A Comprehensive Update on the Medical Treatment of Endometriosis-Correlated Pain Clinically with Emphasis over Pharmacokinetics, Pharmacodynamics, Biochemistry, Safety and Effectiveness of Accessible Options in a Condition not having Permanent Cure Till Date: A Narrative Review
Having comprehensively reviewed the etiopathogenesis, medical, surgical therapies in addition to revival of surgery in endometriosis, in particular circumstances earlier here our main idea is to present the update of the available medical treatments, specifically in case of pain amelioration with emphasis over Pharmacokinetics, Pharmacodynamics, Biochemistry, Safety and effectiveness of currently accessible medical treatment for Endometriosis-correlated pain. Here we conducted a narrative review utilizing search engine PubMed, Google scholar, Web of science, Embase, Cochrane review library utilizing the Mesh terms like; endometriosis; medical treatments; Non Steroidal Anti Inflammatory Drugs (NSAIDS); Combined Oral contraceptives (COC); progestins; selective estrogen receptors modulators (SERM); selective Progesterone receptors modulators (SPRMs); Aromatase Inhibitors (AI); GnRH agonists; GnRH antagonists; Levonorgestrel releasing intra uterine system (LNG-IUS) from 1993 till April 2024.We found a total of 1500 articles out of which we selected 115 articles for this review. No meta-analysis was done. Thereby we have reviewed in detail pros &cons of various NSAIDS, COC’s, SERM’s, SERM’s tamoxifen Raloxifene, Bazedoxifene (BZA) fulvestrant of which are none clinically of use SPRMs, Progestins inclusive of medroxy progesterone acetate (MPA), Norethindrone acetate (NETA) and dienogest, of GnRH agonists-Leuprolide Acetate, of oral GnRH antagonist, relugolix linzagolix, elagolix, of AI’s letrozole, anastrazole, of the SPRMs mifepristone, Asoprisnil, ulipristal acetate (UPA) Vilaprisan & Lonaprisan of which till now only mifepristonel is of little use & UPA for select few where no history of liver disease of all these NSAIDS, COC’s, progestins need to be first line with them having better tolerability, efficacy and economical overall in contrast to 2nd line GnRH agonists, GnRH antagonists or AI’s. Dependent over this, key preferences are isolation of new noncontraceptive in addition to non-hormonal’ approaches for diminishing propagation of endometriosisis, thus chances of pregnancy getting feasible.
Introduction
Endometriosis portrays one of the commonest chronic gynecologic disorders correlated with cyclic pelvic pain, subfertility or both [1]. It influences around 20% women hospitalized in view of pelvic pain in addition to 50% women having infertility [2]. Endometriosis symptoms differ from mild to robust, however in maximum women afflicted with endometriosis possess a requirement on monthly consumption of analgesics as well as usually possess a bad health correlated quality of life (QOL) [3, 4]. Moreover, commonly misdiagnosed result in continuously delivery of efficacious pharmacologic treatment with considerable prohibitive cost incurred [1].
Over the last years various medicines in addition to surgery therapies have been advocated along with used with variable outcomes obtained based over stage of the disease [5]. Despite the utilization of surgery strategy is restricted transitorily for the pain relief in women wishing to conceive spontaneously. However the actions pertaining to the pain constituents do not usually attain success [3]. Furthermore, ovarian surgery possesses the capacity of resulting in inimical total gonadal function along with ovarian reserve apart from being correlated with complications correlated with surgery, based over the region of the endometriotic damage [6]. Although, there is absence of good corroborative proof a meta-analysis performed recently illustrated no advantages of operative laparoscopy regarding fertility correlated or inimical sequelae on contrasting with diagnostic laparoscopy [7]. Taking into account, the publications, the rate of recurrence of pain symptoms subsequent to surgery are not occasional [8]. The other part of surgery is regarding preferences of subjects that is yet uncharted in case of prospective trials [7]. Present medicine choice in endometriosis treatment which has been fashioned with regards to women wanting to postpone or prevent surgery attracts a long term methodology which facilitates a long term controlling of their symptoms for instance chronic pelvic pain [9]. Pharmacologic treatment in the long term circumstances need to balance clinical effectiveness with the acceptablity of the safety profiles. Nevertheless, the objective of endometriosis pharmacologic treatment is abrogating chronic pelvic pain in addition to preservation of woman’s fertility on wanting conception. Here our concentration has been on identification of publication where assessment of presently utilized therapies for endometriosis correlated pelvic pain with the particular emphasis over their characteristics, safety profiles as well as clinical effectiveness. Earlier we have comprehensively reviewed the etiopathogenesis, medical, surgical therapies in addition to revival of surgery in particular circumstances here our main idea is to present the update of the available medical treatments, specifically in case of pain amelioration [10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22].
Methods
Here we conducted a narrative review utilizing search engine PubMed, Google scholar; web of science; embase; Cochrane review library utilizing the MeSH terms like; endometriosis; medical treatments; Non Steroidal Anti Inflammatory Drugs (NSAIDS); Combined Oral contraceptives (COC); Progestins; selective estrogen receptors modulators (SERM); selective progesterone receptors modulators (SPRMs); Aromatase Inhibitors (AI); GnRH agonists; GnRH antagonists; Levonorgestrel releasing intra uterine system (LNG-IUS) from 1990 till April 2024.
Results
We found a total of 1500 articles out of which we selected 115 articles for this review. No meta-analysis was done.
Etiopathogenesis of Endometriosis
Here although we will only focus on medical therapies meant for pain relief we will just briefly introduce the etiopathogenesis-[already reviewed in detail by us in 2016 in Kulvinder KK, et al. [13] and Shi J, et al. [23] (Figure 1).
![Figure 1: Mechanism of endometriosis pathogenesis in the text. Inflammation is the central link in the pathogenesis of endometriosis. Inflammation promotes the synthesis of estrogen. Increased estrogen level promotes apoptosis and the secretion of inflammatory factors like TNF-a and IL-1β, thus forming a vicious circle. Under the stimulation of the inflammatory factors on epigenetic change and/or progesterone receptor mutations, progesterone resistance occurs, which leads to decidualization insufficiency. Driven by inflammation, angiogenesis and lymphangiogenesis increased, neurogenesis, and endometriosis lesions formed and continued to develop. Black arrows: stimulation; red arrows: inhibition; TNF-a: tumor necrosis factorα; IL-1β: interleukin-1β; COX-2: cyclooxygenase type 2; StAR: steroid acute response protein (StAR); ER β: estrogen receptor β; SGK1: serum and glucocorticoid-regulated kinase FOXO-3a: forkhead box class o 3a; PGE2: prostaglandin E2; cAMP: cyclic adenosine monophosphate; P: progesterone; PR: progesterone receptor; VEGF: vascular endothelial growth factor [23].](/fulltextimages/12749/fig_1.png)
Figure 1: Mechanism of endometriosis pathogenesis in the text. Inflammation is the central link in the pathogenesis of endometriosis. Inflammation promotes the synthesis of estrogen. Increased estrogen level promotes apoptosis and the secretion of inflammatory factors like TNF-a and IL-1β, thus forming a vicious circle. Under the stimulation of the inflammatory factors on epigenetic change and/or progesterone receptor mutations, progesterone resistance occurs, which leads to decidualization insufficiency. Driven by inflammation, angiogenesis and lymphangiogenesis increased, neurogenesis, and endometriosis lesions formed and continued to develop. Black arrows: stimulation; red arrows: inhibition; TNF-a: tumor necrosis factorα; IL-1β: interleukin-1β; COX-2: cyclooxygenase type 2; StAR: steroid acute response protein (StAR); ER β: estrogen receptor β; SGK1: serum and glucocorticoid-regulated kinase FOXO-3a: forkhead box class o 3a; PGE2: prostaglandin E2; cAMP: cyclic adenosine monophosphate; P: progesterone; PR: progesterone receptor; VEGF: vascular endothelial growth factor [23].
Non-Steroidal Anti Inflammatory Drugs (NSAIDS)
Subsequent to their getting introduced NSAIDS have been one of the maximum broadly agents utilized over the counter throughout the world, with the maximum utilization in subjects afflicted with chronic pelvic pain in addition to chronic inflammatory situations [9]. As per their biochemical properties NSAIDS might be classified dependent on their selectivity regarding hampering cyclooxygenase (COX)/ prostaglandin–H2 (PGH2). The other classification, albeit occasionally utilized in the clinical scenario is based over their chemical structures, dividing them into main ones obtained from salicylic acid, acetic acid, enolic acid, anthracitic acid or propionic acid [24]. Furthermore, NSAIDS might be classified dependent on their plasma half-life (t1/2) into i) short acting (t1/2<6h) for instance aspirin along with ibuprofen as well as ii) long acting (t1/2>10h) for instance naproxen.
Of the biggest benefits of NSAIDS is considerably greater bioavailability irrespective of the route of delivery in addition to moderate to greater lipid solubility, aiding in their crossing of the blood brain barrier(BBB) [25]. A greater preference for the plasma proteins(for instance albumin) impacts drug depletion, hepatic metabolism basically by for instance the microsomal CYP enzymes possesses the capacity of clearance of NSAIDS in the form of inactive metabolites which get eliminated in the urine as well as bile of this group CYP29 basically aids in clearance of NSAIDS whereas allelic variants in this protein influence pharmacotherapeutic effectiveness that is based over the pharmacogenomic variation in population studies) [26].
Pertaining to the clinical perspectives, despite broadly utilized, NSAIDS do not possess corroboration with decreased quality of proof in view of risks in addition to bias are imprecise [27]. Kauppilla as well as Ronnberg performed a study which illustrated advantageous clinical actions of Naproxen sodium in contrast to placebo regarding treatment of endometriosis associated pain [28]. Presently no validating proof exists in term of any particular NSAIDS has greater efficacy. In view of the well acknowledged atherothrombombotic vascular processes correlated with PGH2hampering agents, non-particular hampering agents of both the enzymes is the only option which might be believed to be having reason for utility regarding pain relief in such group of agents [29]. Moreover clinical practitioners in clinical scenario need greater awareness pertaining to the nephrotoxicity regarding plausible renal failure [30]. Combined Oral contraceptives (COC) Combined Oral contraceptives (COC) portray long term safety approach in treatment of pain associated with endometriosis [9]. Utilization of COC’s is a feasible approach in the form of oral tablets, contraceptives ring or transdermal patches in sequential or continued regimens having low dose or greater dose of specific substances. Despite COC’s yields variable benefits in the form of contraception, controlling of the menstrual cycle, lesser probability of inimical sequelae as well as are cheap, their pharmacokinetics profiles illustrated considerable, inter subject variability modulated by CYP enzyme actions, in addition to variation in ethnicity [31]. These days escalated degree obesity in the population is certainly implicated in maximum inter subject variability; nevertheless occasional case of obesity have not been fully charted. Variable pharmacokinetics studies had conclusions drawn that changes in COC’s metabolism in obese women is a frequent characteristic [32]. In brief obesity basically influences 4 events responsible for absorption, organization, metabolism as well as excretion. Of the critical estimators in case of COC’s clinical actions is hepatic first pass metabolism that defines bioavailability. Pertaining to the estrogen bioavailability for ethinyl estradiol (maximum utilized estrogen constituents) illustrates a wide variety, from 25-65% [33]. Regarding maximum synthetic progestins processes bioavailability is as much as 90% [32]. Regarding patients with normal weight, the time to the maximum quantities in the systemic circulation is 1-3 h, t1/2 varies from 12-24, based over the kind of formulation [31]. The other bothersome thing is the plausible crosstalk amongst and the therapeutic substance [34]. Utilization of COC’s has been done for decades in the form of first line, illustrating plethora of actions over the endometriosis associated symptoms by stimulating atrophy of both eutopic in addition to ectopic endometrium, restricting retrograde menstrual flow, hampering proapoptotic in addition to anti-inflammatory actions over the endometriotic lesions [35]. In reference to the clinical efficacy (leading to lesser endometriosis associated pain) practically a third of patients getting treatment do not display reactions owing to progesterone resistance [10]. Nevertheless, variable randomized controlled trials (RCT), have reported COC’s tobe efficacious in the treatment of pain associated with endometriosis [36]. As far as other strategies (vaginalring /transdermal patches) it might be concluded from whatever patients favour [37, 38]. 143 patients with manifestation in the form of deep infiltrating endometriosis received treatment with desogestrel only contraceptive pill or sequential contraceptive vaginal ring for 12 months. The ultimate outcomes obtained definitely displayed effectiveness in both the arms with greater patient satisfaction with the desogestrel only contraceptive pill arm [37] (Figures 2 & 3) for basic structure of COC’s& progestins only pill [39].
![Figure 2: ** Courtesy ref no-Structure of COC’s [39].](/fulltextimages/12749/fig_2.png)
Figure2: Courtesy ref no-Structure of COC’s [39].
![Figure 3: Courtesy ref no-Structure of progestins only pill [39].](/fulltextimages/12749/fig_3.png)
Progestins
Progestins portray a good clinical alternate agent pertaining to women with the manifestation of pain associated with endometriosis as well as their myriad delivery routes might offer greater advantages regarding compliance in contrast to COC’s [40]. With regards to clinical efficacy, progestins are efficacious in attenuating pain in women having gastrointestinal in addition to rectovaginal endometriosis as well as have illustrated outcomes obtained which are equivalent to that with surgery for the treatment of dyspareunia associated with endometriosis [41]. The basic pharmacological actions of progestins can be concluded as changing the frequency along with degree of tonic pulsatile gonadotropin releasing hormone (GnRH), thereby work on liberation of follicle stimulating hormone (FSH) as well as Luteinizing hormone (LH), thus sequentially influencing repression of ovarian steroid hormone generation subsequent to continued delivery. A mode which is germane to pain associated with endometriosis is leading to decidualization of eutopic in addition to ectopic endometrium, respectively. As per their biochemical structures progestins classification is into 17αhydroxy progesterone or 19 nor testosterone derivatives delivered via variable routes for instance oral formulation, depot subcutaneous as well as intramuscular injections, transdermal patches ,vaginal gel or ring in addition to intra uterine system(IUS) [40, 42]. The quantities of progesterone accessibility ,illustrated their biological effects in target tissues gets impacted by delivery routes, metabolism in addition to bioavailability. Akin to orally delivered COC’s, progestins ingestion orally go via hepatic first pass metabolism leading to significantly diminished active plasma quantities of substances in contrast to parenterally delivered progestins [42]. Furthermore parenterally delivered progestins go via hepatic metabolism, nevertheless, experimental studies have pointed that metabolism might further take place at the region of delivery or target regions where expression of steroid metabolizing enzymes exists for instance skin, vagina endometrium along with uterus [43]. The bioavailability of progestins is akin to that of COC’s, nevertheless, present outcomes are restricted in addition to gets impacted by the inter subject variability [43]. Regarding plasma half-life (t1/2), the germane short t1/2 of progestins quantities reasons out why it is essential to deliver once daily oral progestins for the sustenance of clinical effectiveness. Despite the availability of myriad of progestins, total understanding of pharmacokinetics is restricted which makes it mandatory that performance of future evaluation gets done.
As per the maximum current cochrane review progestins are specifically effective in women afflicted with dysmenorrhea long term safety as well as tolerability [36]. Nevertheless, just a single study (of the 13 used) utilized 100mg/day medroxy progesterone acetate (MPA), was observed tobe efficacious in contrast to placebo regarding regulation of pain associated with endometriosis [44]. Subsequently various randomized controlled studies publications corroborated the utilization of progestins in the form of monotherapy ameliorated pelvic pain correlated with endometriosis [45]. Furthermore, it was advocated to motivate the patients with deep infiltrating endometriosis for the relief of pain symptoms by clinical utilization of progestins [46]. Dienogest, a 4th generation selective progestin having a direct anti-inflammatory actions got interest in a justifiable manner pertaining to the regulation of pain associated with endometriosis along with the recurrence of disease [40]. De Andres, et al. [47], in a systematic review conducted on Dienogest, illustrated considerable effectiveness in the treatment of endometriosis, which was comparable to GnRH analogues possessing greater safety as well as tolerability over GnRH analogues [40]. One more advantage of progestins in contrast to COC’s, is lesser probability of venous thromboembolism (VTE) risk in addition to greater tolerability (implying utilization of progestins is feasible in patients afflicted with migraine with aura in patients<35 years old [48]. Despite well tolerated, economical , in addition to restricted inimical sequelae progestins do not possess the capacity of curing disease with common recurrence of disease following omitting progestins therapy [48] (Figure 4).
![Figure 4: Courtesy ref no-Structure of dienogestrel [23].](/fulltextimages/12749/fig_4.png)
Gonadotropin Releasing Hormone Agonists
Subsequent to the invention of Gonadotropin releasing hormone (GnRH alias Luteinizing hormone releasing hormone (LHRH), variable GnRH analogues have been generated for the treatment of gynecologic disorders for instance - uterine fibroids, endometriosis, in addition to central precocious puberty’’ [49]. GnRH portrays a small decapeptide (pyro-Glu- His-Trp-Ser-Tyr-Leu-ArgPro-Gly-amide) generated as well as stored in mediobasal hypothalamus in addition to possessing a key part in controlling reproduction by controlling the liberation of gonadotropins from the pituitary. The effects of GnRH as well as its analogues get modulated by G- protein coupled receptors( GPCRs) where expression take place over the of pituitary gonadotrophs, placenta, uterus, ovary, in addition to prostate gland [50].
Out of the GnRH agonists, Leuprolide Acetate is the one which apart from having maximum utilization, further provides considerable potent mechanistic mode, clinical pharmacology, safety as well as tolerability [51]. Leuprolide Acetate, represents a synthetic nonapeptide GnRH analogue with the biochemical name (5-oxo-Lpropyl- Lhistidyl-L tryptophyl-Lseryl-Ltyrosyl-D-Leucil-L Leucil,L- arginyl-Nethinyl-L prolinamide acetate with availability in plethora of variable delivery routes along with dosages [52]. In contrast to endogenous GnRH , Leuprolide acetate possesses greater potency in view of longer half- life(t1/2), as well as greater affinity with regards to GnRH receptors with akin bioavailability irrespective of delivery routes(subcutaneous[s/c] vs intravenous[i/v]) [53]. GnRH agonist have further been generated for the nasal(i/n) delivery (for instance Nafarelin).
Despite, believed tobe an agonist, on delivery in therapeutic dosages persistently generates hampering of hypothalamic-pituitary- gonadal (HPG) axis amongst 2-4wks [52]. Nevertheless, these effects totally get reverted once the cessation of the agent takes place. Despite the mechanistic mode modifications is feasible subsequent to the cessation of the therapy, inimical sequelae for instance - changed lipid profiles, hot flushes, as well as elimination of bone mineral density(BMD), their long term utilization gets restricted [53]. Brown, et al. [54], conducted a comprehensive Cochrane systematic review as well as meta- analysis published 12 years earlier, performed assessment of utilization of variable dosages, regimens, in addition to routes of delivery regarding improvement of pain symptoms associated with endometriosis [54]. It was inclusive of, 41 randomized controlled trial (RCT), in the ultimate evaluation having 2935 women. As per the observations of Brown J, et al. [54], GnRH agonist proved to be an alternative with greater advantages in contrast to placebo in addition to danazol in provision of pain relief for pain associated with endometriosis specifically with dysmenorrhea [54]. Various RCT’s have illustrated greater effectiveness of GnRH agonist in contrast to placebo or no treatment [55]; nevertheless, there is restricted corroborative evidence regarding ideal dosages, time period of therapy ,routes of delivery of GnRH agonists. In the studies quoted previously utilization of GnRH agonists was by s/c,i/m,i/n formulations/ routes in various daily along with monthly regimens. Comparison of GnRH agonists have been performed to practically each of the presently accessible hormonal therapies utilized for the treatment of endometriosis associated pain. In summary in contrast to progestins along with COC’s, GnRH agonists possess the capacity of diminishing pain symptoms, improvement of quality of life, nevertheless, without intergroup variation [56, 57]. Pertaining to the variety of routes of delivery amongst GnRH agonists, present proof illustrated that no statistically significant variations amongst groups for pelvic pain, deep dyspareunia in addition to dysmenorrhea were observed [58]. Moreover, Zheng O, et al. [59], illustrated in their meta-analysis that GnRH agonists further possess the capacity of avoidance of recurrence, on utilization of postoperative GnRH agonist treatment for long term (over 6mths) [59] (Figure 5).
![Figure 5: Courtesy ref no-Structure of GnRH agonists [39].](/fulltextimages/12749/fig_5.png)
Gonadotropin R releasing Hormone Antagonists
Apart from GnRH agonists, GnRH antagonists do not stimulate the gonadotropin liberation, flareto start with; nevertheless, result in an immediate repression of gonadotropin liberation which might be reverted by competition with the endogenous GnRH with regards to its pituitary- receptors. One further benefit over the GnRH agonists is the dosage based actions; specifically repression of pituitary in addition to ovarian hormone is sustenance partly in the lesser dosages whereas greater dosages are correlated with complete repression (Figure 5). Illustrates the biochemical structure of GnRH antagonists , as well as their key placement for instance at the 2,3 location , that are implicated in gonadotropin liberation as well as at the location 6 implicated in cleavage of the enzymes. Pertaining to the pharmacokinetics characteristics of GnRH antagonists with particular reference of maximum antagonist delivery (Cmax),a linear design takes place subsequent to single or numerous dosages) [60].
Orally delivered GnRH antagonists in 12 premenopausal women who volunteered for relugolix oral delivery in a single dosage (40mg) led to Cmax of 29.05ng/ml subsequent to 90’ (t1/2 45.42h [61]. GnRH antagonists clearance basically takes place by metabolic along with liver route [62]. The later generation of GnRH antagonists possesses the properties of lesser histamine liberating resulting in improvement of their safety in addition to tolerability [60].
In view of their pharmacodynamics they might be initiated at the time of requirement for controlled ovarian hyper stimulation (COS) for avoidance of LH surge [62]. Akin to the GnRH agonists, the GnRH antagonists possess the capacity of getting translated into day- day clinical practice pertaining to the treatment of endometriosis, uterine fibroids as well as benign prostatic hyperplasia (BPH) [9, 61]. Pertaining to the delivery routes availability of the GnRH antagonists are in the form of oral nonapeptide preparations along with parenterally delivered formulations. Of the maximum current RCT evaluated the actions of the latest oral GnRH antagonist, relugolix linzagolix, over the pain associated with endometriosis [63]. Donnez J, et al. [63], observed in contrast to placebo, dosages≥ 75mg led to significantly greater percentage of the patients with complete response to pelvic pain, dysmenorrhea in addition to non-menstrual pelvic pain at 12 wks. Moreover, mean BMD depletion at 24 weeks escalated in a dosage based patterns for a 200mg regimen [64]. In a phase 2RCT Diamond et al. [65], revealed that elagolix was efficacious in resulting in pain relief on assessment of 155 women having laparoscopically corroborated endometriosis, possessed acceptable efficacy in addition to safety in contrast to placebo. Here elagolix revealed a considerably great clinical actions over diminishing dysmenorrhea in addition to non- menstrual pelvic pain scores with acceptability of safety as well as tolerability.2 double blinded, randomized 6mths phase 3 trial (Elaris-I as well as Elaris-EM-II) performed assessment of 150mg/day as well as 200mg twice/day regimens in contrast to placebo in 155 women having laparoscopically corroborated endometriosis in addition to moderate to robust endometriosis pain symptoms. Despite certain percentage of hypo estrogenic inimical sequelae got illustrated in elagolix study groups, both greater in addition to lesser dosages of elagolix were efficacious in pain relief in dysmenorrhea along with non-menstrual pelvic pain at the time of 6mth duration in women having endometriosis correlated pain. Furthermore, both Elaris trials pointed that elagolix generated improvement of all angles of health correlated QOL which clinically possess a meaning for the patients [65]. A cost evaluation of elagolix versus leuprolide acetate observed that elagolix was possessing superiority over leuprolide acetate regarding therapy of moderate to robust endometriosis correlated pain symptoms at the time of 1-2year duration. Recently in 2022 Guidice C, et al. [66], revealed in SPIRIT trial once daily oral relugolix combination therapy resulted in significant improvement of endometriosis correlated pain along with had good tolerability in 638 patients that got recruited [66].As per this SPIRIT trial outcomes, it got posited this possessed the capacity of meeting the clinical requirement that had not been currently attained with regards to long term medical therapy of endometriosis, diminishing the requirement for utilization of opioid or recurrent surgical therapies [66] (Figures 6-10).
![Figure 7: Courtesy ref no-Structure-activity relationship of Elagolix and 1, 2 and 3 structure [23].](/fulltextimages/12749/fig_7.png)
![Figure 8: Courtesy ref no-Structure-activity relationship of SK12496and structure of 4 [23].](/fulltextimages/12749/fig_8.png)
![Figure 9: Courtesy ref no-Structure-activity relationship of BAY1214784 (linzagolix) [23].](/fulltextimages/12749/fig_9.png)
Aromatase Inhibitors
Theidea of utilization of the 3rd generation aromatase inhibitors (AI)is a selective hamperingof enzyme aromatase cytochrome P450(CYP19A1), crucial enzyme in the synthesis of estrogens leading to repressionof estrogens generation via androgens is found typically in endometrium of women with endometriosis, adenomyosis, leiomyoma ,but not that in healthy women [67]. This enzyme has a role in the androstenedione-T-Estrone to estradiol respectively along with in peripheral tissues.
There, clinical utilization is restricted to adjuvant in addition to Neoadjuvant scenario in breast cancer (BC) therapy; nevertheless, AI’s have illustrated size diminishing actions over endometriotic areas [68]. 3rd generation AI’s possess greater selectivity apart from greater pharmacological robustness in contrast to earlier 2 generations of AIs, further illustrating an attractive pharmacokinetic profiles aiding in once daily oral delivery [69]. More specifically, letrozole, (generally utilization done in prospective studies in endometriosis correlated pain) possesses the properties of pacey absorption , longer plasma half-life, lesser plasma clearance in addition to greater volume organization [69, 70]. Metabolism, as well as excretion takes place via metabolic along with hepatic routes that are modulated by CYP3A4 as well as CYP2A6 [70].
Pertaining to the clinical effectiveness, prospective studies over restricted patient quantities have illustrated advantageous actions of AI’s over the improvement of endometriosis correlated pain symptoms [71]. Moreover, at the time of postoperative follow up, combination treatment with the utilization of AI’s with GnRH agonists for 6mths illustrated greater advantageous outcomes in contrast to GnRH agonists monotherapy for the escalating pain free time period [72]. It is further advantageous for the quick improvement of urinary and pain symptoms in case of bladder endometriosis, with improvement of intestinal symptoms in colorectal endometriosis in addition to diminished ovarian endometriotic cysts [9], Nevertheless, in view of significant inimical sequelae for instance escalated incidence of osteoporosis as well as bone fractures, AI’s utilization is presently not done pertaining to the clinical treatment of disease propagation [71]. Thereby AI’s apparently possess greater advantages in case of patients with recurrent endometriosis who did not display success with GnRH agonists, the GnRH antagonists or steroidal analogues [72]. To overcome these inimical sequelae correlated with systemic delivery, intravaginal ring liberating anastrazole were introduced in the form of alternatives, with advantages of utilization of local delivery [68, 73]. A phase 1RCT over pharmacokinetics, pharmacodynamic, safety as well as tolerability of anastrazole delivered vaginally revealed no other significant inimical sequelae or generation of ovarian cysts [74]. Nevertheless, greater clinical assessment regarding utilization of this strategy is warranted in endometriosis (Figure 9).
![Figure 10: Courtesy ref no-Structure-activity relationship of Letrozole [23].](/fulltextimages/12749/fig_10.png)
Selective Estrogen Receptors Modulators (SERM)
In view of endometriosis is believed to be an estrogen based disease, generation of hypo estrogenic situations, either with the diminishing of the circulating estrogen quantities or with the antagonistic effects over the estrogen receptors portrays one of the main mechanistic modes behind the utilization of well acknowledged medical substances. The proposal pointed that selective estrogen receptors modulators (SERM) might be a practical methodology for the treatment of pelvic pain correlated with endometriotic lesions. Binding of SERM takes place with estrogen receptor- α(ER-α), as well as estrogen- (ER-β) in the target cells working in the form of both agonists in addition to antagonists in variable tissue, that project them as distinct. Thereby they hypothesized SERMs for the treatment of endometriosis correlated pain is being assessed. For example both raloxifene as well as tamoxifen illustrate an agonistic actions in bone along with their antagonistic actionsin in breast; however just tamoxifen manifestation takes place in the form of agonistic actions in uterus [75]. The inimical sequelae felt in patients in receipt of SERM In treatment are inclusive of vasomotor symptoms (VMS), hot flushes, vaginal discharge. Intriguingly ultimate fatal inimical sequelae for instance venous thromboembolism (VTE), despite being correlated with this group of substances is occasional. SERM’s that are clinically utilized are delivered orally , possessing greater bioavailability, other than with raloxifene that goes orally via hepatic first pass metabolism along with produce conjugated glucuronides. All these SERM’s undergo hepatic metabolism with depletion in bile along with excretion taking place in faeces, with minimal quantities in urine. Taking into account these variables, an effective liver working is of considerable significance once thinking of utilization of SERM’s for treatment. Significant binding of SERM’s takes place with plasma proteins (>95%), with end depletion half live varying 27.7h-7 days [76].
Classification of SERM’s might be done into 4 groups
- The trans isomer of a triphenylethylene derivatives for instance Clomiphene Citrate (CC) along with tamoxifen, utilization is for therapy ovarian anovulation along with breast cancer with their utilization restricted in view of endometrial stimulation
- non-steroidal substances for instance - tamoxifen Raloxifene, a benzothiophene derivative
- Indoles--- for instance Bazedoxifene(BZA)
- Steroidal substances- for instance fulvestrant- portraying a pure antiestrogenic substance [75].
- Just occasional agents belonging to SERM’s group have been evaluated pertaining to the treatment of endometriosis.
- The manner stated earlier in view of endometriosis is estrogen based, SERM’s have been posited regarding treatment [77]. Nevertheless, no SERM’s have been displayed to be efficacious for the treatment of endometriosis thus far [78].
Tamoxifen-portrays the first generation SERM has been utilized in the form of adjuvant for the breast cancer. Utilization of tamoxifen in the form of alternatives for the treatment of endometriosis was anticipated, specifically for patients desiring fertility. Nevertheless, with the world- wide utilization for the treatment of breast cancer, there were reports of endometriosis generation in case of post- menopausal women who have been getting tamoxifen for the treatment of endometriosis [79]. Since these actions of tamoxifen were believed to be obtained from estrogen agonistic actions over the endometrium, Assessment of other SERM’s were done which were possessing the greater selective estrogen receptors actions.
Utilization of raloxifene has been done for the treatment of post-menopausal women in view of agonistic actions in bone osteoporotic fractures in addition to cardiovascular well-being. Nevertheless, in the uterus as well as breast it possessed an estrogen- antagonistic action [80]. The idea of utilization of raloxifene in endometriosis treatmentis raloxifene possesses advantageous action over the bone mineral density without simultaneous endometrial stimulation. In animal studies it resulted in reduction in size of the experimental endometriotic implants [81]. In a randomized clinical trial in biopsy corroborated endometriosis possessing chronic pelvic pain, in the raloxifene group significant return of chronic pelvic pain was felt in addition to statistically significant earlier secondary surgery in contrast to placebo group. Patients with pelvic pain associated with endometriosis post surgically got randomly divided into raloxifene in addition to placebo group for 6 months. The dosages employed were considerably greater in view of availability of safety outcomes , however Stratton et al. [82], presumed that continued greater dosages utilization have resulted in stimulation actions over the endometriotic implants, which were not anticipated.
Thereby the conclusions drawn were raloxifene statistically significantly diminished the time for returning of chronic pelvic pain in view of which the Data Safety monitoring Committee terminated the study early [82]. Bazedoxifene(BZA), portraying a 3rd generation SERM possesses great safety profiles, utilization for osteoporosis treatment and avoidance of post-menopausal fractures. It effectively antagonizes estrogen induced uterine endometrial stimulation without countering estrogenic effects in bone or the CNS. In a rat model BZA alone diminished the size of endometriosis lesions, with experimental evidence of anti-proliferative actions [83]. Additionally, BZA was demonstrated to diminish proliferating cell nuclear antigen (PCNA) in addition to estrogen receptor expression in the endometrium of animals treated in contrast to controls. Nevertheless, the efficacy of BZA in humans has not been assessed in endometriosis treatment.
SR16234 portrays the maximum current SERM which possesses antagonistic effect over ER-α as well as part agonistic effect over ER-β. The outcomes obtained from the clinical trial in 2018 pointed that SR16234 might be possessing the capacity of ameliorating pelvic pain associated with endometriosis at the 40mg dosage by oral delivery. Since no other SERM have illustrated clinical effectiveness in endometriosis, portrays in the form of the first SERM possessing revealed efficacy in this arena. No clarification is existent apparently regarding mechanistic modes over SR16234 in endometriosis. In contrast to tamoxifen/ raloxifene, SR16234 apparently is a purer ER-α antagonist which might be one of the explaination for its efficacy in pain associated with endometriosis. The reasons being its robust affinity ER-α as well as ER-β might be of utmost significance [56]. Great larger scale in addition to placebo controlled clinical trials in are mandatory to validate this posit. Continued attempts are getting for finding the ‘’optimal SERM’’ in the form of an alternative to the other for relieving pain associated with endometriosis (Figure 11).
![Figure 11: Courtesy ref no-Structure-activity relationship of Bazedoxifene [23].](/fulltextimages/12749/fig_11.png)
Selective Progesterone Receptors Modulators (SPRM)
Selective progesterone receptors modulators (SPRM’s) represent a class of synthetic ligands possessing variation of actions (agonist, antagonist, mixed) over the progesterone receptors from variable targeted tissues. They have been displayed to be efficacious over variety of hormone based situations for instance uterine fibroids, endometriosis, breast cancer as well as endometrial cancer. In view of it possessing lesser actions over ethinyl estradiol (E2) in addition to androgens quantities SPRM’s treatment is not associated with hypoestrogenic inimical sequelae [84]. One further benefit with SPRM’s is its delivery is feasible by oral as well as vaginal routes. They prevent the hypoestrogenic inimical sequelae associated with other treatment in view of sustenance of mid follicular plasma estrogenic quantities. Since remarkably large percentage of chronic gynecologic disorders get impacted hormonally, SPRM’s might display considerable treatment probability in the absence of the inimical sequelae of the present pharmacologic treatment modalities.
Of the probable theoretical restrictions of daily SPRM’s use might be endometrial estrogen exposure which does not get opposed. As per the endometrial morphology subsequent to SPRM’s utilization, studies have isolated endometrial morphological alterations in view of anti-progestin actions [85]. These endometrial morphological alterations alias progesterone receptors modulators associated endometrial change(PAEC) which portray a spectrum of endometrial pathology designs having the characteristic histology of cystically dilated glands, inactive epithelium along with occasional mitotic figures in a frame work of tightly packed non decidualized stroma [86]. Nevertheless, apart from these, endometrial changes get reverted subsequent to culmination of these agents, however apparently they do not display cytological atypia [87]. Despite PAEC has been believed to be leading to improvement of benign endometrial changes, their assessment is essential for acceptability of their complete safety of SPRM’s [88].
The initial SPRM was invented was RU486 (mifepristone), that possesses progesterone agonistic as well as antagonistic actions. In a phase II/III trial effectiveness was found regarding symptomatic, however inimical sequelae were observed in a significant proportion of patients. Mifepristone delivery (50mg x6mths) patients with endometriosis have been illustrated to possesses significant actions over the symptoms [89]. A Cochrane systematic review encompassing 10 RCT’s implicating 960 patients pointed that mifepristone leads to improvement of endometriosis correlated dysmenorrhea in addition to probably dyspareunia. Amenorrhea as well as hot flushes have been revealed to be inimical sequelae, Despite no menstrual cycle might be advantageous in patients with heavy menstrual bleeding. Nevertheless, no concrete conclusions could be made regarding dosages on accessibility of outcomes [90].
Asoprisnil (J867or As) is a 11β benzaldoxime substituted steroidal SPRM that has illustrated mixed progesterone agonistic as well as antagonistic actions in both animal models in addition to clinical trials performed in women [91]. In case of randomized placebo controlled trial, As(5,10,25mg )was delivered x 12wks to women having laparoscopically corroborated endometriosis along with gave history of moderate to robust pain. Significantly diminished non menstrual pains in addition to dysmenorrhea were observed in contrast to placebo [92]. Cessation of clinical generation was done in 2007 in view of aberrant endometrial alterations in patients [93]. Akin to mifepristone, ulipristal acetate (UPA) was called ‘’antiprogestin’’ once it was generated, with just in recent years they have been named as SPRM’s [94]. It represents a steroid agent that has been approved for emergency contraception in addition to preoperative treatment for symptomatic leiomyomas.
In 2018 the European Medical Agency (EMA) gave a warning regarding a robust risk of liver damage from UPA along with advocated ways for minimizing these inimical sequelae. This agent is contraindicated in women having liver disease, therefore assessment of liver function is essential prior to, at the time of as well as subsequent delivery of agent; recurrent therapies might be offered just to women not fit candidates regarding surgery in addition to patients need to be completely informed regarding risks. Greater studies are required for the clarification of mechanistic modes of hepatotoxicity of UPA along with corroborate that these prophylactic approaches are efficacious. Nevertheless, in the form of an agent implicated in drug induced liver injury (DILI) has not been completely validated [95]. Present information pointed that UPA might be implicated in the idiosyncratic (instead of intrinsic) DILI in addition to continued monitoring regarding minimizing risk of UPA use [96]. Present EMA Guidelines advocated utilization of UPA just as 2nd line treatment of uterine fibroids in premenopausal women, where surgery is not proper or has not been efficacious [95]. In a systematic review conducted by De Manno O, et al. [91], encompassing 10 studies implicating 1450 patients where assessment of consumption of UPA of actions over endometrium was studied. It validated the present belief regarding insight of PAEC’s as well as revealed that it is necessarily a benign disorder reverting on culmination of use. Nevertheless, maximum have restricted follow up have along with have utilized UPA in upto 4intermittent cycles, thus further assessment is prior to concluding its safety over long term utilization [91]. Till date as no RCT’s have been obtained regarding its use for gynecological comorbidities like adenomyosis as well as endometriosis.
There is controversial as well as restricted validation on UPA part in endometriosis treatment. In case of animal studies (In a rat model where endometriosis was induced) UPA induced reduction in size along with atrophy of the experimental endometriotic implants. This was correlated with up regulation of pro apoptotic markers, diminished cell proliferation in addition to proinflammatory markers [97]. Bressler, et al. [98], reported a case report, where significant diminishing of endometriosis correlated refractory chronic pelvic pain occurred on treatment with15mg UPA used for 3mths [98] in contrast to this case report, Donnez J, et al. [99], displayed a wonderful reaction to UPA treatment once delivered as 2 -3mths courses for reduction in size of uterine fibroids [99]. Greater studies are required as well fashioned RCT.
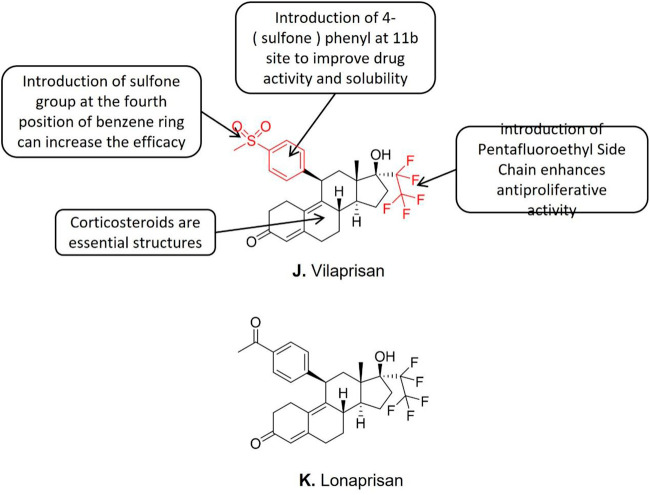
Vilaprisan (BAY1002670), represents a newer, robust orally active SPRM. Its antagonistic actions are 5 in addition to 10 fold greater in contrast to UPA as well as Mifepristone respectively [100]. Vilaprisan has been going through clinical trials for myriad of indications; however for endometriosis correlated pain it got prematurely terminated. Despite illustrating advantageous actions for the treatment of uterine fibroids in addition to for heavy menstrual bleeding, its greater robustness makes it being improbable for it to assume a greater advantageous role for endometriosis treatment [101].
Conclusions drawn are despite certain studies performed with SPRM have illustrated probability of clinical utility for relieving symptoms [102]. None of agents from this class has presently received approval for clinical utility for endometriosis. Despite mifepristone might be possessing certain advantages, the present corroboration does not point regarding therapeutic utility in addition to clinical safety of other SPRM’s regarding long term treatment of endometriosis (Figure 12).
Levonorgestrel Releasing Intra Uterine System(LNG-IUS) /Device
The levonorgestrel releasing intra uterine system(LNG-IUS) was introduced to start with, with the idea of contraception 50yrs back; nevertheless, LNG-IUS demonstrates certain advantages regarding therapies for chronic benign gynecologic disorders, inclusive of abnormal uterine bleeding (AUB) [which is followed by anaemia], endometrial hyperplasia, endometriosis, adenomyosis, uterine fibroids as well as coagulation abnormalities [103, 104, 105], The, levonorgestrel having (molecular structural formula ofC21H28O2) portrays an estrane steroid obtained from 19 nor testosterone-portraying a 2nd generation progestin [103]. Besides contraception action LNG-IUS results in endometrial decidualization, thereby diminishing quantities of menstrual output [104]. Other mechanistic modes influencing endometriosis correlated pain by complete reduced prostaglandin generation, basically impacted by progestins in addition to down regulation of estrogen receptors in glandular along with stromal tissues both [105, 106]. The pharmacokinetic advantages of LNG-IUS were emphasized in the earlier publications with the guidelines given by the European Society of Human Reproduction and Embryology (ESHRE) saying that clinical practitioners might take into account these LNG-IUS in the form of one of the strategies regarding ameliorating endometriosis correlated pain [107]. LNG-IUS illustrated an advantageous action in escalating pain free time period subsequent to surgery in contrast to expectant treatment [108]. Zhu SY, et al. [105], performed a prospective study where they illustrated advantageous outcomes regarding avoidance of recurrence, subsequent to endometrioma surgery where a combination of LNG-IUS with GnRH agonist got used [105]. Longitudinal studies observed significant diminishing of robustness of dysmenorrhea subsequent to 3mths follow up [109]. Nevertheless, irregular bleeding which is not tolerated at the time of first yr of use in addition to continued pain justify the cessation of treatment leading to plausible disadvantages regarding clinical decision making [104]. Moreover, this type of strategy is believed to be a 2nd line method as well as in certain countries believed to be off label therapy regarding this indication [107]. Conclusions regarding LNG-IUS use are it needs to be taken into account in patients possessing robust hypoestrogenic inimical sequelae from 1st line substances used in symptomatic endometriosis.
Noncanonical Treatment options
Plethora of studies have illustrated the advantageous actions of green tea on human health. The maximum current studies have illustrated that constituents which are of advantage in green tea is polyphenol epigallocatechin gallate(EGCG)whose action is avoidance of oxidative stress(OS), diminishing inflammation , in addition to angiogenesis, illustrating its probability of clinical utility in endometriosis treatment. EGCG binding takes place competitively with estrogen receptors in endometrial cells, where it has a hampering action resulting in avoidance of growth of endometriotic implants [110]. Nevertheless, greater comprehensive research with inclusion of, enrollment of patients having endometriosis is the requirement to corroborate if green tea actions are of advantage to justify its plausible utility for endometriosis in the form of a therapeutic substance.
Curcumin portrays a significant anti-inflammatory substance, has been illustrated to possess advantageous actions in the patients having endometriosis. It possesses the capacity of down regulating inflammation by diminishing the actions of nuclear factor κB (NFκB) pathway in the endometrial cells in addition to hampering the expression of inflammatory factors for instance tumor necrosis factor alpha (TNFα), interleukin-1 (IL-1), IL-6, as well as IL-8. Furthermore, it might directly influence adhesions, apoptosis in addition to angiogenesis, in endometriotic implants [111]. Its probability utility in form of dietary therapy for endometriosis needs further assessment.
Patient’s Journey-from Non-Steroidal Anti Inflammatory Drugs ( NSAIDS) to Surgery
Idealization of the medical treatment regarding endometriosis holds big clinical hurdles. The goals of endometriosis treatment are inclusive of attaining long term results in reference to attenuation of pain as well as recurrence rates apart from improvement of QOL [112]. Acknowledged the complicated nature of the etiopathogenesis of endometriosis utilization of combination of strategies is usually imperative for proper treatment of the disease. Initiation of the treatment utilization of hormonal’ therapy along with non-hormonal’ therapy as described earlier regarding pain amelioration as well as restriction of propagation of endometriotic implants. Utilization of NSAIDS regulating inflammation along with hormonal’ for avoidance of proliferation of endometrial cells continues to be the mainstay therapeutic strategy for this gynecologic disorder. Despite the maximum dosages of the NSAIDS that are tolerable by patients gets usually utilized for the abrogation of pain in the endometriosis therapy. Long term utilization is not advocated in view of inimical sequelae [29]. Surgical excision of endometriotic implants as well as adhesions is usually advantageous along with corroborates Histopathological diagnosis in patients not responsive to medical treatment or possessing robust symptoms [113]. As far as choice of variable hormonal’ therapies needs to be individualized strategy subsequent to appropriate evaluation of risks versus advantages regarding decision making of the course of treatment. Surgical assessment of patients desiring conception in addition to treatment is further advocated, despite there being no agreement regarding surgical treatment in reference to infertility [112]. Plenty of attractive comprehensive research is being performed in reference to biomedical targets with concentration over cellular in addition to molecular mechanistic modes leading to endometriosis. This causes an earnest advantageous action over a patient’s diagnosis along with.
Conclusion
Despite considerable improvement of hormonal’ therapy along with non-hormonal’ therapy strategies, the maximum presently accessible therapy strategies for the treatment of endometriosis result in repression of ovarian working as well as do not portray the ultimate answer for the patients. Present management of endometriosis is inclusive of pharmacologic in addition to surgical interventions along with need tailoring appropriately in appropriate time with the initial aim of relieving pain in addition to restoration of fertility. Correct choice of treatment is made in reference to patients’ age, robustness of disease, wanting preservation of fertility. Dependent over the corroboration by publications clinical practitioners need to take into account NSAIDS.COC’s in addition to progestins in the form of first line medical treatment in contrast to 2nd line strategies for instance GnRH agonists/ GnRH antagonists/Ais, these first line substance detailed above, possess greater tolerability as well as are economical. To our misfortune around 20% of patients displayed no relieving of pain with medical treatment whereas other 5-15% of patients culminated in view of usual significant hypoestrogenic inimical sequelae. Taking into account all these issues further research needs to be having isolation of targeted therapies, both hormonal’ therapy along with non- hormonal’ as well as accessible therapies need assessment for variable modes of delivery to assess if lesser inimical sequelae result [114]. For example certain pharmacologic strategies like GnRH agonists, GnRH antagonists or Ais acknowledged for being correlated with significant inimical sequelae, might be delivered by utilization of vaginal routes with probability of lesser inimical sequelae in view of greater stabilization of steady state liberation of agents. Furthermore innovative non-hormonal’ strategies need to be having a goal of evaluating the regulation of endometriosisis in patient wanting fertility. Actually, hormonal’ therapies in the form of first line treatment or for avoidance of recurrent disease subsequent to surgery work as contraceptives which is the biggest restriction of this kind of therapies. Dependent over this, key preferences are isolation of new noncontraceptive in addition to non-hormonal’ approaches for diminishing propagation of endometriosisis, thus chances of pregnancy getting feasible. Recently Othman ER, et al. [115], reviewed how oral GnRH antagonists, inclusive of elagolix, relugolix, as well as linzagolix aid in oral delivery, stimulate dose based diminishing of estradiol quantities, do not result in flare up of endometriosis symptoms to start with, in addition to aid in pacey recovery of ovarian working along with menstruation subsequent to its cessation. Elagolix at a low dosage of 150 mg/day, or the greater dosage of 200 mg twice/day, significantly escalated the percentage of women attaining clinically meaningful diminishing of dysmenorrhea, noncyclic pelvic pain, as well as dyspareunia. Relugolix at an oral dosage of 40 mg daily caused improvement in variable kinds of endometriosis correlated pelvic pain, with an effectiveness in addition to inimical sequelae profile akin to that of GnRH agonists. Adding 1 mg of estradiol along with 0.5 mg of Norethindrone to 40 mg of relugolix (relugolix combination therapy) aids in treatment upto 24 weeks with sustained efficacy as well as an improved inimical sequelae profile. Linzagolix, in a dosage of 75 mg daily, might be utilized alone for treating endometriosis correlated pain. For pelvic pain in addition to dyspareunia, linzagolix might be utilized in a greater dosage of 200 mg daily with hormonal add- back therapy for conservation of bone health. Furthermore as reviewed by us earlier in role of sclerosing therapy in inoperable recurrent endometrioma who presented to us with severe incapacitating pain transvaginally might be used where nothing else works in rare cases who had numerous surgeries as well as for patients desiring fertility now it has come to reverting to surgery in experienced hands in centres only specialized for endometriosis surgeries which would avoid such inimical sequelae of adhesions in hands of inexperienced surgeons causing diminished ovarian reserve (DOR).
References
-
Giudice LC, Kao LC (2004) Endometriosis. Lancet 364(9447): 1789-1799.
-
Chapron C, Marcellin L, BorgheseB, Santulli P (2019) Rethinking Mechanisms, Diagnosis and Management of Endometriosis. Nat Rev Endocrinol 15(11): 666-82.
-
Mehedintu C, Plotogea MN, Ionescu S, Antonovici M (2014) Endometriosis Still a Challenge. J Med Life 7(3): 349-357.
-
Skebro B, Bjedov S, Mikus M, MustacF, Lesin J, et al. (2021) Endometriosis, Pain and Mental Health. Psychiatr Danub 33(Suppl 4): 632-636.
-
Greene AD, Lang SA, Kendzioski JA, Rios JMS, Herzog TJ, et al. (2016) Endometriosis: Where are We and Where are we going? Reproduction 152(3): R63-R78.
-
Coric M, Barisic P, Pavicic D, Karadza M, Banoic M (2011) Electrocoagulation Versus Sutures after Laparoscopic Stripping of Ovarian Endometrioma Asssessed by Antral Follicle Count: Preliminary Results of Arandomized Clinical Trial. Arch Gynaecol Obstet 283(2): 373-378.
-
Leonardi M, Gibbons T, Armour M, Wang R, Glanville, et al. (2020) When to do Surgery and When not to do Surgery for Endometriosis: A Systematic Review and Meta-Analysis. J Minim Invasive Gynaecol 27(2): 390- 407.
-
Singh SS, Gude K, Perdeaux E, Gattrell WT, Becker CM (2020) Surgical Outcomes in Patients with Endometriosis: A Systematic Review. J Obstet Gynaecol Can 42(7): 881-888.
-
Ferrero S, Evangelisti G, Barra F (2018) Current and Emerging Treatment Options for Endometriosis. Expert Opin Pharmacother 19(10): 1109-1125.
-
Kaur KK, Allahbadia GN, Singh M (2012) Comparison of Statins Prospectively to Oral GnRH Antagonists vs Caberline in Mild to Moderate Endometriosis Poster presented in 16th COGI Congress held in Singapore.
-
Kaur KK, Allahbadia G, Singh M (2012) Kisspeptins in Human Reproduction-Future Therapeutic Potentials. J Assist Reprod Genet 29(10): 999-1011.
-
Kaur KK, Allahbadia GN (2015) Medical Management of Leiomyomas-Emphasis for Different Geographical Regions. Journal of Gynecology and Neonatal Biology 1: 1-8.
-
Kaur KK, Allahbadia GN (2016) An Update on Pathophysiology and Medical Management of Endometriosis. Advances in Reproductive Sciences 4(2): 53-73.
-
Kaur KK, Allahbadia GN, Singh M (2017) Current Controversies and Future Directions in Endometriosis Therapy. EC Gynaecology Editors Column 1: 9-13.
-
Kaur KK (2017) Meeting the Challenges of Endometriosis Associated Pain-Newer Options for Future and Research Directions. BAOJ Bioinfo 1: 09.
-
Kaur KK (2018) Spontaneous Conception in a Case of Adenomyosis with Submucus Fibroid Following Treatment with Mifepristone in a 38 year Old Lady with 10year Secondary Infertility. J Hum Bio & Health Edu 2: 14.
-
Kaur KK, Allahbadia GN, Singh M (2019) An Update on Diagnosis and Management of Adolescent Endometriosis - A Short Communication. Acta Scientific Paediatrics 22(5): 48-50.
-
Kaur KK, Allahbadia GN, Singh M (2019) Dissecting the Reduced Ovarian Reserve Seen with Ovarian Enometriomas with That Caused by Surgical Excision of Ovarian Enometriomas-What Comes First. Surgical Medicine Open Access Journal 2(3).
-
Kaur KK, Allahbadia GN, Singh M (2020) Dilemna Regarding Preference of Surgery or Medical Treatment in Case of Tubal Blockade, Endometriosis or Adenomyosis and Pelvic Adhesion Prevention once Surgery is Contemplated - A Systematic Review. Surg Med Open Acc J.
-
Kaur KK, Allahbadia GN, Singh M (2021) Medical Treatment in Uterine Adenomyosis Management - A Systematic Review. Archives of Clinical Case Studies and Case Reports 2: 189-198.
-
Kaur KK, Allahbadia GN, Singh M (2020) Management of Inoperable Recurrent Endometrioma Presenting as Severe Incapacitating Pain Following Leuprolide Acetate Depot by Aspiration, Recurring Again a 2 Yrs Subsequently for Sclerosing Therapy at Present: A Case Report. SunText Rev Case Rep Image 1: 107.
-
Kaur KK, Allahbadia GN, Singh M (2023) A Prototypical Shift back to the Original Role of Surgery for Endometriosis in Specialized Centres in Experienced Hands - A Short Communication. Womens Health Sci J 7(2): 1-6.
-
Shi J, Tan X, Feng G, Zhuo Y, Jiang ZL, et al. (2023) Recent Advances in Drug Therapy of Endometriosis. Front Pharmacol 14: 1199010.
-
Bindu S, Majumdar S, Bandopadhyay U (2020) Non- Steroidal Anti-Inflammatory Drugs and Organ Damage. Biochem Pharmacol 180: 114147.
-
Lees P, Giraudel J, Landoni MF, Toutain PL (2004) PK- PD Integration and PK-PD Modelling of Nonsteroidal Anti-Inflammatory Drugs: Principles and Applicationsin Pharmacology. J Vet Pharmacol Ther 27(6): 491-502.
-
Wyatt JE, Pettit WL, Harirforoosh S (2012) Pharmacogenetics of Non-Steroidal Anti-Inflammatory Drugs. Pharmacogenomics J 12(6): 462-467.
-
Allen C, Hopewell S, Prentice A (2017) Non-Steroidal Anti-Inflammatory Drugs for Pain in Women with Endometriosis. Cochrane Database Syst Rev 4: CD0004753.
-
Kauppilla A, Ronnberg L (1985) Naproxen Sodium in Dysmenorrhea Secondary to Endometriosis. Obstet Gynaecol 65(3): 379-383.
-
Arfe A, Scotti L, Lorenzo CV, Nicotra F, Zambon A, et al. (2016) Non-Steroidal Anti-Inflammatory Drugs and Risk of Heart Failure (HF) in four European Countries: Nested Case - Control Study. BMC 354: i4857.
-
Kleinknecht D (1995) Interstitial nephritis, Nephropathy syndrome and chronic renal failure secondary to Nonsteroidal anti-inflam¬matory drugs. Seminal Nephrol 15(3): 228-235.
-
Goldzieher JW, Stanczyk FZ (2008) Oral contraceptives and individual variability in circulating levels of ethinyl estradiol and progestins. Contraception 78(1): 4-9.
-
Simmons KB, Edelman AB (2016) Hormonal Contraception and obesity. Fertil Steril 106(6): 1282- 1288.
-
Edelman AB, Cherala G, Stanczyk FZ (2010) Metabolism and Pharmacokinetics of contraceptives steroids in obese women : a review. Contraception 82: 314-322.
-
Simmons KB, Haddard LB, Nanda K, Curtis KM (2018) Drug interactions between non rifamycin antibiotics and hormonal Contraception: a systematic review. Am J Obstet Gynaecol 218(1): 88-97.
-
Barbara G, Buggio L, FacchinF, Vercellini P (2021) Medical treatment of endometriosis: tolerability; quality of life and adherence. Front Glob Womens Health 2: 729601.
-
Vercellini P, Trespidi L, Colombo A, Vendola N, Marchini M, et al. (1993) Gonadotropin releasing hormone agonist versus a low dose Oral contraceptives for pelvic pain associated with Endometriosis. Fertil Steril 60(1): 75-79.
-
Maggiore ULR, Remorgida V, Scala C, Tafi E, Venturini PL, et al. (2014) Desogestrel only contraceptive pill versus Sequential contraceptive vaginal ring for the treatment of rectovaginal endometriosis infiltrating the rectum:a prospective open labelcomparative study. Acta Obstet Gynaecol Scand 93(3): 239-247.
-
Vercellini P, Barbara G, Somigliana E, Bianchi S, Abbiati A, et al. (2010) Comparison of contraceptives ring and patch for the treatment of endometriosis. Fertil Steril 93(7): 2150-2161.
-
Mikus M, Goldstagn MS, Lagana AS, Vukorepa F, Coric M, et al. Clinical efficacy, Pharmacokinetics and safety of theavailable medical options in the treatment of endometriosis-related pain: a scoping review. Pharmaceuticals 2023; 16(9): 1315.
-
Bizzarri N, Remorgida V, Maggiore ULR, Scala C, Tafi E, et al. (2014) Dienogest in the patients treatment of rectovaginal endometriosis. Expert Opin Pharmacother 15: 1889-1902.
-
Vercellini P, Somigliana E, Consonni D, Frattaruolo MP, De Giorgio O, et al. (2012) Surgical versus medical treatment for endometriosis-associated severe deepdyspareunia: I. effect on pain during intercourse and patient satisfaction. Hum Reprod 27(12): 3450-3459.
-
Bick A, Louw du Toit R, Skosana SB, Africander D, Hapgood JP (2021) Pharmacokinetics, metabolism and serum concentration of progestins used in contraception. Pharmacol Ther 222: 107789.
-
Konings G, Brentjens L, Delvoux B, Linnanen T, Cornel K, et al. (2018) Intracrine regulation of estrogen and sex steroid levels in endometrium and non gynaecologic tissues; pathology, physiology and Drug discovery. Front Pharmacol 9: 940.
-
Brown J, Kives S, Akhtar M (2012) Progestagens and anti progestagens for pain associated with Endometriosis. Cochrane Database Syst Rev 2012(3): CD002122.
-
Ambacher K, Secter M, Sanders AP (2022) The use of progestin subdermal implants in the management of endometriosis-related pain symptoms and quality of life: a systematic review. Curr Med Res Opin 38(3): 479-486.
-
Angioni S, Nappi L, Pontis A, Sedda F, Luisi S, et al. (2015) Dienogest: A Possibile conservative approach in bladder endometriosis: results of a pilot study. Gynaecol Endocrinol 31(5): 406-408.
-
De Paula Andres M, Lopes LA, Baracat EC, Podgaec S (2015) Dienogest. in the treatment of endometriosis: systematic review. Arch Gynaecol Obstet 292(3): 523- 529.
-
Barra F, Scala C, Ferrero S (2018) Current understanding on Pharmacokinetics, Clinical efficacy and safety of progestins for treating pain associated with Endometriosis. Expert Opin DrugMetab Toxicol 14(4): 399-415.
-
Tarlatzis BC, Kolibiankis EM (2007) GnRH agonists vs GnRH antagonists. Best Pract Res Clin Obstet Gynaecol 21: 57-68.
-
Tzoupis H, Nteli A, Androustou ME, Tselios T (2020) Gonadotropin releasing hormone and GnRH receptor: structure, functionand drug development. Curr Med Chem 27(36): 6136-6148.
-
Wilson AC, Meethal SV, Bowen RL, Atwood CS (2007) Leuprolide Acetate: a drug of diverse clinical applications. Expert Opin Investig Drug 16(11): 1851-1863.
-
Teutonico D, Montanari S, Ponchel G (2012) Leuprolide Acetate: Pharmaceutical use and delivery potentials. Expert Opin Drug Deliv 9(3): 343-354.
-
Shore ND, Guerrero S, Sanahuja RM, Gambus G, Parente A (2019) A new sustained release3 month Leuprolide Acetate formulation achieves and maintains castrate concentrations of testosterone in patients with prostate Cancer. Clin Ther 41(3): 412-425.
-
Brown J, Pan A, Hart RJ (2010) Gonadotropin- releasing hormone analogues for pain associated with endometriosis. Cochrane Database Syst Rev 2010(1): CD008475.
-
Fedelle L. Bianchi S, Bocciolone L, Di Nola G, Fanchi D (1993) Buserelin Acetate in the treatment of pelvic pain associated with minimal and mild endometriosis: a controlled study. Fertil Steril 59(3): 516-521.
-
Harada T, Momoeda M, Taketani Y, Aso T, Fukunaga M, et al. (2009) Dienogest is as effective as intranasal Buserelin Acetate for the relief of pain symptoms associated with endometriosis-a randomized, double blinded , multicenter , controlled trial. Fertil Steril 91(3): 675-681.
-
Strowitzki T, FaustmannT, Gellinger C, Seitz C (2010) Dienogest in the treatment of endometriosis–associated pelvic pain: a 12wk randomized, double blind placebo controlled study. Eur J Obstet Gynecol Repprod Biol 151(2): 193-198.
-
Aggarwal SK, Hamrang C, Henzl MR, Judd HL (1997) Nafarelin vs Leuprolide Acetate Depot for endometriosis. Changes in Bone mineral density and Vasomotor Symptoms. Nafarelin study group. J Reprod Dev 42(7): 413-423.
-
Zheng O, Mao H, Xu Y, Zhao J, Wei X, et al. (2016) Can postoperative GnRH agonist treatment prevent endometriosis recurrence? a meta-analysis. Arch Gynaecol Obstet 294: 201-207.
-
Huirne JAF, Lambalk CB (2001) Gonadotropin releasing hormone antagonists. Lancet 358(9295): 1793-1803.
-
Barra F, Scala C, Della Corte L, Giampaolino F, Ferrero S (2019) Relugolix for the treatment of uterine fibroids. Drug Today 55: 503-512.
-
Tan O, Bukulmez O (2011) Biochemistry, molecular biology, and cell biology of Gonadotropin releasing hormone antagonists. Curr Opin Obstet Gynaecol 23: 238-244.
-
Donnez J, Taylor HS, Taylor RN, Akin MD, Tatarchuk TF, et al. (2020) Treatment of endometriosis associated pain with linzagolix, an oral Gonadotropin releasing hormone antagonist: a randomized, clinical trial. Fertil Steril 114(1): 44-55.
-
Diamond MP, Carr B, Dmowski WP, Koltun W, O’Brien C, Jiang P, et al. (2014) Elagolix treatment for endometriosis associated pain: results from a phase 2 randomized, double blind, placebo controlled study. Reprod Sci 21(3): 363-371.
-
Taylor HS, Guidice C, Lessey BA, Abrao MS, Kotanki Z, et al. (2012) Treatment of endometriosis associated pain with elagolix or oral GnRH antagonist. N Engl J Med 322: 28-40.
-
Guidice C, As SanIes, Arjona Ferreira JC, Becker CM, Abrao MS, et al. (2022) Once daily oral Relugolix combination therapy versus placebo in patients with endometriosis associated pain; two replicate phase 3 randomized double blind studies(spirit 1 and2). Lancet 399: 2267- 2279.
-
Yamamoti T, Noguchi T, Tamura T, Kitawaki J, Okada H (1993) Evidence for estrogen synthesis in adenomyotic tissues. Am J Obstet Gynaecol 169: 734-738.
-
Garzon S, Lagana AS, Barra F, Casarin J, Cromi A, et al. (2021) Novel Drug delivery methods for improving efficacy of endometriosis treatments. Expert Opin Drug Deliv 18(3): 355-367.
-
Lenning P, Pfister C, Martoni A, Zamagni C (2003) Pharmacokinetics of 3rd generation Aromatase Inhibitors. Seminal Oncol 30: 23-32.
-
Lenning P (2003) Clinical Pharmacokinetics of Aromatase Inhibitors and in activators. ClinPharmacokinet 42: 619- 631.
-
Ferrero S, Venturini PL, Gillott DJ, Remorgida V (2011) Letrozole and Norethindrone acetate versus Letrozole and triptorelin in the treatment of endometriosis related pain symptoms: arandomized, controlled trial. Reprod Biol Endocrinol 9: 88.
-
Soysal A, Soysal ME, Ozer S, Gul N, Gezgin T (2004) The effects of Post-surgical administration of goserelin plus anastrazole compared to goserelin alone in patients with endometriosis: a prospective randomized controlled trial. Hum Reprod 19(1): 160-167.
-
Garzon S, Lagana AS, Barra F, Casarin J, Cromi A, et al. (2020) Aromatase Inhibitors for the treatment of endometriosis: a systematic review about efficacy, safety and early clinical development. Expert Opin Investig Drug 29(12): 1377-1388.
-
Schultze-Mosgau M-H, Waellnitz K, Nave R, Klein S, Kraetschmar R, Rautenberg T, et al. (2016) Pharmacokinetics, Pharmacodynamic safety and tolerability of an intravaginal ring releasing anastrazole and Levonorgestrel in healthy post-menopausal women: a phase 1 randomized, controlled trial. Hum Reprod 31: 1713-1722.
-
Dutere M, Smith CL (2000) Molecular mechanisms of Selective estrogen receptors modulators (SERM) actions. J Pharmacol Exp Ther 295(2): 431-437.
-
Morello KC, Wurz GT, De Gregorio MW (2003) Pharmacokinetics of Selective estrogen receptors modulators. Clin Pharmacokinet 42(4): 361-372.
-
Simsa P, Mihalyi A, Kyama CM, Mwenda JM, Fulop V, et al. (2007) Selective estrogen receptors modulators and Aromatase Inhibitors: promising new medical therapies for endometriosis?. Womens Health(Lond) 3(5): 617- 628.
-
Bedawy MA, Alfaraj S, Yong P, Casper R (2017) New developments in the medical treatment of endometriosis. Fertil Steril 107(3): 555-565.
-
Le Bouedec G, Kaufmann P, Pingeon JM, de Latour M, Lemesle P, et al. (1991) Post-menopausal endometriosis developed during tamoxifen treatment. Rev Fr Gynecol Obstet 86(5): 407-410.
-
Nath A, Sitruk-Ware R (2009) Pharmacology and Clinical application of Selective estrogen receptors modulators. Climacteric 12(3): 188-205.
-
Altintas D, Kocku A, Kademir B, Tosun M, Cetinkaya MB (2010) Comparison of the effects raloxifene and anastrazoleon experimental endometriosis. Eur J Obstet Gynecol Reprod Bio 150(1): 84-87.
-
Stratton P, Sinail N, Segars J, Kozlol D, Zimmer C, et al. (2008) Return of chronic pelvic pain from endometriosis after raloxifene treatment: a randomized controlled trial. Obstet Gynecol 111(1): 88-96.
-
Kulak J Jr, Fischer C, Komm B, Taylor HS (2011) Treatment with bazedoxifene, a selective estrogen receptor modulator, causes regression of endometriosis in a mouse model. Endocrinology 152(8): 3226-3232.
-
Lusher SJ, Raaijmakers HCA, Vu-Pham D, Decheing K, Lam TW, et al. (2011) Structural basis for agonism and antagonism for chemically related Selective Progesterone Receptor Modulators. JBiol Chem 286(40): 35079-35086.
-
Mutter GL, Bergeron C, Deligdisch L, Frenczy A, Glant M, et al. (2008) The spectrum of endometrial pathology induced by Progesterone Receptor Modulators. MolPathol 21(5): 591-598.
-
Williams ARW, Bergeron C, Barlow DJ, Frenczy A (2012) Endometrial morphology after treatment of uterine fibroids with the Selective Progesterone Receptor Modulator, ulipristal acetate. Int J Gynaecol Pathol 31(6): 566-569.
-
Whitaker LHR, Murray AA, Mathews R, Shaw G, Williams ARW, et al. (2017) Selective Progesterone Receptor Modulator (SPRM), ulipristal acetate (UPA) and its effects on human endometrium. Hum Reprod 32(3): 531-543.
-
De Milliano I, Van Hattum D, Ket JCF, Huirne JAF, Hehenkamp JAF (2017) Endometrial changes during ulipristal acetate use: DeMilliannoI, a systematic review. Eur J Obstet Gynaecol Reprod Biol 214: 56-64.
-
Kettel LM, Murphy AA, Morales AJ, Yen SS (1998) Preliminary report on the Treatment of endometriosis with the low dose mifepristone (RU486). Am J Obstet Gynecol 178(6): 1151-1156.
-
Fu J, Song H, Zhou M, Zhu H, Wang Y, et al. (2017) Progesterone Receptor Modulators for endometriosis. Cochrane Database Syst Rev 2017(7): CD00981.
-
De Manno D, Elger W, Garg R, Lee R, Schneider B, et al. (2003) Asoprisni (J867): a Selective progesterone receptor modulator for gynaecologic therapy. Steroids 68(10-12): 1019-1032.
-
Chwalisz K, Perez MC, Demanno D, Winkel C, Schubert G, et al. (2005) Selective progesterone receptor modulator in the treatment of leiomyomata and endometriosis. Endocr Rev 26(3): 423-438.
-
Willaims ARW, Critchley HOD, Osei J, Ingamelis S, Cameron IT, et al. (2007) The effects of the Selective progesterone receptor modulator asoprisnil on the morphology of the uterine tissues after 3mths Treatment in patients with symptomatic Leiomyomas. Hum Reprod 22(6): 1696-1704.
-
Critchley HOD, Chodankar RR (2020) 90 years of Progesterone: Selective progesterone receptor modulators in gynaecologic therapies. J Mol Endocrinol 65(1): T15-T33.
-
Middelkoop MA, Bet PM, Drenth JPH, Huirne JAF, Hehenkamp WJK (2021) Risk efficacy balance ulipristal acetate compared to surgical alternatives. Br J Clin Pharmacol 87(7): 2685-2697.
-
Donnez J (2018) Liver injury and ulipristal acetate: an overstated tragedy? Fertil Steril 110(4): 593-595.
-
Huniadi CA, Pop OL, Antal TA, Stamatian F (2013) The effect of ulipristal on Bax/Bcl2, cytochrome c, Ki- 67and cyclooxygenese2 expression in a rat model with surgically induced endometriosis. Eur J Obstet Gynecol Reprod Biol 169(2): 360-365.
-
Bressler LH (2017) Treatment of endometriosis related chronic pelvic pain with ulipristal acetate and associated endometrial changes. HSOAJ Reprod Med Gynaecol Obstet 2: 8.
-
Donnez J, Dolmans MM (2016) Uterine fibroids management: from present to future. Hum Reprod Update 22(6): 665-686.
-
Wagenfeld A, Bone W, Schwede W, Fritsch M, Fisher OM, et al. BAY1002670, a Novel, highly potent and Selective progesterone receptor modulator in gynaecologic therapies. Hum Reprod 2013 28(8): 2253- 2264.
-
Schultze Mosgau MH, Hochel J, Prien O, Zimmermann T, Brooks A, et al. (2018) Characterization of the Pharmacokinetics of vilaprisan: bioavailability, excretion, biotransformation, and Drug-Drug interaction potential. Clin Pharmacokinet 57(8): 1001-1015.
-
Wagenfeld A, Saunders PTK, Whitaker L, Critchley HOD (2016) Selective progesterone receptor modulators: progesterone receptor actions, mode of action on the endometrium and treatment options in gynaecologic therapies. Expert Opin Ther Target 20(9): 1045-54.
-
Grandi G, Farull A, Sileo FG, Facchinetti F (2015) Levonorgestrel releasing intra uterine systems as female contraceptives. Expert Opin Pharmacother 19(7): 667- 686.
-
Schwartz BJ, Alexander M, Breech LL (2021) Levonorgestrel intra uterine device use for medical indicationsin nulliparous adolescents and young adults. J Adolescent Health 68(2):357-363.
-
Zhu SY, Wu YS, Gu ZY, Zhang J, Jia SJ, et al. (2021) Preventive therapeutic options for postoperative recurrence of ovarian endometriomas: gonadotropin releasing hormone agonist with or without Levonorgestrel releasing intra uterine systems insertion. Arch Gynaecol Obstet 303(2): 533-539.
-
Gomes MKO, Rosa-e-Silva JC, Garcia SB, de Sa Rosa-e-Silva ACJ, Turatti A, et al. (2009) Effects of the levonorgestrel releasing intra uterine system on cell proliferation, Fas expression and steroid receptors in endometriosis lesions and normal endometrium. Hum Reprod 24(11): 2736-2745.
-
Dunselman G, Vermeulen N, Becker C, Calhaz-Jorge C, D’Hooge T, et al. (2014) ESHRE guidelines: management of women with endometriosis. Hum Reprod 29(3): 400- 412.
-
Vercellini P, Frontino G, De Giorgio D, Aimi G, Zaina B, et al. (2003) Comparison of Levonorgestrel releasing intra uterine device versus Expectant management after conservative surgery for symptomatic endometriosis: a pilot study. Fertil Steril 80(2): 305-309.
-
Tosti C, Biscione A, Morgante G, Bifulco G, Luisi S, et al. (2017) Hormonal therapy for endometriosis: from molecular research to bedside. Eur J Obstet Gynaecol Reprod Biol 209: 61-66.
-
Chen X, Man GC, Hung SW, Zhang T, Fung LW, et al. (2021) Therapeutic effects of green tea on endometriosis. Crit Rev Food Sci Nutr 63(18): 3222-3235.
-
Vallee A, Lecarpentier Y (2020) Curcumin and endometriosis. Int J Mol Sci 21(7): 2440.
-
D’Alterio MN, Saponars S, Agus M, Lagana AS, Noventa M, et al. (2021) Medical and surgical interventions to improve the quality of life for endometriosis patients: a systematic review. Gynaecol Surg 18: 13.
-
Raffique S, Decherney AH (2017) Medical management of endometriosis. Clin Obstet Gynaecol; 60(3): 485-496.
-
Brichant G, Laraki L, Henry L, Munaut C, Nisolle M (2021) New therapeutics in endometriosis: a review of hormonal, non hormonal and non-coding RNA Treatments. Int J Mol Sci 22(19): 10498.
-
Othman ER, Hendy AA, Mostafa R, Lambalk CB, Mijatovic V (2024) Oral GnRH antagonist in combination with estradiol and Norethindrone acetate for pain relief association with endometriosis:a review of evidence for a novel class of hormonal agents. Int J Womens Health 16: 309-321.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era