Vaccine-Induced Immune Thrombotic Thrombocytopenia (VITT) by A Third Dose of Chadox1 Ncov-19 (Astrazeneca) After BNT162b2 (Pfizer–BioNTech)
An atypical case of VITT was described resulting from a vaccination schedule where the third booster with ChAdOx1 nCoV-19 (AstraZeneca) was administered. The patient received a complete vaccination schedule with two doses of Pfizer–BioNTech (BNT162b2) without any complications before the third dose. However, the patient has developed an infrequent yet extreme prothrombotic; hypercoagulable state caused by platelet-activating anti-platelet factor 4 (PF4) antibodies. This phenomenon is typically triggered by the proximate administration of an adenoviral vector vaccine against COVID-19. The patient’s symptoms began ten days after taking the third dose of the ChAdOx1 nCoV-19 vaccine (AstraZeneca). His main complaints when hospitalized were severe headaches and right abdominal pain. The blood tests and MRI scan imaging findings were very characteristic of VITT, and a rare cerebral venous sinus thrombosis was found. Also, a markedly elevated D-dimer and strong positive PF4-dependent enzyme- immunoassay test results were documented. Due to discerning clinical suspicion, this patient was rapidly treated with immunoglobulin infusion for two days and oral steroids for three days. Subsequently, he was anticoagulated with the new oral anticoagulant edoxaban after platelet numbers recovery. In a few days, platelets normalized, and D-dimer levels decreased, while anti- PF4-dependent enzyme-immunoassay test results showed a slow decline. He was discharged taking oral edoxaban without any squeal.
Essentials
- VITT is an infrequent event in the outlook of Covid-19 and specific vaccines. Moreover, it can be associated with severe morbidity and high mortality, mainly if not detected and treated early [1].
- By the time of the writing of this article, it appears that this was the first case of VITT after the third vaccine dose using ChAdOx1 nCoV-19 (AstraZeneca).
- Cerebral Venous Sinus Thrombosis (CVST) and other thrombosis at strange sites, together with thrombocytopenia, occur within 4 to 30 days after vaccine-based viral platform against Covid-19. That’s why several countries have restricted using these vaccines, especially in younger patients [2].
Introduction
More than 6.1 million people have died from Covid-19 globally [3]. There have been 30,103,751 infections and 660,973 coronavirus-related deaths reported in Brazil since the pandemic began [4], with 3.131 deaths per million people [5]. Brazil has administered at least 419,669,076 doses of COVID vaccines so far. Assuming every person needs two doses, that enough to have vaccinated about 99.4% of the country’s population [4]. Based on evidence from March 2021, concerns began to emerge regarding thrombosis related to the first dose of the ChAdOx1 nCoV-19 (Oxford– AstraZeneca) coronavirus disease 2019 (Covid-19) vaccine. The U.K. Health Security Agency identified the patients who had received a second vaccine dose and contacted the primary care physicians for follow-up. This measure showed that none of the 40 patients had developed severe adverse reactions after receiving the second dose of the vaccine, regardless of the vaccine received [6]. The case in question seems to be the first to depict a young male patient who developed a rare thrombotic adverse event, VITT’s development [7] with cerebral venous sinus thrombosis (CVST) following the booster with adenoviral vector-based vaccine ChAdOx1 nCoV-19 (AstraZeneca). It’s crucial to highlight that Rio de Janeiro has one of the highest Brazilian rates of vaccinated people over 12 years old, with 95.81% of its population fully immunized [8]. According to the View- Hub a map-based platform for visualizing data on vaccine use and impact [9], there are currently 300 studies on the vaccine against Covid-19 in 40 countries, with 68 studies involving AstraZeneca and 168 studies including BioNTech.
Furthermore, 49 studies hold mRNA-based SARS-CoV-2 vaccines as a third booster dose. AstraZeneca [10] recently approved a third dose booster against Covid-19 in the EU. The COV- BOOST study group [11] was the first randomized trial of a third-dose booster vaccine given 10- 12 weeks after an initial course of AZ and Pfizer immunization. The Munro, et al. [11] compared the safety and immunogenicity of different Covid-19 vaccines given as a third (booster) dose. They showed acceptable side-effects, although some schedules were more reactogenic than others, such as is the case of current mRNA third doses. Results of this study with data obtained three months and one year after the third dose will provide more information about the impact of these additional doses on the protection promoted by long-term cell immunity and immunological memory.
Case Report
A Caucasian adult male of 34 years old, previously healthy with no comorbidities, quickly developed fever and chills on the second day after the ChAdOx1 nCoV-19 booster. On the sixth day after the vaccine administration, he developed malaise, severe headache and chills that lasted an hour. On the seventh day, he performed PCR and antigen- based testing for SARS- CoV-2, which resulted negative. On the eighth day after the vaccine, he progressed with a right testicular and perineal oedema, prostration, and pain in the right iliac fossa. At this point, the patient also reported excruciating headaches followed by visual alterations, which led him to be admitted to a hospital on February 24th, 2022. He presented a clinical picture of VITT (Figure 1) with cerebral venous sinus thrombosis ten days after the ChAdOx1 nCoV-19 vaccine booster. The polymerase chain reaction test for the SARS-CoV-2 virus using a nasopharyngeal swab was negative. Also, there was no familiar history of genetic disease, the existence of thrombophilia, allergies, or medications that could trigger thrombocytopenia. Peripheral smear showed reduced platelet number with normal morphology, no abnormal erythrocyte or leukocyte morphology, and no schistocytes. On day two, immunologic blood tests were performed in the hospital for rheumatoid factor, antibodies for cyclic citrullinates peptide, anti- centromere, and chromatin IgG, dsDNA, 𝛽2-glycoprotein-1 class IgM and IgG, anti- cardiolipin IgM and IgG antibodies levels, and lupus anticoagulant. All results were negative, except Anti-Ro SS-A, which was detected. The anti-platelet factor (Anti-PF4) IgG antibodies were detected by ELISA life codes PF4 immunoglobulin G from Immunocor (Waukesha, United States) with an optical density (OD) unit value of 3.35 on hospital admission day (reference OD or greater) and was still elevated at 2.37 even on day 41 after hospital admission. Levels of procalcitonin were normal. Thromboelastometry rotational (roTEM) assays depicted a hypocoagulability pattern due to intense thrombocytopenia and low fibrinogen levels. The roTEM was performed serially to guide the use of edoxaban from thromboprophylaxis to anticoagulant doses in conjunction with the dynamics of platelet count evolution. Doppler studies of the lower extremities did not reveal acute deep venous thrombosis. Figure 1 shows the recovery of the thrombocytopenia (29 109 cells/L at admission) and the elevated D- dimers during hospital admission, along with their pattern of evolution (Figure 2).
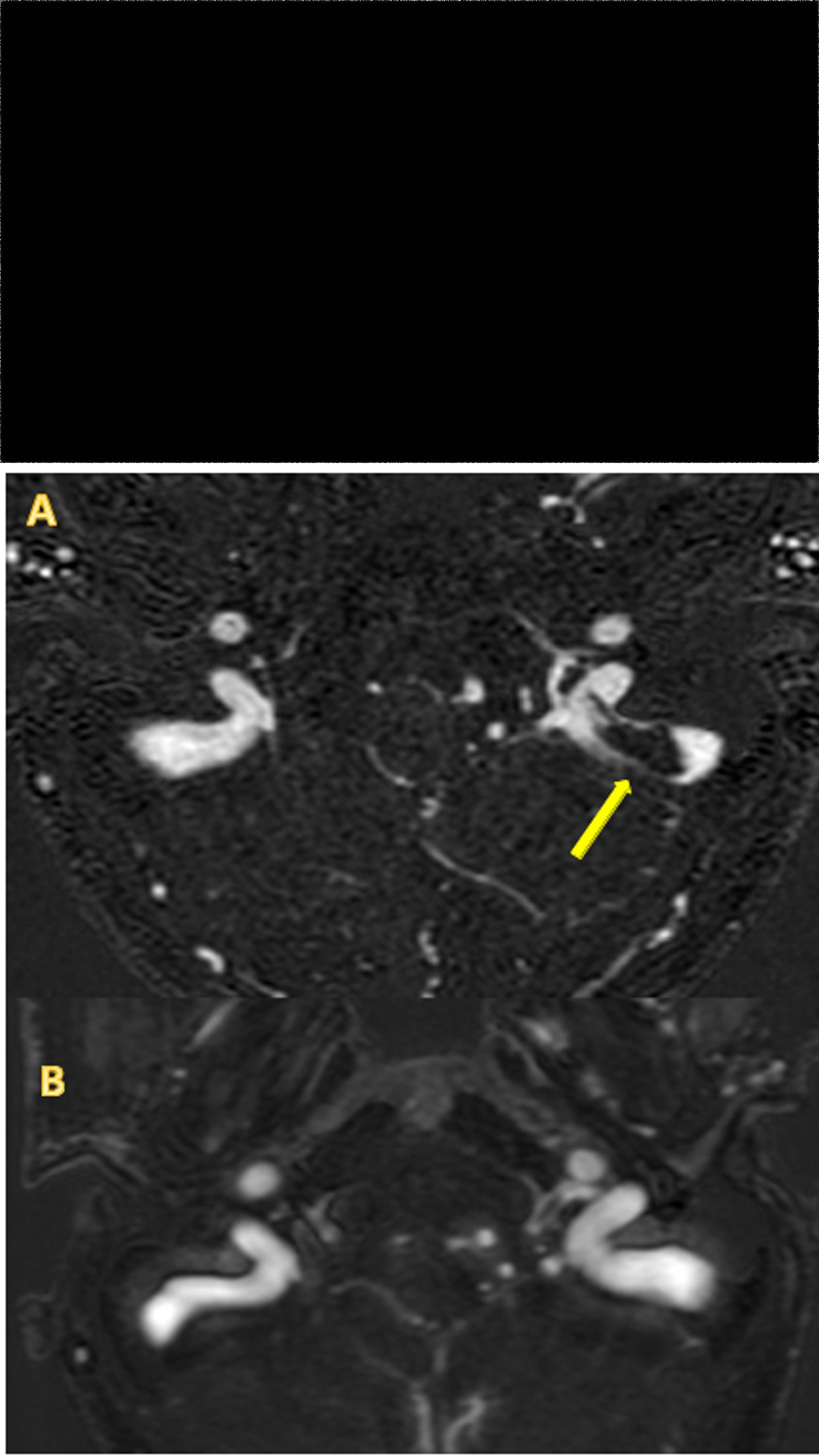
Figure 2A & 2B: Acquired magnetic resonance imaging (MRI) - Spot details of the posterior cranial fossa, in contrast, enhance venous angiography (MRA), showing the lumen of the vessels as white tubular structures A) MRI from hospital admission on February 24th .The arrow points to a black fill in the sigmoid dural sinus indicative of a venous thrombus. B) MRI after hospital discharge on April 27th .Complete resolution of the venous thrombus in the left sigmoid dural sinus.
Discussion
Rapid mass vaccination against COVID-19 effectively protects against severe COVID-19 in real- world settings [12]. Deaths and hospitalizations have been objectively decreased by immunization. Nonetheless, in February 2021, a new thrombotic syndrome was seen many days after vaccinating patients against COVID-19 with ChAd0x1 to-19 (AZ), and similar cases followed with Johnson & Johnson’s Ad26.COV2. S vaccines were reported about two months later [13, 14]. The vaccine-induced thrombosis and thrombocytopenia phenomenon has been given different names, such as thrombosis with thrombocytopenia syndrome (TTS), usually used by agencies and scientific societies. The scientific community has also proposed vaccine-induced immune thrombotic thrombocytopenia (VITT) or vaccine- induced prothrombotic immune thrombocytopenia (VIPIT). Interestingly, VITT closely resembles HIT (heparin-induced thrombocytopenia) in the syndromic process but without heparin utilization [15]. CSVT is the most common site of thrombosis in the series published and occurs at a frequency of 38% to 80% [16]. Hypothetically, a polyanion platform would combine with IgG3 and PF4 to induce platelet activation and degranulation with further PF4 released throughout the activation of FcgRIIa (CD32a) receptor leading to a pathophysiological process that resembles autoimmune HIT [17, 18]. VITT caused by messenger-RNA (mRNA) SARS- CoV-2 vaccines are rare; however, a case report of an mRNA- 1273 SARS-CoV-2 booster-associated VITT with symptoms onset 20 days later was recently published [19]. According to Iba, et al. [20], the VITT acromion can help memorize:
“V” for the vaccine, “I” for the interval (4 – 30 days), “T” for thrombosis, and “T” for thrombocytopenia and thus help in early identification. Recently, Carnevale, et al. [21] pointed out that molecular mimicry between human PF4 and SARS- CoV-2 spike protein is not responsible for the prothrombotic occurrences associated with VITT. Also, Greinacher, et al. [22] described that anti-PF4 antibodies in VITT patients do not interact with epitopes on the spike protein; they function independently. There is evidence that compounds embedded in viral platform vaccines carry a negative charge, such as EDTA (edetic acid), DNA, RNA, polysorbate 80, proteins, and glycosaminoglycans, among others bind and transform this cationic chemokine CXCL4 called PF4 [23]. Healthy young people displayed the appearance of thrombotic events with thrombocytopenia in unusual locations such as brain venous sinus and splanchnic veins, raising the possibility of a rare vaccine-induced prothrombotic disorder. As a result, Canada, Germany, and several European countries have not recommended using the Oxford-AstraZeneca COVID-19 vaccine in younger people. Following this announcement, the University of Oxford discontinued dosing testing in children and adolescents [15, 24]. Suggestively, this case could be another piece of evidence that unbearable headaches in a patient with VITT may be an alert sign as a precursor to cerebral venous sinus thrombosis (CVST) and, as such, must be valued and taken into account by clinicians [25].
Conclusion and Final Remarks
To improve protection, patients who develop VITT should still receive a complete COVID-19 vaccination schedule. However, it is wise to give a booster dose with mRNA vaccines [6, 11], avoiding viral platform vaccines. Currently, VITT cannot be anticipated or prevented. Additionally, clinicians should carefully consider headaches after ChAdOx1 vaccination, even if the platelet count is normal, because of the potential risk of cerebral venous sinus thrombosis, which could happen in a window timeframe 4 to 30 days. Given these assumptions, anticoagulation blocks the generation of thrombin, which is increased in VITT due to the excess activation of platelets and endothelium. High doses of immunoglobulins and adjuvant steroids block anti-PF4 antibodies that activate Fc gamma receptors (FcγIIa/IIIa), which can further increase inflammation, thrombocytopenia and the prothrombotic state. These two precocious approaches are the current pillars of handling VITT. Finally, as already demonstrated by Michalik [26], questions remain about improving vaccine purification methods to attenuate the generation of anti-PF4 antibodies, leading to increasingly safer vaccines.
Authors Contributions
Rubens C Costa-Filho, Ana Tereza A. Monteiro de Souza, and Hugo Caire de Castro Faria-Neto participated in outlining the article. All Authors revised the manuscript critically for important intellectual content and construct. Gabrielle Tantos Nunes and Luiz de Melo Amorim Filho conducted the laboratory assay and supervision. Christiano Penna Luz and Felipe Saddy provided patient care and extended investigations of rising data to outline the manuscript.
Acknowledgments
The authors acknowledge Amarino de Oliveira Jr., MD, senior radiologist assistant at the Department of Radiology of Hospital Pró-Cardíaco, for his valuable help in managing and selecting the best images from magnetic resonance. HCCF-N is a researcher fellowship from CNPq 401700/2020- 8 and CNE/FAPER.
Disclosure of Conflict of Interests
The authors state that they have no conflict of interest.
References
-
Perry RJ, Tamborska A, Singh B, Craven B, Marigold R, et al. (2021) cerebral venous thrombosis after vaccination against COVID-19 in the UK: a multicentre cohort study. The Lancet 398(10306): 1147-1156.
-
Sánchez van Kammen M, Aguiar de Sousa D, Poli S, Cordonnier C, Heldner MR, et al. (2021) Characteristics and Outcomes of Patients with Cerebral Venous Sinus Thrombosis in SARS-CoV-2 Vaccine- Induced Immune Thrombotic Thrombocytopenia. JAMA Neurol 78(11): 1314-1323.
-
(2022) Medicine Coronavirus Resource Center Johns Hopkins University.
-
Reuters (2022) Caribbean C-Tglaat.
-
Coronavirus (COVID-19) deaths worldwide per one million populations as of April 26, 2022, by country.
-
Lacy J, Pavord S, Brown KE (2022) VITT and Second Doses of Covid-19 Vaccine. N Engl J Med 386(1): 95.
-
Nazy I, Sachs UJ, Arnold DM, McKenzie SE, Choi P, et al. (2021) Recommendations for the clinical and laboratory diagnosis of VITT against COVID- 19: Communication from the ISTH SSC Subcommittee on Platelet Immunology. J Thromb Haemost 19(6): 1585-1588.
-
Vacina Mais: OPAS, CNS, Conasse Conasems lançarão ampla campanha de incentivo à vacinação no dia 29/6, às 10h.
-
COVID-19 Data - View-Hub. 2022, this section contains information on vaccine effectiveness studies that have been reported in preprint and published literature and reports.
-
AstraZeneca (2022) Vaxzevria approved in the EU as third dose booster against COVID-19.
-
Munro APS, Janani L, Cornelius V, Aley PK, Babbage G, et al. (2021) Safety and immunogenicity of seven COVID- 19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV- BOOST): a blinded, multicentre, randomised, controlled, phase 2 trial. The Lancet 398(10318): 2258-2276.
-
Paetzold J, Kimpel J, Bates K, Hummer M, Krammer F, et al. (2022) Impacts of rapid mass vaccination against SARS-CoV2 in an early variant of concern hotspot. Nat Commun 13: 612.
-
Greinacher A, Thiele T, Warkentin TE, Weisser K, Kyrle PA, et al. (2021) Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination N Engl J Med 384(22): 2092-2101.
-
Muir KL, Kallam A, Koepsell SA, Gundabolu K (2021) Thrombotic Thrombocytopenia after Ad26.COV2.S Vaccination. N Engl J Med 384(20): 1964-1965.
-
Greinacher A, Selleng K, Warkentin TE (2017) Autoimmune heparin-induced thrombocytopenia. J Thromb Haemost 15(11): 2099-2114.
-
Arepally GM, Ortel TL (2021) Vaccine-induced immune thrombotic thrombocytopenia: what we know and do not know. Blood 138(4): 293-298.
-
Warkentin TE (2021) Heparin-Induced Thrombocytopenia and Vaccine-Induced Immune Thrombotic Thrombocytopenia Antibodies: Fraternal- Not Identical-Twins. Thromb Haemost 121(12): 1558- 1561.
-
Warkentin TE, Pai M (2021) VIPIT versus VITT: what’s in a name? Thrombosis Research 207: 158-160.
-
Langerak T, Bakker GJ, Porcelijn L, Lauw MN, van de Laar RJ, et al. (2022) Vaccine-induced immune thrombocytopenia and thrombosis after mRNA-1273 booster vaccination. Thromb Res 214: 21-22.
-
Iba T, Levy JH, Warkentin TE (2022) Recognizing Vaccine- Induced Immune Thrombotic Thrombocytopenia. Crit Care Med 50(1): e80-e86.
-
Carnevale S, Giovanetti M, Benvenuto D, Ciccozzi M, Broccolo F, et al. (2022) Is Molecular Mimicry between hPF4 and SARS-CoV-2 Spike Protein a Potential Basis for Autoimmune Responses in Vaccinated and Naturally Infected Patients? Semin Thromb Hemost.
-
Greinacher A, Selleng K, Mayerle J, Palankar R, Wesche J, et al. (2021) Immune-Response in C-VSG. Anti-platelet factor 4 antibodies causing VITT do not cross-react with SARS-CoV-2 spike protein. Blood (14): 1269-1277.
-
Greinacher A, Schönborn L, Siegerist F, Steil L, Palankar R, et al. (2022) Pathogenesis of vaccine-induced immune thrombotic thrombocytopenia (VITT). Seminars in Hematology 59(2): 97-107.
-
Vogel G, Kupferschmidt K (2021) Side effect worry grows for AstraZeneca vaccine. Science 372(6537): 14-15.
-
Salih F, Schönborn L, Kohler S, Franke C, Möckel M, et al. (2021) Vaccine-Induced Thrombocytopenia with Severe Headache. N Engl J Med 385(22): 2103-2105.
-
Michalik S, Siegerist F, Palankar R, Franzke K, Schindler M, et al. (2022) Comparative analysis of ChAdOx1 nCoV-19 and Ad26.COV2.S SARS-CoV-2 vector vaccines. Haematologica 107(4): 947-957.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions