Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
Background: In Japanese clinical practice, two approaches using botulinum toxin A (BTA) are used to improve wrinkles in upper and lower forehead areas without any complications, namely upper forehead subcutaneous (sc)/lower forehead intradermal (id) injections and upper forehead sc/glabellar intramuscular (im) injections. Aim: To investigate the therapeutic effects of combining upper forehead sc and glabellar im BTA injections on forehead wrinkles. Methods: Twenty-two participants were assigned to two groups: group A received upper forehead sc/lower forehead id injections, while group B received upper forehead sc/glabellar im injections. Pain intensity, effects on forehead and glabellar wrinkle severity, eyebrow height/balance, side effect questionnaires, and patient satisfaction were assessed. Results: Forehead wrinkle severity was significantly reduced at week 4 in both groups. During the follow-up period, the severity in group B was consistently lower than group A. Glabellar wrinkles significantly improved only in group B. No abnormalities in eyebrow height or balance and no significant differences in pain intensity were observed. No serious side effects were reported, and patient satisfaction was consistently higher in group B than group A. Conclusions: The results suggest that upper forehead sc/glabellar im injections are more useful in treating forehead wrinkles than upper forehead sc/lower forehead id injections.
Introduction
Botulinum toxin A (BTA) injections are the most commonly performed noninvasive procedure to treat forehead wrinkles and are the most frequently performed cosmetic procedure worldwide for rejuvenation of the upper face [1, 2]. Furthermore, wearing protective masks during the recent coronavirus disease pandemic obscured the lower part of the face, thereby highlighting the upper and midface areas. This further increased the popularity of cosmetic procedures, even after the pandemic, to remove forehead wrinkles [3].
Wrinkles are formed by dermal atrophy and repetitive contraction of the underlying facial muscles [3, 4]. BTA inhibits the release of acetylcholine at the neuromuscular junction, causing muscle relaxation, which subsequently smooths the overlying skin and reduces the development of dynamic wrinkles during muscle contraction [2].
When treating forehead wrinkles, BTA is generally injected intramuscularly at 5–8 points in the frontalis muscle, which causes the wrinkles [5]. The therapeutic use of BTA is generally safe and well tolerated [3]. However, since BTA acts directly on the neuromuscular junction, it may cause complications such as eyebrow ptosis, eyebrow asymmetry, and blepharoptosis when muscle relaxation and the associated skin stretching effects are more active than expected [6, 7]. The complication rate has been reported to be 0.6%–20% [8]. Facial expressions reflect and express various emotions. Therefore, it is critical to avoid any complications, either visual or functional, caused by this cosmetic procedure [3]. Obtaining the maximum treatment effect without complications leads to high patient satisfaction.
Most of the BTA-induced complications are caused by excessive muscle relaxant activity as previously described. Therefore, BTA intramuscular (im) injections within 1.5–2 cm above the eyebrows is often avoided to prevent eyebrow ptosis. However, in that case, it becomes difficult to completely remove expression wrinkles in the lower forehead area [3, 9].
The muscle relaxation effect is stronger the closer the injection site is to the muscle. Therefore, to reduce complications in the treatment area, previous studies have used intradermal (id) or subcutaneous (sc) injections rather than im ones or injecting small doses at multiple points [5, 10, 11, 12]. Additionally, a detailed procedure for im injection, particularly to the corrugator supercilii and procerus muscles, to treat glabellar wrinkles without adverse events has also been recently reported for facial muscles where BTA is frequently injected [13, 14]. In Japan, a combined procedure of upper forehead sc and lower forehead id injections has been conventionally used to treat upper and lower forehead wrinkles and avoid any complications [12]. However, recently, a combination procedure involving upper forehead sc and glabellar im injections has been used empirically in daily medical practice. Despite the fact that we have also noted the effectiveness of the treatment in clinical practice, to the best of our knowledge, information regarding its efficacy and side effects has yet to be reported in the literature.
Therefore, this study aimed to clarify the therapeutic effects of combining upper forehead sc and glabellar im BTA injections.
Materials and Methods
Study Participants
A total of 22 women aged between 25 and 61 years with upper and lower forehead wrinkles participated in this study. The inclusion criteria required participants to have slight glabellar wrinkles (glabellar lines) in addition to upper and lower forehead wrinkles. Exclusion criteria included participants with a history of BTA or filler injections such as hyaluronic acid within the past 4 months, those with glaucoma, chronic respiratory, or neuromuscular disease, those who were breastfeeding or pregnant, and those with compensatory frontalis hyperactivity.
Ethics
This study was performed in accordance with the Helsinki Declaration, and all participants provided informed consent. The protocol was approved by the Institutional Review Board of Shiba Palace Clinic, Japan (approval number 152201_rn-35050).
BTA
BTA (50 units/vial, BOTOX Vista®) purchased from Allergan Japan (Tokyo, Japan) was dissolved in 2.5 mL of saline (4 units/0.1 mL) at the time of use. The appropriate units of BTA were injected according to the following experimental design.
Experimental Design
This study was a single-centre prospective randomized controlled pilot study conducted at the Imaizumi Skin Clinic (Tokyo, Japan). Participants (n = 22) were randomly assigned to two groups, namely the upper/lower forehead injection group (group A, n = 11, mean age: 42.36 ± 9.37 years) and the upper forehead/glabella injection group (group B, n = 11, mean age: 44.09 ± 7.59 years).
Figure 1 shows the BTA injection sites for both groups. The upper and lower forehead regions were separated by a horizontal line drawn 2 cm above the eyebrows. In group A, BTA was injected subcutaneously into 9 points (total 6 units) in the upper forehead area and intradermally into 13 points (total 4 units) in the lower forehead area. In group B, BTA was injected subcutaneously into 9 points (total 6 units) in the upper forehead area and intramuscularly into 7 points (total 14 units) in the glabellar complex, which are mainly composed of corrugator supercilia and procerus muscles.
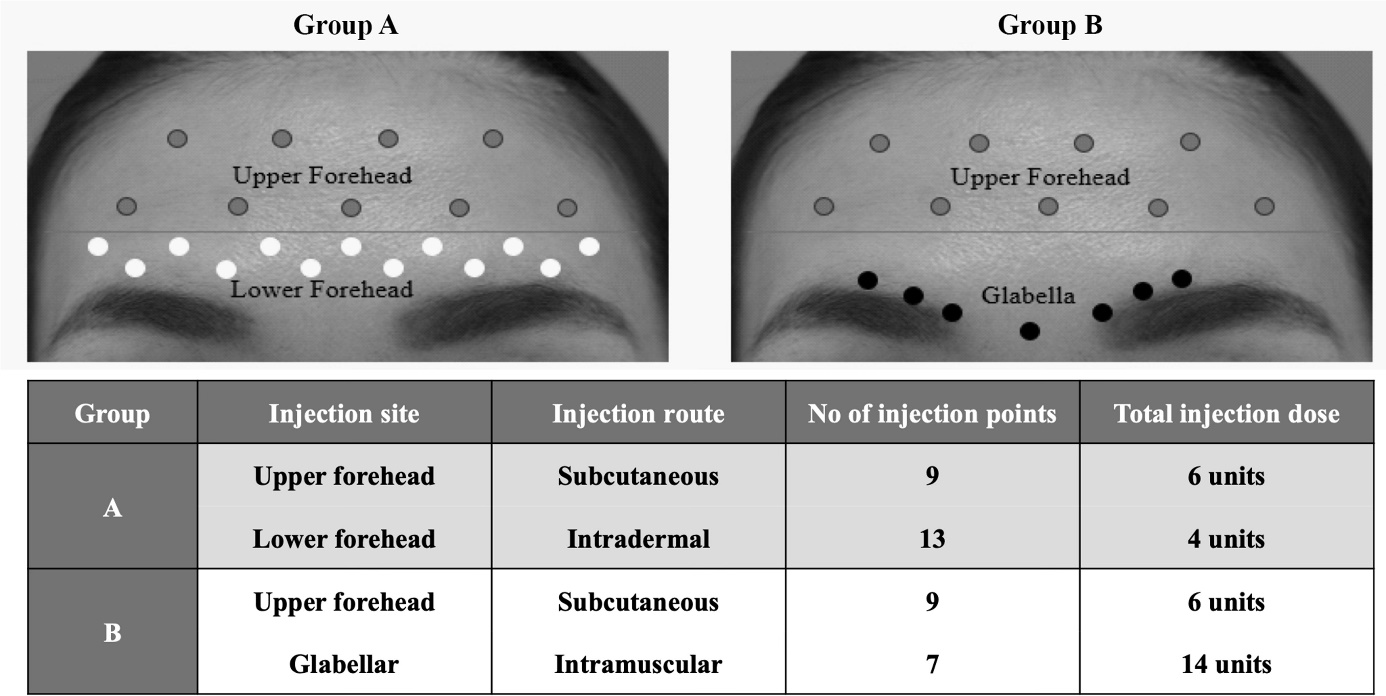
Figure 1: Botulinum toxin A (BTA) injection sites in the forehead and glabellar areas of patients in groups A and B. The upper and lower forehead regions were separated by a horizontal line drawn 2 cm above the eyebrows. In group A, BTA was injected subcutaneously into 9 points (total 6 units) in the upper forehead area and intradermally into 13 points (total 4 units) in the lower forehead area. In group B, BTA was injected subcutaneously into 9 points (total 6 units) in the upper forehead area and intramuscularly into 7 points (total 14 units) in the glabellar complex.
Pain intensity, wrinkle severity, bilateral eyebrow height/ balance, subjective side effect questionnaires, and patient satisfaction reflecting all wrinkle-improving effects and side effects were assessed and compared between the two treatment groups. Pain intensity was assessed immediately after the procedure.
The improvement in forehead wrinkles was evaluated by examining the severity of wrinkles before the BTA injection (week 0) and at weeks 4, 8, and 12 after the injection. Glabellar wrinkles, which were observed in all patients, were also assessed at the same intervals as forehead wrinkles.
Eyebrow height/balance, subjective side effect questionnaires, and patient satisfaction were assessed at weeks 4, 8, and 12.
Evaluation Methods
Pain intensity assessment: Pain intensity immediately after the BTA procedure was assessed for all participants using a 100-mm visual analogy scale (VAS) ranging from 0 (no pain) to 100 (very severe pain) [15]. The patient marked the degree of subjective pain on that line. Pain intensity was quantified by measuring the distance from the 0-mm point.
Wrinkle severity assessment: The status of resting (static) and hyperkinetic (dynamic) wrinkles in the forehead and glabellar areas of the patients was determined by two dermatologists who were not involved in the treatment process.
The degrees of the forehead and glabellar wrinkles observed in both conditions for each patient were classified into five scales according to the wrinkle rating scale, as shown in Figure 2A, using some modifications of previous criteria [16].
The severity of wrinkles for each patient was finally graded into five levels from 0 to 4 by the combination of static and dynamic wrinkle severity, as shown in Figure 2B: Grade 0: no wrinkles in both static and dynamic states, Grade 1: no wrinkles in the static state but minimal wrinkles in the dynamic state, Grade 2: minimal wrinkles in the static state and mild wrinkles in the dynamic state, Grade 3: mild wrinkles in the static state and moderate wrinkles in the dynamic state, and Grade 4: moderate wrinkles in the static state and severe wrinkles in the dynamic state.
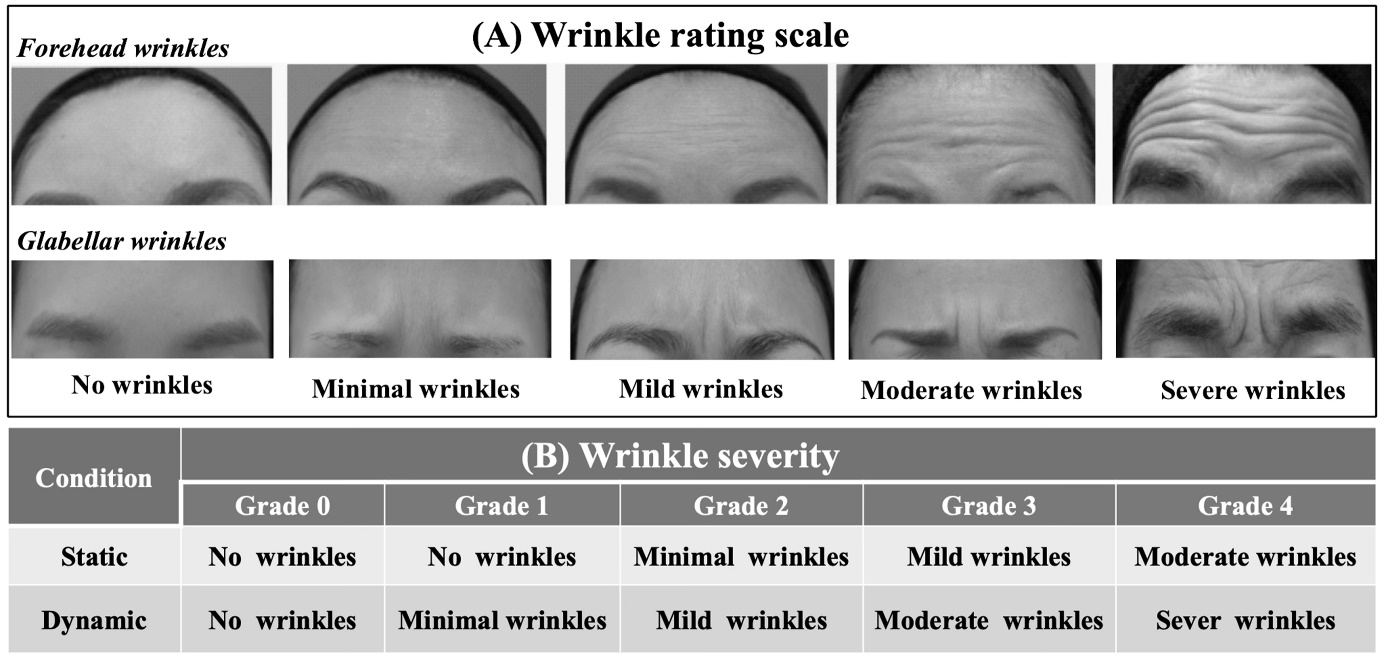
Figure 2: Wrinkle severity assessment. The degrees of the forehead and glabellar wrinkles observed in static and dynamic conditions for each patient were classified into five scales according to the wrinkle rating scale (A). The severity of wrinkles for each patient was finally graded into five levels from 0 to 4 by the combination of static and dynamic wrinkle severity (B).
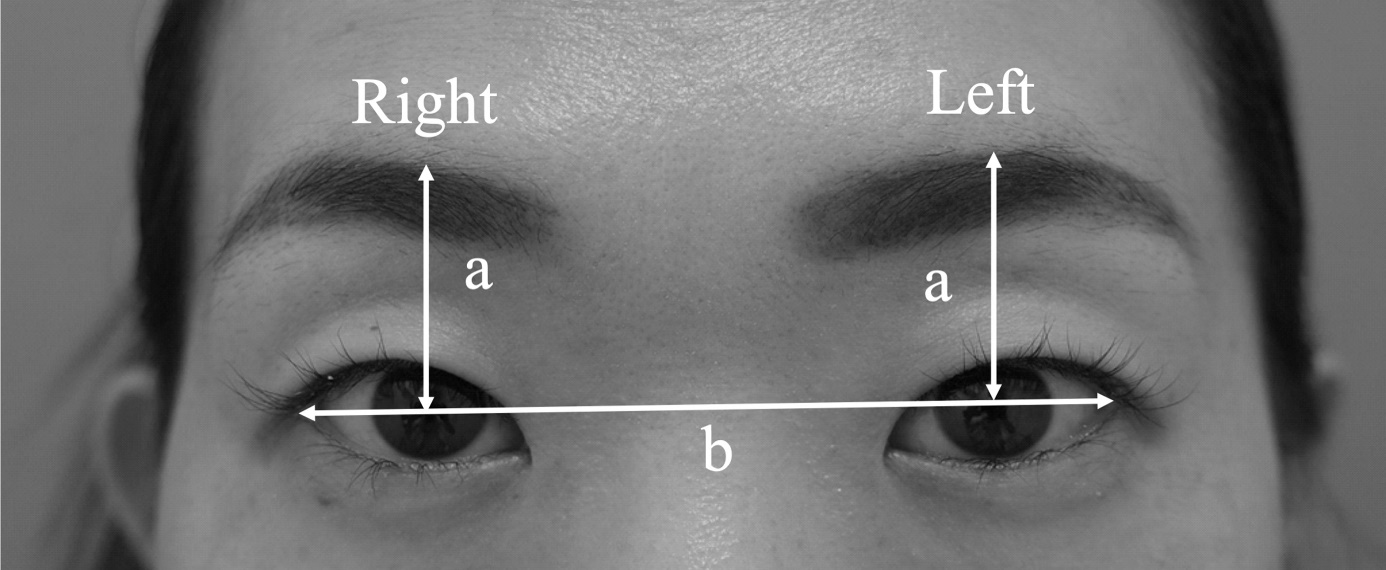
Eyebrow height/balance measurement: All participants’ faces were photographed at rest to measure eyebrow height and balance. Bilateral eyebrow heights were calculated as the normalized eyebrow height ratio according to previously reported procedures [12]. In brief, as shown in Figure 3, Microsoft PowerPoint 2019 (Microsoft, Corp., Redmond, WA, USA) was used to draw a horizontal line (line b) between the bilateral lateral canthus and bilateral vertical midpupillary lines (line a) from line b to the upper edge of the brows. The eyebrow height ratio of each side was normalized by the length of line b using formula (1). The eyebrow balance of both sides was calculated as the balance ratio using formula (2). The value of 1.0 means perfect symmetry. Eyebrow height ratio = length of line a/length of line b (1). Eyebrow balance ratio = eye height ratio of right side/eye height ratio of left side (2).
Subjective adverse effect questionnaire: Various subjective postoperative side effects, including postoperative pain, forehead heaviness, and double eyelid narrowing, were investigated using an open-ended questionnaire.
Evaluation of patient satisfaction after BTA injection: Patient satisfaction after BTA injection was measured for all subjects using a 100-mm VAS scale ranging from 0 (totally dissatisfied) to 100 (totally satisfied) [17, 18]. The patient marked the subjective degree of satisfaction on the line. The satisfaction was quantified by measuring the distance from the 0-mm point.
Statistical analysis: All data for pain intensity, wrinkle severity, bilateral brow height/balance, and patient satisfaction were expressed as mean ± standard error of the mean (SEM). The statistical significance of pain intensity between groups A and B was assessed using the Mann– Whitney U test. The statistical significance of wrinkle severity and patient satisfaction after BTA injections in both groups was assessed using the Mann–Whitney U test (between- group comparisons) or Tukey’s multiple comparison test (postoperative changes) after two-way analysis of variance (ANOVA). The statistical significance of right (R) and left (L) eyebrow heights and postoperative changes in both groups was evaluated using the Mann–Whitney U test and Tukey’s multiple comparison test after two-way ANOVA, respectively. The statistical significance of the R/L balance ratio between both groups and the postoperative changes in both groups was evaluated using the Mann–Whitney U test and Tukey’s multiple comparison test after two-way ANOVA, respectively. The threshold for statistical significance in all analyses was set at P < 0.05. All analyses were performed using GraphPad Prism software version 8.4.2 (GraphPad Software Inc., San Diego, CA, USA).
Results
Pain Immediately after the BTA Procedure
Figure 4 exhibits the levels of subjective pain intensity immediately after BTA treatment in groups A and B, 30.7 ± 7.4 and 24.8 ± 4.0, respectively. No significant differences were observed between the two groups.
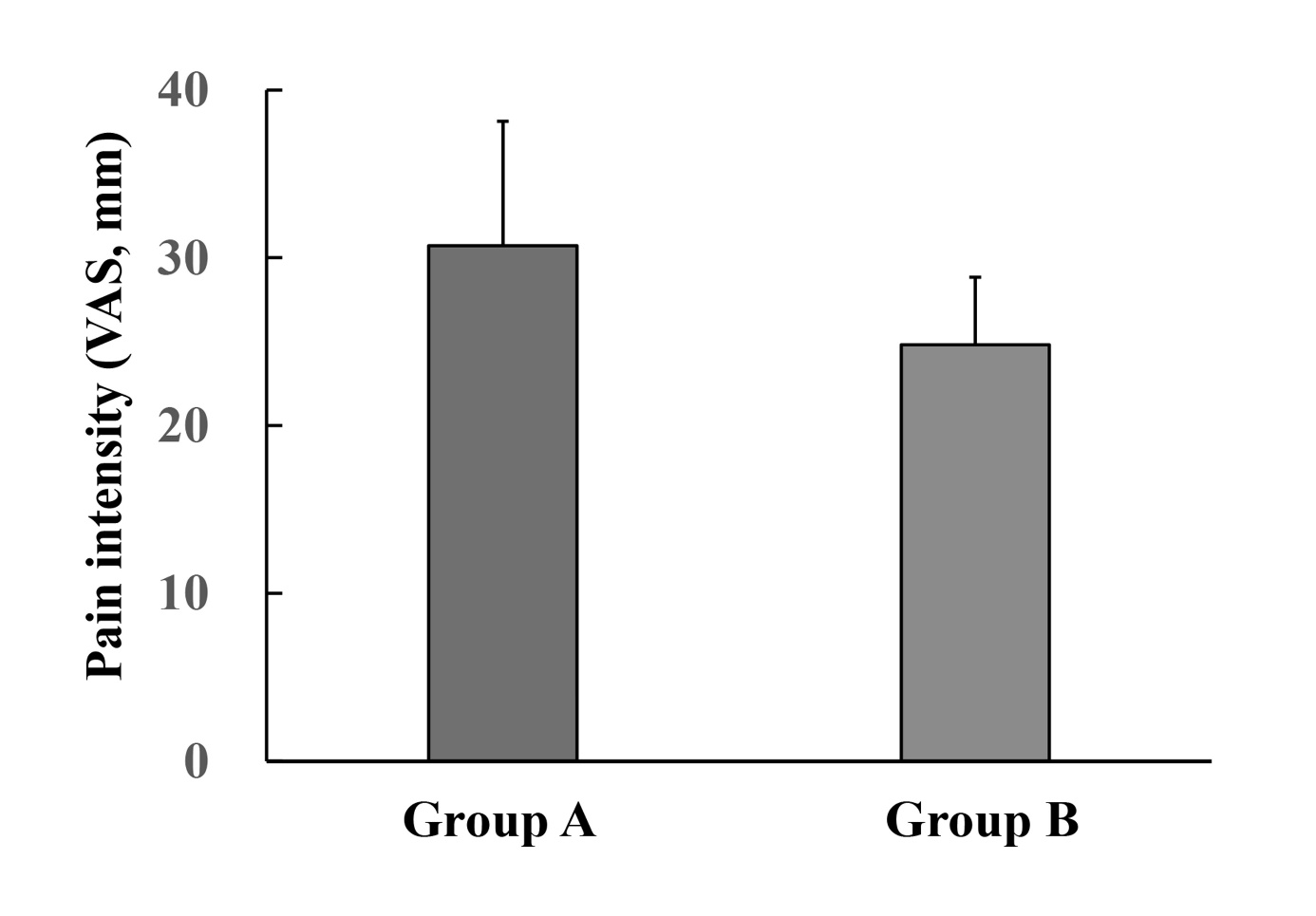
Figure 4: Pain intensity immediately after the BTA procedure. Intensity was assessed using a 100-mm visual analogy scale (VAS) ranging from 0 (no pain) to 100 (very severe pain). The pain intensity was quantified by measuring the distance from the 0-mm point. Each value represents the mean ± SEM (n = 11). No significant differences were observed between the two groups (Mann–Whitney U test).
Improvement Effect of BTA Injection on Forehead and Glabellar Wrinkles
Figure 5A shows the typical dynamic forehead wrinkle status (photos) and changes in wrinkle severity (graphs) after BTA injection in patients of groups A and B. Pretreatment wrinkle severity (week 0) was 1.73 ± 0.19 in group A and 2.09 ± 0.21 in group B, without significant difference between the two groups.
The dynamic wrinkles observed in the upper and lower forehead areas before treatment were almost improved in both groups after week 4. Although the severity was also significantly decreased in both groups (Group A: P < 0.01, Group B: P < 0.001), the severity at week 4 started to increase gradually with time. Nonetheless, the severity in group B was always lower than that in group A during the follow-up period. Statistically, a decreasing trend (P = 0.069) and a significant decrease (P < 0.05) were observed in group B at weeks 4 and 8, respectively.
Figure 5B shows the typical dynamic glabellar wrinkle status (photos) and changes in wrinkle severity (graphs) after BTA injection in patients of groups A and B. All patients in groups A and B had slight dynamic glabellar wrinkles before treatment (Grade 1), with no significant difference between them. Glabellar wrinkles observed before BTA treatment in group A did not improve throughout the 12- week follow-up period. However, group B showed significant improvement (P < 0.001). The severity, which was 1.0 before treatment, improved to 0 (i.e., complete improvement) at week 4. Although the improvement gradually weakened thereafter, it remained >50% (0.45 ± 0.16) at week 12. Statistical comparisons between the two groups showed that group B had a significantly higher improvement at weeks 4 (P < 0.001) and 8 (P < 0.01) compared with group A.
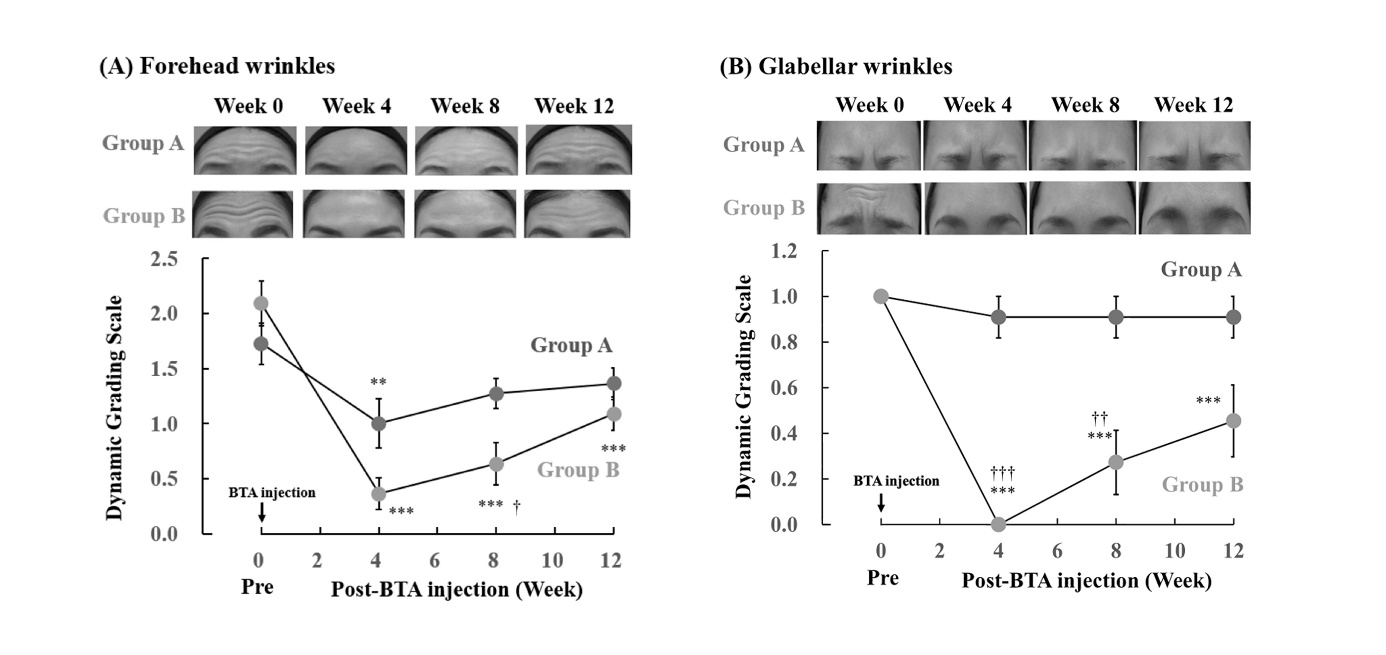
Figure 5: Changes in the severity of forehead (A) and glabellar wrinkles (B) after BTA injection in groups A and B. The photos show the dynamic wrinkle status of the patient’s forehead and glabellar before (week 0) and after BTA injection (weeks 4, 8, and 12) in groups A and B. Wrinkle severity was graded into five levels from 0 to 4. Each value represents the mean ± SEM (n = 11). P < 0.01 and *P < 0.001 vs. pretreatment week 0 (two-way ANOVA + Tukey’s multiple comparison test). †P < 0.05, ††P < 0.01, and †††P < 0.001 vs. group A (two-way ANOVA + Mann–Whitney U test).
Eyebrow Height and Balance
Figure 6 shows the changes in height (Figure 6A) and balance (Figure 6B) of the right and left eyebrows after BTA injection in groups A and B.
Before treatment (week 0), the right (R) and left (L) eyebrow heights were 0.297 ± 0.010 and 0.286 ± 0.012 in group A and 0.310 ± 0.012 and 0.309 ± 0.009 in group B, respectively (Figure 6A). The R/L eyebrow height balance was 1.042 ± 0.024 in group A and 1.006 ± 0.035 in group B (Figure 6B). No significant differences in the eyebrow heights and the R/L balance were observed between the two groups.
Compared with pretreatment, no significant changes were observed in height (Figure 6A) or R/L balance (Figure 6B) of the bilateral eyebrows in both groups at 4, 8, and 12 weeks after BTA treatment.
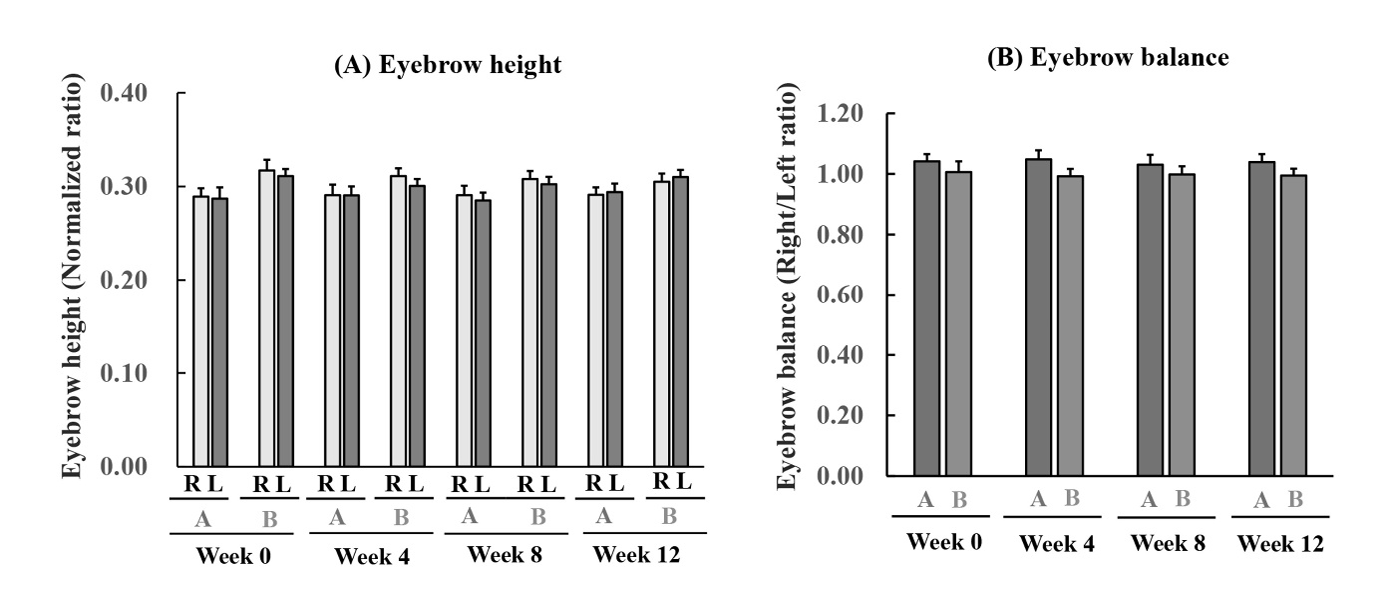
Figure 6: Changes in the right and left eyebrow heights (A) and bilateral eyebrow balance (B) after BTA injection in groups A and B. The height and balance were calculated using formulas (1) and (2). Each value represents the mean ± SEM (n = 11). No significant differences were observed between the height of right (R) and left (L) eyebrows at weeks 0 (pretreatment), 4, 8, and 12 and postoperative changes in both groups (two-way ANOVA + Mann–Whitney U test or Tukey’s multiple comparison test). No significant differences were observed in the R/L balance ratio between both groups and the postoperative changes in both groups (two-way ANOVA + Mann–Whitney U test or Tukey’s multiple comparison test).
Subjective Adverse Effect Questionnaire
In the subjective open-ended questionnaire regarding postoperative side effects, 2 of 11 patients in group A and 1 of 11 in group B complained of mild eyelid heaviness. However, these symptoms improved spontaneously within 4 weeks after BTA injection without any treatment. No complaints of other side effects were reported throughout the 12-week follow-up period.
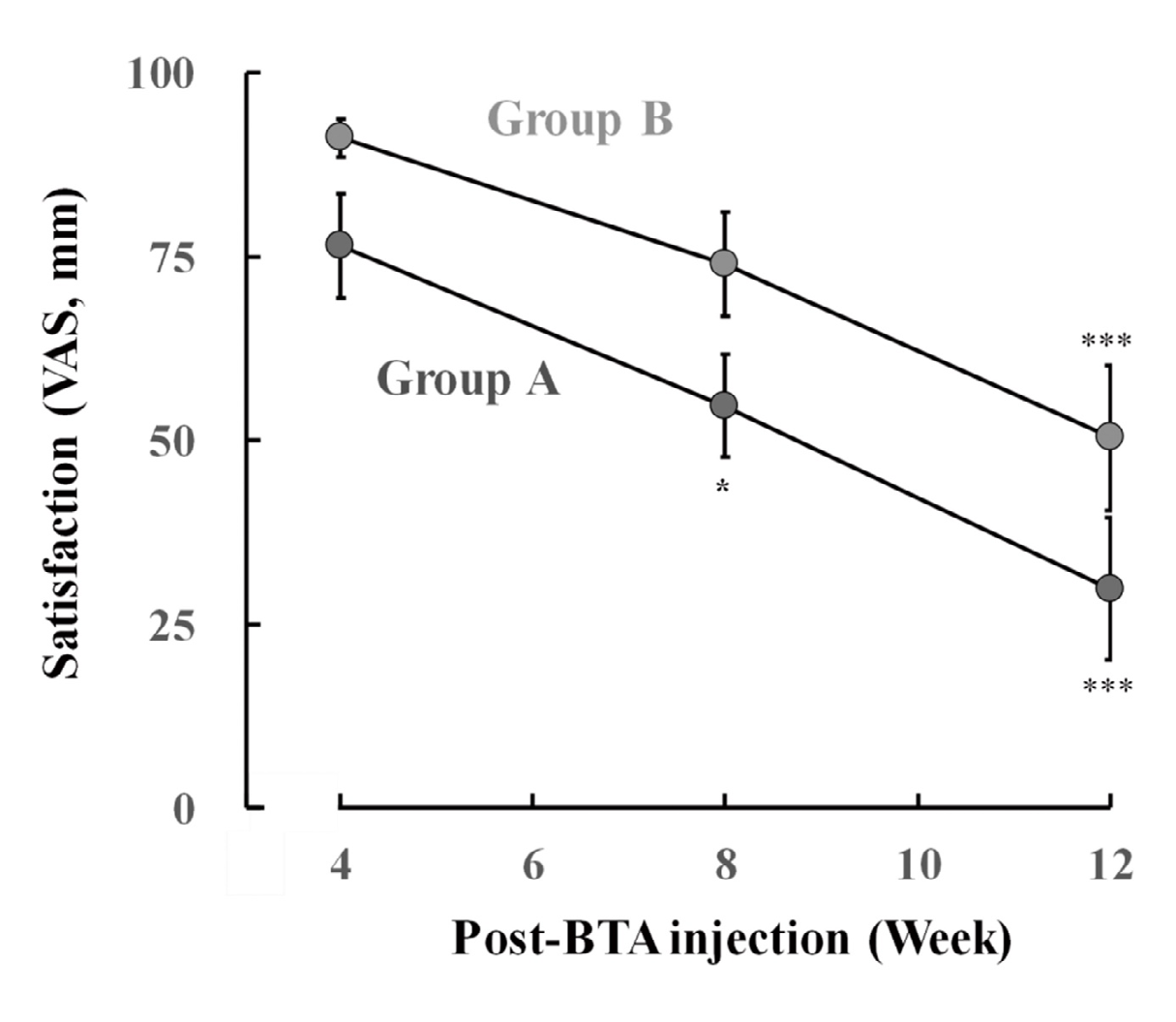
Figure 7: Changes in patient satisfaction after the BTA procedure in groups A and B. The satisfaction was assessed using a 100- mm visual analogy scale (VAS) ranging from 0 (totally dissatisfied) to 100 (totally satisfied). Patient satisfaction was quantified by measuring the distance from the 0-mm point. Each value represents the mean ± SEM (n = 11). *P < 0.05 and ***P < 0.001 vs. week 4 (two-way ANOVA + Tukey’s multiple comparison test). No significant differences were observed between both groups at weeks 4, 8, and 12 (two-way ANOVA + Mann–Whitney U test).
Patient Satisfaction
Figure 7 shows the changes in patient satisfaction after BTA treatment in groups A and B. Patients in both groups showed higher satisfaction at 4 weeks after treatment (Group A: 76.5 ± 7.1, Group B: 91.2 ± 2.6), and there was no significant difference between the two groups. However, the high satisfaction levels in both groups gradually decreased over time. More specifically, a significant decrease was observed at weeks 8 (P < 0.05) and 12 (P < 0.001) in group A and at week 12 (P < 0.001) in group B. Although this difference in changes between the two groups was not statistically significant, the satisfaction levels in group B were consistently higher than those in group A.
Figure 8 shows the correlation between patient satisfaction and forehead wrinkle severity throughout BTA treatment. Each value represents the mean ± SEM (n = 11) of the patient satisfaction (y) and wrinkle severity (x) assessed at weeks 4, 8, and 12 after BTA injection in groups A and B. Our results revealed a high negative linear correlation (y = −50.659x + 111.11 and correlation coefficient R² = 0.7828), indicating that satisfaction increased as wrinkle severity decreased, and vice versa.
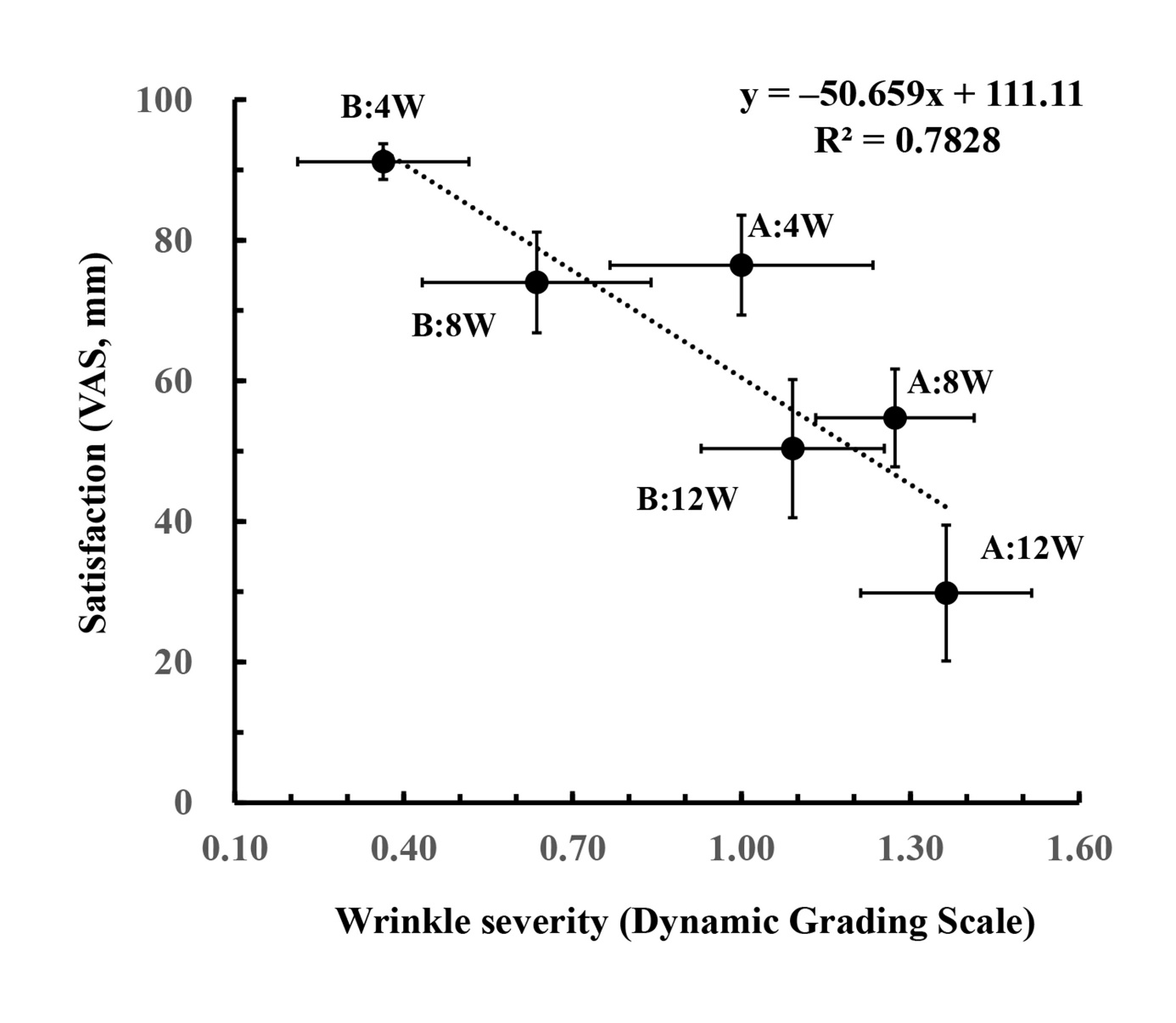
Figure 8: Correlation between patient satisfaction and forehead wrinkle severity throughout BTA treatment. Each value represents the mean ± SEM (n = 11) of patient satisfaction (y) and wrinkle severity (x) assessed at weeks 4, 8, and 12 after BTA injection in groups A (A:4W–A:12W) and B (B:4W–B:12W), revealing a high negative linear approximation correlation (y = −50.659x + 111.11 and correlation coefficient R² = 0.7828).
Discussion
BTA injections are commonly used to treat expression wrinkles on the forehead area and are usually injected intramuscularly [5]. However, complications are a significant issue pertaining to this treatment, including eyebrow ptosis, eyebrow asymmetry, and blepharoptosis caused by excessive muscle relaxant activity [6, 7, 8]. Although the optimal approach to prevent these complications is to avoid im injections above the eyebrows, this makes the complete treatment of wrinkles in the lower forehead area very difficult [3, 9]. In Japan, two procedures involving upper forehead sc/lower forehead id (group A in this study) and upper forehead sc/ glabellar im injections (group B in this study) are performed in daily clinical practice to reduce wrinkles in the upper and lower forehead areas without any complications. The BTA
dose differed between the two groups, with 10 units used in group A and 20 units in group B. The differences between the two procedures were not only limited to the dose but also included the injection site, injection route, and number of injection points (Figure 1). Despite these differences, the varying BTA doses are considered equivalent in terms of efficacy and safety under these conditions. To the best of our knowledge, no study has previously compared the efficacy and complications of these two procedures. This study is the first to evaluate both aspects in a single institution.
In general, BTA improves wrinkles by selectively blocking nerve transmission at the neuromuscular junction [2, 19]. However, its blocking effect gradually fades 3–4 months after the procedure [19, 20, 21] due to the formation of new neuromuscular junctions through nerve sprouting over time [19]. Therefore, repeated injections are usually required to maintain the therapeutic efficacy of BTA [19, 21].
Our results showed that the severity of wrinkles in the entire forehead area, including the upper and lower forehead regions, in both groups significantly decreased at 4 weeks after BTA injection. However, it gradually increased from weeks 8 to 12 (Figure 5A). This result suggests that the wrinkle improvement effect of BTA reached its peak after 4 weeks of treatment and gradually started to fade, in accordance with the results of previous reports [22, 23]. The wrinkle severity in group B was always lower than that in group A, indicating that this treatment approach to improving wrinkles was more effective in group B than in group A. In this study, all patients had slight glabellar wrinkles in addition to forehead wrinkles. Therefore, the effect on glabellar wrinkles was also evaluated (Figure. 5B). Glabellar wrinkles observed before BTA treatment significantly improved in group B but not in group A. This result suggests that group B has an advantage over group A.
Wrinkle relapse is a common process due to the limited durability of BTA action [19, 20]. Therefore, to maintain the therapeutic efficacy of BTA, repeated injections are usually required [19, 21]. Because the muscle fibers of the frontalis muscle are partially fused with the glabellar complex, BTA injection into the glabellar complex may have also affected the muscle fibers of the lower part of the frontalis muscle [9]. Therefore, the wrinkle improvement effect in the entire forehead, including the glabellar area, was consistently higher in group B than in group A, and the effect was superior to that of group A even at 12 weeks. This superiority of group B suggests that the wrinkle improvement effect may be sustained more than that of group A even with repeated injections.
With respect to BTA treatment, it is critical to avoid complications such as eyebrow ptosis, eyebrow asymmetry, and blepharoptosis [7, 8]. The present study demonstrated that there was no statistically significant difference in pain intensity immediately after BTA treatment between the two groups (Figure 4). Additionally, we did not observe any abnormalities pertaining to eyebrow height or balance in both groups after BTA injection (Figure 6), and no serious side effects were reported in the questionnaire. Our findings suggest that both procedures investigated in the present study were appropriate and safe procedures for improving forehead wrinkles, including the lower forehead area.
Despite the fact that patient satisfaction in both groups was found to be higher after four weeks of treatment, it then gradually decreased over time (Figure 7). Patient satisfaction with BTA treatment is a critical success factor in cosmetic procedures and depends on the interaction of numerous variables [22]. Considering that no complications occurred with either procedure, this decrease in satisfaction may be related to wrinkle relapse. Therefore, when we investigated the correlation between wrinkle severity or degree of improvement (x) and satisfaction level (y) after BTA treatment, we identified a high negative linear correlation between these two variables (Figure 8: y = −50.659x + 111.11, correlation coefficient R² = 0.7828). This result clearly reflects patient psychology in that satisfaction increased when wrinkles were improved by BTA treatment, while satisfaction decreased when the improvement effect was not sustained. Therefore, the postoperative decrease in patient satisfaction revealed in the present study might be due to wrinkle relapse rather than to the development of any side effects. Our results showed no statistically significant difference in satisfaction change after one injection between the two groups. However, satisfaction tended to be consistently higher in group B than in group A. This is thought to be because the degree of wrinkle improvement in group B was always greater than that in group A.
Overall, the results of this comparative study suggest that both treatment approaches are appropriate for improving forehead wrinkles, including the lower forehead area, which is difficult to treat without any side effects. The total BTA dose in group B (20 units) was twice that in group A (10 units), indicating that the cost price of BTA in group B was twice that in group A. Therefore, the treatment cost in group B was higher than that in group A. However, compared with group A, group B was characterized by higher treatment efficacy and satisfaction for forehead wrinkles, suggesting that group B might be more suitable or advantageous for improving forehead wrinkles, including the lower forehead area.
This study had several limitations. First, considering the small sample size enrolled, our conclusions need to be validated in future randomized controlled trials with larger sample sizes. Second, this study focused on the efficacy of single-injection treatments. The duration of BTA treatment efficacy impacts not only the retreatment interval but also leads to higher costs and patient inconvenience [22]. Future studies should investigate the effects, duration, and recurrence of repeated treatments.
Conclusion
This study compared the efficacy and complications of two BTA treatments involving upper forehead sc/lower forehead id (group A) and upper forehead sc/glabellar im injections (group B) in patients with upper and lower forehead wrinkles at a single institution. A summary comparing key outcome measures between groups A and B is shown in Table 1. Our results showed that both procedures improved forehead wrinkles, including the lower forehead area, which is difficult to treat, without any complications.
However, treatment in group B consistently exhibited higher efficacy and patient satisfaction than those in group A. Additionally, the glabellar wrinkles before BTA treatment significantly improved in group B but not in group A. Our findings indicate that upper forehead sc/glabellar im injections may be more appropriate or advantageous than upper forehead sc/lower forehead id injections for patients with wrinkles in the upper and lower forehead areas.
| Key Outcome Measures | Comparison Between the Two Groups |
|---|---|
| Pain intensity | A = B |
| Forehead wrinkles improvement | A < B |
| Glabellar wrinkles improvement | A < B |
| Eyebrow height or imbalance: None | A = B |
| Serious side effects: None | A = B |
| Patient Satisfaction | A < B |
Table 1: A summary table comparing key outcome measures between groups A and B. Group A: Upper forehead sc/lower forehead id inje
Acknowledgments
We would also like to thank Enago (https://www.enago. jp) for the English language review. The author would like to thank the Medical Affairs of Allergan Aesthetics Japan. The authors did not receive support from any organization for the submitted work.
Conflict of Interest
The authors declare no conflict of interest.
References
-
Sundaram H, Signorini M, Liew S, de Almeida AR, Wu Y, et al. (2016) Global aesthetics consensus: botulinum toxin type A–evidence-based review, emerging concepts, and consensus recommendations for aesthetic use, including updates on complications. Plast Reconstr Surg 137(3): 518e-529e.
-
Small R (2014) Botulinum toxin injection for facial wrinkles. Am Fam Physician 90(3): 168-175.
-
Borba A, Matayoshi S, Rodrigues M (2022) Avoiding complications on the upper face treatment with botulinum toxin: A practical guide. Aesthet Plast Surg 46(1): 385-394.
-
Fisher GJ (2005) The pathophysiology of photoaging of the skin. Cutis 75(2Supply): 5-8.
-
Jun JY, Park JH, Youn CS, Lee JH (2018) Intradermal injection of botulinum toxin: A safer treatment modality for forehead wrinkles. Ann Dermatol 30(4): 458-461.
-
Kroumpouzos G, Kassir M, Gupta M, Patil A, Goldust MJ (2021) Complications of botulinum toxin A: an update review. J Cosmet Dermatol 20(6): 1585-1590.
-
Nestor MS, Han H, Gade A, Fischer D, Saban Y, et al. (2021) Botulinum toxin-induced blepharoptosis: anatomy, etiology, prevention, and therapeutic options. J Cosmet Dermatol 20(10): 3133-3146.
-
Kim YJ, Lim OK, Choi WJ (2020) Are there differences between intradermal and intramuscular injections of botulinum toxin on the forehead? Dermatol Surg 46(12): e126-e131.
-
Ahn BK, Kim YS, Kim HJ, Rho NK, Kim HS (2013) Consensus recommendations on the aesthetic usage of botulinum toxin type A in Asians. Dermatol Surg 39(12): 1843-1860.
-
Iranmanesh B, Khalili M, Mohammadi S, Amiri R, Aflatoonian MJ (2022) Employing Microbotox technique for facial rejuvenation and face-lift. J Cosmet Dermatol 21(10): 4160-4170.
-
Kandhari R, Kaur I, Gupta J, Al-Niaimi FJ (2022) Microdroplet botulinum toxin: a review. J Cutan Aesthet Surg 15(2): 101-107.
-
Zhang X, Cai L, Yang M, Li F, Han X (2020) Botulinum toxin to treat horizontal forehead lines: A refined injection pattern accommodating the lower frontalis. Aesthet Surg J 40(6): 668-678.
-
Yi KH, Lee JH, Hu HW, Kim HJ (2022) Anatomical proposal for botulinum neurotoxin injection for glabellar frown lines. Toxins (Basel) 14(4): 268.
-
Fagien S, Cohen JL, Coleman W, Monheit G, Carruthers J, et al (2017) Forehead line treatment with onabotulinumtoxinA in subjects with forehead and glabellar facial rhytids: a phase 3 study. Dermatol Surg 43(Suppl 3): S274-S284.
-
Myles PS, Myles DB, Galagher W, Boyd D, Chew C, et al (2017) Measuring acute postoperative pain using the visual analog scale: the minimal clinically important difference and patient acceptable symptom state. Br J Anaesth 118(3): 424-429.
-
Carruthers A, Carruthers J (2010) A validated facial grading scale: the future of facial ageing measurement tools? J Cosmet Laser Ther 12(5): 235-241.
-
Meral SE, Tüz HH, Başlarlı Ö (2021) Evaluation of patient satisfaction after botulinum toxin A injection for the management of masticatory myofascial pain and dysfunction – A pilot study. Cranio 39(1): 12-16.
-
da Silva Ramalho JA, Palma LF, Ramalho KM, Tedesco TK, Morimoto S (2023) Effect of botulinum toxin A on pain, bite force, and satisfaction of patients with bruxism: A randomized single-blind clinical trial comparing two protocols. Saudi Dent J 35(1): 53-60.
-
Ma L, Pan L, Liu W, Liu Y, Xiang X, et al. (2020) Agrin influences botulinum neurotoxin A-induced nerve sprouting via MiR-144-Agrin-MuSK signalling. Front Cell Dev Biol 8: 15.
-
Dolly JO, Aoki KR (2006) The structure and mode of action of different botulinum toxins. Eur J Neurol 13(Suppl 4): 1-9.
-
Solish N, Carruthers J, Kaufman J, Rubio RG, Gross TM, et al (2021) Overview of Daxibotulinumtoxin A for injection: A novel formulation of botulinum toxin type A. Drugs 81(18): 2091-2101.
-
Flynn TC (2010) Botulinum toxin: examining duration of effect in facial aesthetic applications. Am J Clin Dermatol 11(3): 183-199.
-
Wright G, Lax A, Mehta SB (2018) A review of the longevity of effect of botulinum toxin in wrinkle treatments. Br Dent J 224(4): 255-260.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study
- Pheochromocytoma: Therapeutic Agents against the Disease and Chromatographic Methods for their Determination in Biological Fluids