The Impact of Labour Induction at 38-39 Weeks Period of Gestation versus Expectant Management in Low Risk Pregnancies
Background: The recommendations for induction of labour have been restricted to postdated pregnancies, though many studies have assessed the safety of elective induction at term. The aim of the current study was to assess the outcomes of elective induction of labour at 38-39 weeks period of gestation among low risk pregnancies. Methodology: This was a hospital based observational study, on 134 subjects assessed for fetal well-being and induced based on Bishop’s score. The labour and perinatal outcomes were compared between pregnant women subjected to elective induction of labour & expectant group. Results: Of the 67 subject in the electively induced group, 28.4% delivered by a caesarean section in comparison to 31.3% of the 67 subjects in the expectant group (p-0.143). The mode of delivery in either of the groups was independent of the method of induction & parity. The mean induction to delivery time, maternal outcomes and duration of hospital stay was similar in the 2 groups. Fetal outcomes analyzed by NICU admissions was similar in the 2 groups (p-0.635), though the admissions were significantly more in the electively induced group who underwent caesarean section (p-0.001). Conclusion: Induction of Labour at 38-39 weeks in low-risk women did not result in increase in caesarean section or composite adverse perinatal outcomes. Our data may help low-risk women and their clinicians make decisions regarding benefits of induction of labour at term in an institutional setting.
Introduction
Current obstetric practices aim at improving the safety of the mother and her new born during antepartum, intrapartum & postpartum period. Induction of labour refers to the iatrogenic stimulation of uterine contractions before the onset of spontaneous labour with or without rupture of membranes to achieve vaginal delivery [1].
The NICE clinical guideline 70 (NICE CG70) suggests that women with uncomplicated pregnancies should be offered labour induction between 41 and 42 completed weeks to avoid the risks of prolonged pregnancy [2]. But many observational studies and systematic reviews have suggested that elective induction of labour at term may reduce perinatal mortality and morbidity [3, 4, 5], and may even lower the risk of caesarean birth [6, 7]. 2 large randomized controlled trials have compared the labour outcomes following elective induction versus expectant management in uncomplicated pregnancies. One trial was from the United Kingdom, conducted on nulliparous women aged between 35-39 years, induced electively at 39 weeks of gestation.
The labour outcome was compared with women who were expectantly managed. The study reported no increase in the rate of caesarean birth in the electively induced group [8]. The Arrive (A Randomized Trial of Induction Versus Expectant Management) trial, performed in the United States, reported a decrease in caesarean birth in nulliparous women who were induced electively at 39 weeks gestation [9].
The goal of the current study was to compare maternal and infant outcomes in nulliparous and multiparous births at 38-39 weeks of gestation that underwent elective induction of labour (induction without a medical indication) compared with pregnancies that were managed expectantly.
Methodology
This was a hospital based observational study carried out on 134 women delivering in the Department of Obstetrics and Gynecology at AJ Institute of Medical Sciences and Research Institute.
Hospital protocol for induction of labour
All patients are admitted to the hospital 1 day in prior and routine scan with biophysical profile & NST is done. This would assist in assigning the gestational age and estimated fetal weight. The method of the induction is based on the Bishop’s score. If Bishop’s score is unfavorable, Dinoprostone gel is used for cervical ripening every 6 hours for a total of 4 doses in all the cases except in cases of prelabour rupture of membranes, where tablet Misoprostol 25 mcg is used every 4 hourly for a maximum of 6 doses orally. The patients having a favourable cervix (Bishop’s score >7) are induced with Oxytocin. Usage of the oxytocin drip in titrated doses & artificial rupture of membranes is used to augment labour. The patients who do respond to the above protocol over 24 hours or those showing signs of fetal compromise or labour dystocia on pantograph would be taken up for caesarean delivery. Patients are monitored in labour clinically and the progress of labour is charted on a partogram. The patients’ vital parameters are monitored, and per abdomen examination is done one hourly giving special attention to fetal heart sounds and uterine activity. The maternal, labour and fetal outcomes were observed on pregnant women subjected to induction of labour, satisfying the selection criteria during the study period.
Inclusion criteria
All women with low risk singleton pregnancies- in cephalic presentation admitted at 38-39 weeks period of gestation- no medical / obstetrical complications.
Exclusion criteria
a) Scarred uterus b) Contracted/distorted pelvis c) Abnormal placenta position. d) Fetal Macrosomia, severe distress, malpresentation e) Active genital herpes, cervical carcinoma, vaginal obstruction f) Glaucoma/Asthma/history of Dinoprostone hypersensitivity g) Unexplained vaginal bleeding h) Gestational hypertension, chronic hypertension, uncontrolled diabetes, heart disease i) The primary outcome assessed was the number of successful vaginal deliveries that were accomplished in the 2 groups. j) The secondary outcomes studied were the consequences of elective induction or expectant management on the mother and her newborn.
Results
The observation was made on 134 participants, with 67 women at 38-39 weeks of gestation, electively induced group and 67 in the expectantly managed group. Table 1 depicts the sociodemographic details and baseline details of the pregnant women in the 2 groups. It is noted that the women in the 2 groups were similar with respect to age, BMI(predominantly in normal range), parity and estimated fetal weight as per admission scan. All the cases under study were booked at the hospital and were low risk.
| Electively induced group | Expectantly managed group | Comment | |
|---|---|---|---|
| AGE | Range 20-36 yrs (Median - 27.68yrs) | Range 20-36yrs (Median - 27.4 yrs) | Comparative |
| BMI | Comparative | ||
| Underweight | 5.9% | 4.47% | |
| Normal | 83.5% | 86.56% | |
| Overweight | 10.44% | 8.95% | |
| Parity | p value is 0.379 | ||
| Primi Gravida | 35.8% | 44.77% | |
| Multi Gravida | 64.17% | 55.22% | |
| Booked Case | 100% | 100% | Comparative |
| Period Of Gestation At Induction | 38wks+1Day - 39wks | Beyond 40 Wks | -NA- |
| Estimated Fetal Weight | Average-3.1kg | Average-3.2kg | Comparative |
Table 1: Sociodemographic details and baseline characters.
Table 2, describes the intrapartum characteristics of the 2 groups. The median Bishops score was 5 in both the groups. 55.52% were induced with Dinopristone gel, 13.4% with Tablet Misoprostol and 31.3% with oxytocin in the electively induced group. In the expectantly managed group 65.7% were induced with dinopristone gel, 10.4% with Tablet Misoprostol and 23.9% needed oxytocin induction. Repeat doses were needed in 71.64% of the electively induced group versus 59.7% of the expectantly managed group (p-
0.07). 41.79% of the electively induced group and 43.28% of the expectantly managed group required augmentation of labour. Meconium stained liquor was noted that 17.9% of the electively induced group against 22.3% of the expectantly managed group (p-0.381).The mean induction to delivery time had no statistical difference in the 2 groups – with 8.9 hours in the electively induced group and 9.3 hours in the expectantly managed group.
| Electively induced group | Expectantly managed group | Comment | |
|---|---|---|---|
| Modified Bishops Score | |||
| Range - | 3-6 | 4-7 | Comparable |
| Median - | 5 | 5 | |
| Dinopristone | 55.2% | 65.7% | |
| Misoprostol | 13.4% | 10.4% | |
| Oxytocin | 31.3% | 23.9% | |
| Repeat doses were needed | 71.64% | 59.7% | p-0.07 |
| Augmentation | 41.79% | 43.28% | p-0.88 |
| Meconium stained liquor | 17.9% | 22.3% | p-0.381 |
| Induction to delivery time | 8.9hrs | 9.3hrs | p-0.683 |
Table 2: Postpartum parameters.
Graph 1 depicts the labour outcomes in the 2 groups-out of 67 women in the electively induced group 48 underwent vaginal delivery while 46 women out of 67 underwent vaginal delivery in the expectantly managed group. Using Pearson’s Chi square which resulted into a value 0.143 and p value is 0.706 (greater than 0.05), it can be implied that the primary outcome- i.e. mode of Delivery is not influenced by elective induction at 38-39weeks or expectant management.
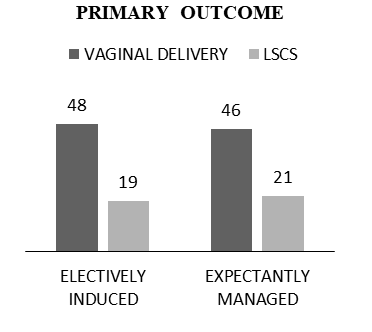
Graph 1: Primary outcome- mode of delivery.
Graph 2 compares the method of induction with the mode of delivery in the 2 groups. It depicts that since the exact significant value by Fischer’s exact test was more than
0.05 for both the groups (0.450 and 0.919), implying that the mode of delivery and method of used for induction are independent factors in both the groups.
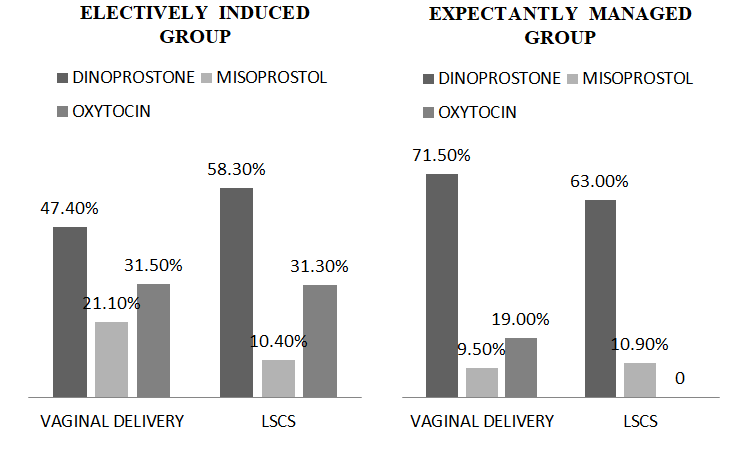
Graph 2: Mode of induction and labour outcomes.
Table 3 illustrates the post-partum parameters noted in the 2 groups. There was no significant difference in the number of women who had PPH (5.9% in both groups) or required blood transfusion (2.9% vs 1.49%). 1 patient in the electively managed group had a cervical tear that was immediately identified and repaired. No cases of uterine rupture, tachysystole, postpartum infections, admission to ICU or maternal mortality were noted.
| Electively managed group | Expectantly managed group | Comments | |
|---|---|---|---|
| Postpartum hemorrhage | 5.90% | 5.90% | - |
| Need for blood transfusion | 2.90% | 1.49% | - |
| 3rd or 4th degree Perineal laceration, cervical tears | 1.49% | 0 | - |
| Uterine rupture & tachysystole | 0 | 0 | - |
| Postpartum infections, admission to ICU, Death | 0 | 0 | - |
| Duration of hospital stay | Mean 3.07days | Mean 2.865 | p-0.488 |
| Vaginal delivery | 2.25 days | 2.41 days | |
| LSCS | 5.15 days | 3.85 days |
Table 3: Postpartum parameters.
Mean duration of hospital stay following vaginal delivery was 2.25 days vs 2.41days in the electively managed group and expectantly managed group. Following LSCS the patients stayed in hospital for over 5.15 days vs 3.85 days in the electively managed group and expectantly managed group. However there was no statistically significant difference with respect to postdelivery hospital stay (p=0.488).
Table 4 and Graph 3 compares the early neonatal outcomes. It can be noted that the 1 and 5 min APGAR scores were similar in the electively induced and expectantly managed group. 13.4% neonates in the electively induced group and 17.9% in the expectantly managed group had NICU admissions with mean duration of NICU stay of 4.2 days and 1.2days respectively. By using Fisher’s exact test between the neonates who had NICU admissions in the electively induced group delivered by LSCS or Vaginal delivery we obtained a p value of 0.001, it implies that the neonates who underwent emergency LSCS in the electively induced group- had higher chance of NICU admission compared to the normal delivery neonates, this was not the case in expectant group where the p value was 1.0.
| Electively induced group | Expectantly managed group | Comments | |
|---|---|---|---|
| Poor 1 min APGAR score | 14.90% | 29.88% | |
| Poor 5 and 10 min APGAR score | 10.44% | 17.90% | |
| NICU admission | 13.40% | 17.90% | p-0.635 |
| Duration of NICU stay | Mean 4.2 days | Mean 1.2days |
Table 4: Early Neonatal Outcomes.
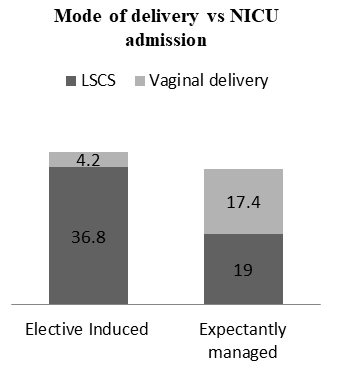
Graph 3: Mode of delivery and proportion of NICU admissions in the 2 groups.
Discussion
Induction of labour is a challenge to the obstetrician, mother, and her fetus. It is considered when vaginal delivery is felt to be the appropriate route of delivery [10]. The timing of delivery is founded by balancing maternal and perinatal risks. Delivery prior to 39 weeks 0 days of gestation was thought to have worse perinatal outcomes [11] while post term pregnancies have higher perinatal risks [12]. Between 39 weeks and 40 weeks 6 days, it was thought to better avoid elective labour induction because of a lack of evidence of perinatal benefit and concern about a higher frequency of cesarean delivery and other possible adverse maternal outcomes [13].
With some recent studies that have compared induction of labour with expectant management of the pregnancy, we have now found that elective induction of labour was associated with a lower rate of caesarean birth6-7 and lowered risk of perinatal death and morbidity3-5 in well developed countries. Guerra et al. reported an elective induction rate of 16.7% in Latin American facilities, while it approximates nearly 77.2% in Sri Lanka, followed by Thailand (44.6%), Japan (41.0%), India (32.1%) and China (20.4%) [13].
Our study depicts that of the 67 subjects in the electively induced group, 28.4% delivered by a caesarean section in comparison to 31.3% of the 67 subjects in the expectant group (p-0.143).There is no statistical difference in the mode of delivery and this is consistent with most other studies & large retrospective cohort studies like the ARRIVE trial. Secondary outcomes with respect to intrapartum characters like- mode of induction, mean induction to delivery time, requirement of additional doses, augmentation, meconium staining and postpartum complications like PPH, need for blood transfusion and duration of hospital stay post delivery were also similar in the 2 groups [14].
Neonatal outcomes measured in terms of APGAR SCORES at 1min, 5min were poorer in the expectantly managed group, yet, NICU admissions was statistically similar in the 2 groups (p-0.635). It was of interest to note that the admissions to NICU were significantly more, and for a longer duration in the electively induced women who underwent caesarean section in comparison to the women who delivered by vaginal route (p-0.001).
Conclusion
Induction of labour at 38-39 weeks in low-risk pregnancies did not seem to result in a surge of caesarean section rate or unfavourable perinatal outcomes. Our study provides information that can be incorporated into discussions between low-risk women and their obstetricians in developing countries like India to make wise decisions regarding benefits of induction of labour at term in an institutional setting.
References
-
Induction of Labour: Our Experience Surg Capt Sushil Chawla, Col Santosh Kumar Singh, Maj Monica Saraswat, Brig Sakthi Vardhan Department of Obstetrics and Gynaecology, AFMC, Pune, Maharashtra, India
-
Stock SJ, Ferguson E, Duffy A, Ford I, Chalmers J, et al. (2012) Outcomes of elective induction of labour compared with expectant management: population based study. BMJ 344: e2838.
-
Darney BG, Snowden JM, Cheng YW, Jacob L, Nicholson JM, et al. (2013) Elective induction of labour at term comparedwith expectant management: maternal and neonatal outcomes. Obstet Gynecol 122(4): 761-769.
-
Gibson KS, Waters TP, Bailit JL (2014) Maternal and neonatal outcomes in electively induced low-risk term pregnancies. Am J Obstet Gynecol 211(3): 249.e16.
-
Cheng YW, Kaimal AJ, Snowden JW, Nicholson JM, Caughey AB (2012) Induction of labour compared to expectant management in low risk women and associated perinatal outcomes. Am J Obstet Gynecol 207(6): 502.e1-8.
-
Wood S, Cooper S, Ross S (2014) Does induction of labour increase the risk of caesarean section? A systematic review and meta-analysis of trials in women with intact membranes. BJOG 121(6): 674-685.
-
Walker KF, Bugg GJ, Macpherson M, McCormick C, Grace N, et al. (2016) Randomized trial of labour induction in women 35 years of age or older. N Engl J Med 374(9): 813-822.
-
Grobman WA, Rice MM, Reddy UM, Tita ATN, Silver RM, et al. (2018) Labour induction versus expectant management in low-risk nulliparous women. N Engl J Med 379(6): 513-523.
-
WHO (2011) WHO Recommendations for Induction of Labour. Geneva, Switzerland: WHO Press.
-
Parikh LI, Reddy UM, Mannisto T, Mendola P, Sjaarda L, et al. (2014) Neonatal outcomes in early term birth. Am J Obstet Gynecol 211(3): 265.
-
American College of Obstetricians and Gynecologists (2014) Practice bulletin no. 146: management of late- term and postterm pregnancies. Obstet Gynecol 124(2 Pt 1): 390-396.
-
ACOG Committee on Practice Bulletins -Obstetrics (2009) ACOG practice bulletin no. 107: induction of labour. Obstet Gynecol 114 (2 Pt 1): 386-397.
-
Guerra GV, Cecatti JG, Souza JP, Faúndes A, Morais SS, et al. (2011) Elective induction versus spontaneous labour in Latin America. Bull World Health Organ 89: 657-665.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era