Patient Characteristics, Clinical Presentation and Maternal- Fetal Outcomes of Women with COVID-19 Admitted At a Tertiary Hospital, South-Western Uganda
Background: The coronavirus disease (COVID-19) outbreak declared a pandemic by the World Health Organization (WHO) in 2019 significantly affected pregnant women. Pregnancy causes immunological and physiological changes making a pregnant woman susceptible to a higher risk of infection with SARS-CoV-2 and death. We described the maternal socio-demographic and obstetric characteristics, clinical presentation, as well as maternal-fetal outcomes among pregnant women with COVID-19 disease at Mbarara Regional Referral Hospital. Methods: We conducted a retrospective cohort study at the COVID-19 treatment unit (CTU) of Mbarara Regional Referral Hospital (MRRH) from May 13, 2020 to July 22, 2021. We reviewed files of pregnant women with a confirmed diagnosis of COVID-19 disease by either Polymerase Chain Reaction or rapid diagnostic test (RDT). We used a chart abstraction tool in Red Cap to capture the information. We described the maternal sociodemographic and obstetric characteristics, clinical presentation, and maternal-fetal outcomes as frequencies and percentages. Results: A total of 30 participants were included in this study. The mean age was 28.6 (±5.8) years, majority were multigravida (66.7%), rural residents (53.3%), with gestational age <37 weeks (58.62%) and had severe or critical disease (43.3%) on admission. The most common symptoms at admission were cough (33%) and fever (25%). Majority of the participants had their pregnancy terminated (60.0%, 18/30). Cesarean delivery was conducted in 12/17 (70.6).13/17 (76.5%) were live births, while (4/17) 23.5% were still births and 13/17 (76.5%) had birth weight of ≥2.5 kilograms. 9/30 (30.0%) of the women died, mainly from respiratory failure (33.3%, n=3) and pulmonary embolism (33.3%, n=3). Conclusion: The maternal mortality among pregnant women admitted with COVID-19 disease was high. The main causes of death were respiratory failure and pulmonary embolism. were delivered by cesarean section with most having live births and a normal birth weight. Health systems need to strengthen measures to handle pregnant women with COVID-19 disease, ensuring well designed effective treatment protocols and intensive care facilities including the critical human resources and equipment that may be required to provide advanced care for pregnant women with COVID-19.
Introduction
The World Health Organization (WHO) declared the coronavirus disease (COVID-19) outbreak, a disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS- CoV-2), as a pandemic in March 2020 [1]. SARS‐CoV‐2 enters the body via the nasal passage and infects pulmonary cells via the SARS‐ CoV ACE2 receptor [2, 3, 4, 5]. The infection is followed by viral replication and release of the virus, causing inflammation‐mediated programmed cell death which releases damage‐associated molecular patterns, which trigger an inflammatory response that leads to excessive inflammation, damage to the integrity of the lung resulting in infection with other microbes. The inflammation caused by SARS‐CoV‐2 may also result in a “cytokine storm” that can lead to multisystem organ failure [6, 7, 8]. Pregnancy causes immunological and physiological changes making a pregnant women susceptible to viral respiratory tract infections, including COVID-19 [9, 10]. Pregnancy does not increase susceptibility to SARS- CoV-2 infection but appears to worsen the clinical course of COVID-19 compared with non-pregnant females [11]. Pregnant women may therefore face a higher risk of infection with SARS-CoV-2 and death due to their adaptation and the immunosuppressive state of pregnancy [12]. COVID-19 has affected more than 530 million people across the world, with approximately six million deaths [13]. World-wide, about 10% of Pregnant women suffer from COVID-19 [14] and 73% of these persons were asymptomatic [15].
The most frequent symptoms of pregnant women with COVID-19 are cough and fever whereas common laboratory findings include lymphocytopenia, elevated C-reactive protein [16, 17]. Studies have linked economic support, religion, marital life and education to COVID-19 infection [18, 19]. Although most (>90 percent) infected pregnant persons recover without undergoing hospitalization, rapid clinical deterioration can occur, and symptomatic pregnant patients appear to be at increased risk of severe disease and death compared with symptomatic nonpregnant females of reproductive age [20]. Risk factors and predictors for severe disease and death in pregnancy include older mean age (especially ≥35 years), obesity, preexisting medical comorbidities (particularly hypertension, diabetes and cardiovascular diseases), and being unvaccinated [21, 22]. There is paucity of information on the socio-demographic characteristics, presentation at admission and birth- outcomes of mothers with COVID-19 infection.
Given the higher risk of unfavorable maternal and perinatal outcomes among women who suffer COVID-19, it is critical to identify those who are likely to have poor birth outcomes in order to plan interventions tailored for them. Mbarara Regional Referral Hospital (MRRH) is a COVID-19 treatment centre with expertise to handle these cases. This study described the socio-demographic and obstetric characteristics, clinical presentation, as well as maternal and fetal outcomes among pregnant women with COVID-19 disease at Mbarara Regional Referral Hospital in south Western Uganda so as to help the clinical teams profile women likely to get poor outcomes and have specific interventions targeted at them.
Methods
Study setting, study design and study population
This was retrospective study that reviewed patient’s charts. It was conducted at the COVID-19 treatment unit (CTU) of Mbarara Regional Referral Hospital (MRRH) and we retrieved charts from May 13, 2020 when we admitted the first patient of COVID-19 in pregnancy to July 22, 2021. MRRH is located in south-western Uganda, Mbarara City. The hospital servesas a regional referral hospital for southwestern Uganda, including some people from neighbouring countries of Rwanda, Tanzania, and the Democratic Republic of Congo. It is also the teaching hospital for Mbarara University Science and Technology (MUST) Medical School. The hospital serves a population of about five million people. It has a total bed capacity of 350 beds, 15 of which are on the CTU. The COVID-19 unit was set up as an emergency response unit during the pandemic. The unit admitted a total of 230 patients, of which 30 were pregnant women. The unit is run by Critical Care Physicians, Emergency Physicians, General Physicians, Obstetrician/Gynecologists and Nurses/Midwives all with additional training in management of COVID-19. Our study population was pregnant women with a confirmed diagnosis of COVID-19 disease by either Polymerase Chain Reaction or rapid diagnostic test (RDT) admitted at MRRH.
Participant recruitment
Patient clinical charts of all pregnant women admitted with confirmed COVID-19 to the CTU of MRRH during the study period were retrieved. All the 30 participants were included in the study.
Data collection and study variables
Data collection was carried out by a trained research assistant using a pretested chart abstraction tool. Data was abstracted from the patient charts into an abstraction tool in RedCap—a secure online software hosted at the Department of Obstetrics and Gynecology of MRRH.
The variables collected included
Socio-demographic characteristics (age, marital status, residence, occupation); Clinical presentation characteristics (severity of COVID-19 disease, respiratory rate, oxygen saturation, pulse rate, blood pressure); obstetric characteristics (parity, gestational age, antenatal care attendance, fetal heart rate, obstetric complications, mode of delivery and indications for delivery); and Maternal-fetal outcomes (status of the mother at time of disposition (alive or dead) and the status of the baby at birth (whether live or still birth).
Data management and analysis
Data were entered into Redcap and exported to STATA version 15 (StataCorp, College Station, Texas, USA) for analysis. We described the maternal socio-demographic characteristics, clinical presentation, and maternal-fetal outcomes as frequencies and percentages.
Results
Socio-demographic and obstetric characteristics of pregnant women with confirmed SARS-CoV-2 infection
The mean age of the participants was 28.6 (±5.8). Majority of the participants were aged 20-35 years (80.0%), were multigravida (66.7%), rural residents (53.3%), unemployed (60.0%) and were married (73.3%). Also, the majority of the participants presented with symptoms were with gestational age <37 weeks (58.6%), had attended less than four antenatal care visits and had severe or critical disease on admission (43.3%). Ninety percent (90%) of the diagnosis was by rapid diagnostic tests (Table 1).
| Variable | Frequency N (%) |
|---|---|
| Mean age (±SD) | 28.6 (±5.8) |
| Age (years) | |
| <20 | 2 (6.7) |
| 20-34 | 24 (80.0) |
| ≥35 | 4 (13.3) |
| Parity | |
| Prime gravida (1) | 10 (33.3) |
| Multi gravida (>1) | 20 (66.7) |
| Residence | |
| Urban | 14 (46.7) |
| Rural | 16 (53.3) |
| Marital status | |
| Married | 22 (73.3) |
| Unmarried | 8 (26.7) |
| Employment status | |
| Employed | 12 (40.0) |
| Unemployed | 18 (60.0) |
| Disease severity at admission | |
| Mild disease | 11 (36.7) |
| Moderate disease | 6 (20.0) |
| Severe disease | 9 (30.0) |
| Critical disease | 4 (13.3) |
| Antenatal care visits | |
| <4 | 19 (63.3) |
| ≥4 | 11 (36.7) |
| Gestation age at symptom onset | |
| <37 | 17 (58.6) |
| ≥37 | 12 (41.4) |
Table 1: Socio-demographic and obstetric characteristics of participants
Clinical presentation of pregnant women admitted with COVID-19 at MRRH CTU
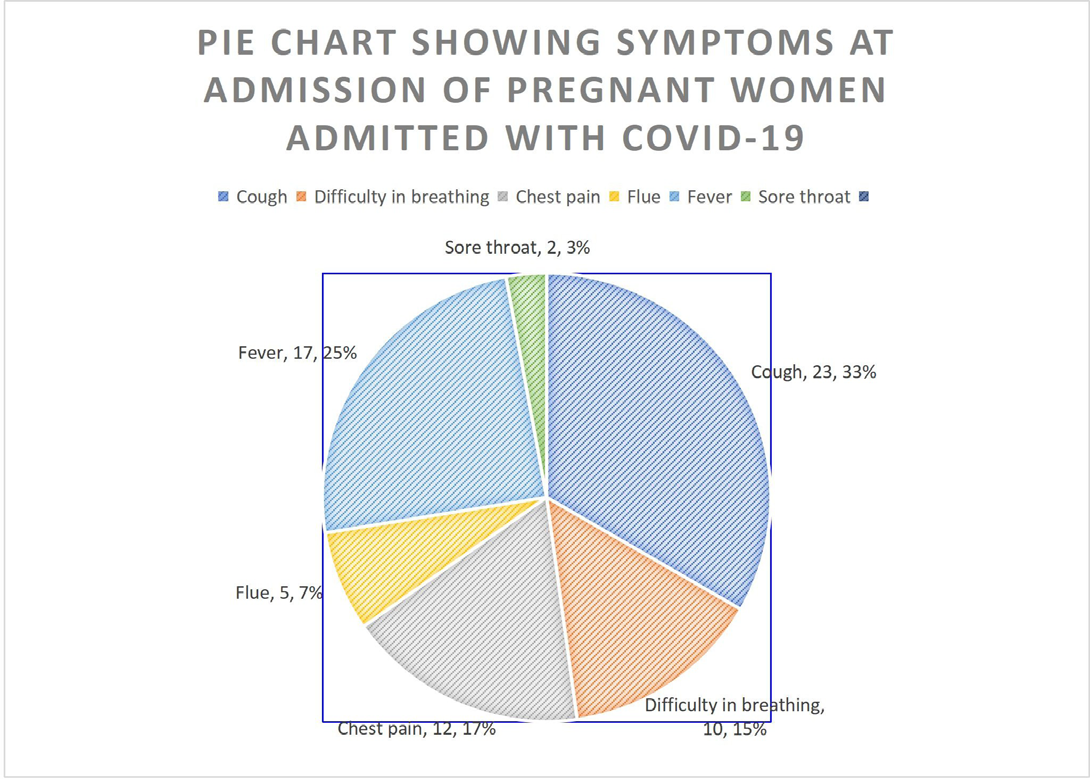
The most common symptoms at admission were cough (33%) and fever (25%) (Figure1). Most of the participants had more than one symptom.
Admission clinical measurements
The median duration of symptoms was 3 days (interquartile range: 2-7 days). The mean duration of symptoms was 3.9 (±2.6). The mean oxygen saturation was 90.0% (hypoxia), with a mean respiratory rate of 28 cycles/ minute (tachypnea) and mean respiratory rate of 111.8 bpm 9 (tachycardia) (Table 2).
| Admission vital signs | Mean (±SD) |
|---|---|
| Systolic blood pressure (mmHg) | 123.3 (±26.1) |
| Diastolic blood pressure (mmHg) | 77.8 (±14.2) |
| Oxygen saturation (%) | 90.9 (±7.6) |
| Temperature | 35.4 (±3.0) |
| Respiratory rate | 28.5 (±8.0) |
| Pulse rate (bpm) | 111.8 (±17.3) |
| Duration of symptoms | 3.9 (±2.6) |
Table 2: Admission clinical measurements
Clinical Care, Delivery, Maternal and Neonatal Outcomes of Pregnant Women Admitted with Confirmed COVID-19 Infection
Majority of the participants had their pregnancy terminated (60.0%: 18/30); of these, 94.4% (17/18) were delivered and one had a spontaneous abortion. Among those who were delivered, 70.6% (12/17) were delivered by cesarean section. Fifty nine percent (58.8%, 10/17) had a cesarean section before onset of labour for indication of severe covid 19 and two or more previous caesarean section scars, while an additional two caesarean sections were due to fetal distress following labour induction. Seventy six percent (76.5%, 13/17) of the delivered babies were live births, while 23.5% (4/17) were still births. 38.5% (5/13) were admitted to neonatal intensive care unit. Seventy six percent (76.5%, n=13) of the babies delivered had birth weight of 2.5 kgs and above. Thirty percent (30.0%, 9/30) of the participants died, and the most common causes of death were pulmonary embolism (33.3%, n=3), pulmonary oedema (22.2%, n=2) and respiratory failure (33.3%, n=3) (Table 3).
| Pregnancy outcomes | No (%) of women (N=30) |
|---|---|
| Pregnancy terminated | |
| Yes | 18 (60.0) |
| No | 12 (40.0) |
| Mode of termination | |
| Delivered | 17 (94.4) |
| Spontaneous abortion | 1 (5.6) |
| Delivery Outcome | |
| Macerated stillbirth | |
| 1 (5.9) | |
| Fresh still birth | 3 (17.7) |
| Live birth | 13 (76.5) |
| Birth weight (kilograms) | |
| <2.5 | 4 (23.5) |
| ≥ 2.5 | 13 (76.5) |
| Neonatal outcome after delivery (n=13) | |
| Discharged healthy | 8 (61.5) |
| NICU admission | 5 (38.5) |
| Died* | 2 (40.0) |
| Discharged home alive and healthy | 3 (60.0) |
| Onset of labour | |
| Spontaneous | 4 (23.5) |
| Induced | 3 (17.7) |
| Cesarean section before labour | 10 (58.8) |
| Mode of delivery | |
| Vaginal delivery | 5 (29.4) |
| Cesarean section | 12 (70.6) |
| Indications for Caesarean section (n=12) | |
| ≥ 2 prior caesarean sections | 4 (33.3) |
| Fetal distress | 2 (16.7) |
| Severe Covid 19 disease | 6 (50.0) |
| Maternal outcome | |
| Maternal death | 9 (30.0) |
| Live mother | 21 (70.0) |
| Causes of death | |
| Respiratory failure | 3 (33.3) |
| Pulmonary embolism | 3 (33.3) |
| Pulmonary oedema | 2 (22.2) |
| Indirect maternal death | 1 (11.1) |
Table 3: ** Clinical care, delivery, maternal and neonatal outcomes of pregnant women admitted with confirmed COVID-19
Infection NICU; Neonatal Intensive Care Unit; *prematurity related deaths Table 3: Clinical care, delivery, maternal and neonatal outcomes of pregnant women admitted with confirmed COVID-19
Discussion
Our study was a retrospective clinical chart review of all 30 pregnant women admitted with confirmed COVID-19 to the CTU of MRRH from May 13, 2020 to July 22, 2021. We documented the socio-demographic characteristics, clinical presentations, and maternal and delivery outcomes. The most common symptoms were cough and fever. This finding is consistent with study findings from a systematic review of 66 studies [23], and an analysis of case series across the globe including studies from USA, Spain, China, Italy and Turkey [24]. Majority (43.3%) of the pregnant women presented with either severe or critical disease. SARS‐CoV‐2 infects pulmonary cells via the SARS‐CoV ACE2 receptor causing viral replication and release of the virus, causing an inflammatory response that leads to excessive inflammation [6]. Theinflammation may also result in a “cytokine storm” that can lead to critical disease [6, 7, 8]. Cesarean delivery was performed in majority (70.59%, 12/17) of the participants. Fifty nine percent (58.82%, 10/17) had a cesarean section before onset of labour. The cesarean section was mode of delivery in 59% of the patients, major indication being COVID-19 related complication. This is consistent with results from a systematic review of articles published between December 2019 and April 2020 where 68.9% of women were delivered via cesarean section, due to COVID-19 status [25]. This is also consistent with results from a systematic review of 108 pregnancies on maternal and perinatal outcomes with COVID-19 where 92% of all pregnancies were by cesarean section [26]. However, in this particular analysis, the major indication was fetal distress as opposed to COVID-19 in our study. Even though COVID-19 is not an indication of cesarean section, many clinicians faced a dilemma of monitoring women during labour especially in resource constrained setting, where the protective wear were not adequate and the clinical staff taking care of these mothers were very few. Cesarean section seemed a quicker way of delivery than the process of obstetric labour monitoring. The fear that COVID-19 could also have compromised the woman’s breathing and therefore creating hypoxic environment for the baby could as well have influenced the decision of doing a cesarean section for majority of the cases. The high number of cesarean deliveries is a worrying observation since most of these women come with short birth intervals in their subsequent pregnancies as earlier documented in a study done in western Uganda [27]. In this study, 23.5% of the babies born were still births and 38.5% of the live babies needed NICU support. Different result from the study on 201 women who had COVID-19 , 2/185 were still births [28]. This is lower than what was reported in a systematic review on maternal and neonatal outcomes associated with COVID-19. infection where 76.9% (11/13) of neonates required NICU admission and 42.8% (40/50) [29]. Among 1,249,634 delivery hospitalizations during March 2020–September
2021, U.S. women with COVID-19 were at increased risk for stillbirth compared with women without COVID-19 (adjusted relative risk [aRR] = 1.90; 95% CI = 1.69–2.15) [30]. The hypoxic environment as a result of respiratory compromised in severe and critical covid disease affects the utero-placental flow of oxygen and can cause a still birth. Also, the high numbers of NICU admission could be because some babies were born with birth asphyxia as well as still births and therefore needed NICU support.
In this study, 30% of the pregnant women with COVID-19 died. The main causes of death included respiratory failure, pulmonary embolism and oedema. The mortality findings are high than what was reported in Maharashtra India where the mortality rate was 0.8% [31] as well as results from a metanalysis where the mortality rate was 1.3% [32]. This mortality rate is much higher than what has been reported world-wide. Pregnant women who contracted COVID-19 during pregnancy are 20 times more likely to die than those who did not contract the virus [33]. Physiological and mechanical changes in pregnancy increase susceptibility to infections, particularly when the cardiorespiratory system is affected, and encourage rapid progression to respiratory failure. Changes in the immune system in pregnancy with a bias toward T-helper 2 (Th2) system dominance, which protects the fetus, leaves the mother vulnerable to viral infection and hypoxic compromise. However, lack of clinical management protocols, expertise as well as equipment to support cases of severe disease and critical disease could have resulted into the high numbers of maternal deaths from COVID-19 [34].
Our study is not without limitations. First, we did a retrospective review of patient files for the information. Some charts had missing information. Second, postmortem studies were not done to confirm the cause of death and we solely relied on the cause of death as documented by the clinical team. The strength of our study lies in it being one of the initial studies to document the maternal and fetal outcomes among woman who had covid 19 disease in a resource limited setting, as most earlier studies were done mainly in the developed countries.
Conclusion
This study found that the maternal mortality among women admitted with Covid 19 disease was high. One in every three pregnant women admitted with Covid 19 died mainly from respiratory failure and pulmonary embolism. The most common symptoms at admission were fever and cough. Four in ten women admitted had severe and critical disease. Most women delivered by cesarean section, with majority having live births and a normal birth weight. Health systems need to strengthen measures to handle pregnant women like havingin tensivists and designing effective treatment protocols that include intubation in order to handle the severe and critical cases of Covid 19 in pregnancy.
Declaration
Ethics approval and consent to participate
This study was approved by the Mbarara University of Science and Technology Research Ethics Committee (09/05-17), and Uganda National council of Science and Technology (HS967ES.). We respected the guidelines of Helsinki and CIOMS-2002 (Council for International Organizations of Medical Sciences) regarding research with humans, avoiding any type of physical or moral harm. Since this was a retrospective review of records at a time when the participants could not be accessed, the study was granted an exemption from requiring informed consent by the Mbarara University of Science and Techology Research Ethics Committee (09/05-17). Confidentiality of the study participants was ensured by using unique identifiers and the charts were kept in a lockable cupboard which was accessible by only the study team.
Contribution to the field statement
The World Health Organization (WHO) declared the coronavirus disease (COVID-19) outbreak, a disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS- CoV-2), as a pandemic in March 2020. Pregnancy causes immunological and physiological changes making a pregnant women susceptible to viral respiratory tract infections, including COVID-19. Pregnancy does not increase susceptibility to SARS-CoV-2 infection but appears to worsen the clinical course of COVID-19 compared with non-pregnant females. Pregnant women may therefore face a higher risk of infection with SARS-CoV-2 and death due to their adaptation and the immunosuppressive state of pregnancy. Given the higher risk of unfavorable maternal and perinatal outcomes among women who suffer COVID-19, it is critical to identify those who are likely to have poor birth outcomes in order to plan interventions tailored for them. This study was able to described the socio-demographic and obstetric characteristics, clinical presentation, as well as maternal and fetal outcomes among pregnant women with COVID-19 disease at resource limited hospital in southwestern Uganda so as to help the clinical teams profile women likely to get poor outcomes and have specific interventions targeted at them.
References
-
Announces COVID W (2020) outbreak a pandemic.
-
Chia PY, Coleman KK, Tan YK, Ong SWX, Gum M, et al. (2020) Detection of air and surface contamination by SARS-CoV-2 in hospital rooms of infected patients. Nature communications 11(1): 2800.
-
Santarpia JL, Rivera DN, Herrera V, Morwitzer MJ, Creager H, et al. (2020) Transmission potential of SARS-CoV-2 in viral shedding observed at the University of Nebraska Medical Center. MedRxiv.
-
Santarpia JL, Rivera DN, Herrera VL, Morwitzer MJ, Creager HM, et al. (2020) Aerosol and surface contamination of SARS-CoV-2 observed in quarantine and isolation care. Scientific reports 10(1): 12732.
-
Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, et al. (2020) SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 181(2): 271-280.e8.
-
Bergsbaken T, Fink SL, Cookson BT (2009) Pyroptosis: host cell death and inflammation. Nature Reviews Microbiology 7(2): 99-109.
-
Tay MZ, Poh CM, Rénia L, MacAry PA, Ng LFP (2020) The trinity of COVID-19: immunity, inflammation and intervention. Nature Reviews Immunology 20(6): 363- 374.
-
Nile SH, Nile A, Qiu J, Li L, Jia X, et al. (2020) COVID-19: Pathogenesis, cytokine storm and therapeutic potential of interferons. Cytokine & growth factor reviews 53: 66- 70.
-
Zheng J (2012) Recent advances in research on the human placenta.
-
Silasi M, Cardenas I, Kwon JY, Racicot K, Aldo P, et al. (2015) Viral infections during pregnancy. American journal of reproductive immunology 73(3): 199-213.
-
Zambrano LD, Ellington S, Strid P, Galang RR, Oduyebo T, et al. (2020) Update: characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status—United States, January 22–October 3, 2020. Morbidity and Mortality Weekly Report 69(44):1641-1647.
-
Mor G, Cardenas I, Abrahams V, Guller S (2011) Inflammation and pregnancy: the role of the immune system at the implantation site. Annals of the new York Academy of Sciences 1221(1): 80-87.
-
Healey CG, Simmons SJ, Manivannan C, Ro Y (2022) Visual Analytics for the CoronavirusCOVID-19 Pandemic. Big Data 10(2): 95-114.
-
Dixit A, Zhou D, Sheikh J, Lawson H, Kew T, Ansari K, et al. (2021) Prevalence and risk-factors of COVID-19 in pregnancy: Living systematic review and metaanalysis. BJOG: An International Journal of Obstetrics and Gynaecology 128(SUPPL 2): 196-197.
-
Allotey J, Stallings E, Bonet M, Yap M, Chatterjee S, et al. (2020) Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. Bmj 370.
-
Juan J, Gil MM, Rong Z, Zhang Y, Yang H, et al. (2020) Effect of coronavirus disease 2019 (COVID‐19) on maternal, perinatal and neonatal outcome: systematic review. Ultrasound in Obstetrics & Gynecology 56(1): 15-27.
-
Boushra MN, Koyfman A, Long B (2021) COVID-19 in pregnancy and the puerperium: A review for emergency physicians. The American journal of emergency medicine 40: 193-198.
-
Malagón Díaz ZS. (2015) Factores asociados a la asistencia al control prenatal en gestantes del municipio de Yopal Casanare, Colombia–2011: Universidad del Rosario.
-
Effati-Daryani F, Zarei S, Mohammadi A, Hemmati E, Yngyknd SG, et al. (2020) Depression, stress, anxiety and their predictors in Iranian pregnant women during the outbreak of COVID-19. BMC psychology 8(1): 99.
-
Pineles BL, Goodman KE, Pineles L, O’Hara LM, Nadimpalli G, et al. (2021) In-Hospital Mortality in a Cohort of Hospitalized Pregnant and Nonpregnant Patients With COVID-19. Annals of Internal Medicine 174(8): 1186-1188.
-
Galang RR, Newton SM, Woodworth KR, Griffin I, Oduyebo T, et al. (2021) Risk factors for illness severity among pregnant women with confirmed severe acute respiratory syndrome coronavirus 2 infection— surveillance for emerging threats to mothers and babies network, 22 state, local, and territorial health departments, 29 March 2020–5 March 2021 73(Suppl 1): S17-S23.
-
Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez- Ocampo E, Villamizar-Peña R, Holguin-Rivera Y, et al. (2020) Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel medicine and infectious disease 34: 101623.
-
Ciapponi A, Bardach A, Comandé D, Berrueta M, Argento FJ, et al. (2021) COVID-19 and pregnancy: An umbrella review of clinical presentation, vertical transmission, and maternal and perinatal outcomes. PloS one 16(6): e0253974.
-
Han Y, Ma H, Suo M, Han F, Wang F, et al. (2020) Clinical manifestation, outcomes in pregnant women with COVID-19 and the possibility of vertical transmission: a systematic review of the current data. Journal of perinatal medicine 48(9): 912-924.
-
Debrabandere ML, Farabaugh DC, Giordano C (2021) A review on mode of delivery during COVID-19 between December 2019 and April 2020. American journal of perinatology 38(4): 332-341.
-
Zaigham M, Andersson O (2020) Maternal and perinatal outcomes with COVID‐19: a systematic review of 108 pregnancies. Acta obstetricia et gynecologica Scandinavica 99(7): 823-829.
-
Byamukama O, Migisha R, Kalyebara PK, Tibaijuka L, Lugobe HM, et al. (2022) Short interbirth interval and associated factors among women with antecedent cesarean deliveries at a tertiary hospital, Southwestern Uganda. BMC Pregnancy and Childbirth 22(1): 1-8.
-
Yoon S, Kang J, Ahn J (2020) Clinical outcomes of 201 neonates born to mothers with COVID-19: a systematic review. Eur Rev Med Pharmacol Sci 24(14): 7804-7815.
-
Smith V, Seo D, Warty R, Payne O, Salih M, et al. (2020) Maternal and neonatal outcomes associated with COVID-19 infection: A systematic review. Plos one. 15(6): e0234187.
-
DeSisto CL, Wallace B, Simeone RM, Polen K, Ko JY, et al. (2021) Risk for stillbirth among women with and without COVID-19 at delivery hospitalization— United States, March 2020–September 2021. Morbidity and Mortality Weekly Report 70(47): 1640-1645.
-
Gajbhiye RK, Mahajan NN, Waghmare RB, Zala S, Chaaithanya IK, et al. (2021) Clinical characteristics, outcomes, & mortality in pregnant women with COVID-19 in Maharashtra, India: Results from PregCovid registry. The Indian Journal of Medical Research 153(5- 6): 629-636.
-
Karimi L, Makvandi S, Vahedian-Azimi A, Sathyapalan T, Sahebkar A (2021) Effect of COVID-19 on mortality of pregnant and postpartum women: a systematic review and meta-analysis. Journal of pregnancy 8870129.
-
EJ CM, Rodríguez A (2021) El diagnóstico de COVID-19 durante el embarazo se asocia a una mayor morbilidad neonatal y morbimortalidad materna.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era