Postpartum Haemorrhage Drills and Skills Building
The Sr. MARCH-OT approach is borrowed from the management of exsanguination haemorrhage in trauma care. This applies well to acute PPH haemorrhage control, hence this conceptual paper to change the ALSO and PROPMT algorithms in severe PPH management. The importance of skilled maternity professional and regular drills in managing massive PPH cases is paramount and cannot be over emphasised. The historical approach borrowed from the ACLS approach of following the DR. ABCDE algorithm does not address the points of emphasis in manoeuvres that help quickly control the bleeding, “Closing the tapâ€. Most obstetric patients are young and have the physiological reserve to maintain the alertness, Airway and Breathing in the early stages of bleeding hence emphasis should be on closing the tap and replacing the red cells and clotting factors while not neglecting the support to Airway and ensuring patient is breathing.
Background
Postpartum haemorrhage, defined as the loss of more than 500 mL of blood after delivery, occurs in 3 to18 percent of births. Blood loss exceeding 1,000 mL is considered physiologically significant and can result in hemodynamic instability. Even with appropriate management, approximately 3 percent of vaginal deliveries will result in severe post-partum haemorrhage. It is the most common maternal morbidity in developed countries and a major cause of death worldwide [1].
Conceptual Paper
The majority of causes of PPH can be remembered by the 4T’s: Tone, Trauma, Tissue, and Thrombin.
Tone of the uterus (i.e., atony) comprises 70% of PPH.
At the time of delivery, blood flow to the uterus reaches 500-900 mL/min. After delivery, high levels of oxytocin help potentiate uterine contraction and vasoconstriction of uterine arteries in order to minimize blood loss. The pathophysiology of uterine atony is often attributed to risk factors:
- Impaired contractions from local inflammation and acidosis of uterine tissue (chorioamnionitis)
- Down regulation of oxytocin receptors (prolonged labour)
- Diminished actin-myosin interaction from an enlarged uterus (fetal macrosomia, multiple-gestation pregnancies).
Importantly, atony can also occur in the absence of risk factors [1].
Trauma during delivery is the second most common cause of 20% PPH. If bleeding from a laceration does not stop with pressure, repair by a qualified provider is required. Packing can be placed to tamponade bleeding until appropriate repair can be performed. Cervical lacerations, often more difficult to visualize, should also be kept in the differential for continued postpartum bleeding of unknown source [1].
Tissue refers to retained products of conception (I.e. placenta) is a cause of 9% of PPH. The disruption of the placenta from the uterine wall helps stimulates uterine contraction. The placenta should always be examined to ensure it is fully intact. Bedside ultrasound showing a thickened endometrial stripe or a mass in the uterus could indicate retained products. Treatment involves manual removal of the retained products, which may need to occur in the operating room if analgesia cannot be achieved adequately for the exam [1].
Thrombin – Inherited or acquired dysfunction in coagulation. This accounts for 1% of PPH. Few are anticipated in patients with known past medical history, which will allow you to provide therapies targeted to haemophilia A, B, or von Willebrand disease [1].
The challenging ones are the acquired coagulopathy can occur as a result of placental abruption or amniotic fluid embolism, leading to significant hemodynamic compromise from disseminated intravascular coagulation or hypofibrinogenemia. Management of bleeding related to coagulopathies involves replacing the factor deficiency and replacing lost RBC.
Some risk factors for PPH can be predicted and measures are put in place to mitigate the morbidity. The challenge is majority will occur in unexpected or in neglected patients [1].
The Sr. MARCH-OT approach is borrowed from the management of exsanguination haemorrhage in trauma care. This applies well to acute PPH haemorrhage control, hence this conceptual paper to change the ALSO and PROPMT algorithms in severe PPH management.
The importance of skilled maternity professional and regular drills in managing massive PPH cases is paramount and cannot be over emphasised. The historical approach borrowed from the ACLS approach of following the DR. ABCDE algorithm does not address the points of emphasis in manoeuvres that help quickly control the bleeding, “Closing the tap” [2].
Most obstetric patients are young and have the physiological reserve to maintain the alertness, Airway and Breathing in the early stages of bleeding hence emphasis should be on closing the tap and replacing the red cells and clotting factors while not neglecting the support to Airway and ensuring patient is breathing (Table 1).
“The PPH drill and management is controlled by the one whose hands are on the uterus and in the vagina”. First line efforts should be to get the uterine contraction by manual and chemical initiatives.
| Shout for help CODE PPH | S | Shout for help CODE PPH | |
|---|---|---|---|
| R | Response check – Talk to patient | R | Response check – talk to patient |
| C | Massage & Compress uterus fundus Chemical compression - uterotonic syntometrine, carboprost (IMI) | M | Massage & Compress the uterus fundus Chemically compress – IMI uterotonics Syntometrine, carboprost (Hemabate) |
| A | Air way support and O2 | A | Air way support and O2 |
| B | Breathing support | R | Respiratory support |
| C | Circulation- IVC access, blood collection-X-match, VBG, Coags, FBC IV Uterotonic, Tranexamic acid PRBC, Plasma, Fibrinogen / cryoprecipitate. Haemostasis | C | Circulation- IVC access, blood collection-X-match, VBG, Coags FBC IV uterotonics, Tranexamic acid PRBC, Plasma and Fibrinogen / cryoprecipitate. Haemostasis |
| D | Disability and Thermal control | H | Hypothermia prevention, homeostasis |
| E | Extra interventions and / UTB – Bakri Rotem / TEG directed balanced replacement or 1:1:1 | OT | Operation theatre and UTB -Bakri / C&C UTB Rotem / TEG directed balanced replacement or 1:1:1 |
Table 1: The paradigm shift to SR. CABCDE or SR. MARCH-OT.
The above approach will remind care givers to close the tap by early uterine massage and compression (Similar to toniquet and pressure dressing in exsanguinating haemorrhage) and prevent further blood loss while allowing time for effect of uterotonics and tranexamic acid. This will reduce acute blood loss and reduce the need for blood transfusion and all course morbidity and mortality from PPH.
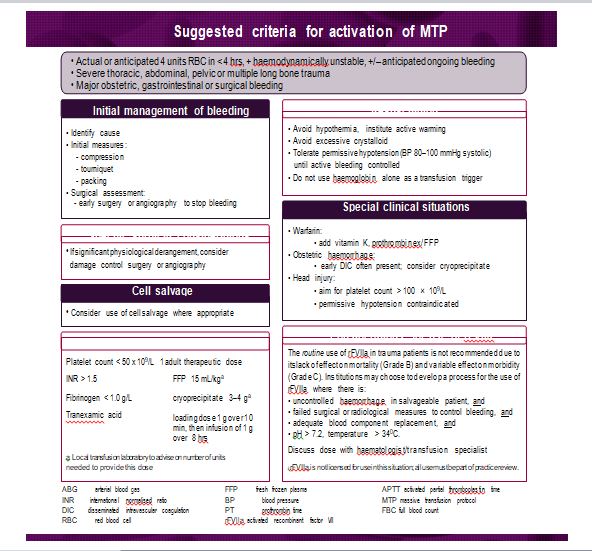
Severe / Massive PPH is an Obstetric Emergency and is a Medical Code Blue (PPH)
SR Stands to remind the first responder or observer should shout for more clinical help like other MET calls. This is done by mouth, telephone special loudspeaker, and red button to siren for help. This call is for all and most senior consultant Obstetrics and Anaesthetics [3].
In most early primary PPH Verbal communication with patient will establish if patient is responsive and that the Airway is open, and patient is ventilating. Most patient are still saturating well on room air.
M /C- Reminds the attended to massage and gently apply firm compression on the uterine fundus to stop active bleeding while other concurrent measures are being instituted of augmented.
Uterine Massage and Bimanual Compression
Brisk blood flow after delivery of the placenta should alert the physician / accoucheur to perform a bimanual examination of the uterus. If the uterus is soft, massage is performed by placing one hand in the vagina and pushing against the body of the uterus while the other hand compresses the fundus from above through the abdominal wall.
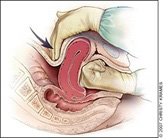
This manoeuvre helps with physical compression on the placental site spiral arteries inlets until the myometrium has contracted strong enough to toniquet the spiral arteries traversing the wall (Figure 1). This procedure is uncomfortable in patients without regional block anaesthesia so provide analgesia in the form of Entonox, Panthorax or fentanyl 1-1.5mcg/kg titrated in 25-50mcg aliquots.
Once the anaesthetist has arrived consider using ketamine for pain control and sedation if extended bimanual compression is needed to stop bleeding while preparing to move into theatre.
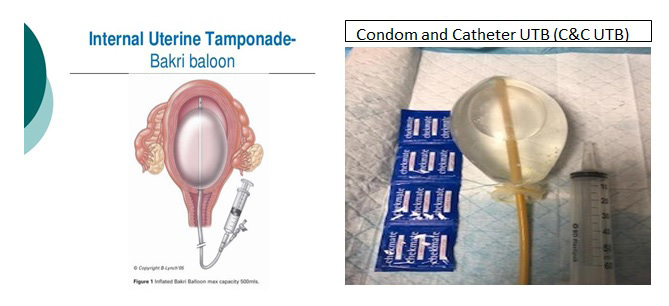
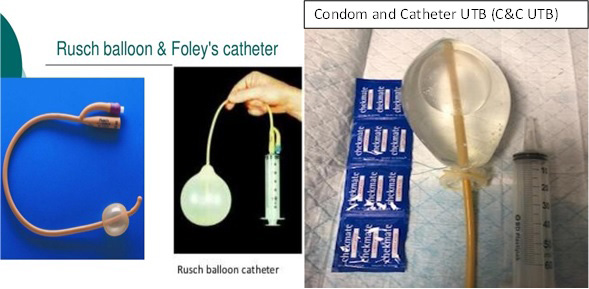
Chemical uterine compression is achieved by use of intramuscular uterotonics like IMI syntometrine (combination of oxytocin and ergometrine), IMI Carboprost (Haemabate) 250mcg, and or Intravenous oxytocin infusion 40 units in 1L at 250mls per hour. Misoprostol Sublingual 200mcg and or 1000mcg PR is a reasonable substitute for carboprost in LMICs Intra uterine tamponade procedures require good anaesthetic and also lighting. If patient has adequate regional block and uterus cleared of any RPOC, the UTB can be placed in the labour room and save precious time and further blood loss while moving to theatre.
Modern labour suites have an adjoining emergency theatre room for use for dire emergencies like severe PPH, Crush C-sections.
Placenta and RPOC may be the cause of PPH and can interfere with efforts in managing the atonic uterus. CCT and removal of placenta or in theatre evacuation of uterus. Placenta should be inspected for completeness by the other helpers and feedback to the lead carer.
For low resourced units with no access to premanufactured UTB should consider using the double condom tied over a 24 Foley’s catheter. This is a low-cost innovation that can save the bleeding woman. Readers are encouraged to practice making these during their PPH drills.
M- The one who’s hand in perineum, Massage and compress the uterus all the time A – Airway needs a close watch as it can get compromised as patient gets into severe shock Airway nurse and doctor once available takes over the role and if needed RSI R– Breathing and respiration monitoring and support is paramount and is done concurrent to all the measures to stop bleeding. Supplementary oxygen may be needed C – Circulatory support and replacement of the lost volume and components of blood helps with homeostasis and coagulation.
• IV- 2x IVC Access using large bore cannular and collecting bloods for tests.
• IV- medications for quick action – Uterotonic infusion, Tranexamic acid 1g ivi.
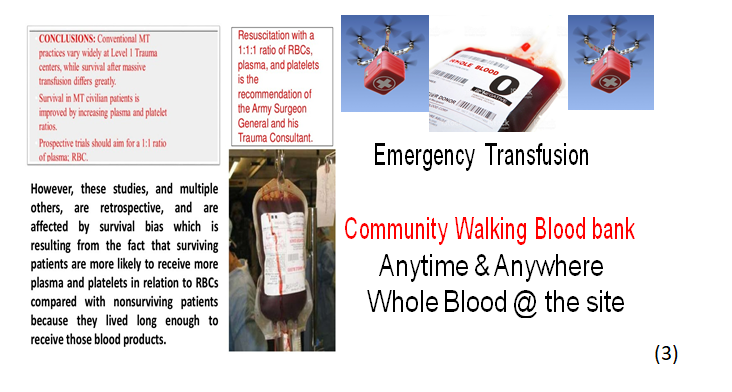
• Early whole blood or (1:1:1) PRBC, Plasma, Platelets, Components blood replacement.
• Coagulation components assessment and replacement.
H - Hypothermia prevention. Hypocalcaemia prevention. Hypotension prevention OT – If above measures not winning, then surgical procedures should be considered early and senior help if not yet available should be summoned. The uterus needs to be evacuated and cleared of any RPOC and preparation for open surgery access to uterus to do advanced surgical procedures.
Advanced Surgical Procedure to Manage PPH
Damage control is one of early interventions emphasised in early management of trauma patients. Taking notes from the trauma care in ED to the labour ward PPH emergencies, early management of obstetric trauma using direct pressure followed by definitive suturing to stop bleeding. “This is the close the tap approach in active management of PPH”.
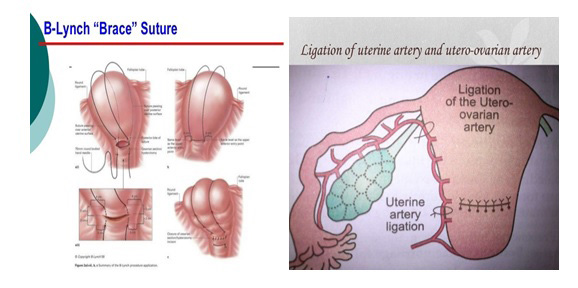
When external pressure or UTB and the various uterotonics are failing to control the bleeding, the care needs to be escalated to in theatre management which include the following procedures, laparotomy to facilitate B- lynch suture application, Uterine plus / minus ovarian brunch ligation (Figures 2 & 3). The devascularisation operation is a desperate step to try an save the uterus. Failure of the devascularisation calls for subtotal or total hysterectomy. This decision does not come lightly but should not be delayed at the expense of life.
These surgical procedures are a life-saving intervention which should be made available at all delivery sites or a fly in obstetrician within 1hr driving or flying distance.
Hysterectomy or Bilateral Uterine Artery Embolization
These procedures are done by or with help of experienced consultant supervision (Figure 5). They are included here to remind the middle level clinician to inform seniors early and plan for escalation of care.
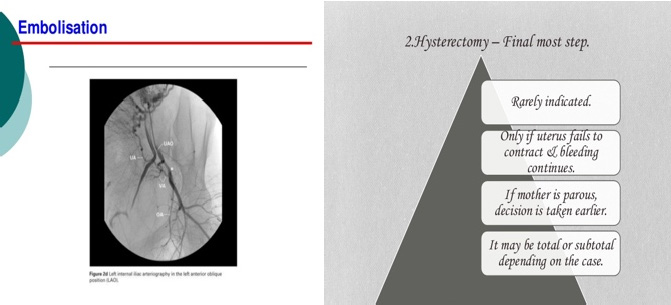
Concurrent resuscitation activities managed by anaesthetist and haematology support Interventional radiology, selective bilateral uterine embolization are a hi- technological minimally invasive approach which is done in tertiary hospitals in high income countries. (Figure 2d).
Blood replacement one area that need to be drilled into our clinicians to reduce morbidity, amount of blood transfusions complications, as well as save many lives (Figures 6 & 7).
Whole blood replacement is the most ideal way to correct all components lost through bleeding but due to short shelf life blood components are stored frozen in different components. The use of ROTEM and TEG to guide components replacements is valuable but not yet readily available especially in remote and low income countries or regions.
References
-
Anderson JM (2007) Prevention and Management of Postpartum Hemorrhage. American Family Physician Journal 75(6): 875-882.
-
Hess JR (2020) Massive blood transfusion, University of Washington School of Medicine: Up to date.
-
Eve Meinhardt, USA Military medicine.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era