Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
A heart attack (MI), is a serious medical disaster that arises when blood supply to the heart is abruptly obstructed mainly due to blood clots. Blockage damages the heart muscle. Common signs of heart attack are chest pain or discomfort, difficulty breathing, swelling in the legs or abdomen, fatigue, and a bluish tint to the skin (cyanosis). Risk factors e.g. smoking, hypertension, diabetes, hyperlipidemia, atherosclerosis & family history increase likelihood of MI. Early detection is critical, using diagnostic tools like (ECG, troponin tests & imaging techniques. Treatments include blood thinners, thrombolytics, beta-blockers, ACE inhibitors, and statins. In Azad Kashmir, MI is the most noteworthy etiological factor of illness and mortality in spite of advancements in heart care. The region faces unique challenges, including a high prevalence of risk factors, inconsistent healthcare practices, and frequent prescription errors. The study reviewed 100 MI prescriptions from regional public healthcare facilities, focusing on drug interactions, dosages, treatment frequency, and duration. The analysis revealed several issues, with the most common error being missing treatment frequency (31.25%), followed by missing doses (25%). Drug-drug interactions were also significant, with pharmacodynamic interactions being the most frequent (36.84%), followed by synergistic (33.08%), antagonistic (27.82%), and pharmacokinetic interactions (2.26%). These outcomes highlight the pressing need for directed interventions to reduce prescription errors and improve MI care. Addressing healthcare inconsistencies, resource limitations, and gaps in professional training can help enhance treatment outcomes. This study provides valuable insights for public health planning & policy-making to manage heart attacks better and reduce their impact in resource-limited settings like AJK.
Introduction
Myocardial Infarction (MI), generally recognized as a heart attack, occurs when blood flow to the heart is abruptly interrupted, typically due to a blood clot. This leads to ischemia, hypoxia, and necrosis of heart muscle cells due to imbalance between oxygen supply & demand. Symptoms comprises chest pain radiating to the shoulder, arm, back and neck. Types By anatomic site: Transmural Infarction Involves the entire heart muscle thickness due to complete blood supply blockage. Subtypes include Anterior wall MI [1], caused by left anterior descending artery (LAD) occlusion. Lateral wall MI: Due to occlusion of circumflex branches or diagonal LAD branches. Inferolateral or Inferior- Posterior wall MI: Result of posterior descending or wrapped LAD artery blockage. Subendocardial Infarction: Affects a localized area of the inner heart wall. By diagnostic basis: ST-Segment Elevation MI (STEMI): Characterized by ST elevation in ECG leads; indicates severe myocardial injury. Non-ST Segment Elevation MI (NSTEMI): Partial obstruction with ST depression or T-wave inversion; associated with cell damage.
Etiology Key factors: Atherosclerosis Plaque buildup leads to coronary obstruction, inflammation, and thrombosis. Lifestyle factors: Smoking [2], alcohol use, stress, obesity. Chronic conditions [3]: Hypertension, diabetes mellitus, dyslipidemia. Demographic factors: Age, male gender, family history. Signs and Symptoms Chest pain (discomfort). Sweating, dyspnea fatigue, and dizziness. Cyanosis, swelling (edema), and weight gain. Palpitations or cough Complications [4]: Cardiogenic shock, break of the heart’s outer wall (ventricular septum), sudden mitral valve dysfunction, and damage to the right ventricle are potential complications. Additional issues include problems produced by reduced blood flow & abnormal heart rhythms e.g. cardiac arrest, blood clots, and inflammation of the heart lining (pericarditis). Depression and thromboembolism. Diagnosis ECG [5]: Detects ST elevation or depression. Biomarkers: Elevated troponins (T, I), CK-MB, and myoglobin. Imaging: Echocardiography, chest X-ray, CT, MRI, and PET scans [6]. Treatment Medications: Antiplatelets [7]: (e.g., aspirin, clopidogrel) prevent clot formation. Anticoagulants: (e.g., heparin) reduce thrombosis risk. Thrombolytics: Dissolve existing clots. Nitroglycerin: Dilates blood vessels. Beta-blockers & ACE inhibitors: Reduce heart workload and improve blood flow. Statins: Lower cholesterol and prevent plaque buildup. Diuretics: Manage fluid retention. Prevention Lifestyle modifications: Healthy diet, regular exercise, smoking cessation, and limited alcohol intake. Medical management: Controlling hypertension, diabetes, and dyslipidemia. Patient education: Stress reduction and routine check-ups. Prevalence of Myocardial Infarction; In Developing Countries Over 80% of cardiovascular deaths occur in low- and middle-income countries. High triglyceride levels, fasting hyperglycemia, and metabolic syndrome components are significant predictors of MI morbidity and mortality. Women and older adults are particularly affected, with metabolic syndrome increasing in-hospital fatality rates. In India, Indians are at a disproportionately high risk [8] for coronary artery disease (CAD), developing it 5–10 years earlier than other ethnic groups. CAD often presents in severe forms before 40 years of age, with elevated triglyceride levels being a unique risk factor. Premature CAD is common, with higher hospitalization and mortality rates compared to other populations. Globally, myocardial infarction (MI) is more common in males than females, primarily due to factors like lipid imbalances and smoking at younger ages. Although hospitalization rates for MI have decreased by 4-5% annually in developed nations, it continues to be a leading cause of premature death worldwide, largely driven by risk factors such as hypertension, dyslipidemia, smoking, and diabetes. Cardiovascular disease (CVD) represents nearly half of all deaths from non-communicable diseases (NCDs), with an estimated 17.3 million deaths annually, expected to rise to more than 23.6 million by 2030. Major contributing factors include obesity [9], which has seen a global prevalence double from 1980 to 2008, causing 2.8 million deaths each year; hypertension [7], which affects around 40% of adults over the age of 25 and contributes to 51% of stroke deaths and 45% of coronary heart disease deaths; and smoking, which has decreased by half in the United States over the past 25 years but remains high in many OECD countries [2]. Drug Classes: Anticoagulants, insulin, opioid analgesics, oral hypoglycemic, and antineoplastic agents are the most implicated in adverse drug events requiring hospitalization. Efforts such as voluntary reporting systems (e.g., FDA and MEDMARX) and structured taxonomies aim to reduce medication errors and improve MI management outcomes. This study aims to investigate the etiological factors contributing to myocardial infarction and to identify and analyze prescription errors in various healthcare systems of Azad Kashmir. By comparing public, private, and informal healthcare settings, the study seeks to uncover gaps in the prevention, diagnosis, and management of myocardial infarction, with the ultimate goal of improving clinical outcomes and optimizing healthcare practices in the region.
Materials and Methods
Selection Criteria Population: Male and female patients visiting heart specialists and physicians. Inclusion Criteria: Age: Patients aged 40–80 years. Gender: Data from both male and female patients. Disease: Prescriptions of myocardial infarction (MI) patients, including those with comorbidities such as hypertension, Type II diabetes, COPD, bacterial/fungal infections, GERD, asthma, hemorrhoids, peptic ulcers, and anxiety disorders. Exclusion Criteria: Prescriptions unrelated to MI or outside the inclusion criteria were excluded to maintain focus on MI-related data. Sample and Sample Size Sample Size: 200 prescriptions were collected, of which 100 relevant to MI were selected. Data Collection Tools and Methods Tools: Researchers personally visited cardiology wards, OPDs at CMH Rawalakot, and doctors’ clinics. Mode: Prescriptions were directly collected from the above sources. Data Analysis Software: Medscape was used to analyze drug interactions. Interaction Types: Synergistic, Antagonistic Pharmacokinetic Statistical
Analysis: Interaction types and their frequency were expressed as percentages. Study Parameters Dose of drugs used for MI Prescription errors and their solutions Drug-drug interactions Diagnostic features Number and frequency of drugs prescribed Objectives Main Objective: To assess the etiology of MI and prescription errors in the Azad Kashmir healthcare system. Specific Objectives: Study the etiology of MI. Identify prescription errors in MI cases. Evaluate rational drug use based on WHO guidelines. Reduce drug-related problems through prescription analysis. Identify drug-drug interactions in MI prescriptions.
Results; Myocardial Infarction Trends, Risks, and Medication Errors
A study involving 100 myocardial infarction (MI) patients in Rawalakot revealed notable patterns in gender and age- specific risk factors. Male patients aged 45 to 65 were found to have a higher occurrence of MI compared to females, who were primarily between 55 and 75 years old. Smoking was identified as a significant risk factor among males, whereas none of the female participants were smokers. Hypertension and hypertriglyceridemia were frequently observed co- morbidities, though their prevalence differed between genders. Hypertension was present in 41.2% of male patients and 30.3% of female patients, whereas hypertriglyceridemia affected 30.7% of females compared to 21.3% of males.
Medication Errors in MI Management: A Critical Issue
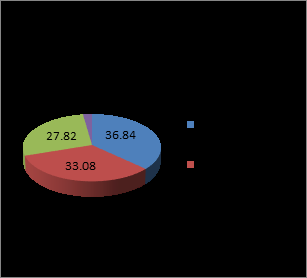
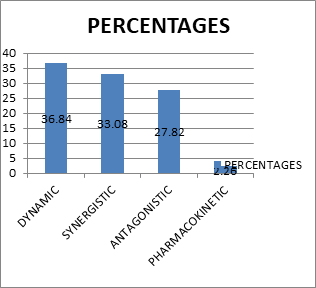
Medication errors were identified as a significant contributor to complications in MI management, emphasizing the importance of proper prescription and drug administration practices. Key findings included: Error Prevalence: Errors in inpatient medication practices were observed in 4.8% to 5.3% of cases, with prescription errors occurring at a rate of 12.3 per 1,000 hospitalizations. Frequent Errors: The most common errors involved omissions, such as failing to prescribe aspirin following an MI, despite established guidelines recommending its universal use for such patients. These omissions were reported in 6.6% to 47% of cases. Impact of Errors: Out of 10,000 medication orders reviewed, 5.3 errors were identified per 100 orders. However, only 0.9% of these errors resulted in adverse drug events. Drug-Drug Interactions: We have evaluated 100 prescriptions. The most common Drug-drug interactions were synergistic, antagonistic, pharmacokinetic, and pharmacodynamic interactions. Drug interactions can reduce a drug’s effectiveness, lead to unforeseen side effects, or enhance the effect of a specific medication.
| Total Drug-Drug Interactions | Synergistic Interactions | Antagonistic Interaction | Pharmacodynamic Interactions | Pharmacokinetic Interactions |
|---|---|---|---|---|
| 66.50% | 33.08% | 27.819% | 36.84% | 2.265% |
Table 1: Drug-drug interactions (66.50%), synergistic (33.08%) antagonistic (27.819%), pharmacokinetic (36.84%), and pharmacodyna
Total Drug-Drug interactions: Total Drug-drug interactions found are 66.50%. Synergistic interactions: Among all positive interactions, there were 33.08% of synergistic interactions. Pharmacokinetic Interactions: In our drug-drug interactions study, out of all positive interactions, we found that there were 2.265% of pharmacokinetic interactions (Metabolic interactions). Antagonistic interactions: Among all positive interactions, there were 27.819% of Antagonistic interactions. Pharmacodynamics Interactions: Among all positive interactions, there were 36.84% of Pharmacodynamic interactions. Among all these drug-drug interactions found, safe/beneficial were and toxic interactions were (33.08%) of synergistic interactions safe/beneficial 15.06% and toxic interactions were 18.02%. Out of 2.265% of pharmacokinetic interactions safe/beneficial were 0.35% and toxic interactions were 1.915%. Among 27.819% of Antagonistic interactions safe/beneficial were 10.819% and toxic interactions were
17%. Out of 36.84% of Pharmacodynamic interactions safe/ beneficial were 22.04% and toxic interactions were 14.8%. Results are depicted in Figures 1 and 2 respectively.
| Disease Name | MI | |||
|---|---|---|---|---|
| Overall ERRORS (%age) | Yes | 32% | Dose | 25% |
| Strength | 18.75% | |||
| Frequency | 31.25% | |||
| Duration | 18.75% | |||
| No | 68% |
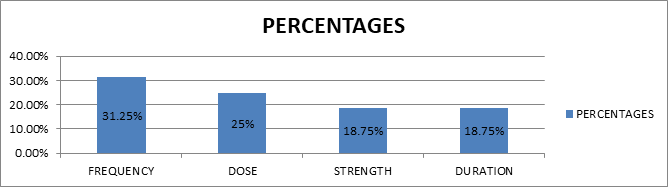
Table 2: Depicts frequency (31.25%), dose (25%), Strength (18.75%) & Duration (18.75%).
This table represents the percentage error of missing dose, missing strength, missing frequency, and missing duration of therapy in the case of myocardial infarction prescriptions. The graph indicates the percentage error of missing dose, missing strength, missing frequency, and missing duration of therapy is 25%, 18.75%, 31.25%, and 18.75%, respectively. The result indicates that the highest percentage of medication error is missing frequency (31.25%). The second highest percentage is missing doses (25%). The least common error is missing duration and strength (18.75%). Results are presented in Figure 3.
Our study highlighted significant issues in the management of myocardial infarction (MI) patients due to prescription errors. A key finding was the 25% rate of missed medication doses, which severely disrupted treatment regimens. Missing doses often resulted in poor disease control and heightened the risk of serious health complications.
Private prescriptions reflected similar concerns, with 25% of patients missing doses. This lack of adherence frequently led to severe complications. Another notable issue was the omission of dosage strength, affecting 18.75% of prescriptions. In such cases, patients often adjusted their medication dosage on their own, either taking too much or too little. This self-regulation could lead to toxic effects or insufficient therapeutic responses, further undermining the effectiveness of treatment and contributing to non- compliance.
The most prevalent error, seen in 31.25% of prescriptions, was the omission of dosing frequency. Properly specifying how often a medication should be taken is essential for ensuring optimal therapeutic outcomes, enhancing patient adherence, and minimizing risks associated with under- dosing or overdosing. Without clear instructions, patients are less likely to follow their prescribed regimens correctly, which jeopardizes the success of treatment.
Another critical oversight was the failure to mention the duration of therapy, reported in 18.75% of prescriptions.
When the duration is not specified, patients may discontinue treatment prematurely, resulting in suboptimal therapeutic effects. Conversely, continuing medication beyond the required period can lead to unnecessary or harmful side effects.
We had selected 200 prescriptions, out of which 50 prescriptions were evaluated. The most common causes of myocardial infarction were hypertension, high cholesterol, diabetes mellitus, and stress. Results are tabulated in Table 3.
| Etiology MI | |||
|---|---|---|---|
| Hypertension | High cholesterol | Stress | DM |
| 29.27% | 28.05% | 19.51% | 23.17% |
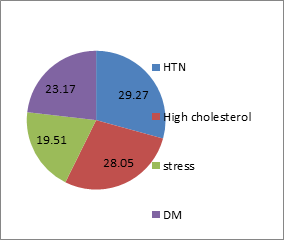
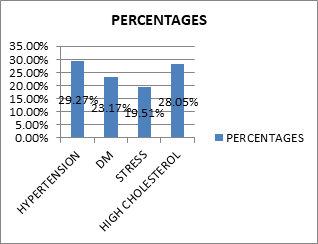
Table 3: Hypertension (29.27%), High cholesterol (28.05 %), Stress (19.51 %) and DM (23.17%).
Myocardial infarction (MI), or heart attack, occurs when blood flow to the heart is blocked by fatty plaques or blood clots in the coronary arteries. Major contributors to MI include: Hypertension (29.27%): High blood pressure leads to arteriosclerosis and plaque buildup, restricting blood flow and increasing the risk of clot formation. High Cholesterol (28.05%): Elevated LDL cholesterol promotes plaque accumulation in arteries, which can rupture and cause blockages. Stress (19.51%): Chronic stress raises blood pressure and heart rate, contributing to artery damage and unhealthy behaviors like smoking or overeating. Diabetes Mellitus (23.17%): Poorly controlled diabetes accelerates atherosclerosis and raises LDL cholesterol, increasing the risk of plaque rupture and clot formation Managing these factors through lifestyle changes and medications is essential to reduce the risk of MI. Myocardial infarction (MI) is caused by risk factors such as hypertension (29.27%), high cholesterol (28.05%), diabetes mellitus (23.17%), and stress (19.51%), all contributing to plaque buildup and artery damage. Managing these factors through lifestyle changes and medications can help reduce the risk of heart attacks and improve heart health. Results are depicted in Figure 4 and Figure 5.
Figure 4 and Figure 5 show the percentages of causes of myocardial infarction: hypertension (29.27%), high cholesterol (28.05%), diabetes mellitus (23.17%), and stress (19.51%).
| Precipitant Drugs | Object Drugs | DDI Type | Effects | Management |
|---|---|---|---|---|
| Aspirin | Captopril/Benazepril/ ramipril/lisinopril | Severe | This may enhance the toxicity of other drugs through pharmacodynamic synergism, potentially leading to renal damage, especially in individuals receiving high doses of aspirin, the elderly, or those who are volume-depleted | Avoid or use alternative |
| Verapamil | Metoprolol/Nebivolol/ bisoprolol | Moderate | Increase toxicicty of one another by unspecified interaction. | Monitor risks of bradycardia and hypertension |
| Amiloride | Spironolactone | Severe | They increases the effect of one another by pharmacodynamic synergism.Both increases k+ serum level. | Do not use the combination, it is contraindicated due to severe hyperkalemia. |
| Olmesartan | Captopril/liosinopril/ ramipril | Severe | increases risks of hypotension, hyperkalemia and renal impairement. | Avoide or use alternative drug. |
| Nitroglycerin PO | Benazepril/Captopril | Moderate | Both increase effect of other by pharmacodynamic synergism. | Monitor,usecaution. Monitor bp as both lower bp. |
| Bisoprolol | Carvedilol/Metoprolol/ Nebivolol | Moderate | These increase serum potassium level. | Use caution,monitor |
| Bisoprolol/Carvedilol/ Metoprolol/Nebivolol | Verapamil | Moderate | Both increase antihypertensive channel blocking and cause hypotension. | Modify therapy / monitor closely. |
| Bisoprolol /Carvedilol/ Metoprolol/Nebivolol | Losartan/amiloride/ Spironolactone | Moderate | Both drugs enhance each other’s effects through pharmacodynamic synergy. There is a risk of fetal harm if administered during pregnancy. | Use caution/monitor |
| Bisoprolol/Carvedilol/ Metoprolol/Nebivolol | Amlodipine | Moderate | Both drugs amplify each other’s effects through pharmacodynamic synergy, with both lowering blood pressure by acting on antihypertensive channels. | Use caution/monitor |
| Bisoprolol | Amiloride/ spironolactone/ Furosemide/ | Moderate | They rise serum potassium level. | Use caution/monitor |
| Bisoprolol /Carvedilol/ | Dobutamine | Moderate | Both drugs amplify each other’s effects through pharmacodynamic synergy, with both lowering blood pressure by acting on antihypertensive channels. | Use caution/monitor |
| Bisoprolol /Carvedilol/ | Olmesartan | Moderate | Beta blockers elevated the effect of olmesartan by pharmacodynamic synergism. | Use caution/monitor |
| Bisoprolol /Carvedilol/ | Aspirin/Amiloride/ spironolactone/ | Moderate | These rise serum potassium level. | Use caution/monitor |
| Verapamil | Atorvastatin | Severe | Verapamil elevates the effect or level of atorvastatin by effecting hepatic/intestinal enzyme CYP3A4 metabolism | Use caution/monitor |
| Verapamil | Clopidogrel | Severe | Verapamil decrease the effect or level of clopidogrel by effecting hepatic/intestinal enzyme CYP3A4 metabolism.. | Use caution/monitor |
| Verapamil | Amiodaron | Severe | Verapamil enhances the effect of amiodarone by influencing the CYP3A4 enzyme involved in hepatic and intestinal metabolism. | Adjust treatment or exercise caution |
| Losartan/olmesartan | Aspirin | Severe | These increase toxicity of one another and cause renal deterioration in elderly and volume depleted persons. | Use caution/monitor |
| Losartan | Furosemide/ hydrochlorothiazide | Moderate | Losartan increase and furosemide and hydrochlorothiazide decline serum potassium level | Adjust treatment or exercise caution |
| Heparin | Aspirin | Moderate | Both elevates anticoagulation. | Adjust treatment or exercise caution |
| Heparin | Losartan | Severe | Heparin can enhance the toxicity of losartan by inhibiting adrenal aldosterone secretion, which may lead to hyperkalemia | Adjust treatment or exercise caution |
| Heparin | Clopidogrel | Severe | Both drugs intensify each other’s effects through pharmacodynamic enhancement, increasing the risk of hemorrhage | Modify therapy/ monitor closely |
| Heparin | Benazepril/captopril/ Ramipril/lisinopril/ olmesartan | Severe | Heparin may increase the toxicity of Benazepril/captopril/Ramipril/lisinopril/ olmesartan | Adjust treatment or exercise caution |
| Amlodipine | Verapamil | Severe | Both increase the antihypertensive channel blocking. | Adjust treatment or exercise caution |
| Aspirin | Bisoprolol /carvedilol / | Severe | Aspirin decrease the effect of Bisoprolol / carvedilol /nebivolol/ metoprolol/ | Adjust treatment or exercise caution |
| Aspirin | Clopidogrel/ enoxaparin/heparin | Moderate | These drugs enhance each other’s toxicity through pharmacodynamic synergy, leading to increased anticoagulation | Monitor closely |
| Aspirin | Furosemide/ hydrochlorothiazide/ dobutamine | Moderate | These may increase the serum potassium level. | Use caution/monitor |
| Aspirin | Spironolactone | Moderate | Aspirin decrease the effect of spironolactone by unspecified interaction. | spironolactone maintenance dose must be titrated to higher dose |
| Aspirin | Olmesartan | Severe | Aspirin decrease the effect of olmesartan by pharmacodynamicantagonism.Long term (<1 week) | Modify therapy/ monitor closely |
| Amiloride | Aspirin | Moderate | Both increase the serum potassium level. | Use caution/monitor |
| Amiloride | Hydrochlorothiazide/ dobutamine | Moderate | Amiloride increase the serum potassium level and hydrochlorothiazide, | Modify therapy / monitor |
| Enoxaparin | Losartan/benazepril / captopril /Ramipril / lisinopril | Severe | Enoxaparin increase the effect of Losartan/ benazepril by pharmacodynamic synergism | Modify therapy / monitor closely |
| Enoxaparin | Aspirin | Severe | Both drugs enhance anticoagulation. Their combined effects are deliberate when prescribed together for the treatment of unstable angina | Modify therapy/ monitor closely |
| Enoxaparin | Clopidogrel | Severe | Either elevates effect of drugs by pharmacodynamic enhanced risk of haemorrhage, | Modify therapy / monitor closely |
| Enoxaparin | Olmesartan | Severe | increase toxicity of olmesartan by pharmacodynamics synergism | Modify therapy/ monitor closely |
| Spironolactone | Furosemide/ hydrochlorothiazide / dobutamine | Severe | Spironolactone increase and furosemide decrease the serum potassium level. | Modify therapy / monitor closely |
| Benazepril /Captopril/ | Aspirin | Severe | Increases toxicity of other and result in renal function | Modify therapy / monitor closely |
| Benazepril | Amiloride/ spironolactone | Moderate | Both increases the serum potassium level. Risk of hyperkalemia and hypotension. | Use caution/ monitor closely |
| Benazepril/lisinopril | Furosemide | Severe | Increase the effect of each other by pharmacodynamic synergism. | Use caution /monitor closely |
| Captopril/Ramipril | Amiloride/ Spironolactone | Severe | Either increase toxicity of other by pharmacodynamic synergism. | Monitor potassium & hypertension |
| Captopril | Spironolactone | Severe | Either increase toxicity of other by pharmacodynamic synergism.. | Use caution/ monitor closely |
| Captopril | Hydrochlorothiazide | Severe | Either increase effect of other by pharmacodynamic synergism. | Monitor blood pressure and renal function. |
| Furosemide | Hydrochlorothiazide | Moderate | Both decline serum potassium level. | Modify therapy / monitor closely |
| Dopamine | Dobutamine | Moderate | Both decrease sedation, increase adrenergic (sympathetic) effect leads to hypertension & rise heart rate. | Modify therapy / monitor closely |
| Hydrochlorothiazide | Metoprolol | Severe | Both drugs may amplify each other’s toxicity, potentially leading to an idiosyncratic reaction such as acute transient myopia | Modify therapy / monitor closely |
| Dobutamine | Furosemide / hydrochlorothiazide | Moderate | Both decrease serum potassium level. | Use caution /monitor closely |
| Olmesartan | Aspirin/ bisoprolol | Moderate | These increase the serum potassium level. | Modify therapy / monitor closely |
| Amiodarone | Atorvastatin | Moderate | Amiodarone increase level or effect of atorvastatin | Use caution / monitor closely |
| Amiodarone | Bisoprolol /metoprolol | Moderate | Both increase the action of each other by pharmacodynamic synergism. | Use caution /monitor closely |
| Amiodarone | Verapamil | Moderate | Amiodarone increase the effect or level of verapamil by pharmacodynamic synergism | Use caution /monitor closely |
| Amiodarone | Captopril/benazepril | Moderate | Both increase the effect of pharmacodynamic synergism. | Use caution /monitor closely |
| Amiodarone | Hydrochlorothiazide | Moderate | Amiodarone enhances the effect of hydrochlorothiazide by competing with it for renal tubular clearance due to their basic cationic properties. | Use caution /monitor closely |
| Amiodarone | Losartan | Moderate | Amiodarone elevates the effect or concentration of losartan by influencing the hepatic enzymes CYP2C9/10, potentially inhibiting the conversion of losartan into its active metabolite, E-3174. | Monitor patient therapeutic response to determine dosage of losartan. |
| Amiodarone | Carvedilol /nebivolol / metoprolol | Severe | Amiodarone enhances the effect of these drugs by influencing the hepatic enzyme CYP2D6. It should be used cautiously in patients taking beta-adrenergic blockers, especially if there is a suspected underlying sinus node dysfunction, such as bradycardia or sick sinus syndrome, or if partial AV block is present. | Monitor for signs of bradycardia or heart lock when amiodarone and beta adrenergic blocker are coadministered. |
Table 4: “Drug-Drug Interactions: Precipitant Drugs, Object Drugs, Types, Effects, Management of (MI).
Drug combinations like Clopidogrel + Aspirin & Aspirin + Enoxaparin prevent clots, while Amiodarone + Beta- blockers regulate rhythms. ACE inhibitors + Statins control hypertension and cholesterol, improving heart health. Results are tabulated in Table 5.
| Combination of Drugs | Occurrences |
|---|---|
| Clopidogrel+Aspirin | 49 |
| Aspirin+Enoxaparin | 46 |
| Aspirin + ACEI | 45 |
| Nitroglycerin+ACEI | 43 |
| Amiodarone +B-blocker | 35 |
| Bisoprolol+ Amlodipine | 20 |
| Atorvastatin+Verapamil | 20 |
| Olmesartan+ACEI | 15 |
| Aspirin + Benazepril | 15 |
Table 5: Most Prevalence of Drug-Drug Interactions occurrences in Cardiovascular Therapy.
Discussion
Myocardial Infarction (MI) is a critical and potentially fatal condition resulting from reduced or obstructed blood flow to the heart. It is the leading cause of death worldwide, responsible for approximately 17.3 million fatalities annually, a figure projected to rise to over 23.6 million by 2030. The current study was conducted on 100 MI patients of different genders (males and females) in district Poonch, combined military hospital (CMH) Rawalakot and then prescriptions are evaluated. Total Drug-Drug interactions found are 66.50%. Out of all positive interactions, there were 33.08% Synergistic interactions. In our drug-drug interactions study, out of all positive interactions, we found that there were 2.265% pharmacokinetic interactions. Out of all positive interactions, there were 27.819% of Antagonistic interactions. Out of all positive interactions, there were 36.84% of Pharmacodynamics interactions. The percentages of dose errors found were: The highest percentage of medication error is missing frequency (31.25%). The second highest percentage is missing doses (25%). The least common error is missing duration (18.75%) and strength (18.75%). High cholesterol level: Atherosclerosis is primarily driven by dyslipidemia, marked by high cholesterol levels, which is a key risk factor for cardiovascular conditions. Elevated low-density lipoprotein (LDL) levels and reduced high-density lipoprotein (HDL) levels are strongly linked to the onset of myocardial infarction (MI) and stroke. The leading cause of MI is the partial or total obstruction of the epicardial coronary arteries, usually caused by plaques that are vulnerable to rupture or breakdown [7]. This disease process generally starts in early adulthood and is characterized by lipid buildup in the arterial walls, accompanied by inflammation and vascular injury. Over time, certain plaques become more unstable and inflamed, increasing the likelihood of rupture. When rupture occurs, the exposed sub-endothelial matrix and plaque material come into contact with the blood, triggering the formation of occlusive blood clots. This chain of events manifests clinically as MI, with symptoms including chest pain (angina), damage to heart muscle cells, and impaired heart function. Additionally, other coronary artery disorders, such as plaque erosion or spontaneous coronary artery dissection, can also lead to MI. However, their prevalence compared to plaque rupture is unclear and remains a subject of debate, largely due to the limited availability of autopsy research [10]. Diabetes Mellitus: Type 2 diabetes is a long-term condition marked by the body’s inability to produce enough insulin or efficiently use it. This disorder arises from a combination of hereditary factors and environmental influences. Several risk factors for type 2 diabetes overlap with those for coronary artery disease (CAD), such as advanced age, hypertension, abnormal lipid levels, obesity, sedentary lifestyle, and stress. The growing prevalence of diabetes significantly increases the associated risk of CAD. Diabetes mellitus is a well-recognized contributor to cardiovascular diseases, raising the risk of coronary heart disease by two to four times. On average, people with diabetes have a shortened life expectancy of approximately eight years due to higher death rates. Over 80% of fatalities linked to coronary artery disease and 75% of hospitalizations in diabetic individuals are attributed to this condition. Diabetes heightens the risk of myocardial infarction by accelerating the progression of atherosclerosis, adversely impacting lipid levels, and fostering the formation of atherosclerotic plaques. Regarding myocardial infarction, diabetes is a significant risk factor and is frequently associated with a greater mortality rate in diabetic patients compared to those without diabetes [3]. Stress: Chronic stress, social isolation, and anxiety significantly elevate the risk of heart attack and stroke. Acute psychological stress is also strongly linked to an increased risk of coronary heart disease. Research has shown that intense grief, such as that experienced after losing a loved one, can trigger the onset of myocardial infarction. During periods of stress, the sympathetic nervous system becomes activated, leading to a rise in catecholamine levels. This, in turn, increases oxygen demand in the heart due to elevated blood pressure, heart rate, and myocardial contractility. The added strain on the heart may ultimately result in myocardial infarction. The causes of myocardial infarction have been quantified as follows: hypertension accounts for 29.27%, high cholesterol for 28.05%, diabetes mellitus for 23.17%, and stress for 19.51%. Hypertension: Both systolic and diastolic hypertension significantly increase the risk of myocardial infarction, with higher blood pressure levels correlating to greater risk. Elevated systolic and diastolic pressure contribute to the development of atherosclerosis in coronary arteries, which can lead to heart attacks. The relationship between hypertension and myocardial infarction is particularly strong, especially in older adults, where hypertension is responsible for nearly 70% of cardiac diseases and poses severe risks to heart health [7]. Adhering to prescribed medication regimens and adopting lifestyle changes, such as improved diet, regular exercise, and stress management, can effectively control hypertension and substantially lower the risk of myocardial infarction Future Prospects This study highlights key areas for improving myocardial infarction (MI) care in Azad Kashmir. Future efforts should focus on: Standardized Protocols to Developed uniform diagnostic and treatment guidelines to streamline MI management across healthcare systems. Education and Awareness Train healthcare professionals on MI etiology and error prevention. Raise public awareness about cardiovascular risk factors and preventive measures. Healthcare System Strengthening Enhance infrastructure and resource allocation, especially in rural areas. Establish efficient referral networks for timely MI diagnosis and treatment. Technological Integration Implement electronic prescribing systems to minimize medication errors. Use telemedicine to improve specialist care access in remote regions. Research and Policy Conduct ongoing studies to assess interventions and understand MI trends. Develop region-specific public health policies for prevention and improved care. By addressing these areas, the study can guide interventions to reduce MI-related morbidity and mortality, enhancing cardiovascular health in Azad Kashmir. Conclusion: This study highlights the multifactorial etiology and significant prescription errors contributing to the burden of myocardial infarction (MI) in different healthcare systems of Azad Kashmir. The key findings can be summarized as follows: Etiological Factors: Adjustable risk factors e.g. high blood pressure, diabetes, abnormal cholesterol levels, smoking, and inactivity, were the main contributors to myocardial infarction (MI). Inherited factors, including age, sex, and family history, also had a considerable influence on the risk. Additionally, socioeconomic disparities impacted people’s ability to access preventive healthcare and obtain timely treatment. Healthcare System Comparison: Significant differences in the quality of care were observed between public, private, and traditional healthcare systems. Public healthcare facilities often face resource limitations and a lack of skilled personnel, leading to delays in diagnosis and treatment. Private healthcare offered better access but at a higher cost, limiting affordability. Traditional healthcare systems lacked scientific validation and were associated with delayed patient referrals. Recommendations for Improvement: Enhanced Education: Public awareness campaigns focusing on lifestyle modifications and risk factor control can help reduce MI incidence. Capacity Building:
Training healthcare providers on evidence-based treatment protocols and minimizing prescription errors is essential. Policy Development: Strengthening healthcare infrastructure, improving resource allocation, and integrating traditional medicine into evidence-based practices can address disparities. Monitoring Systems: Implementation of electronic health records and prescription monitoring tools can reduce errors and improve patient outcomes. This study underscores the need for a unified, multidisciplinary approach to prevent MI and improve treatment outcomes in Azad Kashmir. Addressing the systemic gaps in healthcare delivery and emphasizing preventive measures can significantly reduce the burden of MI in the region. Prescription errors; A notable frequency of prescription mistakes was found, especially related to incorrect drug choices, incorrect dosages, and the overuse of multiple medications (polypharmacy). Issues such as improper administration of antiplatelet and anticoagulant medications, inadequate lipid control, and non-compliance with clinical guidelines were widespread across different healthcare settings.
Conclusion
This study highlights the multifactorial etiology and significant prescription errors contributing to the burden of myocardial infarction (MI) in different healthcare systems of Azad Kashmir. The key findings can be summarized as follows: Etiological Factors: Adjustable risk factors e.g. high blood pressure, diabetes, abnormal cholesterol levels, smoking, and inactivity, were the main contributors to myocardial infarction (MI). Inherited factors, including age, sex, and family history, also had a considerable influence on the risk. Additionally, socioeconomic disparities impacted people’s ability to access preventive healthcare and obtain timely treatment. Healthcare System Comparison: Significant differences in the quality of care were observed between public, private, and traditional healthcare systems. Public healthcare facilities often face resource limitations and a lack of skilled personnel, leading to delays in diagnosis and treatment. Private healthcare offered better access but at a higher cost, limiting affordability. Traditional healthcare systems lacked scientific validation and were associated with delayed patient referrals. Recommendations for Improvement: Enhanced Education: Public awareness campaigns focusing on lifestyle modifications and risk factor control can help reduce MI incidence. Capacity Building: Training healthcare providers on evidence- based treatment protocols and minimizing prescription errors is essential. Policy Development: Strengthening healthcare infrastructure, improving resource allocation, and integrating traditional medicine into evidence- based practices can address disparities. Monitoring Systems: Implementation of electronic health records and prescription monitoring tools can reduce errors and improve patient outcomes. This study underscores the need for a unified, multidisciplinary approach to prevent MI and improve treatment outcomes in Azad Kashmir. Addressing the systemic gaps in healthcare delivery and emphasizing preventive measures can significantly reduce the burden of MI in the region. Prescription errors; A notable frequency of prescription mistakes was found, especially related to incorrect drug choices, incorrect dosages, and the overuse of multiple medications (polypharmacy). Issues such as improper administration of antiplatelet and anticoagulant medications, inadequate lipid control, and non-compliance with clinical guidelines were widespread across different healthcare settings.
Recommendations
- Raising public awareness about lifestyle changes and risk management.
- Training healthcare professionals in evidence-based practices to reduce errors.
- Strengthening healthcare infrastructure and resource allocation.
- Integrating validated traditional practices into mainstream healthcare.
- Utilizing electronic health records and prescription monitoring tools to enhance care quality. A unified, multidisciplinary strategy addressing healthcare gaps and focusing on prevention can significantly alleviate the MI burden in the region.
Conflict of Interest
The authors find no conflict of interest.
References
-
Vaisrub S (1976) Subendocardial infarction: a prognostic paradox. Jama 235(9): 943-944.
-
Newby ED, Wright AR, Labinjoh C, Ludlam AC, Fox AAK, et al. (1999) Endothelial dysfunction, impaired endogenous fibrinolysis and cigarette smoking. Circulation 99(11): 1411-1415.
-
Connor BE, Khaw KW (1988) Diabetes mellitus an independent risk factor for stroke. American journal of epidemiology 128(1): 116-123.
-
Anurag B, Anukr S, Paru R (2015) Acute Complications of Myocardial Infarction the Current Erain. Journel of Investigting Medicine 844-855.
-
Thygesen K, Alpert SJ, Chaitman RB, Bax JJ, Morrow AD, et al. (2018) Fourth universal definition of Myocardial infarction. Circulation 138.
-
Timmis AD (1990) Early diagnosis of acute myocardial infarction. BMJ (Clinical research ed.), 301(6758): 941- 942.
-
Pedrinelli R, Ballo P, Fiorentini C, Denti S, Galderisi M, et al. (2012) Hypertension and acute myocardial infarction. Journal of cardiovascular medicine 13(3): 194-202.
-
Gangulay K, Goshal P, Saha S, De S (2015) Acute Myocardial Infarction in the Young. Indian Perspective, pp: 297-300.
-
Laslett LJ, Alagona P, Clark BA, Drozda JP, Saldivar F, et al. (2012) The Worldwide Environment of Cardiovascular Disease: Prevalence, Diagnosis, Therapy, and Policy Issues. American College of Cardiology 60: 1-49.
-
Healy B (1990) Endothelial cell dysfunction. Journal of the American college of Cardiology 16(2): 357-358.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study
- Pheochromocytoma: Therapeutic Agents against the Disease and Chromatographic Methods for their Determination in Biological Fluids