Acute Intestinal Ischemia and Mesenteric Vein Thrombosis with Mortality During Pregnancy
Objective: We present a case of acute intestinal ischemia and mesenteric venosus thrombosis in a first trimester pregnant woman with surgical treatment. Case presentation and intervention: Our case was a 23-year-old multigravid woman at 8 weeks gestation. She presented to Ataturk University Research Hospital with complaints of abdominal distention, nausea, vomiting and constipation. The first day after admission, complained of more intense vomiting, abdominal distenrion and pain. An emergency laparotomy was performed. The part of jejenum, entire ileum, part of the ascending colon were necrosis, and thrombosis was discovered in the mesenteric venosus. The necrotic intestine was resected and a end-to-end colo-jejunal anostomosis was perormed. Postoperative, the patient was started on anticoagulants and antibiotherapy in intensive care. Unfortunately, the patient died on the second day after the operation. Conclusion: Mesenteric ischemia and MVT in pregnancy is a rare, but important cause of intestinal ischemia. When a pregnant patient presents with an acute abdomen, mesenteric ischemia and MVT should be included in the differential diagnosis.
Introduction
Acute mesenteric ischemia is commonly seen in old patients. Acute intestinal ischaemia is caused by mesenteric venous thrombosis in 5-15% of patients. Mesenteric vein thrombosis (MVT) is rare and difficult to diagnose due to its nonspecific presentation. If diagnosis or treatment were delayed, it can be fatal because intestinal infarction or variceal bleeding may occur [1–4] . The mortality rate among patients with acute MVT ranges from 20 to 50% [5]. A wide range of prothrombotic states have been linked to MVT, including cancer, trauma, intraabdominal inflammatory conditions, the postoperative state, oral contraceptive use, in vitro fertilization-embryo transfer (IVF-ET), cirrhosis and portal hypertension, and those caused by heritable or acquired factors, including deficiencies of protein C, protein S or antithrombin III [5, 6, 7, 8]. Pregnancy itself is a risk for hypercoagulopathy.We present a case of acute intestinal ischemia that ends with mortality during pregnancy.
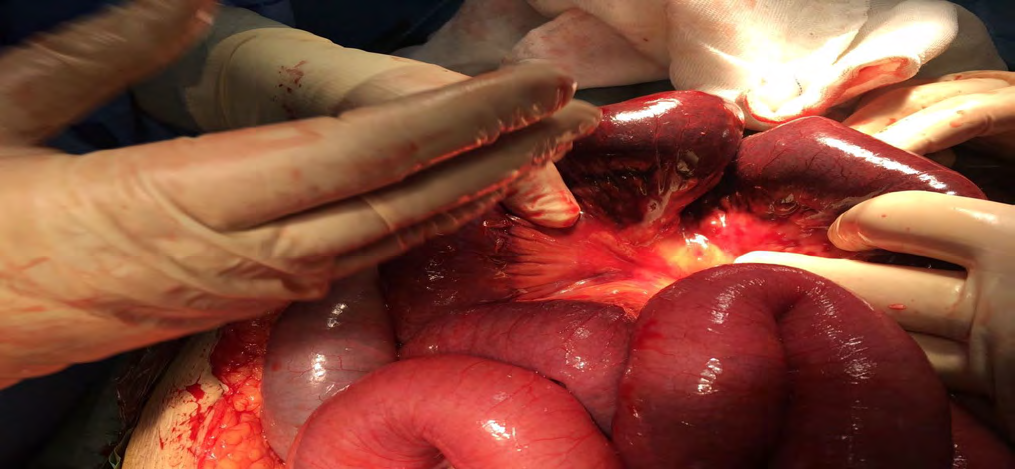
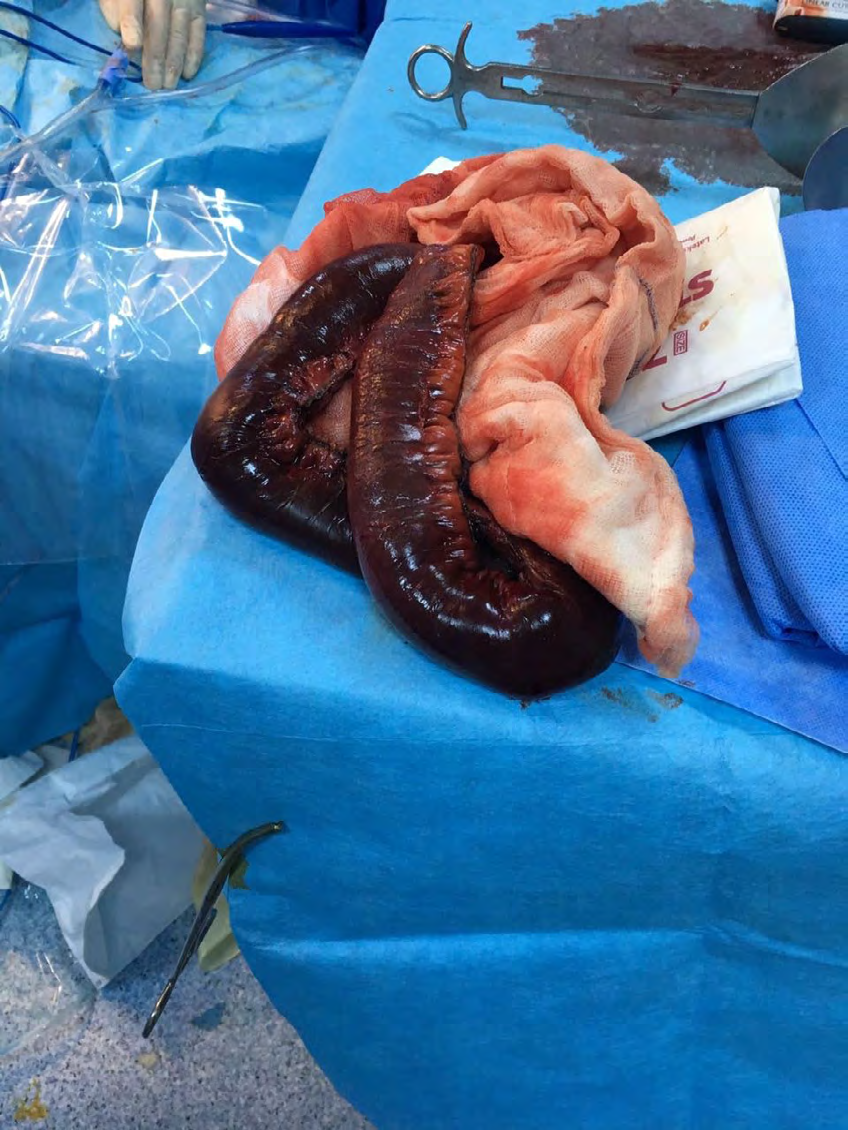
A 23-year-old multigravid woman, at 8 weeks gestation attended our obstetric clinic complaining of abdominal distention, nausea, vomiting for 24 h. She had no significant medical, surgical or family history and no history suggestive of thromboembolism. Anamnesis has been found to be constipated for 8 days. She had not used oral contraceptives or any other hormonal therapy. She did not have a history of alcohol and smoking. A physical examination on admission showed a gravid uterus just below the umbilicus. Abdominal distension was evident but defensive and rebound absent. Bowel sounds were close to normal. A labarotory examination revealed a leukocyte count of 13.1 × 109/L with neutrophils accounting for 73.9% , hemoglobin level of 98.6 g/L and platelet count of 187 × 109/L. Biochemical parameters and coagulation profile tests were within normal limits. Obstetric ultrasound was compatible with the 8-week-old fetus. In magnetic resonance imaging, there was no finding other than mild dilation in the intestinal segments. After approximately 24 hours, laparotomy decision was taken due to the increase in symptoms of the patient (nausea, vomiting, abdominal distention) and the development of diffuse abdominal pain. On exploration, approximately 1200 mL of serous peritoneal fluid was found in the abdomen. The part o jejenum, entire ileum, part of the ascending colon were necrosis, and thrombosis was discovered in the mesenteric vein (Figures 1-3). The necrotic intestine, measuring approximately 160 cm, was resected and an end-to-end colojejunal anastomosis was performed. The patient’s hematological parameters during the operation showed a white cell count of 17.72 × 109/L, neutrophils accounting for 87%, hemoglobin of 8,1 g/dL and a platelet count of 144 × 109/L. The patient was transferred to the surgical intensive care unit after operation. intravenous antibiotics, total parenteral nutrition and full anticoagulation with low molecular weight heparin were initiated postoperatively. After leaving the intensive care unit, it was planned to terminate the pregnancy with the consent of the patient and the family. Unfortunately, the patient died on the 2nd postoperative day.

Discussion
Mesenteric venous thrombosis (MVT), clinical presentation may vary from an asymptomatic condition to intestinal infarction and shock. Advances in imaging techniques have permitted the diagnosis of mesenteric venous thrombosis to be made before laparotomy is performed, but there is often a considerable delay in the diagnosis due to a low degree of suspicion on the part of clinicians and the unspecific clinical presentation [9]. Diagnosis during pregnancy.
becomes difficult due to confusion of symptoms. For this reason, it is more difficult to diagnose in pregnant women, there are delays in diagnosis and it can cause maternal mortality as in our case. Most patients have thrombotic tendencies or risk factors. The predisposing factors are hypercoagulable states (protein C deficiency, protein S deficiency,antiphospholipid antibody, factor V Leiden mutation and antithrombin III deficiency), inflammatory state (appendicitis, diverticulitis, pancreatitis), portal hypertension, pregnancy, oral contraceptive use, abdominal injury and cancer [1, 2, 3, 4]. Pregnancy itself is already a risk actor for hypercoagulopathy, and it requires us to be vigilant to think that MVT may develop even if it is not possible to have any other risk factor in our presented case. In most cases of acute MVT, the main symptom is abdominal pain. Other symptoms are nausea/vomiting, fever and abdominal distention. In our case, other symptoms were evident except for fever. however, these symptoms are closely related to the symptoms of pregnancy (especially hyperemesis gravidarum) in early weeks. Mesenteric ischemia and MVT should be kept in mind in pregnant women as delay in diagnosis significantly increases mortality and morbidity.
Conclusion
Although pregnancy was not the primary cause of mesenteric ischemia and MVT, it did play a role in inducing the acute intestinal ischemia and necrosis. Pregnancy is itself a risk for hypercoagulability, this case indicates that pregnant patients should be counseled about the high risk of acute mesenteric ischemia and thrombosis.
References
-
Chan CM, Chen WL, Chen JH, Wu YL, Huang CC (2009) Pregnancy-Induced Acute Intestinal Infarction in a Woman with Chronic Idiopathic Mesenteric Vein Thrombosis under Regular Anticoagulation Treatment. Med Princ Pract 18(5): 422-424.
-
Morasch MD, Ebaugh JL, Chiou AC, Ma tsumura JS, Pearce WH, et al. (2001) Mesenteric venous thrombosis: a changing clinical entity. J Vasc Surg 34: 680-684.
-
Warren S, Eberhard TP (1935) Mesenteric vein thrombosis. Surg Gynecol Obstet 61: 102-121.
-
Grendell JH, Ockner RK (1982) Mesenteric venous thrombosis. Gastroenterology 82: 358-372.
-
Kumar S, Sarr MG, Kamath PS (2001) Mesenteric venous thrombosis. N Engl J Med 345: 1683-1688.
-
Dorais J, Jones K, Hammoud A, Gibson M, Johnstone E, et al. (2011) A superior mesenteric vein thrombosis associated with in vitro fertilization. Fertil Steril 95(2): 804.e11–3.
-
Hmoud B, Singal AK, Kamath PS (2014) Mesenteric venous thrombosis. J Clin Exp Hepatol 4: 257-263.
-
Guan X, Huang L, Li L (2018) Acute mesenteric venous thrombosis in a pregnant woman at 35 weeks of gestation: a case report and review of the literature. BMC Pregnancy and Childbirth 18(1): 487.
-
Ozcan C, Anadol E (2008) Mesenteric Venous Thrombosis. Turkiye Klinikleri J Gen Surg-Special Topics 1(1): 102-106.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era