The National HIV Curriculum: Howard University’s Innovative Approach to Strengthening the Nation’s HIV Clinical Workforce
HIV has remained a stubborn burden in the African American community. HIV-experienced clinicians are critical for positive outcomes that align with the HIV care continuum. Howard University (HU) used the National HIV Curriculum (NHC,2015) via distance base technology to fill the void and strengthen HIV care, particularly among students and faculty at our Historically Black Colleges and Universities (HBCUs). One major program success was HUs ongoing ability to access a dedicated core of health sciences faculty to champion the NHC. This approach ensured the successful integration of the NHC into the course offerings at the various HBCUs. The effective integration was accomplished despite the unequal challenge that the COVID-19 pandemic unleashed on the vulnerable communities served by our HBCUs. The project success was achieved through the development and strengthening of ongoing partnerships with our cohort of HBCUs, conducting ongoing needs assessments and responding promptly to the findings, emphasizing training opportunities in addition to the NHC, and providing on-demand technical assistance and resources to our partners. Howard University surpassed by 459% its original goal of engaging 1964 students to take the NHC. At the conclusion of the four-year project performance period 10,983 students completed all or part of the NHC.
Introduction
The overarching goal of the Howard University National HIV Curriculum Project (H-NIP) [1] was to expand the HIV clinical workforce by assisting health profession program (HPP) students at Historically Black Colleges and Universities (HBCUs) to receive specialized training in the care and management of persons living with HIV/AIDS by completing all or part of the NHC [2]. Released in 2017, the NHC is a free, online curriculum targeting multidisciplinary, novice-to- expert health professionals, students, and faculty who treat or aspire to treat people with or at risk for HIV meet the core competency knowledge for the disease. The focus of the plan is to strengthen existing accredited academic and training programs and curricula of multiple health professions institutions with HIV competencies. The emphasis is on nursing, medical, pharmacy, and dental programs, including graduate education/residency programs.
The expected impact is an enhancement of the student’s knowledge, skills, and overall HIV competence with respect to the treatment of People with HIV (PWH). Credit towards a health care degree or certificate for the health care professional is one expected benefit of this effort. The NHC consists of 6 modules that included Screening and Diagnosis, Basic HIV Primary Care, Antiretroviral Therapy, Co-Occurring Conditions, Prevention of HIV, and Key Populations. This module contain thirty-seven lessons and is deemed ideal for health professions programs to use in an effort to prepare students to medically manage People with HIV (PWH). The Curriculum was developed with support from the Health Resources and Services Administration HIV/AIDS Bureau (HRSA HAB). The long-term outcome of this initiative is to enhance the quality of HIV Centers and competently care for PLWH.
Project Justification
In the U.S., HIV disproportionately impacts ethnic minorities, particularly African Americans, and this cohort of individuals are also more likely to live in medically underserved areas and to prefer being treated by ethnic minority providers [3, 4]. The majority of physicians of color are more likely to work in medically underserved areas and to treat racial/ethnic minorities than non-minority physicians Goodfellow, et al. [5] Marrast, et al. [6]. Among Black physicians currently in practice the majority receive their training from a HBCU [7].
More than 35 years into the HIV epidemic, HIV remains a quandary of exceptional proportions for public health. And, even as we move from crisis to control, the estimated 1.1million people in the United States living with HIV is expected to increase [8]. Data show that health care for PWH has improved substantially, as evidenced by prognosis and life expectancy over the past two decades Trickey, et al. [9]. This is so because, despite not having a vaccine or a cure, there are ongoing scientific breakthroughs that have yielded tools to alter the course of this pandemic by controlling it. Disturbingly, workforce data indicate that the number of well-trained providers who manage PWH is declining, due to retirement and other factors such as young providers are choosing medical careers outside of HIV and primary health care and several are not adequately exposed to HIV training during pre-professional education since HIV medicine is not taught in many health professions academic or training programs because it is generally not required by school accrediting agencies. Furthermore, many do not manage sufficiently large caseloads to hone their skills in HIV treatment and care. Despite this, the demand for their services is increasing with an estimated shortage equaling roughly 30 percent of the actual supply of providers [10, 11]. Furthermore, as more PWH who are out of care, are successfully linked and retained, and the HIV population ages, the need for clinicians to provide HIV primary care will increase, particularly among clinicians with extensive experience in providing both HIV care and the management of multiple chronic conditions.
This pattern prevails despite many studies establishing that providers who have received specialized training in HIV care and treatment and who manage large volumes of patients, regardless of their discipline, deliver better quality care and report better patient outcomes than low volume providers and those lacking specialized HIV training Landovitz, et al. [12]. For example, studies have found that HIV clinical pharmacists have patients with HIV who are more adherent to their medication and have better viral suppression than pharmacists who lack HIV specialization Saberi, et al. [13].
The lack of HIV providers is further exacerbated by the shortage of primary care providers that, regardless of their training or experience, can assume the responsibility of managing PWH. The national map of Health Professional Shortage Areas (HPSA) [14] indicates the shortage is particularly acute in urban areas and the deep South where HIV prevalence is higher. The lack of providers with the requisite skills and experience in treating PWH negatively impacts the availability of qualified instructors to deliver HIV care content to HPP students and/or provide the experiential learning opportunities that have been identified earlier as a key training need for students. The lack of focus on HIV during clinical training cuts across disciplines and ultimately affects the number of HIV-trained clinicians available to serve PWH [15] Watt N, et al. [16] A nationwide survey of family medicine residency program directors, for example, found that only 25% thought that the graduates in their programs were adequately trained in HIV primary care and the majority (79%) thought that their existing curriculum should be modified and/or faculty capacity increased to address HIV more adequately Prasad, et al. [17]. Furthermore, fewer than 25% of the program directors reported having a formal HIV curriculum as part of the residency course. They also lacked faculty with HIV expertise to deliver training on HIV care and treatment.
Some providers themselves recognize the inadequacy of their preparation to manage PWH. A survey of internal medicine residents in four large U.S. cities revealed that while 50% had 30 or more inpatient HIV encounters in the 12 months prior to the survey, the majority had little or no outpatient experience managing PWH. In fact 39% felt unprepared to deliver HIV outpatient care as many residents lacked the opportunities to provide such care and typically only saw between 1 and 5 patients Phillips, et al. [18].
However, although there is no credentialing process for HIV specialization, the American Academy of HIV Medicine (AAHIVM) requires providers to be managing at least 20 patients before they are eligible to take the AAHIVM HIV specialist certification exam [10]. Thus most internal medicine residents would be ineligible.
The groundwork has been laid to develop a core-set of competencies that primary care providers must have in order to develop quality care Portillo, et al. [19, 20]. Additionally, various programs have been launched to improve the capacity of different disciplines to provide quality HIV care Farley, et al. [21, 22, 23] and by and large these have been successful. For example, an evaluation of HRSA HAB’s Community-Based Dental Partnership Program (CBDPP) found that after a community-based rotation dental students who had the opportunity to treat PWH showed an increased knowledge of and willingness to treat PWH when compared to prior their rotation knowledge and attitudes Hamershock, et al. HRSA-Ryan White [24, 25]. However, the proposed project involves a comprehensive effort to focus on several disciplines at multiple institutions with the goal of effecting systemic change in the way clinicians are trained to manage PWH nationwide.
In light of these data, HRSA HAB seeks to promote completion of the NHC as part of its workforce pipeline strategy to ensure that there is cadres of culturally competent, trained professionals available to serve the communities that are most impacted by HIV. H-NIP sought to engage the faculty and students to:
- collaborate with the H-NIP team on integrating the NHC into their respective training curricula by allowing the Howard team to review their training curricula and provide recommendations on how to integrate the NHC into their existing curricula and/or develop a stand -alone NHC course;
- nominate at least two faculty members to attend training on the NHC;
- provide the necessary support to the trained faculty members to begin teaching the NHC curriculum no later than month 4 of year 2 of the grant;
- enroll at least quarter of the students in the program in the elective NHC course offered in Year 1 of the grant;
- enroll at least half of the students in the program in the NHC course offered in Years 2 and 3 of the grant; and
- Provide input on the accreditation of the NHC course as a mandatory part of the training requirements for their respective programs. Howard’s proposal to HRSA promised to assist 1964 HBCU health profession program (HPP) students to complete all or part of the NHC by the end of the project’s performance period in August 2022.
Methods
Baseline and Follow-up Technology Assessment and Support
Howard understood that most HBCUs operate under severe resource constraints that hampered their ability to benefit fully from the NHC e-learning platform. Therefore, we retained a seasoned health information technology consultant to assess and enhance the capacity of each participating HPP to access and utilize the NHC e-learning platform effectively and efficiently starting in Year 1. The consultant then provided on-demand tech support to faculty and students who encountered difficulties in registering for the NHC or accessing NHC content. The consultant also provided technical assistance (TA) to HPP faculty on how to access and evaluate students’ NHC performance records. In subsequent project years, the consultant continued delivering tech support, including onboarding HPPs who were newly recruited to the project.
Tailored Technical Assistance (TA)
Although H-NIP partners are HBCUs, they are not a homogenous group. Therefore, throughout the life of the program we held regularly scheduled, one-on-one discussions with each HPP. These exchanges set priorities and expectations for project implementation, provided a forum to respond to the HPP’s inquiries and led us to proactively identify challenges and opportunities. As a complement to the periodic check-ins, at the start of each program year, H-NIP program staff conducted additional annual in-depth needs assessment with each HPP to inform the design, development, and delivery of culturally tailored support. Based on these inquiries, we recognized that HPPs varied in their ability to integrate the curriculum. Thus, we employed a culturally sensitive tailored approach as was warranted to successful integration.
Identification of NHC Champions within each HPP
When recruiting HPP partners, we identified an NHC faculty champion at each program. This individual helped to market H-NIP to program faculty and students and to ensure a consistent pipeline of students in the program. We selected champions based on their ability and commitment to be fully engaged with H-NIP and their relationship with the leadership (program Chairs, Deans, Provosts, Presidents) at their respective institutions, whose support was needed to facilitate NHC integration. The champions also leveraged their respective resources with credentialed professionals, academic institutions, and professional associations to facilitate the integration efforts.
A Faculty Train the Trainer (TOT) Program
The H-NIP Faculty TOT enhanced the capacity of HPP faculty to support students in completing the NHC. Needs assessments that we conducted in the first year of the program revealed that many HPP faculty lacked the expertise to assist students with various components of the NHC. Therefore, we engaged seasoned HIV clinicians and academicians to provide culturally competent training and support to faculty so that they in turn could assist their institutional peers to promote the NHC successfully within their departments and among their students.
The TOT instructors employed real-life case studies to enhance faculty trainees’ knowledge and skills relative to HIV clinical decision making and concepts addressed in the NHC. Even after the project concludes, the H-NIP Faculty TOT case study bank will remain freely accessible to HPP faculty at HBCUs and other institutions who are interested in honing their HIV clinical skills and learning about the NHC. The TOT webinars and virtual office hours created a forum for expert and peer-peer consultation and created mentoring relationships that we anticipate will continue beyond the life of H-NIP.
At the conclusion of the project 46 faculty members, including all NHC Champions, had completed the six-week long TOT. TOT participants represented 24 HPPs and 18 institutions. At the conclusion of the TOT, each trainee developed and implemented a plan to engage faculty at his/ her institution to adopt the NHC and promote it to their students. This effort ensures the sustainability of the NHC integration effort beyond the HRSA funding period. Increased Access to Educational Resources for Our Implementing Partners: In addition to the online TOT instructional resource library, H-NIP leveraged other resources to enhance HPP faculty’s knowledge and skills. The Howard University Telehealth Training Center’s website became a resource hub for our partners. The site provides a plethora of resources including journal articles from our Louis Stokes Health Library, updates from HRSA, CDC, NIH, and other government as well as non-governmental academic bodies in addition to current and seminal HIV-related resources that HPP faculty used to inform their NHC integration efforts.
Implementation Challenges
The lengthy process of curriculum approval at many of the HPPs posed a challenge for NHC integration. Therefore, we had to amend our initial plan to fully integrate the NHC into existing curricula and instead work with HPP faculty to integrate the NHC as a curriculum supplement. To increase uptake of the NHC most HPP faculty opted to promote the NHC as an extra credit option, although a few did require NHC completion as a prerequisite for receiving a final grade in the course.
An additional challenge was the packed HPP schedules. Time constraints prevented several HPPs from requiring students to complete the entire NHC. Instead, HPP faculty opted to steer students towards the HPP modules that were most relevant to students’ interests and future career goals. For example, pharmacy HPPs required their students to complete the NHC ARV module.
Finally, the COVID-19 pandemic posed numerous disruptions to HPP instructional schedules. HPPs started late, with some not opening after the lockdown in March 2020 until January 2021. Faculty reported that due to the retirement and resignation of some of their peers, their teaching workload increased significantly. Students’ workloads also increased as some were forced to take courses that they had missed or those that were not offered during the prior academic year because of the COVID-19 related lockdown. This created financial hardships for some of our HBCU students. Consequently, they had to seek part-time employment, thereby lessening the time available for their studies. This included taking and completing the NHC. Once classes resumed, several institutions switched to distance learning or a hybrid of distance learning and in-person instruction. These changes created additional challenges for faculty and students to remain engaged, as they lacked the peer interactions that are present during in-person learning.
Core H-NIP Performance Measurement Data
Howard University surpassed by 459% its original goal of engaging 1964 students to take the NHC. At the conclusion of the four-year project performance period, we reported that 10,983 students completed all or part of the NHC. This total represents 7,716 students from our HBCU partners, and 3,267 from our associate Chamberlain University. Furthermore, 51 faculty completed the NHC. Additionally, the sustainability of our work is ensured by the legacy of the H-NIP Faculty Training-of-Trainers (TOT), which includes not only trained faculty at each of our academic HPPs but also a freely accessible online library of case studies and other instructional materials designed to enhance faculty’s ability to support students in completing the NHC.
Our efforts led to almost 7000 students expressing an interest in working in the field of HIV clinical care upon completion of their health profession studies. Our work is expected overall, to diversify and strengthen the HIV clinical workforce pathway by expanding the overall health care professionals who are motivated, educated, and knowledgeable in areas to counsel, diagnose, treat, and medically manager people with HIV (Tables 1 & 2).
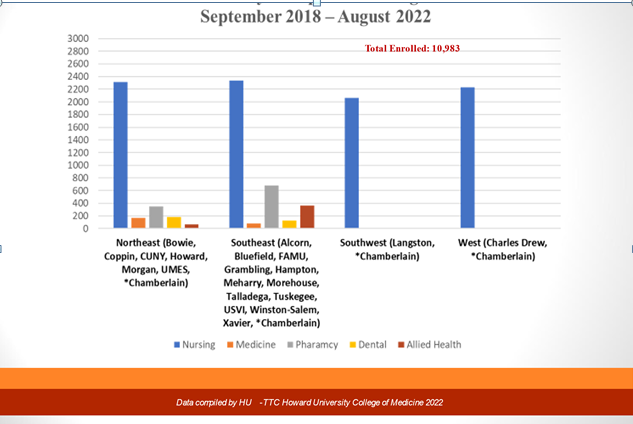
As shown in the following chart, nursing was by far the mostly commonly represented discipline followed by pharmacy with medicine and allied health tying for third place. Given this enrollment pattern, not surprisingly, the NHC was integrated most often into nursing curricula.
Figure 1 show the number of students trained and the associated disciplines. Dentistry was the discipline that reported the highest proportion of students completing the entire six-module NHC. Although nursing, because of the large number of nurse enrolls, reported the highest number of students completing the entire curriculum. As a discipline, nurses were the most trained across all geographic regions. In the Southeast pharmacists, and allied health professionals were the most trained whereas; in the Northeast pharmacists were the most trained (Figure 1).
| Measure | Value |
|---|---|
| Program Reach | |
| Institutional Engagement | |
| # of HBCUs recruited | 20 |
| # of HPPs introduced to the NHC | 28 |
| # of HPPs with faculty trained to offer the NHC | 51 |
| Disciplines represented by the faculty trained to offer the NHC | Nursing- 30; Pharmacy – 8; Allied health 6; Medicine 4; Dentistry -3; |
| Student Enrollment | |
| # of students enrolled in NHC courses | 10,983 |
| Disciplines represented by student enrollees | |
| Nursing | 6044 (78% of Total enrollment) |
| Pharmacy | 781 (10%) |
| Medicine | 272 (3.5%) |
| Allied Health | 270 (3.5%) |
| Dental | 246 (3.1%) |
| Other | 103 (1.3%) |
| NHC Integration | |
| # of courses that integrated the NHC | 40 courses |
| # of courses that integrated the NHC by discipline | |
| Nursing | 20 courses |
| Pharmacy | 10 courses |
| Medicine | 4 courses |
| Dentistry | 3 courses |
| Allied Health | 3 courses |
| Program Outcomes | |
| % of students earning CME/CNE for completing NHC modules | 79% |
| % of students completing the entire NHC | 4% |
| % of students by discipline completing the entire NHC | |
| Dental | 48% |
| Medicine | 39% |
| Allied Health | 19% |
| Other | 19% |
| Nursing | 2% |
| Pharmacy | 2% |
Table 1: H-NIP Performance Measurement Data.
Impact of the Overall Project
Despite the myriad and devastating challenges brought on by the COVID-19 pandemic and the subsequent death and early retirement of faculty from our HBCUs, we were able to staff the entire project throughout the funding period without delays. The ready pool of trained faculty from our Training-of-Trainers (TOT) made this replacement seamless. Consequently, we were able to continue to strengthen and expand our pool of students and faculty alike with our readily available resources.
We successfully grew our partnership to 28 programs from 20 HBCUs. This means that we were able to train far greater number that we proposed as noted earlier in this report . Ensuring sustainable support for the NHC at each institution was a key goal for this project. Almost 40 percent of our partners developed individual syllabus to accompany the NHC and in so doing help to ensure that this training would be fully integrated into the course offerings for years to come. During year 1, a total of 699 students enrolled to complete the curriculum; in year 2 we experienced a 99% increase with a total of 1,390 students enrolled. In year 3, 5043 students enrolled for an increase of 263% over year 2 and a 621% increase over year 1. In year 4 a total of 10,983 students participated. This was a 118% increase enrollment from year 3.
We conducted annual student surveys to assess the impact of the NHC on students’ self-perceived competency in HIV clinical skills and interest in working in HIV clinical care. As shown in Table 3 below, students’ self-perceived efficacy with respect to different domains of HIV clinical skills increased significantly once students completed the relevant NHC modules. Interviews conducted with HPP staff and H-NIP student participants indicated that the ARV modules were the hardest for students to master. Thus, not surprisingly, this module had the lowest student self-efficacy rating of the six (6) NHC modules. Interest in working in HIV clinical care increased after completion of the NHC with 16% more students indicating an interest in this career option than prior to taking the NHC.
| Measure | Value | |
|---|---|---|
| Self-reported competency in HIV clinical care | Pre NHC | Post NHC |
| % of students feeling competent overall relative to HIV clinical care | 44 | 90 |
| % of students feeling competent in HIV Screening and Diagnosis | 43 | 95 |
| % of students feeling competent in HIV primary care | 45 | 93 |
| % of students feeling competent in ARV therapy | 39 | 88 |
| % of students feeling competent in Co-Occurring Infections | 40 | 92 |
| % of students feeling competent in HIV Prevention | 50 | 97 |
| % of students feeling competent in HIV and Key Populations | 48 | 97 |
| Interest in working in the field of HIV clinical care | ||
| % of students expressing an interest in becoming an HIV clinician prior to taking the NHC | 73% | |
| # of students expressing interest in becoming an HIV clinician after taking the NHC | 89% |
Table 2: Student’s Self-Perceived Efficacy.
Implications
H-NIP demonstrated that it is possible to assist HBCUs, where the majority of Black clinicians are trained, to integrate the NHC in their health profession program curricula. This achievement occurred despite the challenges posed by the COVID-19 epidemic. However, lack of funding prevented us from tracking students to verify whether their expressed interest in a career in HIV clinical care over time, came to fruition. Likewise, we were unable to follow up with faculty TOT graduates to ascertain whether they continue to promote the NHC and support students in completing all or part of the curriculum. Future studies should build the case for promoting the NHC by exploring the association with uptake of the NHC and a career, rather than merely the intent to pursue a career, in HIV clinical care.
Another area of future study is capacity building for HBCU faculty to enable them to contribute more fully to shape the next generation of HIV clinicians. Our project revealed the persistent resource challenges that impede HBCU faculty’s engagement in strengthening the HIV clinician pipeline. Future research should identify targeted interventions to redress this lack.
References
-
Spach DH, Wood BR, Kalapila AG, Budak JZ (2015) In: Spach DH, et al. (Eds,). National HIV Curriculum. Hiv. Uw.edu; NCH.
-
Adams J, Chacko K, Guiton G, Aagaard E (2010) Training Internal Medicine Residents in Outpatient HIV Care: A Survey of Program Directors. Journal of General Internal Medicine 25(9): 977-981.
-
CDC (2019) HIV by Race/Ethnicity. U.S. Department of Health & Human Services Centers of Disease Control and Prevention.
-
Nelson A (2003) Unequal treatment: confronting racial and ethnic disparities in health care. Choice Reviews Online 40(10): 5843.
-
Goodfellow A, Ulloa JG, Dowling PT, Talamantes E, Chheda S, et al. (2016) Predictors of Primary Care Physician Practice Location in Underserved Urban and Rural Areas in the United States: A Systematic Literature Review. Academic Medicine: Journal of the Association of American Medical Colleges 91(9): 1313-1321.
-
Marrast LM, Zallman L, Woolhandler S, Bor DH, McCormick D (2014) Minority Physicians’ Role in the Care of Underserved Patients. JAMA Internal Medicine 174(2): 289-291.
-
AAMC (2017) Association of American Medical Colleges at a Glance: Black and African American Physicians in the Workforce.
-
HIV (2021) US Statistics, HIV.
-
Trickey A, May MT, Vehreschild J, Obel N, Gill MJ, et al. (2017) Survival of HIV-positive patients starting antiretroviral therapy between 1996 and 2013: a collaborative analysis of cohort studies. The Lancet HIV 4(8): e349-e356.
-
Gatty R (2016) The American Academy of Hiv Medicine www.aahivm.org August 2016 Patient Care. In: Gatty R (Ed.). Practice Management & Professional Development Information for HIV CARE Providers HIV Specialist. The American Academy of HIV Medicine.
-
SCRIBD (2014) NACO Annual Report 2012-13 - English | PDF | Hiv/Aids | Sexually Transmitted Infection.
-
Landovitz RJ, Desmond KA, Gildner JL, Leibowitz AA (2016) Quality of Care for HIV/AIDS and for Primary Prevention by HIV Specialists and Nonspecialists. AIDS Patient Care and STDs 30(9): 395-408.
-
Saberi P, Dong B, Johnson M, Greenblatt, Cocohoba J (2012) The impact of HIV clinical pharmacists on HIV treatment outcomes: a systematic review. Patient Preference and Adherence (6): 297-322.
-
HRSA (2019) Health Resources and Services Administration Shortage Areas. U.S. Department of Health & Human Services.
-
Siegler EL, Brennan-Ing M (2017) Adapting Systems of Care for People Aging With HIV. Journal of the Association of Nurses in AIDS Care 28(5): 698-707.
-
Watt N, Sigfrid L, Legido-Quigley H, Hogarth S, Maimaris W, et al. (2017) Health systems facilitators and barriers to the integration of HIV and chronic disease services: a systematic review. Health Policy and Planning 32(4): iv13-iv26.
-
Prasad R, Amico FD, Wilson SD, Hogan L, Nusser JA, et al. (2014) Training family medicine residents in HIV primary care: a national survey of program directors. Family Medicine 46(7): 527-531.
-
Phillips KA, Cofrancesco J, Sisson SD, Wu AW, Bass EB, et al. (2010) A Multicenter Study of Internal Medicine Residents’ Perceptions of Training, Competence, and Performance in Outpatient HIV Care. Aids Patient Care and Stds 24(3): 159-164.
-
Portillo CJ, Stringari-Murray S, Fox CB, Monasterio E, Rose CD (2016) The HIV Primary Care Workforce of Tomorrow: The UCSF Integrated HIV/AIDS Primary Care Capacity Nurse Practitioner Program. Journal of the Association of Nurses in AIDS Care 27(3): 214-222.
-
Relf MV, Harmon JL (2016) Entry-Level Competencies Required of Primary Care Nurse Practitioners Providing HIV Specialty Care: A National Practice Validation Study. Journal of the Association of Nurses in AIDS Care 27(3): 203-213.
-
Farley JE, Stewart J, Kub J, Cumpsty-Fowler C, Lowensen K, et al. (2016) Development of The Johns Hopkins University School of Nursing Adult/Geriatric Primary Care Nurse Practitioner Program in HIV Prevention, Treatment, and Care. Journal of the Association of Nurses in AIDS Care 27(3): 223-233.
-
Fessler DA, Huang GC, Potter J, Baker JJ, Libman H (2016) Development and Implementation of a Novel HIV Primary Care Track for Internal Medicine Residents. Journal of General Internal Medicine 32(3): 350-354.
-
McGee KS, Relf M, Harmon JL (2016) The Development of an HIV Training Program for Nurse Practitioners. Journal of the Association of Nurses in AIDS Care 27(3): 240-245.
-
Hamershock RA, Rajabiun S, Fox JE, Mofidi M, Abel SN, et al. (2014) Dental Students’ HIV/AIDS-Related Knowledge, Attitudes, and Intentions: Impact of the U.S. Health Resources and Services Administration’s Community-Based Dental Partnership Program. Journal of Dental Education 78(8): 1106-1117.
-
HRSA-Ryan White HIV/AIDS Program (2022) Part F: Dental Programs | Ryan White HIV/AIDS Program. Ryanwhite.hrsa.gov.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era