Does Human Blastocyst Transfer Increase the Success Rate in Artificial Reproductive Technology (ART) Treatment
All over the world, many of the ART centres, especially those without experience perform Cleavage stage on not blastocyst transfers. Although it has been proved without doubt that Blastocyst transfer is better, the personal experience of failure after shifting to Blastocyst transfer has demotivated many from the shift. The aim of this article was to explain to the reader how we at the University hospital took evidence based decisions and improved our culture conditions while increasing our pregnancy rates. Although the outcome of an ART cycle depends on a multitude of clinical and laboratory factors, this study pursued to critically explore the various advantages and disadvantages of changing the protocol in a German lab to international standards where blastocyst culture is the norm. 1126 ART cycles were performed from 2014 to 2018 in the University Reproductive Medical Unit of UKSH, Kiel. There was an improvement in pregnancy rates from 2014 to 2018 in both cleavage stage transfer (day 3) and blastocyst transfer with a 1.4 time increase every year. Improvement in the lab culture conditions had profound effect in increasing pregnancy rates. The article aims at encouraging the reader to make decisions to improve lab blastocyst culture conditions before shifting to blastocyst culture to improve pregnancy rates and not blindly shift overnight to blastocyst for all.
Introduction
After 40 years of successful human In Vitro Fertilization (IVF), Intra Cytoplasmatic Sperm Injection (ICSI) therapeutic modalities have made a great progress. Although there is a change word-wide to move to blastocyst Embryo Transfer (ET) to improve pregnancy rates, it is still a topic of debate. The primary aim of this study was to critically analyse if a predominant shift to blastocyst culture and transfer improved the chances of a patient getting pregnant when they were undergoing an ART cycle in the Reproductive Unit of the University Hospital, Kiel, Germany. The critical analysis included all the possible benefits and disadvantages of shifting from day 2/3 to day 5 culture and the potential factors in our lab that improved embryo culture conditions to have optimal ideal blastocyst rates. The Vienna consensus clearly states that 60% is the benchmark for the Key performance indicator of “Blastocyst development rate” and 40% for “Good blastocyst development rates”. In the course of the evaluation, we realised that if the ideal blastocyst development rate was >40% [1, 2], it was an excellent evaluation of the culture system in the lab and provided early detection of negative outcomes due to changes in the conditions in the lab [3].
Patients and Methods
Inclusion criteria for the 1126 evaluated IVF/ICSI cycles were: patients of the University Reproductive Medical Unit who underwent stimulation for egg retrieval and had this procedure done by trans-vaginal follicular puncture, had fertilization after IVF/ICSI and had an embryo transfer in the same cycle. When an embryo transfer is performed in the same cycle as the stimulation, it is called a “fresh embryo transfer”. Patients in whom ICSI was performed with testicular aspirated sperm and not with ejaculated sperm.
Ethical approval for our evaluation was not necessary to obtain as the study consist of a retrospective analysis of patients data. All patients gave written informed consent for their data evaluation.
Ovarian Stimulation, Oocyte Retrieval and Embryo Transfer
Controlled ovarian hyperstimulation was performed using recombinant FSH (Gonal-F, Bemfola, Rekovelle, Puregon oder Ovaleap) or urinary extracted HMG (Menogon, Pergoveris). Pituitary down-regulation was achieved by GnRH antagonist (Orgalutran (0,25mg/ 0,5ml)) from Day 6 of the stimulation and the dose (125-450 IU/day) was adjusted based on the ultrasound monitoring of follicular growth. During follicular monitoring, when at least 3 of the follicles were >17mm in diameter, a HCG trigger of Ovitrelle (6500 IU) or alternatively Brevactid (5000/ 10.000 IU) was given. Trans-vaginal ultrasound guided oocyte retrieval either with or without anaesthesia was performed 36 hours after triggering with HCG. Oocyte retrievals were planned on Mondays, Wednesdays and Fridays while the embryo transfers were planned for day 2/3/5, depending on the previous discussion with the couple and the embryo development.
The embryo transfer was performed under abdominal ultrasound guidance by an after-load technique. Conventional luteal support was followed. A serum beta- HCG measurement was performed 14 days after the transfer to confirm pregnancy. A beta-HCG of more than 20 IU was considered positive for pregnancy.
Laboratory Techniques and Culture Systems
Routine IVF/ ICSI were performed. After 16-18 hours of the ICSI, i.e. on Day 1 a fertilization check was performed. When a Day 2/3 transfer was planned, according to the Embryo Protection Act (ESchG- Embryonen-Schutz-Gesetz), only 1, 2, or 3 zygotes were left in culture and on day 2/3, the embryos were graded according to the morphology scoring system proposed by European Society of Human Reproduction and Embryology (ESHRE) [4] and then transferred. If a day 5 transfer was planned, according to the German Middleway (DMW- Deutscher Mittelweg) [5], 2 and 6 fertilized oocytes were cultured till Day 5 and 1, 2 or 3 developmentally appropriate embryos were transferred.
On day 5, the embryos were graded according to the ESHRE consensus workshop [4]. Based on the morphological grading of the blastocyst, they were divided into ideal embryos and not-deal embryos. Ideal embryos had, at least a grade 3 for the blastocoel cavity, a grade B for the inner cell mass and a grade B for the trophectoderm. Any day-5 embryos not reaching these minimum criteria were considered a non-ideal embryo.
Over the period of 5 years, our lab changed its culture technique 3 times to stay abreast with the latest technology available for embryo culture [6]. From 2013 to 2018, all three incubators were used for patients parallelly. Randomly, patient’s embryos were either cultured in a conventional incubator (Heracell™ 240i CO2 Incubator, Thermo Fischer Scientific), bench-top incubator (IVF Cube, AD-3100, Astec) or time lapse incubator (Esco MIRI® Time-Lapse Incubator).
In the conventional incubator, around 6% CO2 was the only gas used for maintaining the pH of the culture media. The oxygen concentration was that of atmosphere – 21%. In the bench-top and time lapse incubators, along with 6% CO2, 5% O2 form the atmosphere was maintained by adding 89% nitrogen gas to the incubator [7].
Statistical Analysis
Data analysis was performed using computer software JASP [8] for descriptive statistics, independent sample t-tests, χ2 test and fisher’s exact tests. While comparing descriptive statistics between the two groups for bias, Welch test was used if the distribution was normal and if not, the Mann- Whitney test was used.
The data of binomial logistic regression analysis was computed using JAMOVI (1.2.16 current). All the variables that were assessed were included in all the logistic regression analysis in order to correct any probable bias. The variables were: Age of the woman [9], number of IVF attempts [10], number of oocytes retrieved [11], mature oocytes, immature oocytes, fertilized oocytes, number of embryos transferred [12], doctor who performed the oocyte retrieval and embryo transfer, embryologist who performed the oocyte screening, ICSI/IVF and embryo transfer, culture incubator used and status of the catheter after the embryo transfer [13]. The logistic regression analysis data was accepted only when the Nagelkerke R2 value was >0.2.
Results and Discussion
General Comparison of Pregnancy Rates
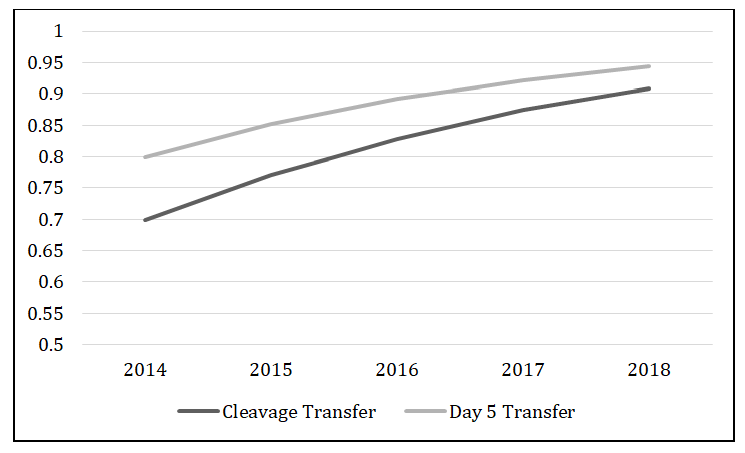
Analysis of the pregnancy rates in each year from 2014 to 2018 (Tables 1 & 2) showed no statistical difference in the pregnancy rates between the years for Day 2 transfer (p=0.96), Day 3 transfer (p=0.67) and combined cleavage stage transfer (p=0.45). When pregnancy rates of cleavage transfers were compared with day 5 transfers for each individual year, no significance was found (p value ranging from 0.06 to 0.73). On individually analysing the difference between the years, it was found that the most significant (p=0.005) improvement in pregnancy rates were between 2017 and 2018 for blastocyst transfer.
| 2014 | 2015 | 2016 | 2017 | 2018 | Grand total | |
|---|---|---|---|---|---|---|
| Day 2 transfers | 94 | 91 | 101 | 111 | 98 | 495 |
| Pregnant | 32 | 20 | 27 | 30 | 20 | 139 |
| Percentage Pregnant | 34% | 22% | 26.70% | 27% | 30.60% | 28.10% |
| Day 3 transfers | 42 | 48 | 69 | 78 | 59 | 296 |
| Pregnant | 9 | 10 | 20 | 23 | 18 | 80 |
| Percentage Pregnant | 21.40% | 20.80% | 29% | 29.50% | 30.50% | 27% |
| Cleavage transfers | 136 | 139 | 170 | 189 | 157 | 791 |
| Pregnant | 41 | 30 | 47 | 53 | 38 | 219 |
| Percentage Pregnant | 30% | 21% | 27.60% | 28% | 24% | 26% |
| Day 5 transfers | 37 | 44 | 56 | 73 | 125 | 335 |
| Pregnant | 7 | 13 | 14 | 16 | 52 | 102 |
| Percentage Pregnant | 18.90% | 29.50% | 25% | 21.90% | 41.60% | 30.40% |
Table 1: Comparison of pregnancy rates in each year from 2014 to 2018 based on day of transfer. (Cleavage transfer is day 2 and d
| Mean | Std. Deviation | Minimum | Maximum | P value | T-Test | ||
|---|---|---|---|---|---|---|---|
| Age | Cleavage | 35,9 | 4,7 | 23 | 48 | 0.003 | Welch |
| Age | Day 5 | 35,0 | 4,3 | 25 | 44 | 0.003 | Welch |
| ART attempt number | Cleavage | 1,8 | 1,2 | 1 | 10 | 0.36 | Mann-Whitney |
| ART attempt number | Day 5 | 1,9 | 1,2 | 1 | 7 | 0.36 | Mann-Whitney |
| No. Of COCs | Cleavage | 8,6 | 5,6 | 1 | 32 | 0.3 | Mann-Whitney |
| No. Of COCs | Day 5 | 12,0 | 5,2 | 2 | 35 | 0.3 | Mann-Whitney |
| No. Of M2 | Cleavage | 6,3 | 4,5 | 1 | 31 | <0.001 | Mann-Whitney |
| No. Of M2 | Day 5 | 8,9 | 4,0 | 2 | 27 | <0.001 | Mann-Whitney |
| No. Of 2PN | Cleavage | 4,2 | 3,3 | 1 | 24 | <0.001 | Mann-Whitney |
| No. Of 2PN | Day 5 | 6,4 | 3,2 | 1 | 25 | <0.001 | Mann-Whitney |
| No. Of Embryos transferred | Cleavage | 1,8 | 0,5 | 1 | 3 | <0.001 | Welch |
| No. Of Embryos transferred | Day 5 | 1,9 | 0,5 | 1 | 3 | <0.001 | Welch |
Table 2: Comparison of basic characteristics of patients with the t-test value. p < 0.05 was considered significant.
An analysis comparing the baseline characteristics of the patients that could influence pregnancy rates found that age, number of oocytes retrieved, number of mature oocytes and number of oocytes fertilized showed a significant difference in the distribution between the cleavage and the blastocyst group.
Improvement of Pregnancy Rates From 2014 To 2018
Based on the significant difference between the groups, we added this information and other information as explained in “2.4 Statistical analysis” to the logistic regression model to correct the possible bias. A logistic regression analysis (Figure 1) with these variables to control their effect showed a calculated odds ratio of 1.4, i.e. from 2014 to 2018, per year there was an increase in the pregnancy rates by 1.4 times.
However, on scrutinizing the quality of embryos transferred (Figures 2-4), it was found that the number of ideal embryos for transfer had increased steady over the years (p<0.001). On further inspection, the number of ideal cleavage embryos did not show a significant increase (p=0.1) but, the increase in the number of ideal blastocysts was significant (p<0.001).
Based on the fact that the pregnancy rates improved over the years, we broke down the data to identify the factors that changed over 5 years. There was no variation in the basic patient characteristics and no significant changes in the stimulation protocol, type of gonadotrophin used and, timing and medication used for final oocyte maturation. There was no change in the method or timing of the oocyte retrieval or embryo transfer procedure. There was no change in the luteal phase support provided. In the clinics and the lab, the same documented standard operating procedures were followed from 2014 to 2018. A statistical analysis of the pregnancy rates between both the doctors based on who performed the oocyte aspiration (p=0.07) and embryo transfer (p=0.38) was done and no significant difference was found.
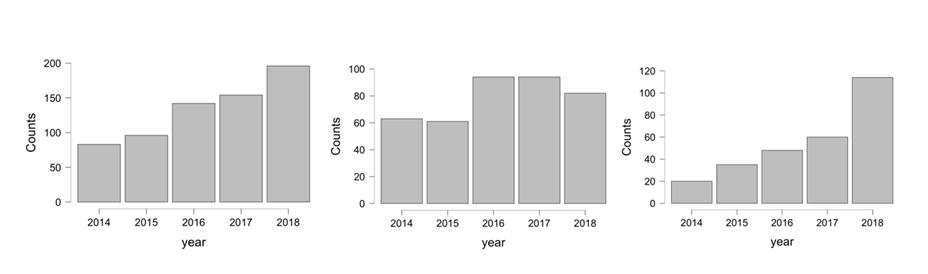
(a) (b) (c) (a)Total ideal embryos (b) Ideal cleavage embryos (c) Ideal day 5 embryos (cleavage + day 5) Figure 2: Histograms depicting the number of ideal embryos transferred each year. (a) number of total ideal embryos (cleavage + day 5) transferred (b) number of ideal cleavage embryos (c) number of ideal day 5 embryos transferred.
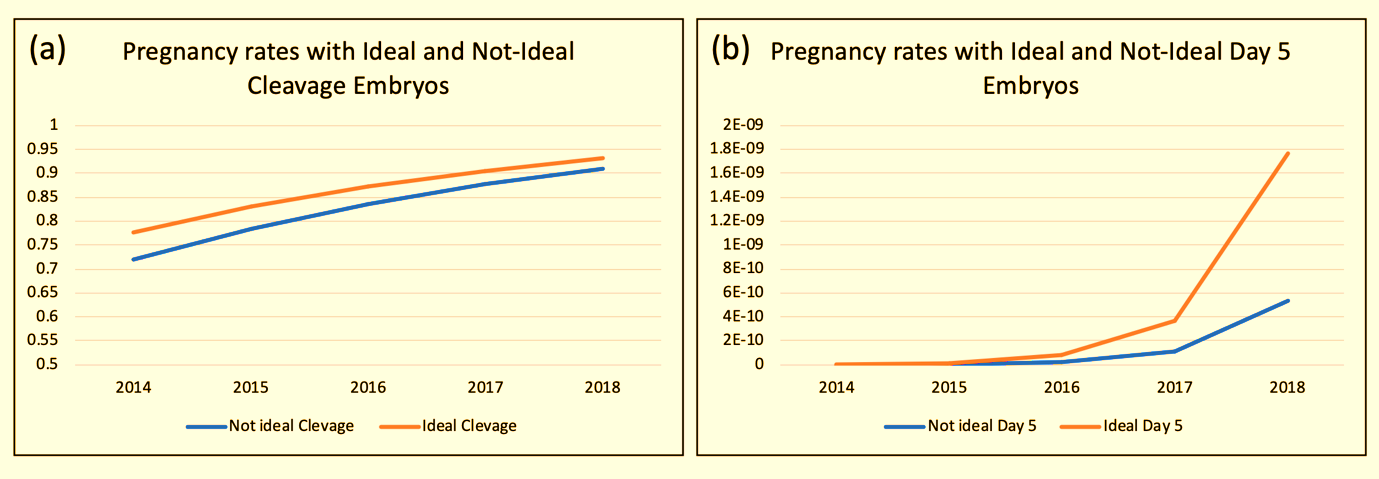
The pregnancy rates improved significantly (Figure 3) with the transfer of an ideal day 5 embryos compared to a not-ideal day 5 embryos (p=0.001). The pregnancy rates increased by 4.8 times each year with the transfer of ideal day 5 embryos.
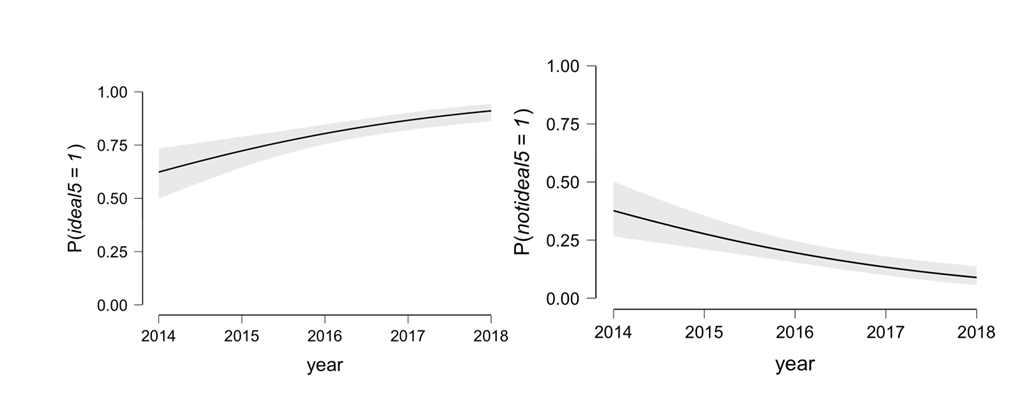
A logistic regression analysis (Figure 4) of the number of ideal day 5 embryos produced per year shows an increase by 1.5 times per year in the number of ideal day 5 embryos from 2014 to 2018. There was 4 times increase in numbers after the bench-top incubator was introduced and 8 times after the time-lapse incubator was introduced. While there was a rise in the number of ideal day 5 embryos, there was a simultaneous fall by 0.64 times in the number of not-ideal day 5 embryos per year.
| Pregnant | Not pregnant | Total | |
| Ideal Day 5 Embryo | 102 | 175 | 277 |
| Not-ideal Day 5 Embryo | 4 | 58 | 58 |
| 106 | 229 | 335 | |
| Figure 5: Clustered column showing patients who got pregnant compared to those who did not get pregnant after transfer of an ideal or not-ideal day 5 embryos. |
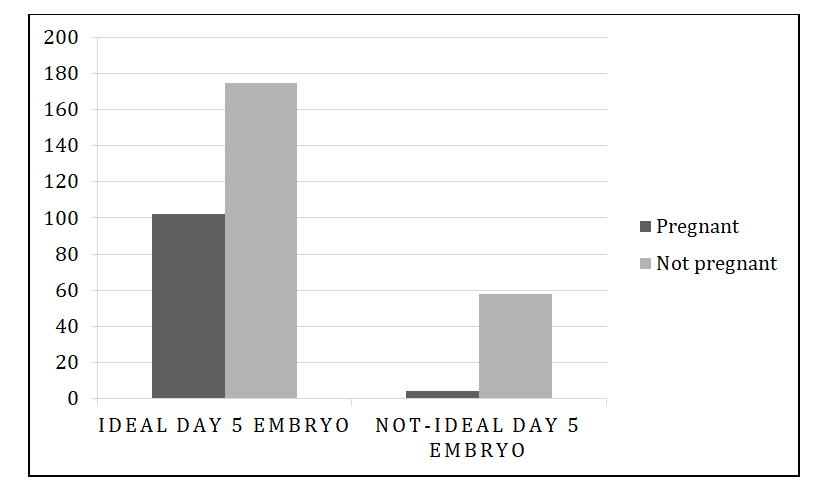
Extreme significance (Figures 5-7), p=0.0001, power 99%) was noticed when the pregnancy rates were compared between those patients who received a transfer of an ideal day 5 embryo and those that received a transfer of a not-ideal day 5 embryo.
While exploring the reason for increase in the number of ideal day 5 embryos leading to an improvement in the pregnancy rates, it was observed that there was no significant difference based on the embryologist who performed oocyte screening (p=0.37), the ICSI (p=0.68) or the embryo transfer (p=0.34).
There was no significant change in the operating protocols in the lab. The only significant change was addition of new culture incubators in the lab from 2014 to 2018. On further investigation, a significant difference (Figure 6, p=0.01) was found in the number of ideal embryos that resulted from the culture in each incubator.
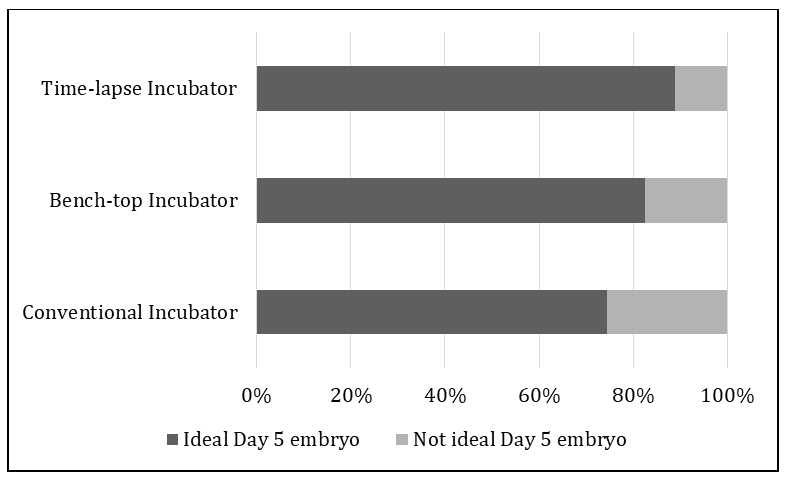
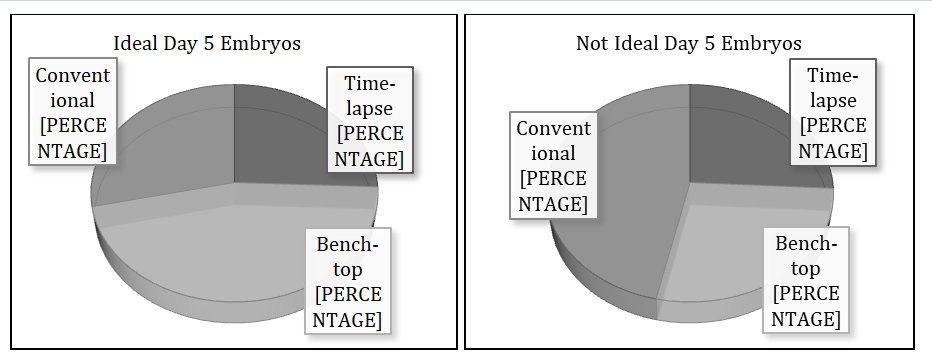
As depicted in Figures 6 & 7 and Table 3, the most ideal day 5 embryos were produced in the Bench-top / time- lapse incubators and the most not-ideal day 5 embryos were produced in the conventional incubator. Additionally, the comparison of the incubators with each other revealed there was no difference (Table 3), (p=0.23) in the production on ideal embryos between the bench-top and the time- lapse incubators and the most significant difference (Table, p=0.004, power 84%) in the culture of ideal embryos was seen between the conventional and the time-lapse incubators.
| Ideal Day 5 embryo | Not ideal Day 5 embryo | Total | |
|---|---|---|---|
| Conventional Incubator | 79 (75%) | 27 (25%) | 106 |
| Bench-top Incubator | 71 (83%) | 15 (17%) | 86 |
| Time-lapse Incubator | 127 (89%) | 16 (11%) | 143 |
| 227 | 58 | 335 (Grand total) |
Table 4: Percentages and absolute numbers of ideal embryos that developed in each culture incubator.
Culture conditions in the lab have been without question been proven to affect the pregnancy outcomes [14]. On evaluation of lab parameters that could have contributed to the improvement in pregnancy rates, it was observed that, pregnancy rates were significantly higher when an ideal blastocyst was transferred compared to a not-ideal blastocyst.
It has been observed that when the blastocyst morphology is “ideal”, i.e. a higher expansion grade, top quality inner cell mass and trophectoderm, it was found to be genetically euploid [15]. But, observing an ideal blastocyst in culture does not obviate the need for Pre-implantation genetic testing as flaws are noticed in time-lapse and in certain circumstances especially in older women, aneuploidy was in such embryos. An in-vitro study of the interaction between the endometrium and a good or bad quality embryo demonstrated that decidual cells are programmed to select embryos that are perceived to be competent to prevent investing energy in growth and development of a less viable embryo [16]. Hence, a higher pregnancy rate in ideal day 5 embryo transfer group could be explained by increased chances of implantation due to apparent euploidy and the active involvement of the endometrium as a bio-sensor in helping the ideal blastocysts implant.
In-vivo, a human embryo develops at a constant temperature of 37°C ±2 and the embryo has low oxygen (5%) environment [17] and a dynamic system around it always maintaining the right pH for its further development [18]. It is known that a change in the temperature by 2 degrees causes non-reversable damage in the spindle of the oocyte causing abnormal cleavage [19]. A change in the temperature could cause a change in the pH of the media which accounts for fragmentation in embryos [20]. It has been extensively studied that a low oxygen tension (5%) in incubators gives increased blastocyst rates and higher pregnancy rates [21].
The clear improvement of pregnancy rates were seen parallelly with the increase in the number of ideal day 5 embryos which were due to the shift in the culture conditions in the lab. The best culture condition for maximum ideal day 5 embryos was low oxygen (5%) with either bench-top incubator culture system or the uninterrupted time-lapse system.
The advantages of a time-lapse incubator [22] are that embryo development can be continuously monitored without physically removing them from the incubator with the advantage of maintaining a stable culture environment [23] and limiting the exposure of embryos to changes in gas composition, temperature, and movement. The Cochrane Review of 2019 states that the quality of evidence at present is insufficient to state that time-lapse incubators with uninterrupted culture are better than a conventional incubator [22].
The limitation of this study was that the sample size of blastocyst group was relatively small and not all proven and un-proven confounding factors were taken into account. A larger randomized controlled study should be carried out in the future to further confirm these findings.
Conclusion
The 1126 ART cycles that were performed from 2014 to 2018 in the University Reproductive Medical Unit of UKSH, Kiel showed that there was an improvement in pregnancy rates of 1.4 times every year from 2014 to 2018 in both cleavage stage transfer and blastocyst transfers. There was a significant rise in the pregnancy rates with blastocyst transfer compared to cleavage stage transfer as a direct result of increase in the number of morphologically ideal blastocysts cultured in the lab due to improvement in the lab culture conditions by shifting from conventional incubators which had atmospheric oxygen tension (21%) to the sustained stable culture conditions (temperature and pH) of bench-top and time-lapse incubators which had 5% oxygen. The improvement in culture conditions had a higher impact on day 5 rather than day 2/3 culture as it could be speculated that the blastocyst stage is more susceptible to changes in the culture environment than cleavage stage. Hence, ideal day 5 embryos were an excellent tool to assess the culture system in the lab. The limitation of this study was that the sample size of blastocyst group was relatively small and a larger randomized controlled study should be carried out in the future to further confirm these findings.
Conflicts of Interest
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
References
-
Jones GM, Trounson AO, Gardner DK, Kausche A, Lolatgis N, et al. (1998) Evolution of a culture protocol for successful blastocyst development and pregnancy. Human Reproduction 13(1): 169-177.
-
(2017) The Vienna consensus: report of an expert meeting on the development of ART laboratory performance indicators. Reprod Biomed Online 35(5): 494-510.
-
Hammond ER, Morbeck DE (2019) Tracking quality: can embryology key performance indicators be used to identify clinically relevant shifts in pregnancy rate? Hum Reprod 34(1): 37-43.
-
Balaban B, Brison D, Calderón G, Catt J, Conaghan J (2011) The Istanbul consensus workshop on embryo assessment: proceedings of an expert meeting. Hum Reprod 26(6): 1270-1283.
-
Kliebisch TK, Bielfeld AP, Krüssel JS, Baston-Büst DM (2016) The German Middleway as Precursor for Single Embryo Transfer. A Retrospective Data-analysis of the Dusseldorf University Hospital’s Interdisciplinary Fertility Centre - UniKiD. Geburtshilfe Frauenheilkd 76(6): 690-698.
-
Swain JE (2014) Decisions for the IVF laboratory: comparative analysis of embryo culture incubators. Reprod Biomed Online 28(5): 535-547.
-
Kasterstein E, Strassburger D, Komarovsky D, Bern O, Komsky A, et al. (2013) The effect of two distinct levels of oxygen concentration on embryo development in a sibling oocyte study. J Assist Reprod Genet 30(8): 1073- 1079.
-
Announcing JASP 0.12.
-
Cetin MT, Kumtepe Y, Kiran H, Seydaoglu G, et al. (2010) Factors affecting pregnancy in IVF: age and duration of embryo transfer. Reprod Biomed Online 20(3): 380-386.
-
Meldrum DR, Silverberg KM, Bustillo M, Stokes L (1998) Success Rate with Repeated Cycles of In Vitro Fertilization Embryo Transfer. Fertility and Sterility 69(6): 1005-1009.
-
Hariton E, Kim K, Mumford SL, Palmor M, Bortoletto P, et al. (2017) Total number of oocytes and zygotes are predictive of live birth pregnancy in fresh donor oocyte in vitro fertilization cycles. Fertil Steril 108(2): 262-268.
-
Mehta VP, Patel JA, Gupta RH, Shah SI, Banker MR, et al. (2018) One Plus One Is Better Than Two: Cumulative Reproductive Outcomes Are Better after Two Elective Single Blastocyst Embryo Transfers Compared to One Double Blastocyst Embryo Transfer. J Hum Reprod Sci 11(2): 161-168.
-
Goudas VT, Hammitt DG, Damario MA, Session DR, Singh AP, et al. (1998) Blood on the embryo transfer catheter is associated with decreased rates of embryo implantation and clinical pregnancy with the use of in vitro fertilization-embryo transfer. Fertil Steril 70(5): 878-882.
-
Wale PL, Gardner DK (2016) The effects of chemical and physical factors on mammalian embryo culture and their importance for the practice of assisted human reproduction. Hum Reprod Update 22(1): 2-22.
-
Minasi MG, Colasante A, Riccio T, Ruberti A, Casciani V, et al. (2016) Correlation between aneuploidy, standard morphology evaluation and morphokinetic development in 1730 biopsied blastocysts: a consecutive case series study. Hum Reprod 31(10): 2245-2254.
-
Macklon NS, Brosens JJ (2014) The human endometrium as a sensor of embryo quality. Biol Reprod 91(4): 98.
-
Kalleas D, McEvoy K, Horne G, Roberts SA, Brison DR (2020) Live birth rate following undisturbed embryo culture at low oxygen in a time-lapse incubator compared to a high-quality benchtop incubator. Hum Fertil (Camb) 2020: 1-7.
-
Sciorio R, Smith GD (2019) Embryo culture at a reduced oxygen concentration of 5%: a mini review. Zygote 27(6): 355-361.
-
Wang W-H, Meng L, Hackett RJ, Odenbourg R, Keefe DL (2001) Limited recovery of meiotic spindles in living human oocytes after cooling–rewarming observed using polarized light microscopy. Human Reproduction 16(11): 2374-2378.
-
Elder K, Van den Bergh M (2015) Troubleshooting and Problem-Solving in the IVF Laboratory. Cambridge: Cambridge University Press.
-
Gelo N, Kirinec G, Baldani DP, Vrcic H, Jezek D, et al. (2019) Influence of human embryo cultivation in a classic CO2 incubator with 20% oxygen versus benchtop incubator with 5% oxygen on live births: the randomized prospective trial. Zygote 27(3): 131-136.
-
Armstrong S, Bhide P, Jordan V, Pacey A, Marjoribanks J, et al. (2019) Time-lapse systems for embryo incubation and assessment in assisted reproduction. Cochrane Database Syst Rev 5: Cd011320.
-
Swain JE (2019) Controversies in ART: considerations and risks for uninterrupted embryo culture. Reprod Biomed Online 39(1): 19-26.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era