Facility Based Audit of Maternal Near Miss, Maternal and Neonatal Mortality in a Tertiary Hospital, South-West Nigeria: One-Year Review
Background: There is a poor linkage between MPDSR audits on the one hand, and the quality improvement processes proffered by them. This usually leads to varied implementation of recommendations. Buy-in from the community and health facilities are needed for full implementation. To better identify and track causes of maternal and perinatal mortality, it is necessary to combine review of maternal near-miss morbidities with findings at MPDSR meetings. Objectives: A. Evaluate near-miss morbidity and near-miss to mortality ratio. B. To compare the nature of near-miss morbidity with maternal mortality. C. To compare findings of near-miss maternal morbidity with maternal mortality among women who registered for care and those who did not. Design: Retrospective study. Methods: Monthly review of data collected on maternal near-miss morbidity and maternal mortality at MPDSR meetings for all women who delivered at our facility from 1st December 2022 till 31st December 2023. Results: The near-miss incidence ratio was 70 per 1000 live births while the maternal mortality ratio was 1399 per 100000 live births. Hypertensive disorders of pregnancy and sepsis were responsible for 85.8% of maternal mortality. Despite contributing 62.4% to maternal near-miss events, obstetric haemorrhage was responsible for 14.2% of maternal mortality. Unbooked patients were responsible for 83% near-miss morbidity and 95% of mortality occurred in this same group. Conclusion: While we have made some progress in our care of women with Postpartum haemorrhage, hypertensive disorders of pregnancy remains a cause for concern for both maternal near-miss morbidity and maternal mortality. Health workers should be trained to recognise and promptly refer women with hypertensive disorders for expert care pre-delivery, intrapartum and postpartum. Antenatal care and facility delivery for all pregnant women remain the pathways towards reducing near-miss morbidity and maternal mortality ratio.
Oladiran F Ayodeji1*, Mathew Adeyemo1, Michael Gbala1 and Bola Akinkunmi2
Keywords: Clinical Audit; Maternal Near-Miss; Maternal Mortality
Background
Maternal and perinatal mortality remain high in sub- Saharan Africa, especially in Nigeria. Nigeria has one of the highest figures of maternal mortality ratios (MMR) of 1047 per 100,000 live births (WHO 2023) [1]. Initial efforts to reduce the high MMR were focussed on identifying and reducing the major causes of maternal mortality, with little attention paid to perinatal mortality and near-miss maternal morbidities. Maternal morbidity, particularly near-miss events, poses a significant public health challenge, especially in low-resource nations like Nigeria. Near-miss maternal morbidity refers to severe complications during pregnancy, childbirth, or the postpartum period that nearly results in maternal death but are averted through timely intervention. In Ondo state in south-west Nigeria, the introduction of free maternity services and the launching in 2009 of the Confidential Enquiries into Maternal Mortality in Ondo State (CEMDOS), led to a significant reduction of maternal mortality [2]. Stand-alone initiatives, like CEMDOS in Ondo state was later replaced by a national program encompassing both maternal and perinatal audit.
In 2016, with the assistance of WHO, CEMDOS transited to Maternal and Perinatal Death Surveillance and Response (MPDSR) [3, 4]. By carefully watching maternal and perinatal deaths, trends in mortality can be detected and recurrence prevented through appropriate actions and responses implemented both at facility and regional levels. The MPDSR however threw up other challenges of implementation. State-level implementation of MPDSR in Nigeria was found to be inadequate because it is focussed on facility-based maternal deaths alone [5]. There is a poor linkage between MPDSR audits on the one hand, and the quality improvement processes proffered, leading to varied implementation of recommendations. Buy-in from the community and lower-level health facilities is needed for full implementation. The poor and inconsistent implementation at subnational and facility levels in Nigeria was confirmed by the recent work of Kinney MV and co-workers in 2020 [6]. In order to understand the social and cultural circumstances surrounding maternal and perinatal deaths, there is increasing advocacy for community-based MPDSR audits [7]. Community-based MPDSR brings greater participation and increasing collaboration with community leaders, society influencers and health care workers at the primary health centres [7].
The knowledge of maternal health and advocacy for preventing maternal deaths become a shared responsibility and can be domiciled where they are most needed. Obviously, the local political administration both local and state must be involved in this effort. At the facility level, efforts to track and reduce maternal and perinatal mortality must pay due attention to prevalent maternal near-miss morbidity in order to halt progression to full blown mortality. This is because inherent in near-miss events are the lessons of maternal death avoidance. Lazzerini and colleagues have confirmed the effectiveness of facility-based maternal near-miss review in reducing maternal mortality and quality of maternal care in high-burdened countries [8]. The health care worker takes centre stage in this process that leads to maternal death avoidance. The study by Merali and co-workers confirmed that health worker related factors accounted for 67% of avoidable factors in audits [9]. Therefore, understanding the dynamics of near-miss maternal morbidity in Nigeria is crucial for designing effective interventions aimed at reducing maternal mortality and improving maternal health outcomes. While this is well known, it is however not being commonly practiced [10]. There is need for continuous acquisition of clinical skills by health care workers both at primary care centres up to the tertiary facilities. This will help the prompt identification and management of maternal morbidities at these facilities. There is significant evidence that the inclusion of maternal near-miss audits as part of MPDSR meetings improve the quality of obstetric care at different levels of healthcare delivery [6, 10].
Such inclusion may familiarize and focus the attention of clinical practitioners and other healthcare workers on prevalent morbidities leading to continuous feedback to institutional managers. The aim of this paper is to record our experience and evaluate the contributions of near- miss maternal morbidities review as part of the regular MPDSR audit at the facility level in South-west Nigeria. This approach may ensure better implementation of MPDSR recommendations at the facility level by focusing healthcare workers on the prevalent near-miss morbidities. Continuous outreach of tertiary hospitals to less specialized level of care would, on the long run, stem the progression of maternal morbidities to maternal and perinatal mortalities. Such endeavors may add to the ongoing efforts to enhance maternal healthcare in order to reduce maternal mortality rates in Nigeria and other similar settings. This paper shares our experiences on the patterns of near-miss maternal morbidities and maternal mortality over a one-year period.
Objectives
- To determine the incidence of maternal near-miss morbidity and maternal near-miss to mortality ratio.
- To compare the nature of maternal near-miss morbidity with that of maternal mortality.
- To compare near-miss maternal morbidity and maternal mortality among women who registered for care at our facility (booked), with those who did not.(Unbooked)
Methods
Study Settings
The University of Medical Sciences Teaching Hospital, formerly known as the Mother and Child Hospital Ondo, came into existence in December 2012 in Ondo city, south- west Nigeria. A free maternal health service was provided at inception till 2016.A criteria-based contributory health insurance scheme, launched in December 2019, is now in operation in the state [11]. It incorporates subsidized fees for consultation, drugs and deliveries, both vaginal and surgical. The study was conducted from 1st of December, 2022 to 31st of December, 2023.
Subjects
All women who were admitted to our facility for their labour and deliveries and were within 42 days postpartum were eligible for this audit. Regular monthly audits of maternal near miss, maternal mortality and neonatal mortality were carried out during the period of this study by the institutional committee called MPDSR committee. This comprised of obstetricians, neonatologist, midwives and record officers. All women who met the WHO criteria3 for near-miss were selected for review of their case files each month by health information officers and their data inputted in the pro-forma forms provided. This was done prior to our monthly MPDSR meeting. WHO criteria for near-miss included a set of clinical, laboratory and interventional based criteria [3]. As is the usual practice, all records of maternal, perinatal and neonatal mortality were made available for the monthly auditing. Maternal and neonatal deaths were as defined by WHO in the MPDSR notification forms. The respective case-files were made available at these monthly audit meetings by the same information officer for perusal, confirmation and discussion. Relevant data was collected month by month from the case files into prepared pro-forma forms.
Data Treatment
The data on diagnostic conditions of maternal near- miss, causes of mortality, maternal booking status and neonatal outcome were collected. The data generated were analyzed using SPSS for window software version 25. The results were presented by frequency table, pie chart and bar chart. The Ethics Committee of the University of Medical Sciences Teaching Hospital, Ondo, waived the need for ethics approval for the collection, analysis, and publication of the retrospectively obtained and anonymised data for this study.
Result
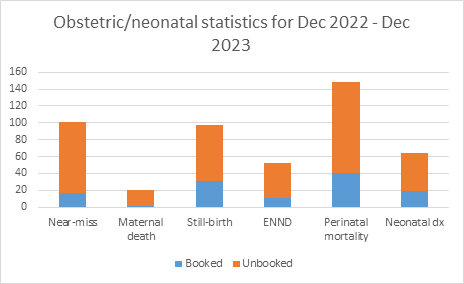
During the period of study, there were a total of 1526 deliveries, of which 1429 were live births. A total of 1,160 (76%) deliveries were in booked patients while the remaining 366 (24%) were in unbooked patients. The total number of near-miss cases was 101 while there were 20 maternal deaths. There were 19 (95%) mortalities in unbooked parturients and a single mortality in a booked patient. This same category of women (unbooked) contributed 83.2% of maternal near-miss cases. Details are presented in below (Table1, Figure 1).
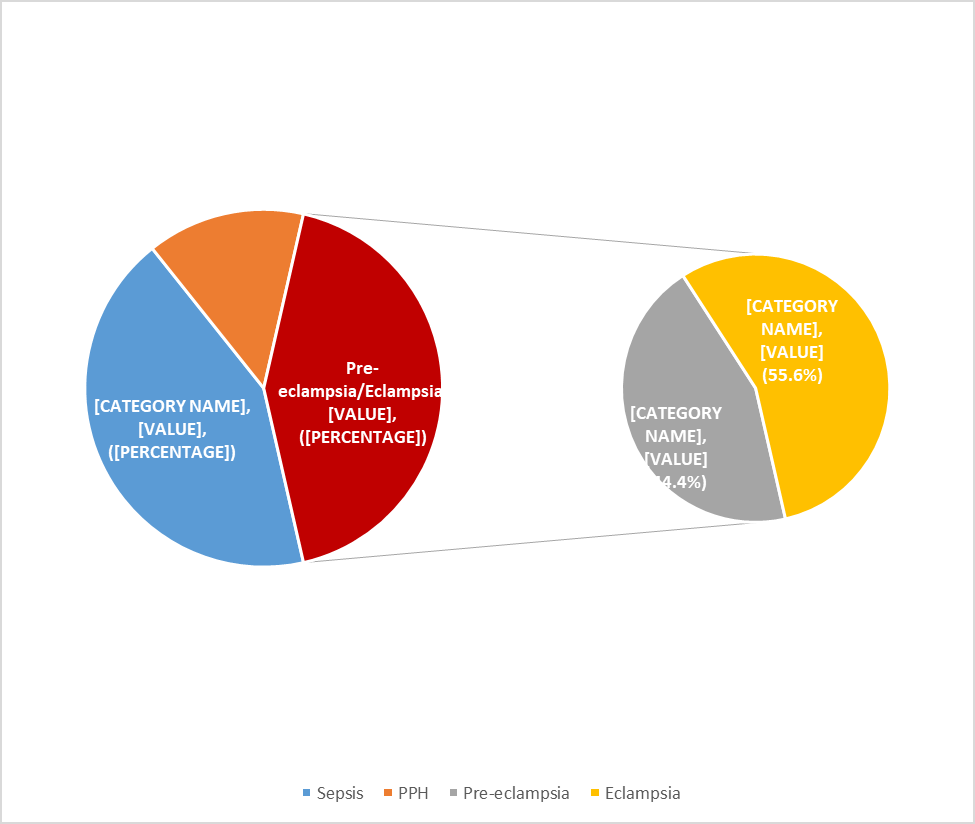
The most common causes of maternal mortality was hypertensive disorders of pregnancy (42.9%) and sepsis (42.9%) (Table 2,Figure 2). Postpartum haemorrhage (PPH) was responsible for 14.2% of maternal deaths. The most common type of near-miss was obstetric haemorrhage (62.4%), hypertensive disorders of pregnancy (29.6%), while sepsis was present in 5% of patients (Table 3). The calculated mortality index was higher for sepsis (64.2%) than for hypertensive diseases of pregnancy (23%) respectively. Obstetric haemorrhage had the lowest mortality index of 4.5%.
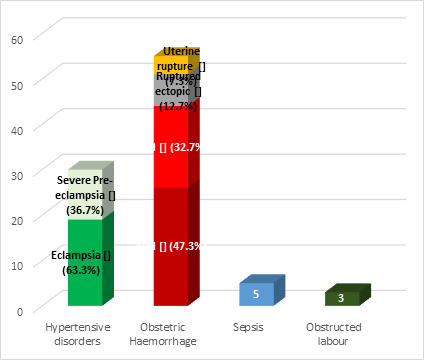
The maternal near-miss incidence ratio was 70 per 1000 live births; maternal mortality ratio was 1399 per 100000 live births, and maternal near-miss: maternal mortality ratio was 5:1. Maternal mortality index was 16.5% overall, while severe maternal outcome ratio was 85 per 1000 live births (Table 4).The maternal near-miss cases were caused by hypertensive diseases in pregnancy, obstetric haemorrhage, sepsis and obstructed labour. Though the obstetric heamorrhage was the leading cause of severe maternal outcome, it contributed lowest to maternal death. Maternal sepsis accounted for 5% of near-miss, 11.6% of severe maternal outcome but 42.9% of maternal deaths. Hypertensive diseases of pregnancy (inclusive of both severe pre-eclampsia and eclampsia) accounted for 32.3% of maternal near-miss, 32.2% of severe maternal outcome but 42.9% of maternal death during the study period. Obstructed labour contributed the lowest percentage to the maternal near-miss and accounted for none of the maternal mortality cases (Table 3, Figure 3).
During the study period, the total number of stillbirths was 97, while the number of early neonatal deaths was 52, making the perinatal mortality rate to be 104 per 1000 live births. The neonatal mortality rate was 45 per 1000 live births. The maternal booking status impacted greatly on fetal outcome (Tables 1 & 4) and (Figure 1).
| Month | Total Births | Booking status | Near miss | Maternal death | Still birth | Early Neonatal death | Perinatal Mortality | Neonatal death |
|---|---|---|---|---|---|---|---|---|
| Dec-22 | 116 | Booked | 0 | 0 | 2 | 2 | 4 | 3 |
| Unbooked | 10 | 2 | 8 | 1 | 9 | 1 | ||
| Jan-23 | 100 | Booked | 1 | 0 | 3 | 1 | 4 | 1 |
| Unbooked | 5 | 0 | 5 | 3 | 8 | 3 | ||
| Feb-23 | Booked | 0 | 0 | 1 | 1 | 2 | 2 | |
| 117 | Unbooked | 4 | 3 | 7 | 5 | 12 | 5 | |
| Mar-23 | Booked | 3 | 0 | 1 | 1 | 2 | 1 | |
| 132 | Unbooked | 6 | 2 | 8 | 5 | 13 | 5 | |
| Apr-23 | Booked | 5 | 1 | 2 | 2 | 4 | 3 | |
| 125 | Unbooked | 6 | 1 | 7 | 1 | 8 | 1 | |
| May-23 | Booked | 1 | 0 | 2 | 1 | 3 | 1 | |
| 154 | Unbooked | 7 | 3 | 2 | 4 | 6 | 4 | |
| Jun-23 | Booked | 0 | 0 | 4 | 1 | 5 | 2 | |
| 115 | Unbooked | 4 | 0 | 4 | 5 | 9 | 6 | |
| Jul-23 | Booked | 0 | 0 | 1 | 0 | 1 | 0 | |
| 119 | Unbooked | 7 | 1 | 4 | 3 | 7 | 4 | |
| Aug-23 | 101 | Booked | 2 | 0 | 2 | 1 | 3 | 2 |
| Unbooked | 3 | 1 | 3 | 2 | 5 | 4 | ||
| Sep-23 | 98 | Booked | 1 | 0 | 3 | 0 | 3 | 0 |
| Unbooked | 6 | 3 | 3 | 1 | 4 | 1 | ||
| Oct-23 | 142 | Booked | 1 | 0 | 5 | 0 | 5 | 1 |
| Unbooked | 11 | 4 | 6 | 5 | 11 | 6 | ||
| Nov-23 | 100 | Booked | 2 | 0 | 2 | 0 | 2 | 2 |
| Unbooked | 7 | 0 | 3 | 4 | 7 | 3 | ||
| Dec-23 | 107 | Booked | 1 | 0 | 3 | 1 | 4 | 1 |
| Unbooked | 8 | 0 | 6 | 2 | 8 | 2 | ||
| Total | Booked | 17 | 1 | 31 | 11 | 42 | 19 | |
| Unbooked | 84 | 20 | 66 | 41 | 107 | 45 | ||
| 1526 | 101 | 21 | 97 | 52 | 149 | 64 |
Table 1: Morbidity and Mortality Data for the Period of Study.
| Causes | Freq | % |
|---|---|---|
| Sepsis | 9 | 42.9 |
| PPH | 3 | 14.2 |
| Pre-eclampsia/Eclampsia | 9 | 42.9 |
| Pre-eclampsia | -4 | -44.4 |
| Eclampsia | -5 | -55.6 |
| Total | 21 | 100 |
Table 2: Causes of Maternal Mortality.
| Causes of maternal near misses | Frequency (%) |
|---|---|
| Hypertensive disease in pregnancy | 30 (29.6%) |
| Eclampsia | 19 |
| Severe Pre-eclampsia | 11 |
| Obstetric haemorrahge | 63 (62.4%) |
| APH | 30 |
| Uterine rupture | 5 |
| Post-partum Haemorrhage | 20 |
| Ruptured ectopic pregnancy | 8 |
| Sepsis | 5 (5.0%) |
| Obstructed labour | 3 (3.0%) |
| Total | 101 (100%) |
Table 3: Identified causes of Maternal Near Misses (MNM).
| Indices | Numbers |
|---|---|
| Total number of deliveries | 1526 |
| Total no. of live births (LB) | 1429 |
| No. of near-miss cases (MNM) | 101 |
| No. of maternal mortality cases (MD) | 20 |
| Maternal near-miss incidence ratio ( MNM / LB ) | 70 / 1000LB |
| Maternal mortality ratio ( MD / LB ) | 1399 / 100000LB |
| Maternal near-miss: maternal mortality ratio (MNM : MM) | 5 : 1 |
| Maternal mortality index ( MD / (MNM+MD) ) | 16.50% |
| Severe maternal outcome ratio ( (MNM+MD) / LB ) | 85 / 1000LB |
| Perinatal mortality rate ( PD / LB ) | 104 / 1000LB |
| Neonatal mortality rate ( ND / LB ) | 45 / 1000LB |
Table 4: Maternal Near-Miss and Mortality Indices. (LB- live birth; MNM- Maternal near-miss; MM- Maternal mortality; PD- Perinata
Discussion
Our maternal mortality ratio (MMR) in this study was 1399 per 100000 live births, while our maternal near-miss incidence was 70 per 1000 live births. These figures are higher than 1088 per 100000 live births and 15.8 per 1000 live births respectively obtained by Oladapo and co-workers from their nationwide multicentre cross-sectional study of 46 public tertiary hospitals in Nigeria [11]. However, our figure for MMR was lower than 2931.4 per 100000 live births obtained from a single tertiary hospital in Sagamu, southwestern Nigeria, over a three-year period [12]. Our maternal near-miss incidence of 70 per 1000 live births is indicative of the poor detection and late referral of these high-risk women to our facility. The overall mortality index of 16.5% suggests that on average; about two out of ten women did not survive their near-miss event. There is an urgent need to improve these outcome measures. Both obstetric haemorrhage and hypertensive disease of pregnancy were responsible for 92% of near-miss maternal morbidity.
While obstetric haemorrhage contributes 62.4%, hypertensive disease of pregnancy added another 29.6% to maternal near-miss. Our results agree with those of Oladapo and co-workers in their Sagamu, Nigeria study [12]. Sepsis and obstructed labour contributed 5% and 3% to maternal near-miss. Despite its low 5% contribution to near-miss morbidity, sepsis was responsible for 42.9% of maternal mortality, sharing the same figure with Pre-eclampsia/ Eclampsia. Postpartum haemorrhage (PPH) was responsible for 14.2% cases of maternal mortality, despite obstetric haemorrhage contributing the highest percentage (62.4%) to near-miss morbidity. Postpartum haemorrhage (PPH) has ceded its position as the number one cause of maternal mortality hitherto in our facility, to Pre-eclampsia/Eclampsia. This finding has been confirmed by other studies. Ephraim Samuels and colleague from Jos University Teaching Hospital in Nigeria found that hypertensive disorders in pregnancy as leading cause of maternal mortality being responsible for 47.36% of such deaths [13].
Hypertensive disorders of pregnancy are largely the purview of health workers who should promptly recognize and refer this anomaly for urgent expert treatment. The high contribution of 29.6% to maternal near-miss morbidity should be reduced by identification and prompt referral for treatment. Healthcare workers must have a low threshold to raised blood pressure. Failure of recognition of this sign may progress to pre-eclampsia/Eclampsia, with possible irreversible organ damage. Obstetric haemorrhage in general, has a low maternal mortality index of 4.5%. Better access to stored blood for transfusion, better management of 3rd stage of labour and prompt implementation of management protocols, may be responsible for this shift. This study has shown that sepsis has a high case-fatality rate, contributing 42.9% to maternal mortality in our series, despite the very low contribution (5%) to maternal near-miss morbidity. In addition, sepsis has the highest mortality index of 64.2%. Our finding is in agreement with those of Akpan and co-workers in their study from southern Nigeria [14].
Delay of access to treatment and the probable use of substandard and inadequate antibiotic regimen, may be responsible for this scenario. This finding should be investigated further. Our overall maternal death to near- miss ratio was 1:5. This figure is comparable with that of Oladapo in Sagamu, Nigeria of 1:4.8, and that by Ephraim Samuels and colleague of 1:4.5 from Jos University Teaching Hospital, Nigeria. The impact of booking status on near- miss morbidity and maternal mortality is made clear by the findings in this study. Unbooked women contributed 83.2% near-miss morbidity, while also being responsible for 95% maternal mortality. Booked women with better antenatal care had 16.8% near-miss morbidity and a far lower maternal mortality of 5%. Lower near-miss morbidity seems to lead to lower maternal mortality. The important lesson here is to ensure pregnant women are registered for antenatal care and have access to skilled attendant at delivery.
However, factors influencing maternal health services utilization must be taken into account in addressing this issue.15. Effective intervention to promote maternal health utilization must at least target community and policy- level factors [15]. It is important for political leaders to garner the political will that will ensure that obstetric care is brought closer to where people live with attendant well-organized ambulance services for efficient referral system [16]. Our poor perinatal mortality rate with a high stillbirth component, reflects poor health seeking behavior of our unbooked patients in this study. The morbidities that eventually cause fetal demise can be detected and treated at the antenatal clinic.
Conclusion
By highlighting near-miss morbidity at monthly MPDSR meetings, and reminding healthcare providers constantly about these, may foster better identification and expert treatment of same. Improving the hospital’s capacity to identify hypertensive disorders of pregnancy and sepsis is an important next step. This would require the design of protocols for the management of these morbidities and continuous outreach to less specialized levels of healthcare to train their personnel. Continuous monitoring of the implementation of MPDSR recommendations at the primary health centres is a necessity. These actions are more likely to halt the progression of near-miss to maternal mortality. The healthcare seeking behavior of women in the community must be improved through advocacy, and the enlistment of community leaders assured through the periodic outreach interactions with different strata of the community. Political leadership should be encouraged to garner the necessary will to bring maternal services closer to the people, thereby eradicating the delays characteristic of women who fail to utilize maternal health services.
Acknowledgement
We thank all the Consultant Obstetricians in our facility for the use of obstetric data of their patients. We acknowledge the help of Dr Obafemi, our obstetrics resident, for graphical presentation of data. We thank Ms Tomi Omiwole of our Health Information Unit for the presentation of case files of all patients at our monthly MPDSR meetings and collating data on near-miss morbidities for all patients.
Conflict of Interest
There are no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
-
World Health Organization. Trends in Maternal Mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division.
-
Oyeneyin L, van den Akker T, Durojaiye O, Obaado O, Akanbiemu F, et al. (2019) Confidential enquiries into maternal deaths in Ondo state, Nigeria- a comparative analysis. BMC Pregnancy and Childbirth 19(1): 514.
-
Pattinson R, Say L, Souza JP, van den Broek N, Rooney C (2009) WHO maternal death and near-miss classifications. Bull World Health Organ 87(10): 734.
-
(2014) Federal Ministry of Health National Guideline for Maternal Perinatal Death Surveillance and Response in Nigeria. Abuja FMOH.
-
Gebhardt GS, de Waard L (2024) Audit as a tool for improving obstetric care in low- and middle-income countries.Best Practice Research Clinical Obstetrics Gynaecology 94: 102477.
-
Kinney MV, Ajayi G, de Graft-Johnson J, Hill K, Khadka N, et al. (2020) It might be a statistic to me, but every death matters: An assessment of facility-level maternal and perinatal death surveillance and response systems in four sub-Saharan African countries. PLoS One 15(12): e0243722.
-
Bayley O, Chapota H, Kainja E, Phiri T, Gondwe C, et al. (2015) Community-linked maternal death review (CLMDR) to measure and prevent maternal mortality: a pilot study in rural Malawi. BMJ Open 5(4): e007753.
-
Lazzerini M, Richardson S, Gardelli V, Erenbourg A (2018) Effectiveness of the facility-based maternal near- miss case reviews in improving maternal and newborn quality of care in low-income and middle-income countries: a systematic review. BMJ Open 8(4): e019787.
-
Merali HS, Lipsitz S, Hevelone N, Gawande AA, Lashoher A, et al. (2014) Audit-identified avoidable factors in maternal and perinatal deaths in low-resource settings: a systematic review. BMC Pregnancy Childbirth 14: 280.
-
Oladapo OT, Adetoro OO, Ekele BA, Chanal C, SJ Etuk, et al. (2016) When getting there is not enough: a nationwide cross-sectional study of 998 maternal deaths and 1451 near-misses in public tertiary hospitals in a low-income country. BJOG 123(6): 928-938.
-
Famakinwa A (2019) Ondo kickstarts contributory health scheme; launch “Abiyamo” maternal, child health insurance.
-
Oladapo OT, Sule-Odu AO, Olatunji AO, Daniel OJ (2005) Near-miss obstetric events and maternal deaths in Sagamu, Nigeria: a retrospective study. Reprod Health 2: 9.
-
Samuels E, Ocheke AN (2020) Near-miss and maternal mortality at the Jos University Teaching Hospital. Niger Med J 61: 6-10.
-
Akpan U, Asibong U, Omoronyia E, Arogundade K, Agan T, et al. (2020) Severe Life-Threatening Pregnancy Complications “near-miss’ and Maternal Mortality in a Tertiary Hospital in Southern Nigeria: A Retrospective Study. Obstetrics and Gynecology International 2020: 3697637.
-
Babalola S, Fatusi A (2009) Determinants of use of maternal health services in Nigeria- looking beyond individual and household factors. BMC Pregnancy and Childbirth 9: 1-13.
-
Kuti O, Ayodeji OF, Awowole IO, Adesina OA, Raji HO, et al. (2020) Reducing Maternal Mortality in Nigeria: Why Progress is Stalled and the Way Forward. Trop J Obstet Gynaecol 39(2): 10-17.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era