Clinical Evaluation of Patients Suffering from Breast Cancer & Determination of Treatment Therapies and Better Strategies Related to Breast Cancer
Breast cancer is the most prevalent cancer among women globally, with Pakistan reporting one of the highest rates in Asia. This disease typically involves abnormal growths in the breast, originating from either connective tissues or epithelial cells. A study conducted in Rawalakot, Azad Jammu, and Kashmir aimed to explore the prevalence of breast cancer, assess diagnostic and treatment approaches, and identify strategies for prevention. The research spanned six to eight months, during which data were collected through a detailed questionnaire and medical records from the Combined Military Hospital (CMH) and the local community. The questionnaire focused on patients' medical history, demographic details, diagnostic methods, treatment strategies, and preventive measures. The study found that most breast cancer patients were aged 41 to 60, with 66% being married women. Invasive breast cancer accounted for 70% of cases, while 30% were classified as non-invasive. Additionally, 66% of the cases involved the right breast. Genetic factors were linked to 64% of the cases, with the remaining attributed to other causes. Biopsy and mammography were the most frequently used diagnostic techniques. Hormonal therapies, including tamoxifen and estrone, were commonly prescribed as part of post-surgical treatment plans. However, despite these interventions, 68% of patients experienced a recurrence of breast cancer following surgery. These findings highlight the critical need for improved awareness of breast cancer, emphasizing early detection and prevention. Educational campaigns and initiatives promoting regular self-examinations could significantly reduce disease severity and improve outcomes. Timely diagnosis and appropriate treatment are essential for enhancing survival rates and quality of life for women affected by this disease. The recurrence rate can be reduced by adjuvant therapy (i.e. chemotherapy, hormone therapy, targeted therapy, and radiation therapy), healthy lifestyle choices (i.e. healthy diet, exercise, weight management, alcohol reduction, smoking cessation) and ongoing monitoring.
Introduction
Breast cancer is the most common malignancy among women worldwide, with approximately 570,000 cases reported annually. In Asia, Pakistan has the highest incidence, with around 90,000 cases each year [1, 2, 3]. Cancer is characterized by the uncontrolled growth of cells, which proliferate to form a mass or lump called a tumor. The type of cancer is named based on the part of the body where the tumor originates. Tumors are classified as benign (localized and non-invasive) or malignant (capable of spreading to other parts of the body). Breast cancer, also known as breast carcinoma, results from the unchecked growth of epithelial cells in the breast’s ducts or lobules. This malignancy disrupts normal cellular function and can originate in either the ducts or lobules of the breast tissue leading to metastasis in the entire breasts [4].
The primary types of breast cancer include: • Infiltrating Ductal Carcinoma (IDC): Originating in the epithelial lining of large or intermediate ducts, this accounts for 80% of cases. • Lobular Infiltrating Carcinoma (LIC): Arises from the epithelium of terminal ducts and lobules, representing 10% of cases. • Inflammatory Breast Cancer: A rare type (3%) in which cancerous cells block lymph vessels in the breast skin, causing inflammation. • Paget’s Disease of the Breast: Extremely rare (1%) and often misdiagnosed as dermatitis.
Breast cancer progresses through five stages: **
- Stage 0: Non-invasive cancer confined to the ducts or lobules without invading surrounding tissues.
- Stage I: A small tumor (0.2–2 mm) localized in the lymph nodes.
- Stage II: Tumor spread to 1–3 axillary lymph nodes or areas above and below the collarbone, but still non- metastatic.
- Stage III: Cancer affecting the chest wall, causing swelling or ulceration; includes inflammatory breast cancer.
- Stage IV:** The most advanced stage, where cancer metastasizes to distant organs such as the lungs, liver, brain, or bones
- Symptoms of breast cancer include a firm, painless lump in the breast (occasionally painful), changes in breast shape, redness, swelling, tenderness, nipple discharge, or lumps in the armpit [4].
- The exact cause of breast cancer remains unclear, but several risk factors have been identified: **
- Age: The risk increases with age.
- Family History: The risk is greatly increased with a family history of breast cancer, and the risk increases with the number of afflicted relatives and the age of diagnosis [5].
- Genetic Factors: Mutations in BRCA1 and BRCA2 genes are strongly associated with the disease [6, 7].
- Hormonal Factors: Early menarche or late menopause contributes to increased risk [8, 9].
- Lifestyle Factors:** Alcohol consumption, tobacco use, and radiation exposure are associated with higher risk [10, 11]. Early detection, awareness of risk factors, and timely intervention are essential for improving outcomes and reducing breast cancer prevalence.
Pathogenesis
Breast carcinoma is a type of cancer that can either be non-invasive or invasive, originating from the epithelial cells within the breast tissue. The majority of breast cancers are either ductal or lobular, accounting for over 90% of cases. This cancer tends to spread through lymphatic vessels and the bloodstream, and it takes about five years for it to become large enough to be felt as a lump. As the tumor grows, it invades nearby structures, such as the lobules, the connective tissue, and the lymphatic vessels of the breast, leading to ulceration and skin infiltration. The tumor continues to grow and can spread to other distant parts of the body. One key characteristic of these cancerous cells is their reliance on hormone receptors, particularly estrogen and progesterone, which fuel their growth. The prognosis for breast carcinoma largely depends on factors such as the size of the tumor, whether lymph nodes are affected, the grade of the tumor, and whether it has metastasized to other parts of the body [12].
Diagnosis and Treatment of Breast Cancer: Diagnosis of breast carcinoma at the early stage is essential for preventing the prognosis of the disease. Certain methods and technologies have been used for the detection and diagnosis of breast carcinoma, including BSE (breast self-examination)biopsy, ultrasound, immunologic test, mammography and thermography Treatment of breast cancer includes surgery, radiation [13, 14], and systematic therapy (chemotherapy(drug used to target cancer, hormonal therapy and targeted therapy) [15, 16] Early Breast Cancer Trialists’ [17, 18, 19, 20].
Literature Review
Breast cancer is increasingly becoming a primary global health concern, with over a million women diagnosed with the disease each year and more than 410,000 women dying from it annually [21, 22]. It is the most common form of cancer among women, representing nearly one-third of all cancer cases and cancer-related deaths worldwide. After lung cancer, breast cancer is the second most common cause of cancer mortality. The chance of developing invasive breast cancer is about 12.6% [23]. Mortality rates are exceptionally high among women who are either very young (under 35) or older (over 75) [24].
Many women diagnosed with breast cancer struggle with a lack of understanding about the tumor’s specific characteristics and the biology of their disease, which makes it harder to manage their treatment effectively [25]. The rate of breast cancer varies greatly by region. For example, Eastern Africa has an incidence rate of 19.3 cases per 100,000 women, while Western Europe has a much higher rate of 89.7 cases per 100,000 women [26]. In Asia, women are more likely to have estrogen receptor-negative breast cancer, and about 15% of sporadic breast cancer cases in Caucasian women related to BRCA1 have a basal-like phenotype.
Each year, over a million new cases of breast cancer are diagnosed worldwide, including in countries such as Hong Kong, Singapore, China, Brazil, South Africa, Zimbabwe, Uganda, North Africa (e.g., Algiers), and several countries in South Asia, including India and Pakistan Among Asian countries, Pakistan has the highest rate of breast cancer, with nearly 34.6% of all female cancer cases being breast cancer [27]. In the Kashmir region, breast cancer is the most prevalent cancer among women, particularly those aged between 45 and 50. In these cases, about 65.1% of tumors are found to be between 2 and 5 cm in size [28].
Methodology
The research utilized a structured questionnaire to collect comprehensive data on patients’ conditions and treatment. The questionnaire covered socio-demographic details (age, marital status, occupation) lifestyle factors (smoking, alcohol use & physical activity), medical history, laboratory test results, and treatment side effects. Additionally, it explored the continuity of treatment post-surgery and any recurrence of breast cancer. The aim was to gain a thorough understanding of treatment trends and patient experiences, as well as to identify any gaps in awareness and care. This data contributed to improving early diagnosis and treatment protocols.
The research used a structured questionnaire to gather data on various aspects of patient’s conditions and treatment. It covered socio-demographic details (age, marital status, occupation) lifestyle factors (smoking, alcohol use & physical activity), medical history, lab test results, and treatment side effects. The questionnaire also explored how patients continued treatment post-surgery and whether they experienced any recurrence of breast cancer. This comprehensive approach aimed to provide insights into patient experiences and treatment adherence. A cross- sectional study was conducted using random sampling to obtain a diverse and representative sample from the local community.
The study aimed to evaluate breast cancer treatment trends, patient awareness, and early detection practices. Data was collected from patients’ prescriptions, medical records, and case reports with prior consent, ensuring confidentiality in line with ethical standards. Breast cancer develops when epithelial cells in the breast’s ducts or lobules grow uncontrollably, leading to tumor formation. It can begin in (ductal carcinoma) or lobules (lobular carcinoma) and spread to surrounding tissues. The disease remains a significant health risk and a leading cause of cancer-related deaths in women.
Results
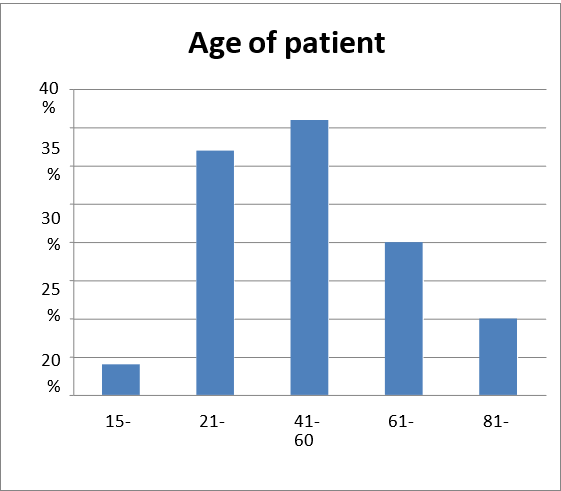
| Age of Patient | Disease Occurrence Rate |
|---|---|
| 15-20 years | 4% |
| 21-40 years | 32% |
| 41-60 years | 36% |
| 61-80 years | 20% |
| 80-100 years | 10% |
Table 1: Age of patients & disease occurrences.
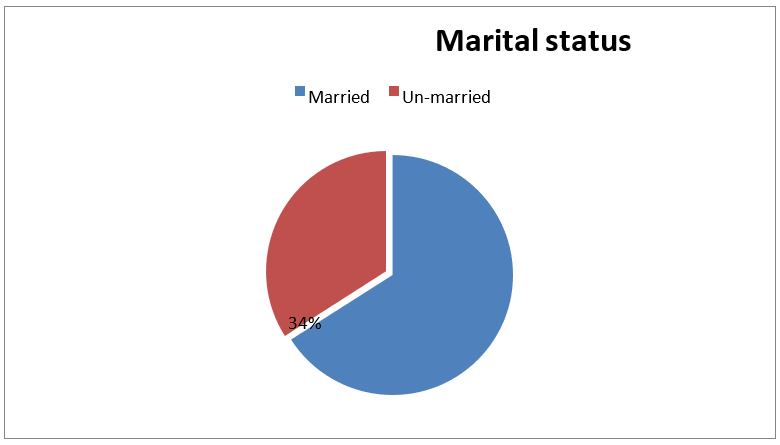
| Disease Occurrence Rate | |
|---|---|
| Married | 62% |
| Unmarried | 32% |
Table 2: Marital status and disease occurrence rate related to breast cancer.
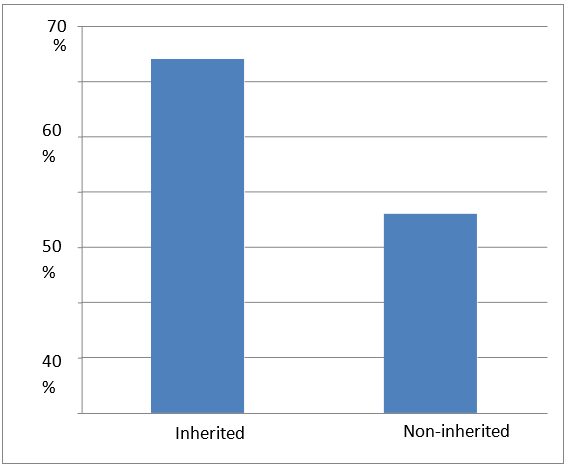
| Disease Occurrence Rate | |
|---|---|
| Inherited | 64% |
| Non-inherited | 36% |
Table 3: Inheritance status & disease occurrence.
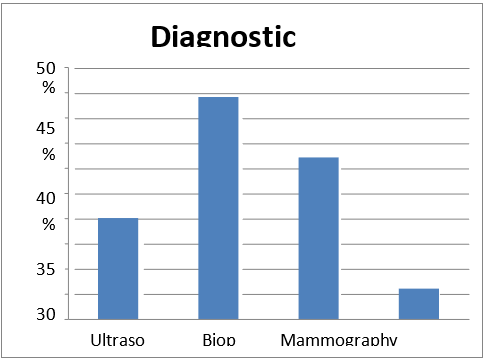
| Diagnostic Method | Diagnosis Rate |
| Ultrasound | 20% |
| Biopsy | 44% |
| Mammogram | 32% |
| Immune test | 6% |
Table 4: Diagnostic method & rate.
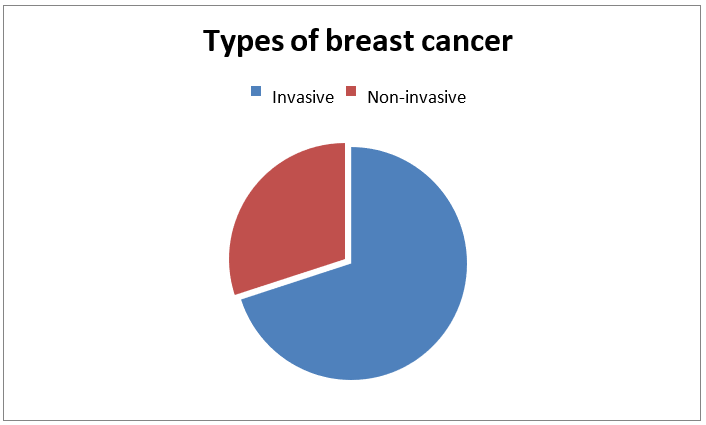
| Disease Occurrence Rate | |
|---|---|
| Invasive | 85% |
| Non-invasive | 15% |
Table 5: Type of breast cancer and disease occurrence rate.
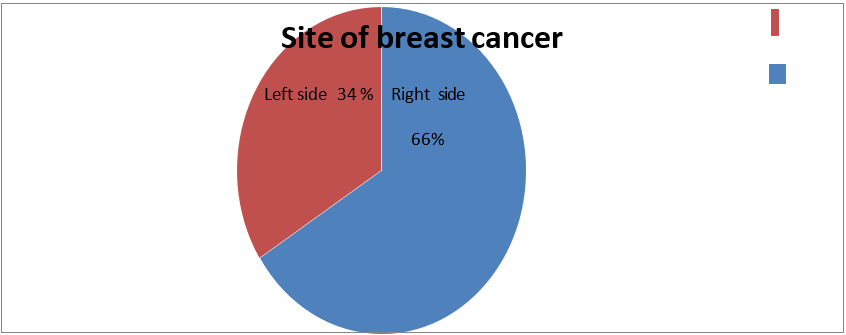
| Disease Occurrence Rate | |
|---|---|
| Right side | 66% |
| Left side | 34% |
Table 6: Site of breast cancer disease occurrence rate right and left side.
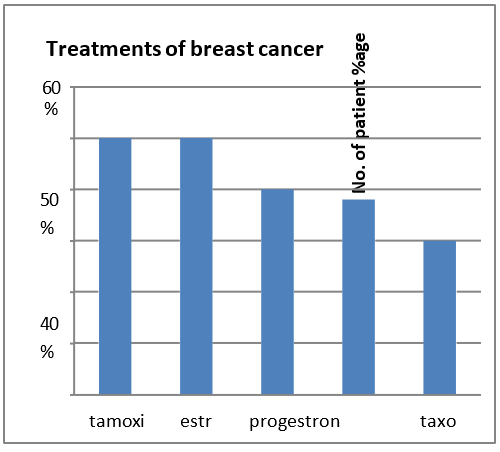
| Types of treatment for breast cancer | Prescription rate |
| Tamoxifen | 50% |
| Estron | 50% |
| Progesterone | 40% |
| Anastrazole | 38% |
| Taxones | 30% |
Table 7: Breast cancer treatment.
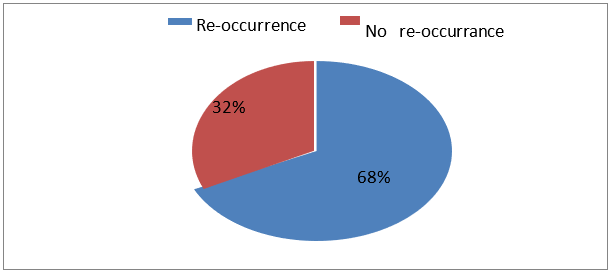
| No. of patients | |
|---|---|
| Reoccurrence | 68% |
| No reoccurrence | 32% |
Table 8: Reoccurrence & No reoccurrence of disease and Number of patients.
Discussion
Breast cancer, a leading cause of cancer-related death, exhibits distinct patterns in its occurrence and response to treatment across different demographic, clinical, and diagnostic factors. This study highlights key findings regarding patient age, marital status, family history, diagnostic approaches, cancer type, and treatment strategies, all of which are crucial for understanding the disease’s prevalence and recurrence. The highest incidence of breast cancer was observed in individuals aged 41-60 years (36%), followed by those aged 21-40 years (32%). These findings suggest that breast cancer primarily affects middle-aged women, with a lower incidence in older age groups. Only 10% of cases were found in those aged 80-100 years, indicating that the disease is either more aggressive or more readily detected in younger to middle-aged women. Married individuals had a significantly higher incidence of breast cancer (62%) compared to unmarried individuals (32%). While this could be due to social, lifestyle, or genetic factors, further investigation is needed to determine the reasons behind this discrepancy. It may also suggest that married individuals are more likely to seek medical attention or are diagnosed at later stages of the disease. A significant 64% of patients reported a family history of breast cancer, indicating that inherited genetic mutations, such as those in BRCA1 and BRCA2, are important risk factors. However, 36% of cases were non-inherited, suggesting that other factors like lifestyle, environmental exposures, and hormonal influences contribute to the onset of the disease.
Biopsy (44%) and mammography (32%) were the most commonly used methods for diagnosing breast cancer, followed by ultrasound (20%) and immune tests (6%). These results emphasize that while mammograms remain a key diagnostic tool, biopsies are essential for confirming malignancy and staging the cancer. The limited use of immune tests suggests that this diagnostic approach is still evolving and not yet widely adopted in clinical settings. The majority of cases were diagnosed as invasive breast cancer (85%), which is more difficult to treat due to its ability to spread beyond the breast tissue. Non-invasive breast cancer, accounting for 15% of cases, is less aggressive and remains confined to the ducts or lobules. Early detection of non-invasive cancer is crucial for better treatment outcomes. Breast cancer was more commonly found in the right breast (66%) than in the left (34%). The reasons for this difference are not fully understood, but it may be related to anatomical or hormonal factors. More research is needed to explore the underlying causes of this discrepancy. Tamoxifen and Estron (50% each) were the most frequently prescribed treatments, reflecting their widespread use in hormone receptor-positive breast cancer. Other treatments, such as progesterone (40%) and anastrazole (38%), were also commonly prescribed, while taxanes (30%) had a lower prescription rate. These findings underscore the importance of hormonal therapies in managing breast cancer and highlight the continued use of targeted treatments alongside newer options like immunotherapy. A significant portion of patients (68%) experienced breast cancer recurrence, highlighting the need for ongoing monitoring and adjustments to treatment plans. While 32% of patients did not experience recurrence, this points to the effectiveness of certain treatment regimens. However, it also underscores the need for continued research to improve long-term survival and reduce the risk of recurrence. This study reveals the complexities of breast cancer and identifies key factors influencing its occurrence, treatment, and recurrence. By further investigating the relationships between these variables, clinicians and researchers can develop more personalized, effective strategies for managing the disease. Statistical analyses that consider age, family history, diagnostic methods, and treatment options are essential for optimizing patient care and improving outcomes. Future studies should explore the underlying reasons for observed trends and focus on enhancing early detection and treatment strategies.
Conclusion
In conclusion, this study offers important insights into the occurrence, clinical characteristics, and treatment outcomes of breast cancer in Rawalakot. The results highlight a high incidence of breast cancer among middle-aged women, with invasive ductal carcinoma being the most commonly diagnosed type. Early-stage cases showed positive responses to standard treatments, while more advanced cases had a higher recurrence rate, suggesting that more advanced and personalized treatment approaches are needed. The study also points to a potential genetic influence, as many cases were linked to hereditary factors within the population. Furthermore, limited access to specialized diagnostic tools and treatment options has been identified as a significant barrier to early detection and effective management of the disease. These findings stress the need for improving healthcare infrastructure in Rawalakot, particularly by expanding access to diagnostic services, establishing comprehensive early screening programs, and ensuring the availability of advanced treatment options. Raising public awareness about early detection and the importance of regular screenings is also crucial. Moreover, further research into the genetic aspects of breast cancer could lead to the development of more targeted prevention and treatment strategies. Finally, investing in the training of healthcare professionals in breast cancer management will be essential to improve patient outcomes. Addressing these gaps will help enhance the overall management of breast cancer in Rawalakot and similar regions.
References
-
Youlden DR, Cramb SM, Dunn NA (2012) The descriptive epidemiology of female breast cancer: An international comparison of screening, incidence, survival and mortality. Cancer Epidemiology 36(3): 237-248.
-
Saeed, S., & J, N (2020) Epidemiology of breast cancer in Pakistan: A review. Asian Pacific Journal of Cancer Prevention 21(1): 1-6.
-
Schwartz GF, Hughes KS, Lynch HT, Fabian CJ, Fentiman IS, et al. (2008) Proceedings of the International Consensus Conference on Breast Cancer Risk, Genetics, & Risk Management, April, 2007. Cancer 113(10): 2627-2637.
-
Shah R (2014) Pathogenesis, prevention, diagnosis and treatment of breast cancer. World Journal of Clinical Oncology 5(3): 283.
-
National IFHACE (2021) Breast cancer: managing family history. Clinical Knowledge Summaries.
-
Tutt A, Ashworth A (2020) The relationship between BRCA1/2 and breast cancer. Nature Reviews Cancer 20(12): 789-804.
-
Turnbull C, Rahman N (2008) Genetic Predisposition to Breast Cancer: Past, Present, and Future. Annual Review of Genomics and Human Genetics 9(1): 321-345.
-
Li SY, Wu J, Ding L (2020) The impact of early menarche and late menopause on breast cancer risk: A systematic review and meta-analysis. Frontiers in Oncology 10: 853.
-
Kelsey JL, Gammon MD, John EM (1993) Reproductive Factors and Breast Cancer. Epidemiologic Reviews 15(1): 36-47.
-
Clemons M, Loijens L, Goss P (2000) Breast cancer risk following irradiation for Hodgkin’s disease. Cancer Treatment Reviews 26(4): 291-302.
-
Secretan B, Straif K, Baan R, Grosse Y, El Ghissassi F, et al. (2009) A review of human carcinogens—Part E: tobacco, areca nut, alcohol, coal smoke, and salted fish. The Lancet Oncology 10(11): 1033-1034.
-
Kruper L, Holt A, Xu XX, Duan L, Henderson K, et al. (2011) Disparities in reconstruction rates after mastectomy: patterns of care and factors associated with the use of breast reconstruction in Southern California. Ann Surg Oncol 18(8): 2158-2165.
-
Beitsch PD, Shaitelman SF, Vicini FA (2011) Accelerated partial breast irradiation. Journal of Surgical Oncology 103(4): 362-368.
-
Whelan TJ, Pignol J, Levine MN, Julian JA, MacKenzie R, et al. (2010) Long-Term Results of Hypofractionated Radiation Therapy for Breast Cancer. New England Journal of Medicine 362(6): 513-520.
-
Mauri D, Pavlidis N, Ioannidis JPA (2005) Neoadjuvant Versus Adjuvant Systemic Treatment in Breast Cancer: A Meta-Analysis. JNCI Journal of the National Cancer Institute 97(3): 188-194.
-
von Minckwitz G, Untch M, Blohmer J, Costa SD, Eidtmann H, et al. (2012) Definition and Impact of Pathologic Complete Response on Prognosis After Neoadjuvant Chemotherapy in Various Intrinsic Breast Cancer Subtypes. Journal of Clinical Oncology 30(15): 1796-1804.
-
(2001) Familial breast cancer: collaborative reanalysis of individual data from 52 epidemiological studies including 58 209 women with breast cancer and 101 986 women without the disease. The Lancet 358(9291): 1389-1399.
-
Romond EH, Perez EA, Bryant J, Suman VJ, Geyer CE, et al. (2005) Trastuzumab plus Adjuvant Chemotherapy for Operable HER2-Positive Breast Cancer. New England Journal of Medicine 353(16): 1673-1684.
-
National IFHACE (2025) Early and locally advanced breast cancer: diagnosis and management. NICE Guideline NG101.
-
European SFMO (2024) Early breast cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Annals of Oncology 35(2): 159-182.
-
Bray F, Laversanne M, Weiderpass E, Soerjomataram I (2021) The ever‐increasing importance of cancer as a leading cause of premature death worldwide. Cancer 127(16): 3029-3030.
-
Coughlin SS, Ekwueme DU (2009) Breast cancer as a global health concern. Cancer Epidemiology 33(5): 315- 318.
-
Smith HO, Kammerer-Doak DN, Barbo DM, Sarto GE (1996) Hormone replacement therapy in the menopause: a pro opinion. CA: A Cancer Journal for Clinicians 46(6): 343-363.
-
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, et al. (2021) Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians 71(3): 209-249.
-
Ginsburg OM, Love RR (2011) Breast Cancer: A Neglected Disease for the Majority of Affected Women Worldwide. The Breast Journal 17(3): 289-295.
-
Ferlay J, Shin H, Bray F, Forman D, Mathers C, et al. (2010) Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. International Journal of Cancer 127(12): 2893-2917.
-
Bhurgri, Y (2004) Karachi Cancer Registry Data-- implications for the National Cancer Control Program of Pakistan. Asian Pac J Cancer Prev 5(1): 77-82.
-
Siegel R, Naishadham D, Jemal A (2013) Cancer statistics, 2013. CA: A Cancer Journal for Clinicians 63(1): 11-30.
- Gallic and Citric Acid Present in the Peels of Tropical Fruits as an Alternative in the Fight against Cancer
- Treating the Forehead Lines with Combination of Forehead and Glabellar Botulinum Toxin Among Japanese Patients
- Medieval Recipes by Al-Zahrāwī for Heart Palpitations Treatment
- Etiology and Prescription Errors of Myocardial Infarction in Different Health Care Systems of Azad Kashmir
- Early Diagnosis and Multidisciplinary Management of Turner Syndrome: A Paediatric Case Study
- Pheochromocytoma: Therapeutic Agents against the Disease and Chromatographic Methods for their Determination in Biological Fluids