Cornual Ectopic Pregnancy: Diagnostic and Therapeutic Difficulties, a Case Report at the Teaching Hospital of Angre / Abidjan (Ivory Coast)
Cornual ectopic pregnancy (CEP) is defined by implantation of the ovular sac in the rudimentary horn of a bicorn uterus. By extension, pregnancies implanted in the horn of a partitioned uterus or in the stump of a fallopian tube in a patient who has undergone a salpingectomy are sometimes grouped under this definition. This is a rare pathology in daily practice and it represents about 2% of EP with a mortality rate of 2-2.5% per uterine rupture, doubled compared to other tubal ectopic pregnancy. We report a case of late evolutionary left cornual pregnancy in myomatous uterus, discovered with minimal blackish metrorrhagia with pelvic pain due to 10-week amenorrhea in a 30-year-old patient, gravida 7 primipara (5 spontaneous miscarriages). After a diagnostic wandering, the exploratory laparotomy confirmed a left cornual pregnancy in myomatous uterus. A cornual resection was carried out with simple postoperative recoveries.
Introduction
Ectopic pregnancy (EP) accounts for 2-3% of all pregnancies [1]. The etiologies of EPs are dominated by sexually transmitted infections including chlamydia trachomatis in developing countries. Despite technological progress, there are difficulties in the diagnosis of EP, particularly in cornual localization. Indeed, it is characterized by its clinical polymorphism, with as a major risk uterine rupture [2, 3]. Thus we report a case of cornual ectopic pregnancy whose particularity was the diagnostic difficulties as often encountered in an under-medicalized environment, in sub-Saharan Africa.
Background
This is a 30-year-old patient, gravida 7 primipara (5 spontaneous miscarriages). She presented with 10-11 weeks of pregnancy secondary amenorrhea and consulted for pelvic pain and minimal bleeding, with a positive urine betaHCG test. Clinically, the hemodynamic status was stable. Pelvic examination found a size of the uterus commensurate with gestational age of around 10 weeks and a finger cot bringing blackish blood. This prompted a first emergency ultrasound, which concluded in an undisturbed EP. The gestational sac was measured at 42 mm, is a gestational age of 09 weeks. The level of β HCG was 20,000 IU / ml. As the clinical examination was not revealing, in the absence of a laparoscopy, a second ultrasound was suggested. Rather, it concluded that an intrauterine pregnancy of 10 weeks + 2
days (Figures 1 & 2). Within 48 hours the second dosage of β HCG not having doubled a third ultrasound was performed by a referent sonographer. She demonstrated an extrauterine gestational sac but intra mural (Figure 3).

Figures 1 & 2: Diagnostic wandering with estimation of a 10-week evolutionary monoembryonic pregnancy in the intrauterine position.
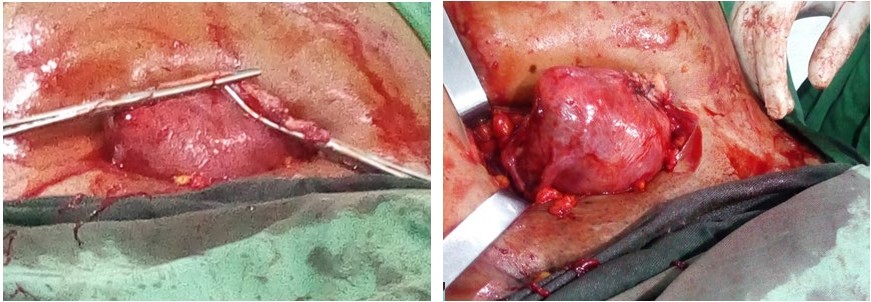
The indication of the exploratory laparotomy was set. This confirmed the left uterine ectopic pregnancy associated with a myomatous uterus (Figures 4 & 5). A left cornual resection associated with a basic myomectomy was performed (Figures 6 & 7). The surgical follow-up was simple. Chlamydia serology returned positive. The patient was placed on Azithromycin. 6-month contraception with a minidosed estrogen was instituted. The anatomopathological analysis of the surgical specimen revealed, in addition to the product of conception, proximal tubal lesions similar to chronic salpingitis.
Figures 4 & 5: Appearance of left cornual EP during exploratory laparotomy and presence of a sub-serous fibroma (FIGO type VII) next to the right horn.
Figures 6 & 7: Therapeutic aspects with left cornual resection and myomectomy.
Discussion
Cornual, interstitial and angular EPs are often grouped together and represent the same clinical and therapeutic entity. Strictly speaking, interstitial EP develops in the intramural portion of the proboscis. It is a canal 0.7 mm wide and about 1 to 2 cm long, the muscle wall of which allows relatively late development (7 to 16 weeks). The gestational sac is placed next to the round ligament [1]. Angular EP develops at the level of the tubal ostium at the bottom of the uterine horn. Unlike interstitial pregnancy, it is located in the axis of the round ligament. The risk of rupture is rarer here since it is an implantation in the endometrial cavity. A EP implanted in the rudimentary horn of a bicornuate uterus is defined as cornual. By extension this definition applies to pregnancies implanted in the horn of a septate uterus. Some also group under this definition the development of trophoblastic tissue on the remaining stump of a tube that has been treated by salpingectomy [4].
Cornual ectopic pregnancies (CEP) are rare, accounting for 2-4% of EPs [5, 6]. Their management is poorly codified, often guided by the clinical picture.Their development is longer and clinical signs later. Free peritoneal rupture is, however, frequent and often brutal. It is often very hemorrhagic and causes a catastrophic picture since the wall at this place is very vascularized. As a result, the mortality rate is doubled compared to conventional tubal EPs. Despite modern methods which allow increasingly early diagnosis and sometimes conservative treatment, their management remains problematic in an under-medical environment [3, 4, 7]. However, in certain situations the diagnosis of cornual pregnancy is difficult in the absence of laparoscopy [7], as was the case in our observation with this diagnostic wandering. As with classic EP, the diagnosis is essentially based on a summary of the clinic, the determination of plasma hCG and transvaginal ultrasound [8]. In summary, as described by Timor-Tritsch [9], there are three essential criteria: an empty uterine cavity, a gestational sac separated by more than 1 cm from the uterine cavity, a myometrial crown around this sac. are quite specific (88 to 93%) but the sensitivity, around 40%, is poor [10, 11]. Typically, the initial hCG level is often higher compared to tubal EPs. This is explained by the greater ease of the horn to undergo development related to pregnancy. Thus, compared to a conventional tubal EP, the interactions between the egg and its implantation bed would be of better quality, improving the kinetics of hCG. For the same reason, it is not uncommon to observe cardiac activity within these EPs [12, 13].
The treatment of ectopic pregnancy should be fully determined taking into account the general condition of the patient, the desire to have children, the results of the ultrasound, the serum hCG levels and the changes in the levels of hCG. Surgery and methotrexate drug therapy are commonly chosen treatments around the world. However, surgery is the first choice of treatment. Indeed, surgical procedures are widely used, safe and fast. In addition, medical treatment with methotrexate is not commonly used in developing countries. Laparoscopic surgery is the gold standard in industrialized countries, and above all allows the definitive diagnosis of cornual EP. But it has a second therapeutic goal, the smooth transition from observation to treatment at the same time of operation [14]. Randomized controlled trials comparing laparotomy to laparoscopic surgery for ectopic pregnancies were systematically reviewed in the 2007 Cochrane review. Compared to laparotomy, laparoscopic surgery offers a shorter duration of surgery (73 min versus 88 min. min), causes less perioperative bleeding (79ml vs. 195ml) and a shorter hospital stay (1 to 2 days vs. 3 to 5 days) and shorter recovery time (11 days vs. 24 days) [13].
Typical surgical procedures for EPs, as in our observation, are salpingectomy with corneal resection or cornuotomy [15]. Other teams perform medical treatment or salpingostomy when conditions allow, with conservative purposes [13]. It is also possible to initiate treatment with methotrexate supplemented by surgical treatment [5].
In terms of pregnancy prognosis, salpingostomy was reported to be less likely to increase the rate of intrauterine pregnancy than salpingectomy, while it significantly increases recurrent ectopic pregnancy. It was also reported that in tubal pregnancies, where the opposing fallopian tube gives normal results, laparoscopic salpingectomy does not decrease the incidence of postoperative intrauterine pregnancy, but decreases the chances of continuing extra pregnancy, uterine and recurrent ectopic pregnancies [2]. Therefore, treatment by laparoscopic surgery remains preferred. In all cases, cornual resection exposes the patient to uterine rupture, which should be kept in mind for the management of subsequent pregnancies.
Conclusion
Cornual EPs are rare diagnostic entities that pose a risk of short-term hemorrhagic rupture and medium-term recurrence. The therapeutic choice is guided mainly by the clinical picture. The fertility prognosis and subsequent obstetric prognosis appear to be similar to other EPs. More studies are needed to guide management based on HCG level or ultrasound criteria.
References
-
Jourdain O, Fontages M, Schiano A, Rauche F, Gonnet JM (2003) Management of other adnexal ectopias (cornual, interstitial, angular and ovarian. J Gynecol Obstet Biol Rprod 32(7): 93-100.
-
Hayata E, Tsuchiya T, Maemura T, Katagiri Y, Hasegawa T, et al. (2015) Recurrence of ectopic pregnancy in the rest of the fallopian tube after partial Ipsilateral salpingectomy. Open Journal of Obstetrics and Gynecology 5(7): 57946.
-
Neossi GM, Nkigoum NA, Nko’o A (2017) Late and fortuitous discovery of right corneal pregnancy on Routine Ultrasound. Health Sci Dis 18(4): 116-119.
-
Benifla JL, Bardou D, Sebban E, Darai E, Madelenat P (1997) Unusual locations of ectopic pregnancy. Fernandez H. Ectopic pregnancy.
-
Dagar M, Srivastava M, Ganguli I, Bhardwaj P, Sharma N, et al. (2018) Interstitial and Cornual Ectopic Pregnancy: Conservative Surgical and Medical Management. J Obstet Gynaecol India 68(6): 471-476.
-
Nikodijevic K, Bricou A, Benbara A, Moreaux G, Nguyen C, et al. (2016) Cornual ectopic pregnancy: management, subsequent fertility and becoming obstetric. Gynécologie Obstétrique & Fertilité 44(1) : 11-16.
-
Bentin C, Grandjean F (2016) A rare case of ectopic pregnancy: corneal pregnancy after salpingectomy. Louvain Médical 12: 693-697.
-
Kouamé N, N’Domoua A, N’Gbesso R, Keita A (2011) Cornual pregnancy: a rare entity of ectopic pregnancy. Imagerie de la femme 21(2) : 68-71.
-
Timor Tritsch IE, Monteagudo A, Matera C, Veit CR (1992) Sonographic evolution of cornual pregnancies treated without surgery. Obstet Gynecol 79(6): 1044-1049.
-
Fisch JD, Ortiz BH, Tazuke SI, Chitkara U, Giudice LC (1998) Medical management of interstitial ectopic pregnancy: a case report and literature review. Hum Reprod 13(7): 1981-1986.
-
Mishell DR (1992) Comprehensive Gynecology. Herbst AL, Mishell DR, Stenchever MA Droegmuller W. St Louis MI USA, Mosby Year Book Inc pp: 457-490.
-
Hajenius PJ, Mol F (2007) Interventions for tubal ectopic pregnancy. Cochrane Database of Systematic Reviews 24: CD000324.
-
Dubuisson JB, Morice P, Chapron C (1996) Salpingectomie - Le choix chirurgical laparoscopique pour la grossesse extra-utérine. Reproduction humaine 11: 1199.
-
Taran FA, Kagan KO, Hübner M, Hoopmann M, Wallwiener D, et al. (2015) The Diagnosis and Treatment of Ectopic Pregnancy. Dtsch Arztebl Intv 112(41): 693-704.
-
Prenaud C, Scherier S, Malgras B (2017) Management of a corneal ectopic pregnancy. Journal of Visceral Surgery 154(6): 467-468.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era