Male Partner Involvement in Pregnancy-Related Care in Pakistan: A Cross-Sectional Study
Background: Maternal mortality remains a significant public health concern in developing countries, including Pakistan, with a substantial portion attributed to pregnancy-related causes. The pivotal role played by male partners in providing support and addressing pregnancy-related complications faced by women cannot be overstated. Objective: This study aimed to assess the level of male partner involvement in pregnancy-related care. Methodology: A cross-sectional study was conducted in Peshawar district, involving 271 mothers selected from Hayatabad Medical Complex. Ethical approval was obtained from the institute, and consent was secured from all participants. Data collection was carried out using a validated questionnaire. Results: The majority of participants (59.4%) fell within the 30 to 40 age group. Among them, 82.7% identified as housewives, and 61.3% had no formal education. Encouragingly, 74% of respondents reported a high level of male partner involvement in pregnancy-related care, while 26% indicated limited involvement. Conclusion: This study underscores the positive trend of male partners actively participating in the care of expectant mothers. However, it also highlights the ongoing need for targeted counseling and education programs to further enhance their engagement in pregnancy-related care.
Introduction
The majority of maternal deaths (99%) are the responsibility of developing countries, with sub-Saharan Africa accounting for more than half of these occurrences. In 2015, around 58,000 maternal fatalities (19%) and 45,000 maternal deaths (15%) occurred in Nigeria, Pakistan and India, respectively. This accounted for more than one third of all maternal deaths that occurred in the world [1, 2, 3] Similar to other developing and developed countries, maternal mortality rate in Pakistan is also very high. The maternal mortality ratio of Pakistan is 186 per 100,000 live births [4]. Although the health of mothers is dependent on a wide range of circumstances, such as their socioeconomic standing and their surrounding environment, one significant component that has been overlooked throughout the years is the role that males play in the process [5]. Both the International Conference on Population and Development (ICPD), which took place in Cairo, Egypt in 2014, and the Fourth World Conference on Women, which took place in Beijing, China
in 2015, acknowledged the significance of the role that men play in ensuring the sexual and reproductive health of themselves and their partners. The International Center for Population Dynamics (ICPD) encouraged extra efforts to be made to highlight men’s shared responsibilities and to promote their active participation in maternal care [6]. In spite of this, pregnancy and childbirth continue to be seen as something that only women should be concerned with in the majority of African countries [7]. In most cases, men do not accompany their partners to antenatal or postnatal care or to services related to family planning. Additionally, men are not expected to be there during the labour or delivery of their children [8].
Men may not participate in prenatal, postnatal, newborn, or post-abortion care because they do not receive any information from health providers that is beneficial to them regarding the health of the mother and the baby, or about their roles in it. This may be the reason why men do not participate in prenatal, postnatal, newborn, or post- abortion care [9]. The idea that men should be involved in the maternal care of their pregnant partners has gained momentum and has become important because of the realization that men’s behavior can significantly affect the health outcomes for women and babies. The belief that men should be involved in maternal care of their pregnant partners has gained momentum and has become important because of this realization [10]. There have been a number of studies that have highlighted the role that men can play in improving the health of their pregnant wives [11]. It was claimed that 86 percent of prenatal patients at the University College Hospital in Ibadan preferred having their husbands there during the labour process with them. According to the findings of yet another study that was carried out in Kenya by the United Nations Population Fund (UNFPA), husbands have a significant impact on their wives’ decisions about the utilization of reproductive health services such as family planning [12]. These highlight the reality that men have an important role to play in protecting the health of women during pregnancy, childbirth, and beyond, despite the fact that there is a tendency to ignore the relevance of this fact [13].
Involvement of men in care connected to pregnancy is beneficial for gender equality, among other reasons (PRC). In the majority of households, the males hold the financial authority and serve as the primary decision-makers in all matters, including the management of pregnancies [14]. In nations like Pakistan, where patriarchal family structures are typical, this experience is comparable. They might use this chance to ensure that their expectant wives seek maternity care or make plans for skilled delivery care. Women’s limited access to health services has a number of root causes, one of which is gender inequality. Men can assist their spouses in overcoming gender-based obstacles to care-seeking and effective home care techniques. Men’s actions have an impact on both men and women’s reproductive health as well as the wellbeing of their offspring [15, 16]. However, because they are not involved in reproductive, maternity, and child health services and education, males frequently lack the knowledge necessary to make educated decisions [17]. Men must comprehend the significance of and their roles in pregnancy- related care in order to assist their wives in making the best decision regarding the use of sexual and reproductive health (SRH) services.
A cross-sectional study was carried out in Nigeria to evaluate the highlight the male partner involvements in the pregnancy relate care of the wives. Overall 367 participants were included in the study. The findings of the study revealed that most people (89.9%) thought they had a part to play in the care of their partners during labour and delivery (92.9%), and in the care of the newborn (97.5%). In terms of overall pregnancy-related care engagement, 56.9% were excellent. 20% of couples went to prenatal (19.6%) and postpartum (19.9%) clinics with their spouses. Good knowledge respondents were substantially more likely to accompany their partners to prenatal care (p=0.008) and postnatal care clinics, take part in birth preparation, and help with infant care [18].
Similarly, another similar study was carried out in Uganda. It was shown that few men participated in mother and child health care. Male participation in MCH was hampered by patriarchal communal beliefs and practices that influenced gender roles. Furthermore, there was insufficient awareness of the significance of male participation [19].
Moreover, another cross-sectional study was carried out to evaluate the involvement of the men in pregnancy related care. The findings of the study reported that male participation in prenatal care was very high (53.9%). The majority of responders (89%), decided to seek prenatal treatment together. At least once, more than half of respondents (63.4%) accompanied their spouses to the prenatal clinic. Less than a quarter (23.5%) of males was able to talk about pregnancy-related difficulties with their partner’s medical professionals [20].
In addition, an exploratory study was carried out to explore the factors which affect the male involvement in the pregnancy related care of the spouse. The major barriers to men getting involved in maternal health were lack of knowledge, social stigma, shyness/embarrassment, and work obligations [21]. Similarly, lack of education, knowledge about the importance of antenatal care, embarrassment and work burden are some of the factors reported by another study which affect the involvement of the husband in pregnancy related care [22]. Previous research on male involvement in antenatal care and family planning services, particularly accompanying partners to antenatal care clinics, were mostly directed at women. Interventions to lessen the burden of maternal illness and mortality in Pakistan can be informed by taking into account men’s knowledge and attitudes regarding their engagement in their partners’ obstetric care. This study was done to evaluate how men perceive, feel about, and participate in prenatal care. This will aid in understanding men’s personalities and act as a template for initiatives that specifically target reproductive health.
Methodology
Study Setting
This cross-sectional study was conducted at Hayatabad Medical Complex (HMC) in Peshawar, Khyber Pakhtunkhwa, within the gynecology ward. HMC is a tertiary care hospital with 700 beds, offering comprehensive gynecology and obstetrics services in the Peshawar district.
Study Duration
Data collection occurred over a six-month period, starting on January 2nd and ending on June 25th, 2022.
Sample Size Determination
The sample size was determined utilizing an online sample size calculator, adopting a 95% confidence interval, and a margin of error set at 5%. The anticipated sample size was calculated based on a previous proportion of 72% [18]. The formula employed for this calculation was:
( ) ( ) 2 2 * 1 * 1 n z p p d α = − −
Where: n: Preferred sample size p: Estimated prevalence d: Margin of error set at 0.05 z The standard normal deviation, conventionally set at 1.96 for a 95% confidence interval (α = 0.05). Hence, the calculated sample size for the study was 271 participants.
Sampling Techniques
Consecutive sampling techniques were employed to select participants for the study. Sampling Selection Criteria Inclusion Criteria: All pregnant women visiting the gynecology unit of HMC Peshawar during the specified data collection period were included in the study. Exclusion Criteria: Women who declined or were unwilling to participate in the study were excluded from the sample.
Data Collection Instrument
The data for this study were gathered using an adopted questionnaire, which was derived from a previously conducted research [18]. This questionnaire was thoughtfully structured and comprised three distinct sections, each serving a specific purpose. Section A: Socio-demographic Profile: The initial segment, denoted as “Section A,” was dedicated to collecting socio- demographic information from the participants. This part of the questionnaire included questions aimed at gathering essential background data. Section B: Perception of Male Involvement in Pregnancy- Related Care: The second segment, designated as “Section B,” encompassed a series of fourteen questions. These questions were designed to gauge the participant’s perceptions concerning the various roles that men can play in pregnancy- related care. This section sought to explore how participants viewed male involvement in this context. Section C: Assessment of Male Partner Involvement: The final portion, referred to as “Section C,” consisted of a comprehensive set of 26 questions. This section was specifically tailored to assess the degree of male partner involvement in pregnancy-related care. Participants’ responses to these questions were evaluated to determine the extent of their male partners’ engagement in this crucial aspect of care. Categorization of Involvement: Based on the responses collected, participants’ involvement in pregnancy-related care was categorized into two groups: “Poor Involvement” (defined as a score of less than 50%) and “Good Involvement” (characterized by a score exceeding 50%). This categorization allowed for a clear distinction between participants with varying levels of male partner involvement in the care during pregnancy.
Data Collection Procedure
The study began by securing the necessary ethical and institutional approvals. First permission was obtained from the Institute of Nursing Sciences, Khyber Medical University, ensuring compliance with ethical standards and research protocols. This step was essential to validate the study’s adherence to ethical principles and guidelines. Then an official Permission from hospital administration of Hayatabad medical complex was also obtained. Then investigators visited the outpatient department and approached the Participants who were visiting the hospital for their routine antenatal checkups became the target population for the study. These individuals were approached in a respectful and non-intrusive manner to seek their participation in the research. Prior to commencing data collection, participants provided written informed consent. Subsequently, the questionnaire was administered, and participants who faced reading challenges received assistance from the investigator to ensure accurate response recording. This meticulous data collection process spanned three months for comprehensive coverage.
Data Analysis
Data were analyzed using SPSS version 24. Frequencies and percentages were calculated for all the variables. Mean and standard deviation was calculated for contentious variables. Ethical Consideration: Written informed consent was signed by each study participant. Prior to gathering the data, the participants were fully informed of the study’s aims and objectives. The participants assured that the study would not give you any financial benefits. Data were gathered in a separate room to protect participant confidentiality, and participants assured that the data would never be shared with anyone other than the supervisor.
Results
Socio demographic profile of the Participants: The majority (59.4%) of the participants were from the age group of 30 to 40 years. Most (82.7%) of the participants were house wives while 61.3% of the participants were illiterate. The majority (72%) of the participant was reported that their monthly income is below 20 thousand (Table 1).
| Variables | Frequency | Percent (%) |
|---|---|---|
| Less than 30 Years | 61 | 22.5 |
| 30-40 Years | 161 | 59.4 |
| More than 40 Years | 49 | 18.1 |
| Total | 271 | 100.0 |
| House wife | 224 | 82.7 |
| Employed | 47 | 17.3 |
| Total | 271 | 100 |
| Illiterate | 166 | 61.3 |
| Primary | 57 | 21 |
| Secondary | 27 | 10 |
| Master | 21 | 7.7 |
| Total | 271 | 100.0 |
| Less than 20000 | 195 | 72.o |
| 20000-30000 | 44 | 16.2 |
| 31000-40000 | 17 | 6.3 |
| More than 40000 | 15 | 5.5 |
| Total | 271 | 100.0 |
Table 1: Socio-demographic profile of the participants, n=271.
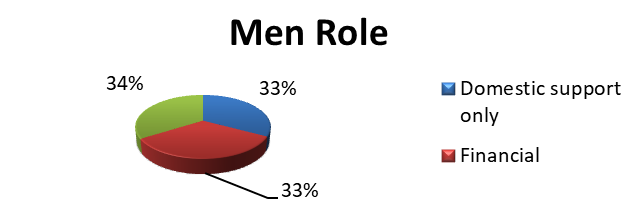
Men Role in Pregnancy related Care
The majority (34%) of the participants were reported that men have both role in domestic and financial role in pregnancy relate care followed by financial (33%) and domestic support [23] (Figure 1).
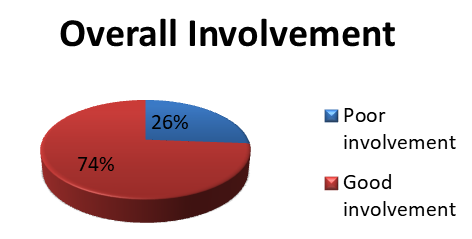
Overall Pregnancy Related Care
Overall, involvement of the men in the pregnancy related care was assessed. The majority (74%) of the participants reported good involvement of the male partner in pregnancy related care while 26% of the participants were reported poor involvement (Figure 2).
Discussion
The majority (74%) of the participants reported good involvement of the male partner in pregnancy related care while 26% of the participants were reported poor involvement. This is comparable to Nasreen et al. [24], who studied men’s awareness and knowledge of maternal, neonatal, and child health in rural Bangladesh and involvement in the pregnancy related care. In the Bangladesh study, both control and intervention group respondents had good involvement. Another study also supported the findings of the current study and reported that more than half (56.9%) of the respondents had good involvement in pregnancy related care [18]. There is a common misconception that women are solely responsible for pregnancy, childbirth, and the upbringing of their children [25]. However, the participation of men in these stages of life is extremely important, particularly in patriarchal societies like Nigeria, due to the elevated position of men in these societies [26].
However, the majority of studies have demonstrated that men can play a vital role in lowering maternal and newborn morbidity and mortality and, as a result, enhancing the overall wellbeing of both the mother and the child [17]. It has been observed that the support of the husband is a good predictor of future practice and ongoing use of family planning [23]. A study that was conducted in the Philippines in showed that the continuation rate of family planning among women whose husbands supported their contraceptive practice is significantly higher than the continuation rate of family planning among women whose husbands did not support [27]. This finding was supported by the fact that the study was conducted in 1984. In addition, Kalembo et al. [23] shown that the presence of a male partner was seen to enhance the number of people who utilized PMTCT services [28].
This finding is similar to the findings of a study that was carried out in India, where the majority (87.5% of the husbands) of the respondents were present during the delivery of their wives. Close to two-thirds of the respondents (66.1% of the total) accompanied their wives while they were in labour [29]. The vast majority of the respondents accompanied their pregnant partners to the postpartum clinic. The findings of Sadhana and colleagues in India are supported by this evidence. Nearly all of the participants in this study made sure to remind their wives to keep their appointments at the ANC clinic and PNC clinic. Previous research has found that this is consistent with its conclusions [30].
Even though men are not the recipients of pregnancy- related care services directly, their comprehension, participation, and support are essential for women to have in order for them to be able to obtain basic pregnancy-related care services. Low male involvement is a major determinant, and it has been shown that increasing their participation is vital for the reduction of maternal and infant morbidity and mortality in developing countries, despite the fact that many other factors contribute to increased maternal and infant morbidity and mortality in these countries [28, 31].
In spite of the fact that males participated in pregnancy-related care on average in this study, their level of involvement in the performance of care chores such as accompanying their spouse to prenatal and postnatal care or assisting in the changing of the baby’s diaper was low. The males who participated in this study reported a greater level of engagement in the provision of money and food, as well as the decision-making process regarding the partner’s attendance during antenatal care clinic appointments. The findings of other researchers who have conducted studies on men’s roles and involvement in maternal health care have been noted as being very comparable. This study found that just one out of every five respondents actively participated in accompanying their wives to antenatal care visits, which is consistent with the findings of earlier research [32, 33, 34].
The fact that the level of support differs across domains may be an indication of a difference in men’s ability to participate in sociocultural acceptable ways (like directing a female partner to behave in a particular way), as opposed to more stigmatized ways. Directing a female partner to behave in a particular way such as being absent from paid work to attend maternal and child health services.
Conclusion
The involvement of male partners in pregnancy-related care plays a pivotal role in providing essential support to expectant mothers during this critical phase. This study identified varying levels of involvement across different domains of pregnancy-related care. Notably, a high degree of involvement was reported in areas such as offering reminders and providing financial support. Conversely, the engagement of male partners in performing care tasks, such as accompanying their partners for clinic visits, was notably lower among the respondents. These findings underscore the importance of targeted interventions to enhance male partner participation in comprehensive pregnancy-related care [35, 36, 37, 38, 39, 40, 41].
Study Strength & Limitation
The study stands out as the first of its kind in Peshawar, Khyber Pakhtunkhwa, focusing on the assessment of male partner involvement in pregnancy-related care. This pioneering effort paves the way for a deeper understanding of this crucial aspect of healthcare in the region. The findings of this study also have the potential to be of substantial importance. By shedding light on the level of male partner engagement in pregnancy-related care, it can contribute significantly to efforts aimed at enhancing the quality of care provided to expectant mothers. One notable limitation is that the data collection was confined to a single healthcare sector. The study’s precision could have been further enhanced by collecting data from multiple healthcare sectors, providing a more comprehensive view of male partner involvement in pregnancy-related care.
Recommendations
Healthcare Professional Involvement
It is imperative for healthcare professionals to take an active role in educating male partners about their vital contributions to the care of pregnant women. This educational effort can serve as a catalyst for increased male involvement in pregnancy-related care.
Comprehensive Education
Male partner education should be pursued on multiple fronts. Counseling sessions specifically tailored to enlighten them about their role in pregnancy-related care are highly recommended. These sessions can effectively address misconceptions and encourage active participation.
Expanded Study Scope
To gain deeper insights into this crucial aspect of healthcare, it is advisable to conduct a similar study with a larger sample size. Additionally, involving multiple healthcare sectors in the research can provide a more comprehensive understanding of male partner involvement in pregnancy- related care. Such an expanded study would offer a more nuanced perspective and potentially yield more robust recommendations for enhancing male partner participation.
Declarations
- Source of Funding This research did not receive any specific grant from funding agencies in the public, commercial, or not for- profit sectors.
- Conflict of Interests The Authors have no any conflict of interest to declare.
- Ethics Approval The Ethical Review Committee of the Khyber medical University, Institute of nursing sciences has granted ethical approval for this study on 20/1/2022/ with No: KMU- INS/10-14-5792.
- Authors Contributions The cross-sectional study framework was crafted by Ihsan Ullah. Data collection was carried out by Nadeem Nadia, Mohibulah Niqab Nida. Additionally, Munira Nadeem and Naima conducted a comprehensive review of the existing literature. The subsequent stages of the study, including statistical analysis, data interpretation, and manuscript composition, were collaboratively accomplished by Ihsan Ullah and Niqab. Finally, the completed manuscript underwent a thorough review and received approval from all contributors.
- Acknowledgment The authors extend to Shabnam Shah, a dedicated lecturer at the Institute of Nursing Sciences, who provided invaluable assistance during both data collection and analysis planning. Furthermore, the authors would like to express their appreciation to the former Director of INS- KMU and the Director of ORIC KMU for their encouragement and support in shedding light on the important issue of transgender rights, which served as a profound motivation for us to conduct an in-depth investigation into this matter.
- Availability of Data and Materials Original datasets will be offer upon reasonable request to the corresponding author
References
-
Hoyert DL (2022) Maternal mortality rates in the United States, 2020. Indian J Appl Res 2(12): 132-139.
-
WHO (2019) Maternal mortality: evidence brief. J Nurses Prof Dev 2(1): 122-131.
-
WHO (2019) Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Matern Child Health J 2(2): 232-241.
-
Hanif M, Khalid S, Rasul A, Mahmood K (2021) Maternal mortality in rural areas of Pakistan: challenges and prospects. Rural Heal 27: 1040-1047.
-
Mullick S, Kunene B, Wanjiru M (2015) Involving men in maternity care: health service delivery issues. Agenda Spec Focus 6: 124-135.
-
Nations U, Cook RJ, Dickens BM, Fathalla MF (2020) Population and Development: Program of Action adopted at the International Conference on Population and Development. Cairo Dep Econ Soc Inf Policy Anal 2(11): 321-329.
-
Iliyasu Z, Abubakar IS, Galadanci HS, Aliyu MH (2010) Birth preparedness, complication readiness and fathers’ participation in maternity care in a northern Nigerian community. Afr J Reprod Health 14(1): 21-22.
-
Mackert M, Guadagno M, Lazard A, Donovan E, Rochlen A, et al. (2018) Engaging men in prenatal health via eHealth: findings from a national survey. JMIR Pediatr Parent 1(2): e9513.
-
Albuja AF, Sanchez DT, Lee SJ, Lee JY, Yadava S (2019) The effect of paternal cues in prenatal care settings on men’s involvement intentions. PLoS One 14(5): e0216454.
-
Deibel M, Zielinski RE, Rising SS, Kane-Low L (2018) Where are the dads? A pilot study of a dads-only session in group prenatal care. J Perinat Neonatal Nurs 32(4): 324-332.
-
Mangeni JN, Nwangi A, Mbugua S, Mukthar VK (2012) Male involvement in maternal healthcare as a determinant of utilisation of skilled birth attendants in Kenya. East Afr Med J 89(11): 372-383.
-
Morhason BIO, Olayemi O, Ojengbede OA, Adedokun BO, Okuyemi OO, et al. (2018) Attitude and preferences of Nigerian antenatal women to social support during labour. J Biosoc Sci 40(4): 553-562.
-
Narang H, Singhal S (2013) Men as partners in maternal health: an analysis of male awareness and attitude. Int J Reprod Contraception Obstet Gynecol 2(3): 388-393.
-
Britta CM (2015) Barriers to and attitudes towards promoting husband’s involvement in maternal health in Katmandu. Nepal Soc Sci Med 62(11): 2798-2809.
-
Ahmed S, Jafri H, Rashid Y, Yi H, Dong D, et al. (2019) Autonomous decision-making for antenatal screening in Pakistan: views held by women, men and health professionals in a low–middle income country. Eur J Hum Genet 27(6): 848-856.
-
Bilwani S, Anjum G (2022) Gender differences in making moral decisions: The ethics of care perspective in Pakistan. Ethics Soc Welf 16(1): 73-89.
-
Kadam SS, Payghan BS (2013) Role of father in key areas of maternal and child health: A cross-sectional study. Int J Curr Res Rev 5(6): 119-123.
-
Falade FO, Adebayo AM (2020) Male partners’ involvement in pregnancy related care among married men in Ibadan, Nigeria. Reprod Health 17(1): 14.
-
Muheirwe F, Nuhu S (2019) Men’s participation in maternal and child health care in Western Uganda: perspectives from the community. BMC Public Health 19(1): 1-10.
-
Teklesilasie W, Deressa W (2020) Barriers to husbands’ involvement in maternal health care in Sidama zone, Southern Ethiopia: A qualitative study. BMC Pregnancy Childbirth 20(1): 1-8.
-
Nasreen HE, Leppard M, Al Mamun M, Billah M, Mistry SK, et al. (2012) Men’s knowledge and awareness of maternal, neonatal and child health care in rural Bangladesh: a comparative cross sectional study. Reprod Health 9(1): 1-9.
-
Peter ND (2017) Factors associated with male involvement in maternal health care services in Jinja district, Uganda. Uganda Makerere Univ Sch public Heal 5: 68.
-
Robert CJP, Oppong K, Tuoyire DA (2017) male involvement in maternal health care Anamabo. Int J of Reproductive Med Mon.
-
Gibore NS, Bali T, Kibusi SM (2019) Factors influencing men’s involvement in antenatal care services: A cross- sectional study in a low resource setting, Central Tanzania. Reprod Health 16(1): 1-11.
-
Mullany BC (2016) Barriers to and attitudes towards promoting husbands’ involvement in maternal health in Katmandu, Nepal. Soc Sci Med 62(11): 2798-2809.
-
Kalembo FW, Zgambo M, Mulaga AN, Yukai D, Ahmed NI (2013) Association between male partner involvement and the uptake of prevention of mother-to-child transmission of HIV (PMTCT) interventions in Mwanza district, Malawi: a retrospective cohort study. PLoS One 8(6): e66517.
-
Toure LB (2019) Male involvement in family planning: a review of selected program initiatives in Africa. In SARA.
-
Secka E (2022) Men’s involvement in care and support during pregnancy and childbirth. Int Acad J Adv Pract Nurs 3: 222-229.
-
Glazener CMA (2017) Sexual function after childbirth: women’s experiences, persistent morbidity and lack of professional recognition. BJOG An Int J Obstet Gynaecol 104(3): 330-335.
-
Ezeh AC, Seroussi M, Raggers H (2016) Men’s fertility, contraceptive use, and reproductive preferences. Int Arch Med 18: 656-661.
-
Muheirwe F, Nuhu S (2019) Are health care facilities and programs in Western Uganda encouraging or discouraging men’s participation in maternal and child health care? Int J Health Plann Manage 34(1): 263-276.
-
Olugbenga BAI, Asekun OEO, Adewole AO, Adeomi AA, Olarewaju SO (2013) Perception, attitude and involvement of men in maternal health care in a Nigerian community. J public Heal Epidemiol 5(6): 262-270.
-
Becker S (2016) Couples and reproductive health: a review of couple studies. Stud Fam Plann 27(6): 291- 306.
-
Swetha T, Roseline V, Shivaswamy MS (2019) Knowledge and perception of men about postnatal care: community based study. Hindu 2(2): 185-190.
-
Geller SE, Koch AR, Garland CE, MacDonald EJ, Storey F, et al. (2018) A global view of severe maternal morbidity: moving beyond maternal mortality. Reprod Health 15(1): 31-43.
-
Collier AY, Molina RL (2019) Maternal mortality in the United States: updates on trends, causes, and solutions. Neoreviews 20(10): e561-74.
-
Bhatta DN (2019) Involvement of males in antenatal care, birth preparedness, exclusive breast feeding and immunizations for children in Kathmandu, Nepal. BMC Pregnancy Childbirth 13(1): 1-7.
-
Yargawa J, Leonardi BJ (2015) Male involvement and maternal health outcomes: Systematic review and meta- analysis. J Epidemiol Community Health 69(6): 604-612.
-
Tessema KM, Mihirete KM, Mengesha EW, Nigussie AA, Wondie AG (2021) The association between male involvement in institutional delivery and women’s use of institutional delivery in Debre Tabor town, North West Ethiopia: Community based survey. PLoS One 16(4): 1-15.
-
Dzinamarira T, Kuupiel D, Vezi P, Mashamba TP (2021) A scoping review on health education programs for improving Men’s engagement with health services in low- and middle- income countries. Public Heal Pract 2: 100177.
-
Awasthi S, Nandan D, Mehrotra AK, Shankar R (2018) Male participation in maternal care in urban slums of district Agra. Indian J Prev Soc Med 39(3): 181-183.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era