD | 9.2 ± 7.26 |
| Male/ Female | 70 / 17 |
| Clinical Involvement | |
| Oral Ulcers | 87 (100% ) |
| Genital Ulcers | 80 (91.95% ) |
| Ocular Involvement | 55 (63.2%) |
| Skin Lesion | 47 (54% ) |
| Vascular | 25 (28.7%) |
| Neuro | 19 (21.8%) |
| Arthritis | 27 (31 %) |
| GIT | 5 (5.7 %) |
| Chest | 6 (6.9 %) |
| Active patient | 37 (42.5%) |
| Laboratory Investigations | |
| ESR mmHg/hr (mean ± SD) | 30.21 ± 25.12 |
| Heamoglobin gm% (mean ± SD) | 12.95 ± 1.45 |
| WBC 1000/mm3 (mean ± SD) | 7.97 ± 3.35 |
| Neutrophils 1000/mm3 (mean ± SD) | 59.21 ± 11.25 |
| PLT 1000mm3 (mean ± SD) | 235.9 ± 69.9 |
Table 4: Demographic, clinical features and laboratory data of 87 patients with BD Parameter Value Demographic Data.
All patients have oral ulcer (100%), 80 patients have genital ulcers (91.95%), 55 patients have ocular manifestations (63.2%), 47 patients have skin manifestations (54 %), 25 patients have vascular manifestations (28.7%), 19 patients have neurological manifestations (21.8%), 27 patients have arthritis (31%), 5 patients have GIT manifestations (5.7%), 6 patients have chest manifestations (6.9%). Patients with two or more lesions in the previous 4 weeks were regarded to have active disease; there were 37 patients in active state (42.5%) and 41 patients in inactive state (57.5%) at the time of blood sampling. 87 ages matched healthy normal controls (41 male & 40 female )were included. There was no significant difference in age or sex between the selected group of patients and healthy controls. The detailed demographic and clinical characteristics of patients are presented in (Table 4).
Association Between Tlr1 Gene Polymorphisms and BD
TLR1 (1805 T/G)) Genotyping: TLR1 (1805 T/G) was genotyped using RFLP. The PCR product was 280 bp. The size of PCR products was determined relatively to the migration of 100 bp step ladder (Figure 1).

TLR1 (1805 T/G) genotypes and allele frequencies in patients with BD and healthy controls are shown in (Table 5). Three genotypes were seen in TLR1 (1805 T/G). Analysis of TLR1 (1805 T/G) revealed that TT genotype was found more frequently in BD patients and healthy controls and increase in the frequency of T allele over G allele. The distribution of genotypes between BD patients and healthy controls (TT 74.7 %, 23 % TG and 2.3 % GG versus 87.36 % TT, 12.64 % TG and 0% GG respectively. It was found that patients with BD had significantly lower frequency of TT genotype (P <0.05) than healthy control and significantly higher frequency of TG, GG genotypes (P <0.05). Also it was found that patients with BD had significantly higher frequency of G allele and this allele is positively correlated with BD patient (P<0.01), it might be risk allele. But patients with BD had significantly lower frequency of T allele and this allele is negatively correlated with BD patient (P<0.01), it might be protective allele.
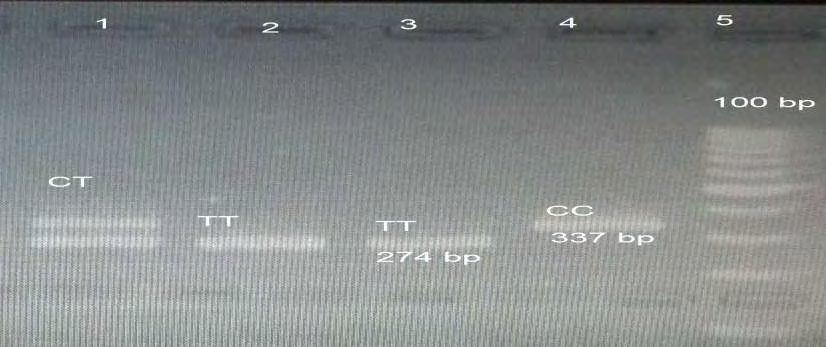
Tlr3 (1377 C/T) Genotyping: TLR3 (1377 C/T) was genotyped using RFLP. The size of PCR products was 337 bp was determined relatively to the migration of a 100 bp stepladder. TLR3 (1377 C/T) genotypes and allele frequencies in patients with BD and healthy controls are shown in (Table 6). Analysis of TLR3 (1377 C/T) revealed that increase in the frequency of T allele over C allele in both BD and control group. The distribution of genotypes between healthy controls and BD patients (8% CC, 29.9% CT, 62.1% TT versus 1.1% CC, 46 % CT, 42.9% TT respectively). It was found that patients with BD had significantly lower frequency of CC genotype (P <0.01) than healthy control. Also BD patient have higher frequency of CT genotype than healthy control (P <0.01) (Figure 2).
| Control group | BD group | P | OR (95% CI) | |
|---|---|---|---|---|
| TLR3 gene | (N= 87) | P | OR (95% CI) | (N= 87) |
| Genotype (N, %) | ||||
| C /C | 7 (8%) | 1 (1.1%) | <0.01 | 0.133(0.3-0.594) |
| C /T | 26(29.9%) | 40 (46%) | <0.01 | 1.997(1.285-3.103) |
| T /T | 54 (62.1%) | 46(52.9%) | Ns | 0.686(0.447-1.051) |
| CT or TT | 80 (92%) | 86 (98.9%) | <0.01 | 7.525(1.684-33.629) |
| Allele Frequency (N, %) | ||||
| C | 40 (23%) | 42 (24.14%) | Ns | 1.0659(0.5717-1.5395) |
| T | 134 (77%) | 132 (75.86%) | Ns | 0.9382(0.58-1.7491) |
Table 5: Genotype distribution and allele frequency of TLR3 1377C/T) in patients with BD and normal controls.
Association between Clinical Findings and Tlr1 1805 T/G & Tlr3 1377 C/T Genotypes
In order to investigate the association between clinical findings and TLR genotypes in BD, the patients were classified according to the clinical features of the disease. As shown in (Table 7). In TLR1 1805 T/G it was found that BD patients with arthritis had significantly lower frequency of TT & TG genotypes (P< 0.05& <0.05 respectively) than patients without arthritis also BD patients with activity had significantly lower frequency of GG genotype (P <0.05) than patients without activity. In TLR3 1377 C/T it was found that BD patients with vascular involvement had significantly lower frequency of TT genotype (p< 0.05) than patients without vascular involvement.
| Oral Ulcer | Genital Ulcer | Other Skin | Ocular Involvement | Vascular Involve ment | Neural Involvement | Arthritis Involvement | Chest Involvement | GIT Involvement | Activity | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | no | yes | No | yes | no | yes | no | yes | no | yes | no | yes | no | yes | no | yes | no | yes | no | |
| Number | 87 | 0 | 80 | 7 | 47 | 40 | 55 | 32 | 25 | 62 | 19 | 68 | 27 | 60 | 6 | 81 | 5 | 82 | 37 | 50 |
| TLR1 (1805 G/T | ||||||||||||||||||||
| T allele | 149 85.6% | 0% | 154 88.5% | 10 71.4% | 92 97.9% | 76 95% | 106 93.4% | 62 96.9% | 50 100% | 98 94.2% | 36 94.7% | 132 97.1% | 52 96.3% | 116 96.7% | 12 100% | 156 96.3% | 10 100% | 158 96.3% | 74* 100% | 94* 94% |
| G allele | 25 14.4% | 0% | 6 11.5% | 4 28.6% | 2 2.1% | 4 5% | 4 6.6% | 2 3.1% | 0% | 6 5.8% | 2 5.3% | 4 2.9% | 2* 3.7% | 4* 3.3% | 0% | 6 3.7% | 0% | 6 3.7% | 0% | 6 6% |
| TLR3 (1377 C/T) | ||||||||||||||||||||
| C allele | 42 24.1% | 0% | 74 46.3% | 8 57.1% | 44 46.8% | 50 96.2% | 52 47.3% | 30 53.1% | 30* 60% | 52* 41.9% | 16 42.1% | 66 48.5% | 26 48.1% | 56 46.7% | 8 66.7% | 74 45.7% | 4 40% | 78 47.6% | 32 43.2% | 50 50% |
| T allele | 132 75.9% | 0% | 86 53.7% | 6 42.9% | 50 53.2% | 2 3.8% | 58 52.7% | 34 46.9% | 20 40% | 74 58.1% | 22 57.9% | 70 51.5% | 28 51.9% | 64 53.3% | 4 33.3% | 88 54.3% | 6 60% | 86 52.4% | 42 56.8% | 50 50% |
Table 6: Association of the most common clinical findings of the disease and TLR1 & 3 alleles in BD. Patients P<0.05 is considere
Association between Clinical Findings and TLR1 1805 T/G & TLR3 1377 C/T Alleles
In order to investigate the association between clinical findings and TLR alleles in BD, the patients were classified according to the clinical features of the disease. As shown in (Table 8). In TLR1 1805 T/G It was found that BD patients with activity had significantly lower frequency of T allele (P <0.05) than patients without activity, activity is negatively correlated with T allele. It might protective allele against activity. also BD patients with arthritis had significantly lower frequency of G allele (P< 0.05) than patients without arthritis. arthritis activity is negatively correlated with G allele. It might protective allele against arthritis In TLR3 1377 C/T It was found that BD patients with vascular involvement had significantly lower frequency of C allele (P <0.05) than patients without vascular involvement. Vascular involvement is negatively correlated with G allele. It might a protective allele against vascular involvement.
| Oral Ulcer | Genital Ulcer | Other Skin | Ocular Involvement | Vascular Involve ment | Neural Involvement | Arthritis Involvement | Chest Involve ment | GIT Involve ment | Activity | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | no | yes | No | yes | no | yes | no | yes | no | yes | no | yes | no | yes | no | yes | no | yes | no | |
| Number | 87 | 0 | 80 | 7 | 47 | 40 | 55 | 32 | 25 | 62 | 19 | 68 | 27 | 60 | 6 | 81 | 5 | 82 | 37 | 50 |
| TLR1 (1805 G/T | ||||||||||||||||||||
| T allele | 149 85.6% | 0% | 154 88.5% | 10 71.4% | 92 97.9% | 76 95% | 106 93.4% | 62 96.9% | 50 100% | 98 94.2% | 36 94.7% | 132 97.1% | 52 96.3% | 116 96.7% | 12 100% | 156 96.3% | 10 100% | 158 96.3% | 74* 100% | 94* 94% |
| G allele | 25 14.4% | 0% | 6 11.5% | 4 28.6% | 2 2.1% | 4 5% | 4 6.6% | 2 3.1% | 0% | 6 5.8% | 2 5.3% | 4 2.9% | 2* 3.7% | 4* 3.3% | 0% | 6 3.7% | 0% | 6 3.7% | 0% | 6 6% |
| TLR3 (1377 C/T) | ||||||||||||||||||||
| C allele | 42 24.1% | 0% | 74 46.3% | 8 57.1% | 44 46.8% | 50 96.2% | 52 47.3% | 30 53.1% | 30* 60% | 52* 41.9% | 16 42.1% | 66 48.5% | 26 48.1% | 56 46.7% | 8 66.7% | 74 45.7% | 4 40% | 78 47.6% | 32 43.2% | 50 50% |
| T allele | 132 75.9% | 0% | 86 53.7% | 6 42.9% | 50 53.2% | 2 3.8% | 58 52.7% | 34 46.9% | 20 40% | 74 58.1% | 22 57.9% | 70 51.5% | 28 51.9% | 64 53.3% | 4 33.3% | 88 54.3% | 6 60% | 86 52.4% | 42 56.8% | 50 50% |
Table 7: Association of the most common clinical findings of BD patient and TLR1 & 3 genotypes in the patients with Behcet’s dise
Association between and TLR 1(1805 T/G) TLR(1377 C/T) Haplotype and Occurrence of BD
The frequency of TLR1 1805 T/G and TLR3 1377 C/T- haplotypes in patients with BD and healthy controls is show The TT was the most frequent haplotypes in both patients, TG is the least frequent haplotype in both patients and controls with absence of CG haplotype in controls, there was insignificant haplotypes in distribution of haplotypes in both patients and controls.
Discussion
BD is a is a chronic, relapsing, and debilitating systemic vacuities of unknown aetiology with the clinical features of mucocutaneous lesions, ocular, vascular, articular, neurologic, gastrointestinal, urogenital, and pulmonary involvement [10]. Evidence of neutrophil, NK and T-lymphocyte hyperactivity with enhanced proinflammatory cytokine production highlights an underlying dysregulation in immune response [11]. The involvement of both innate and adaptive immune responses raises doubts as to whether BD is auto-inflammatory, autoimmune or possibly both [12]. The most substantiated immunopathogenesis hypothesis speculates that the pathology can be triggered by microbiological factors in genetically susceptible individuals [13]. BD usually appears as a sporadic disease, but a familial aggregation is well known and an increased prevalence has been observed in siblings and parents of paediatric patients [14]. Despite a number of controversial viewpoints about familial inheritance, the existence of a Mendelian autosomal recessive entity in multicase families with an affected paediatric member has been pointed out, suggesting that genetic load might be somewhat higher in children with BD than in adults [15].
The close association of the HLA-B*51 allele with BD represents the clearest evidence of a genetic contribution to the disease. A large number of serological studies show a linkage between the disease and HLA-B*51 [16]. Considerable effort has been made to understand whether HLA-B*51 participates in BD pathogenesis or if it represents a marker for any other predisposing genes in linkage disequilibrium with it [17]. However, HLA–B*51 has been identified as the genetic marker most strongly associated with BD, it has been reported that the highest contribution made by the HLA-B locus to overall genetic susceptibility in BD is 19%. This is why other susceptibility genes have been extensively investigated in BD [18].
BD disease is characterized by infiltration of lymphocytes and neutrophils into the affected organs. Because cytokines are involved in the regulation of functions of lymphocytes and phagocytes, they play an important role in the pathogenesis of BD [19]. Th1 type cytokines were reported to be increased in BD and probably contribute to neutrophil and endothelial cell activation [20].
APCs express receptor called Toll like receptors (TLR) which are one of PRR and essential components of the innate immune system as recognition of microbial antigens occurs via PRRs that are expressed by innate effector cells. Microbial recognition results in a rapid and efficient immne response against invading microorganisms [4].
In this study Patients group enrolled had increase in the number of males over females 4 / 1, the domination of the number of male over female in our study is consistent with the epidemiology data from Egyptian population [21] and the age of onset in patients group in this study is around the third decade of life. Moreover, BD showed a male preponderance in Middle Eastern countries and the Mediterranean basin [22]. In contrast, Japan and Korea where women are more commonly affected. We focused upon TLR1 (1805 G/T) and TLR3 (1377 C/T) polymorphism. To the best of our knowledge this study is first to be done on Behçet’s disease. According to this study All patients have oral ulcer (100%), 80 patients have genital ulcers (91.95%), 55 patients have ocular manifestations (63.2%), 47 patients have skin manifestations (54 %), 25 patients have vascular manifestations (28.7%), 19 patients have neurological manifestations (21.8%), 27 patients have arthritis (31%), 5 patients have GIT manifestations (5.7%), 6 patients have chest manifestations (6.9%). Patients with two or more lesions in the previous 4 weeks were regarded to have active disease; there were 37 patients in active state (42.5%) and 41 patients in inactive state (57.5%) at the time of blood sampling.
A. Analysis of TLR1 (1805 T/G) revealed that TT genotype was found more frequently in BD patients and healthy controls and increase in the frequency of T allele over G allele. The distribution of genotypes between BD patients and healthy controls (TT 74.7 %, 23 % TG and 2.3 % GG versus 87.36 % TT, 12.64 % TG and 0% GG respectively). It was found that
- Patients with BD had significantly lower frequency of TT genotype (P <0.05) than healthy control.
- patients with BD had significantly higher frequency of TG genotype (P <0.05) than healthy control
- BD patient have higher frequency of G allele. G allele is positively correlated with BD patient (P<0.05) , it might be risk allele
- BD patient had significantly lower frequency of T and this allele is negatively correlated with BD patient (P<0.01), it might be protective an allele.
B. Analysis of TLR3 (1377 C/T) SNP that increase in the frequency of T allele over C allele in both BD and control group. The distribution of genotypes between healthy controls and BD patients (8% CC, 29.9% CT and 62.1% TT versus 1.1% CC, 46 % CT, 42.9% TT). It was found that
- Patients with BD had significantly lower frequency of CC genotype (P <0.05) than healthy control.
- BD patient have higher frequency of CT genotype than healthy control. T allele is positively correlated with BD patient (P<0.05), it might be risk allele.
- Patients with vascular involvement had significantly lower frequency of TT genotype (P <0.05).
- BD patients with vascular involvement had significantly lower frequency of C allele (P <0.05) and patients without involvement.
References
-
Abdelmoktader A (2018) Genetic Evidence in Behcet Disease Pathogensis. Virol Immunol J 2(1): 000136.
-
Abdelmoktader A (2018) Genetic Association of Promoter FOXP3 Gene Polymorphism with Behcet’s Disease in Egyptians Patients. Virol Immunol J 2(2): 000147.
-
Abdelmoktader A (2017) Role of Cytokines in Behcets Disease. Virol Immunol J 1(4): 1-5.
-
Mogensen TH (2009) Pathogen recognition and inflammatory signaling in innate immune defenses. Clin Microbiol Rev 22(2): 240-273.
-
Hansson GK, Edfeldt K (2005) Toll to be paid at the gateway to the vessel wall. Arterioscler Thromb Vasc Biol 25(6): 1085-1087.
-
Akira S, Uematsu S, Takeuchi O (2006) Pathogen recognition and innate immunity. Cell 124(4): 783-801.
-
Kim HM, Park BS, Kim JI, Kim SE, Lee J, et al. (2007) crystal structure of the tlr4-md-2 complex with bound endotoxin antagonist Eritoran. Cell 130(5): 906-917.
-
Ramasawmy R, Cunha-Neto E, Fae KC, Borba SC, Teixeira PC, et al. (2009) Heterozygosity for S180L Varient of MAL-TIRAP, a Gene Expressing an Adaptor Protein in the Toll-Like Receptor pathway, Is associated with low risk of developing chronic chagas cardiomyopathy. J Infect Dis 199(12): 1838-1845.
-
Pandey S, Mittal B, Srivastava M, Singh S, Srivastava K, et al. (2011) Evaluation of TLR 3 1377 C/T , 9(G2848A) gene polymorphism in cervical cancer susceptibility. Mol Biol Rep 38(7): 4715-4721.
-
Alpsoy E (2012) new evidence-based treatment approach in Behçet’s disease. Patholog Res Int 2012: 871019.
-
Takeno M, Shimoyama Y, Kashiwakura J, Nagafuchi H, Sakane T, et al. (2004) Abnormal killer inhibitory receptor expression on natural killer cells in patients with Behcet’s disease. Rheumatol Int 24(4): 212-216.
-
Direskeneli H (2006) Autoimmunity vs autoinflammation in Behcet’s disease: do we oversimplify a complex disorder? Rheumatology 45(12): 1461-1465.
-
Direskeneli H (2001) Behcet’s disease: infectious aetiology, new autoantigens, and HLA-B51. Ann Rheum Dis 60(11): 996-1002.
-
Piga M, Mathieu A (2011) Genetic susceptibility to Behçet’s disease: role of genes belonging to the MHC region. Rheumatology 50(2): 299-310.
-
Molinari N, Koné Paut I, Manna R, Demaille J, Daures JP, et al. (2003) Identification of an autosomal recessive mode of inheritance in paediatric Behcet’s families by segregation analysis. Am J Med Genet A 122A(2): 115- 118.
-
Durrani K, Papaliodis GN (2008) The Genetics of Adamantiades-Behcet’s Disease. Semin Ophthalmol 23(1): 73-79.
-
Fei Y, Webb R, Cobb BL, Direskeneli H, Saruhan- Direskeneli G, et al. (2009) Identification of novel genetic susceptibility loci for Behcet’s disease using a genome- wide association study. Arthritis Res Ther 11(3): R66.
-
Gul A, Ohno S (2012) HLA-B*51 and Behçet Disease. Ocul Immunol Inflamm 20(1): 37-43.
-
Gül A (2001) Behcçet’s disease: an update on the pathogenesis. Clin Exp Rheumatol 19(5): S6-S12.
-
Arayssi T, Hamdan A (2004) New insights into the pathogenesis and therapy of Behcet’s disease. Curr Opin Pharmacol 4(2): 183-188.
-
Mahla RS, Reddy MC, Prasad DV, Kumar H (2013) Sweeten PAMPs: Role of Sugar Complexed PAMPs in Innate Immunity and Vaccine Biology. Front Immunol 4: 248.
-
Cho SB, Cho S, Bang D (2012) New Insights in the Clinical Understanding of Behçet’s Disease. Yonsei Med J 53(1): 35-42.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions