Mammary Myofibroblastoma: Report of an Uncommon Case
Mammary myofibroblastoma is an uncommon benign mesenchymatous tumor, representing less than 1% of mammary tumors. First individualized in 1987, it’s a benign tumor of unknown etiology, occurring in equal incidence in post-menopausal women and men. It has with a very large morphological spectrum but its management is surgical and the diagnosis is histological and immune histochemical. We hereby report a case of a myofibroblastoma in a 28-year-old woman that was successfully managed surgically. The particularity of our case is the very young age of our patient, since the cases described in the literature are tumors in post-menopausal women. This case raises the issue of pathology’s polymorphism.
Introduction
Mammary myofibroblastoma is an uncommon benign solid mesenchymal tumor which differential diagnosis with other solid mesenchymal tumors can be challenging and only histological [1]. It is mainly localized in the breast but extra mammary localizations were described in the literature. Its incidence is equal in post-menopausal women and men. Although this tumor is histologically confused with other spindle cell tumors, immunohistochemistry adjusts the diagnosis, hence the large clinic radio histological spectrum. Its management is essentially surgical excision [1].
We hereby report an uncommon case of mammary myofibroblastoma in a 28-year-old patient aged that presented with painless nodule of the right breast with one-year progressive evolution. Core biopsy was in favor of a mesenchymal tumor and the patient benefited from a surgical resection. Further anatomopathological and immune histochemical examination made the diagnosis of a mammary myofibroblastoma. The patient benefited from a 5-years follow-up that showed no recurrence.
We here by present the case of a 28-year-old woman, without any particular pathological history, nor history of neoplasia in the family, who presented in our structure with fortuitous discovery of right breast’s mass with one year progressive increase in size without any associated sign. Clinical examination revealed a patient with overall condition preserved and a BMI of 29.3. Breast examination found asymmetrical breasts, right breast’s voussure in the upper outer quadrant without any skin abnormalities nor nipple areola plate’s abnormalities. (Figure 1) Right breast’s palpation showed firm, mobile and painless nodule at the upper outer quadrant, with a regular contour measuring 7x5 cm. Left breast was without any abnormalities. Both ganlionic areas were free. Rest of the examination was unremarkable.

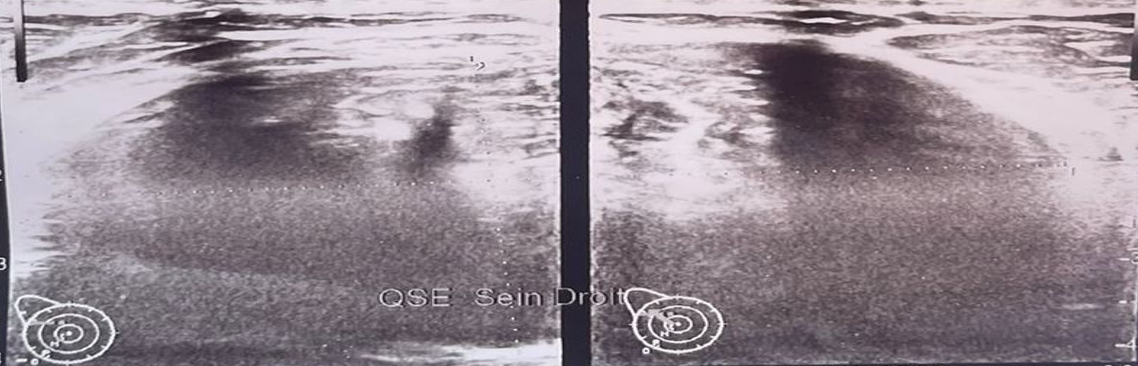
Mammary ultrasound showed mammary gland with tigerish appearance with the presence of two well-defined oval formations which long axis was parallel to the skin and echostructure was hypoechogenic and heterogeneous. Their localization was for the first one in the right upper outer quadrant measuring 69x40 mm and for the second one in the lower outer quadrant of 9x4 mm. Lymph nodes were free of any adenopathy. These nodules were classified ACR BI-RADS 3 (Figures 2 & 3). Core biopsy of the bigger breast nodule objectified tumor proliferation of fascicular architecture made up of spindle-shaped cells with oval nuclei of little atypical shape, expressing a low mitotic activity, with absence of ductal structures within the proliferation, without necrosis and nor sign of malignancy (Figure 4). Given nonspecific tumor characteristics and its size, surgery excision was decided.

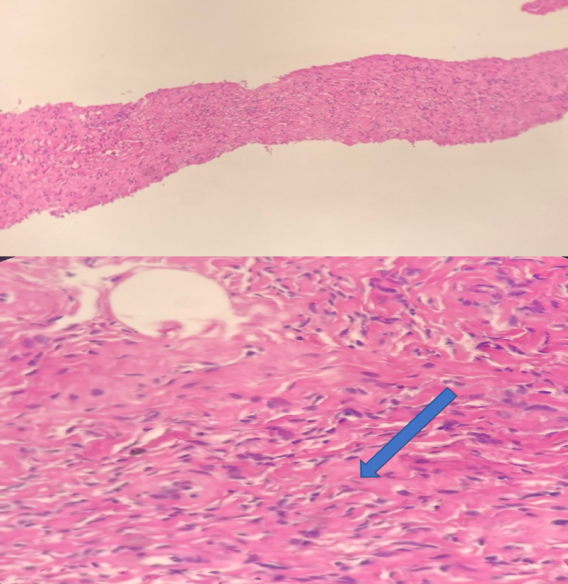
The patient benefited from large tumorectomy under general anesthesia. Pathological examination of the operative piece showed proliferation enveloping residual mammary ducts, with monomorphic spindle-shaped cells arranged in short and intersecting bundles, with elongated and regular nuclei free of cytonuclear atypia and mitosis. The stroma was found fibrous and rich in collagen fibers and capillaries. Resection margins were free. Immunohistochemistry showed large expression of CD34, without expression of AML, Desmin, CD31, Beta-catenin, S-100 Protein, PR nor ER. These histological and immunohistochemistry findings were in favour of mammary myofibroblastoma. The patient benefited from a 5-years follow-up that showed no recurrence.
Discussion
MFB is an uncommon mesenchymal benign tumor that differentiates from breast tissue’s stromal structures [1]. Exceptional extra-mammary sites have also been described, with predominance for the inguinal region [1]. Wargotz et al. [2] first described myofibroblastoma as a complex entity. The authors documented 16 individual cases, 11 of which were men, underlining the male predominance of this tumor [2]. Subsequently, multiple cases of MFB have been cited in women over the past decades. This increased incidence was attributed to the rise in mammography screening [3]. Nevertheless, less than a hundred cases have been reported in the literature, and even less in the younger female population, hence the difficulty of considering this diagnosis in a young woman. MFB occurs most frequently in patients aged between 40 and 87 [3]. This adds to the particularity of our young patient.
Literature didn’t find any relationship between MFB and the patient’s race, medical conditions, drug use nor other effects of growth promoters [1, 2, 3]. However, recent studies showed an association between MFB and renal or prostatic neoplasia [4, 5]. MFB have also been reported after excision of breast cancer at the level of surgical scar tissue or after chest trauma [6]. In the literature, three etiopathologic theories have been described to explain the pathophysiology of this uncommon tumor [6]. Firstly, steroidal sex hormones contribution was suggested such as estrogen, progesterone and androgen, which receptors were present in several cases. This first theory explained also the gynecomastia often associated in male patients [6]. Secondly, disruption of cytokine secretion and inflammation after trauma could lead to development of tumor growth factors such as TGFβ [6]. Finally, fibrosis in the surgery site was also described [4]. All these theories weren’t compatible with our case.
Clinically, mammary myofibroblastoma may be asymptomatic and diagnosed during women’s mammographic screening or symptomatic in the context of men’s gynecomastia [6]. Typically, this tumor presents as an unilateral, painless, mobile breast mass [6]. The nodule tends to grow slowly over a period of months to years [3, 7]. In terms of size, lesions generally measure between 1 and 4 cm but much larger nodules measuring up to 16 cm were described [8, 9]. MFB’s radiological findings generally shows nonspecific image without malignancy sign [7, 9, 10]. Breast ultrasound often finds a well-circumscribed heterogeneous and hypoechogenic image, mostly classified as benign [10]. In our case, the lesion was in line with the literature, classified as ACR BI-RADS 3. Given her young age and the benign nature of the ultrasound results, mammography was not requested for our patient. Doppler ultrasound, CT scan and MRI are not commonly used.
In the light of this pathology’s polymorphous spectrum, several differential diagnostics can be considered, including benign tumors such as fibro adenomas, lymphangiomas, angiolipomas, hematomas and abscesses and malignant tumors like phyllodes, carcinomas and sarcomas [5]. Thus histological diagnosis, specifically by core biopsy, is mandatory but rarely conclusive [3, 11]. MFB’s histological analysis shows short fascicles of spindle cells separated by thick bands of collagen [2]. MFB has usually well-defined boundaries with pseudocapsule surrounding compressed breast tissue with low mitotic index atypia and without atypia [2]. Immunohistochemistry founds high expression of CD 34, vimentin and actin [2]. CD34 is considered as a good marker for this pathology [10]. Surgical excision is the MFB’s gold standard management in addition to providing diagnostic confirmation [10, 11]. Malignant transformation of myofibroblastoma or recurrence has never been reported in the literature. The patient benefited from a 5-years follow- up that showed no recurrence. MFB’s prognosis is excellent [5].
Conclusion
Mammary myofibroblastoma is an uncommon benign solid tumor representing less than 1% of all breast tumors. Since the widespread introduction of mass screening for breast cancer, MFB’s incidence has increased in menopausal women. Nevertheless, it remains very uncommon in young women like our patient. Practitioners should consider this uncommon benign entity and choose surgical excision in the event of an inconclusive biopsy. Furthermore, they have to reassure patients of the excellent prognosis after diagnosis’ confirmation given by the histological analysis of the surgical specimen. This work has been reported in line with the SCARE 2020 criteria [12].
Author contribution
Khaoula Lakhdar: study concept and design, data collection, data analysis and interpretation, writing the paper. Najia Zeraidi: study design, data collection, data interpretation, writing the paper. Oumaima Sardhaoui: study concept and design, data collection, data analysis and interpretation, writing the paper. Soukaina Mouiman: study concept and design, data collection, data analysis and interpretation, writing the paper. Aziz Slaoui study concept and design, data collection, data analysis and interpretation, writing the paper. Aziz Baydada: study concept, data collection, data analysis, writing the paper.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
- Availability of data and materials
- Supporting material is available if further analysis is needed.
- Declaration of competing interest
- The authors declare that they have no competing interests.
References
-
Toker C, Tang CK, Whitely JF, Berkheiser SW, Rachman R (1981) Benign spindle cell breast tumor. Cancer 48: 1615-1622.
-
Wargotz ES, Weiss SW, Norris HJ (1987) Myofibroblastoma of the breast. Sixteen cases of a distinctive benign mesenchymal tumor. The American Journal of Surgical Pathology 11(7): 493-502.
-
Metry M, Shaaban M, Youssef M, Carr M (2016) Myofibroblastoma of the breast: literature review and case report. Case Reports in oncological Medicine 1714382.
-
Comer JD, Cui X, Eisen CS, Abbey G, Arleo EK (2017) Myofibroblastoma of the male breast: A rare entity with radiologic-pathologic correlation. Clinical imaging 42: 109-112.
-
Sanmugasiva VV, Hamid MTR, Fadzli F, Kaur S, Abd Rahman N, et al. (2018) Myofibroblastoma of the breast. The Malaysian Journal of Pathology 40: 349-353.
-
Taliaferro AS, Fein-Zachary V, Venkataraman S, Mehta TS, Patel A, et al. (2017) Imaging features of spindle cell breast lesions. AJR Am J Roentgenol 209(2): 454-464.
-
Omar LA, Rojanapremsuk T, Saluja K, Merchant KA, Sharma PB (2006) Radiologic and histologic presentation of male mammary myofibroblastoma. Baylor University Medical Center 29(3): 321-322.
-
Magro G, Bisceglia M, Michal M, Eusebi V (2002) Spindle cell lipoma-like tumor, solitary fibrous tumor and myofibroblastoma of the breast: a clinico-pathological analysis of 13 cases in favor of a unifying histogenetic concept. Virchows Arch 440(3): 249-260.
-
Wickre M, Valencia E, Solanki M, Glazebrook K (2021) Mammary and extramammary myofibroblastoma: Multimodality imaging features with clinicopathologic correlation, management and outcomes in a series of 23 patients. The British Journal of Radiology 94 (1120): 20201019.
-
Yoo EY, Shin JH, Ko EY, Han BK, Oh YL (2010) Myofibroblastoma of the female breast: Mammographic, sonographic, and magnetic resonance imaging findings. Journal of Ultrasound in Medicine 29(12): 1833-1836.
-
Landeyro J, Díaz ML, Raventós A, Vadillo J, Martínez MS (2012) Cytological diagnostic clues in fine needle aspiration of breast myofibroblastoma: a case report. Diagnostic Cytopathology 40(12): 1107-1111.
-
Agha RA, Franchi T, Sohrabi C, Mathew G, Kerwan A, et al. (2020) The SCARE 2020 guideline: updating consensus Surgical Case Report (SCARE) guidelines. Int J Surg 84: 226-230.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era