Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study
Turner syndrome is the most common sex chromosome abnormality in females, occurring in approximately 1 in 2,000 live births. It is primarily characterized by short stature and gonadal dysfunction, which often lead to delayed or absent puberty and infertility. Early diagnosis of Turner syndrome is crucial, as it allows for the timely initiation of a multidisciplinary management plan, addressing both physical and psychosocial aspects of the condition. Growth hormone therapy plays a pivotal role in improving height outcomes in affected individuals, particularly when started at an early age. Additionally, estrogen replacement therapy is essential for initiating the development of secondary sexual characteristics, maintaining uterine health, and ensuring proper bone mineralization to prevent osteoporosis in later life. We report the case of a 10-yearold female child who presented with complaints of short stature, a webbed neck, and widely spaced nipples. Upon clinical examination and evaluation, the patient exhibited phenotypic features consistent with Turner syndrome. Chromosomal analysis via karyotyping confirmed the diagnosis. Early therapeutic intervention, including growth hormone and planned estrogen replacement therapy, was initiated to optimize growth and development outcomes. This case underscores the importance of early recognition and tailored treatment for improving the quality of life in individuals with Turner syndrome.
Sibi K¹*, Blesson SS², Ganesha M², Vigneswaran G³ and Shashikumar R⁴
Abbreviations
SDS: Standard Deviation Score; TS: Turner Syndrome; SHOX: Short Stature Homeobox; MRI: Magnetic Resonance Imaging; FSH: Follicle Stimulating Hormone; IGF-1: Insulin like Growth Factor-1; HS: Hashimoto’s Thyroiditis.
Introduction
Typically, the onset of growth failure occurs during the prenatal period, and a gradual decrease in the standard deviation score (SDS) of height is often observed during the early years of a child’s life [1]. Turner syndrome (TS) occurs approximately 1 in every 2,000-2,500 live female births, making it the most prevalent chromosomal abnormality in females. Additionally, TS is a significant contributor to short stature in girls and ranks among the leading causes. Generally, a single body cell contains 46 chromosomes or 23 pairs of chromosomes. In males, there are X and Y sex chromosomes (46, XY), while females have two X sex chromosomes (46, XX). However, Turner syndrome (TS) is a chromosomal abnormality found in girls, resulting from the partial or complete absence of one X chromosome (45 XO) in some or all cells of the body. The condition arises due to the lack of structural irregularities of one of the X chromosomes. Women affected by this condition generally exhibit characteristics such as reduced height, hypergonadotropic hypogonadism, and mild skeletal dysplasia [2]. Untreated girls with TS typically have a final height around 20 cm shorter than that of typical female subjects [3].
Turner syndrome (TS) was named by Dr. Henry Turner, an Oklahoma physician, in 1938 after he observed several cases with common characteristics. These included women with short stature, webbing of the neck, cubitus valgus, and sexual infantilism [4]. Infants diagnosed with TS frequently experience a significant occurrence of growth failure. Nevertheless, the exact timing and pattern of the onset of growth and developmental deficiencies remain uncertain [5]. In 1959, the discovery was made that the disease results from the presence of monosomy or structural abnormalities in the X chromosome [6]. The primary cause of short stature in Turner syndrome (TS), the most frequently observed physical characteristic, can largely be attributed to the haploinsufficiency of expression of SHOX in chondrocytes. SHOX is a member of a family of homeobox genes, which are transcriptional regulators and crucial regulators of developmental processes [7]. From the 6th week of gestation onwards, SHOX is specifically found in the initial and subsequent pharyngeal arches of the developing embryo [8]. The atypical growth life is caused by either Haploinsufficiency or complete loss of function of SHOX. This leads to abnormal proliferation and differentiation of chondrocytes, resulting in delayed growth [3].
Case Report
A 10-year-old female patient was presented in a Government hospital in November 2019 with complaints of failure to gain growth. She was born by normal delivery and had a low birth weight of 1.75 kg. Cried immediately after birth, she passed urine and meconium within 24 hours and there was no history of difficulty in breastfeeding. No history of neonatal hyperbilirubinemia. She was immunized with Hepatitis B, OPV, and BCG vaccines. On general examination, the girl was alert, afebrile, and prepubertal with stable vitals and no abnormalities detected in the systemic examination.
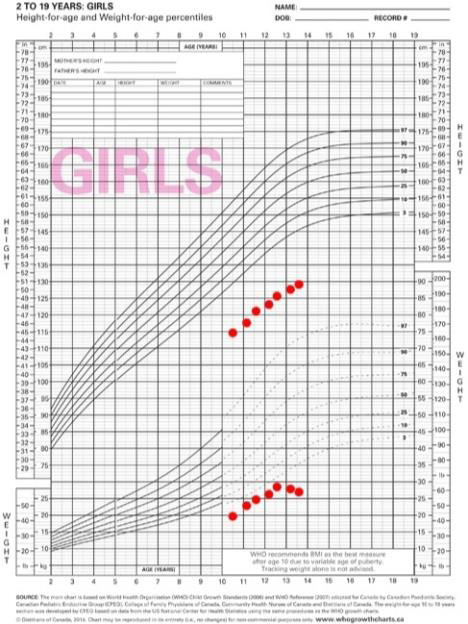
She had a webbed neck and widely placed nipple. Her anthropometric measurement showed a height of 114.5cm (-3SDS), a weight of 19.5kg (-2SDS), and a BMI of 14.87kg/ m2. Head circumference was 45.5 cm. Investigation revealed that the thyroid function , renal function, Luteinizing Hormone(1.17 IU/ml), Follicle Stimulating Hormone (16.9 IU/L), and cortisol (429.56 nmol/L) are within normal range. Serum growth hormone (fasting) was represented in Table1. Serum IGF1(149.6 ng/ml) were normal. The report of the MRI brain was normal. The bone age was 9 years.
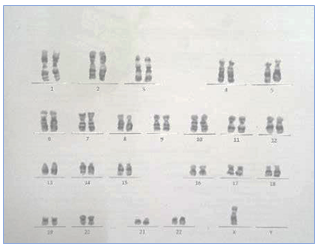
The chromosomal karyotyping was performed and chromosomal analysis showed a TS variant of 45, XO (Figure 1). Based on cytogenetic study and clinical findings, the patient was diagnosed with Turner syndrome. Following a thorough assessment and diagnosis of the disease, the parents were counseled regarding the child’s condition and were recommended a follow-up appointment after three months. Growth hormone (somatropin) 3 units were given subcutaneously once daily. At 12 years of age, the FSH (109 IU/L) and LH (18.4 IU/L) were increased. Gonadal failure was established. Since bone age is only 10, Growth hormone therapy was continued, and start pubertal induction at 13 years of age. At 13 years of age, her FSH (135 IU/L) and LH (25.6 IU/L) were increased and was started with Estradiol 1mg (1/4 HS daily) and advised to review periodically every three months (Table 1 & Figure 2).
| Growth Hormone (ng/ml) | |
|---|---|
| 0 | 13 |
| 30 | 2.7 |
| 60 | 0.87 |
| 90 | 11.1 |
| 120 | 8.4 |
Table 1: Growth hormone stimulation test.
Discussion
The human genome consists of a total of 46 chromosomes which comprise 22 pairs of autosomes along with the X and Y chromosomes. At birth, females possess two fully formed X chromosomes. However, individuals with Turner syndrome typically have 44 autosomes in addition to a single X chromosome. In Turner syndrome, girls may either lack one chromosome (45 XO) or have a portion of it missing. In the case of mosaicism, certain areas of the body contain normal cells with two chromosomes (46 XX), while other areas have one X chromosome missing (45 XO) [5, 9].
We reported a case of Turner syndrome in a 10-years old female child based on chromosomal analysis and physical findings. In chromosomal analysis, the results were 45 XO chromosomes which confirmed Turner syndrome. All patients with TS share a common phenotypic trait of being short stature. Additional characteristics exhibited by these patients include a shortened neck, a wide chest, genu valgum, and nail dysplasia [10]. Similarly in this patient, the physical findings show characteristic features like a webbed neck and widely placed nipple and short stature. The growth hormone peak and peak were good but pathological short stature was present due to Turner syndrome. She was treated with Inj. Growth hormone (somatotropin) 3 units subcutaneously. After treatment with growth hormone, her height increased at a rate of 5cm/year.
In India, Reddy Danda VS, et al. [11] did a study on growth hormone treatment in Turner syndrome which was conducted over an extended period where growth hormone was administered to 16 girls diagnosed with Turner syndrome. The results showed that the patient’s height SDS and body mass index indicated a positive effect of growth hormone treatment for individuals with Turner syndrome. According to the general guideline, it is recommended to initiate patients with small doses of estrogen at the age of 12. This allows the patients to start developing secondary sexual characteristics, as well as the uterus, while also enhancing liver function, cognitive function, and overall quality of life [12]. Gonadal failure was established in our patient and hence estradiol 1mg (1/4) HS was started at the age of 13 years. Multiple research studies have observed a diminished presence of vitamin D in the blood of individuals with TS, which can contribute to a decrease in bone mineral density [13, 14]. Consequently, enhancing bone health in TS patients can be greatly aided by the implementation of vitamin D supplementation and adopting an active lifestyle that involves weight-bearing activities and regular participation in sports [15]. Continuous monitoring and care are necessary for the effective management of Turner Syndrome (TS), with an emphasis on the patient’s psychological well- being, reproductive health, and physical development. This approach aims to reduce potential complications linked to TS.
Conclusion
Turner syndrome is just a small part of who you are. Embrace your uniqueness and shine brightly. In summary, this case study highlights the significance of timely identification, prompt intervention, and comprehensive coordination of care in Turner syndrome. Patients should receive specialized healthcare and support to manage their unique needs and optimize their well-being. Indian government provides growth hormone therapy through government healthcare programs and hospitals to improve the quality of life. It is important for individuals and families affected by turner syndrome to connect with local healthcare providers and support organizations to access the specific support available in their region.
Conflicts of Interest
The author declares there was no conflict of interest.
References
-
Bondy CA, Turner Syndrome Consensus Study Group (2007) Care of girls and women with Turner syndrome: a guideline of the Turner Syndrome Study Group. J Clin Endocrinol Metab 92(1): 10-25.
-
Davenport ML (2010) Approach to the patient with Turner syndrome. J Clin Endocrinol Metab 95(4): 1487- 1495.
-
Munns CJ, Haase HR, Crowther LM, Hayes MT, Blaschke R, et al. (2004) Expression of SHOX in human fetal and childhood growth plate. J Clin Endocrinol Metab 89(8): 4130-4135.
-
Turner HH (1938) A syndrome of infantilism, congenital webbed neck, and cubitus valgus. Endocrinology 23(5): 566-574.
-
Kasagani SK, Mutthineni RB, Jampani ND, Nutalapati R (2011) Report of a case of Turner’s syndrome with localized aggressive periodontitis. J Indian Soc Periodontol 15(2): 173-176.
-
Ford CE, Jones KW, Polani PE, Almeida JCD, Briggs JH (1959) A sex-chromosome anomaly in a case of gonadal dysgenesis (Turner’s syndrome). Lancet 1(7075): 711- 713.
-
Marchini A, Rappold G, Schneider KU (2007) SHOX at a glance: From gene to protein. Arch Physiol Biochem 113(3): 116-123.
-
Clement-Jones M, Schiller S, Rao E, Blaschke RJ, Zuniga A, et al. (2000) The short stature homeobox gene SHOX is involved in skeletal abnormalities in Turner syndrome. Hum Mol Genet 9(5): 695-702.
-
Zhong Q, Layman LC (2012) Genetic considerations in the patient with Turner syndrome-45, X with or without mosaicism. Fertil Steril 98(4): 775-779.
-
Broeck JVD, Massa GG, Attanasio A, Matranga A, Chaussain JL, et al. (1995) Final height after long-term growth hormone treatment in Turner syndrome. J Pediatr 127(5): 729-735.
-
Danda VS, Sreedevi P, Arun G, Rao PS (2017) Growth hormone treatment in Turner’s syndrome: A real world experience. Indian J Endocrinol Metab 21(3): 378-381.
-
Cui X, Cui Y, Shi L, Luan J, Zhou X, et al. (2018) A basic understanding of Turner syndrome: Incidence, complications, diagnosis, and treatment. Intract Rare Dis Res 7(4): 223-228.
-
Landin-Wilhelmsen K, Bryman I, Windh M, Wilhelmsen L (1999) Osteoporosis and fractures in Turner syndrome - Importance of growth-promoting and estrogen therapy. Clin Endocrinol (Oxf) 51(4): 497-502.
-
Gravholt CH, Lauridsen AL, Brixen K, Mosekilde L, Heickendorff L, et al. (2002) Marked disproportionality in bone size and mineral, and distinct abnormalities in bone markers and calcitropic hormones in adult Turner syndrome: a cross-sectional study. J Clin Endocrinol Metab 87(6): 2798-808.
-
Cleemann L, Hjerrild BE, Lauridsen AL, Heickendorff L, Christiansen JS, et al. (2009) Long-term hormone replacement therapy preserves bone mineral density in Turner syndrome. Eur J Endocrinol 161(2): 251-257.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Pheochromocytoma: Therapeutic Agents against the Disease and Chromatographic Methods for their Determination in Biological Fluids