Resistin -420 C>G Polymorphism in Female Patients of Acne in Pakistan
Acne vulgaris is an inflammatory skin disorder of pilosebaceaous units. The clinical characteristics are seborrhea, sebaceous glands, non inflammatory lesions, inflammatory lesions and severe scaring. Propionibacterium acnes are the main pathophysiological factor influencing the acne development. Resistin gene is a novel proinflammatory cytokine involved in the initiation of inflammatory disorders like cardiovascular diseases, obesity and atherosclerosis. Various SNPs have been discovered in human RETN gene which is involved in different inflammatory disorders. Purpose of this study was to analyze RETN -420 C>G polymorphism in female acne patients of Pakistani population. About 58 control female subjects and 76 acne female patients were recruited for this study. In order to examine the RETN -420 C>G polymorphism in the promoter region, PCR and RFLP techniques were used. Statistically significant P value <0.05 for the RETN -420 C>G polymorphism was obtained in genotype/alleles frequencies between acne patients and control female subjects. Significant association between genotype frequencies, disease severity and acne scars distribution among female patients was also observed. It is concluded that RETN -420 promoter polymorphism was not associated with family history and skin types; however it was significantly associated with acne pathopysiology.
Introduction
Acne is an epidermal cutaneous chronic inflammatory disorder of sebaceous glands involving altered keratinization, androgen-induced sebum overproduction, bacterial colonization, and inflammation of the pilosebaceaous units located at the base of hair follicles of face, neck, chest, and back [1]. The sequence of events leading to the development of different acne lesions is not fully understood [2]./The detection of genetic factors involved in the development of acne may provide an insight into the biological pathways affecting disease initiation or progression and may aid for new therapies [3].
Resistin gene (‘resistance to insulin’) was originally named for its ability to resist insulin action [4]. Resistin is a 12.5kD Cysteine-rich protein that consists of 108 amino acids in human [5]. The human resistin gene is located on chromosome 19 and is expressed mainly in monocytes and macrophages, and its expression in human adipose tissue is predominantly owing to non-adipocyte resident inflammatory cells [6]. The levels of resistin and their gene polymorphism may play a role in many inflammatory diseases such as inflammatory bowel disease, chronic pancreatitis and atherosclerosis [7]. During hyperkeratinization the epithelial cells of the follicular wall accumulates in the lumen of pilosebaceaous follicles. Adrenal androgen and gonadal hormones stimulate sebum production by sebaceous glands. Microcomedones formation takes place and becomes larger in size due to accumulation of sebum [8]. The pressure develop and converts the micro comedones into visible comedones results in the rupturing of follicular wall and release of comedones contents in to the surrounding tissue, give signal to the formation of inflammatory lesions [9]. Formation of inflammatory lesions occurs by the process called comedogenesis. It was reported that Bacterial population called Propoinibacterium acnes (P.acnes) are gram positive anaerobic bacteria in sebaceous follicles. When ligands such as P.acnes come in contact with TLR’s located at surface of monocytes it regulates NFқB [10] through intracellular domain and activates the expression of genes which mediates the immune response against P.acnes [11]. Through TLR- dependent pathway regulates high sebum production and hyperkeratinization of follicular wall [12]. Recent reports suggested that acne vulgaris is inflammatory process rather than infection in which bacteria worsen the acne lesion [8]. Acne vulgaris is classified on the base of disease severity into mild acne to moderate- severe acne. During development of acne there is formation of black heads, white heads, papules, pustules, cysts and nodules [13].
There are also some other risk factors of acne vulgaris (socioeconomic impact). Reports showed that 80-90% population are affected by acne in developed countries while in non-industrialized and non-modernized countries the ratio was less due to simple life style [8]. (Diet) Previous studies have been suggested that in acne patients due to excessive use of sweet foods and carbohydrates affected the blood glucose level and shows resistance toward carbohydrates metabolism [14]. One study tells that stress activates specific regions in neuro-peptides which stimulates the pathogenic step of acne pathogenesis and undergoes in the formation of acne lesions [15]. Study reported that in acne vulgaris an endogenous hormones play a significant role includes androgen, estrogen, progesterone, glucocorticoid, insulin like growth factors (IGF), progesterone and testosterone [16]. It was reported that in westernized countries the prevalence of acne in teenagers is approximately 47% to 90% [17]. One survey study claimed that 3% cases held in 7 to 9 years, 30% cases in 10 to 12 years, 78% cases in 13 to 15 years, 93% in 16 to 18 years old individuals, 47% of acne was reported in women aged 20-29 years and 30% was reported in women aged 30-39 years [18]. In Pakistan the individuals aged between 13 to 35 years had acne problems and about 1/5th of them were concerned with dermatologist [19].
As reviewed resistin is a mediator of inflammation. It was suggested that in endothelial cells resistin mediates the expression of adhesion molecules by activating monocytes [20, 21]. The study suggested that SNP-420 C>G (rs1862513) is widely studied promoter variant of resistin located in exon2 and 420 nucleotide upstream from translatory region. Binding of transcription factor to the promoter region become altered due to polymorphism [22] the stimulating proteins Sp-1 and Sp- 3 bind with G alleles and increase the promoter activity [23]. The SNP -420 C>G is most significant polymorphism in promoter region of resistin gene [24]. The present study aimed to investigate the relation of different clinical variants (disease severity, acne scars, skin type, family history) and association of resistin gene polymorphisms (RETN −420C>G) in a sample of Pakistani population with acne vulgaris as well as controls.
Subjects and Methods
Subjects
A case control study was conducted on female patients having acne vulgaris. The study population comprised 134 individuals. 58 healthy female subjects (age 21.78 ± 2.10) were enrolled from Quaid e Azam University Islamabad considered as group A-control and 76 female were considered as group-B case (age 22.59 ± 4.34) recruited from Benazir Bhutto Hospital, Rawalpindi. Inclusion criteria for Group-A control were normal female without acne scars and no past history of acne lasting more than 1 week, Group-B female patients having clinically diagnosed acne vulgaris (comedones, papules, nodules, greasy skin, and scarring mainly on the face and minor extent on back and chest) were recruited for this study. Acne was classified as mild, moderate and severe in group B female patients. From each participant written informed consent was obtained. The information was on family history of acne, sex, current treatment, type of lesion, acne scars, type of skin and acne severity. The research was reviewed and approved by the Institutional Review Board, Quaid-i-Azam University.
Collection of Blood Specimens
The blood specimen’s collection was done from output department of Benazir Bhutto hospital (BBH) Rawalpindi Pakistan. The 5mL blood was collected with sterile syringes (Becton Dickinson Pakistan). Initially blood was transfer to ethylene diamine-tetra acetic acid (EDTA) tubes (BD, USA) and gently inverted to mix as anti-coagulant with blood. Blood samples were kept in ice box for transportation to laboratory. The samples were kept at 4ºC for further analysis.
DNA Extraction from Blood
For genomic DNA extraction, Standard Phenol- Chloroform method was followed [25]. The result of genomic DNA was check on 1% agarose gel.
PCR Assay
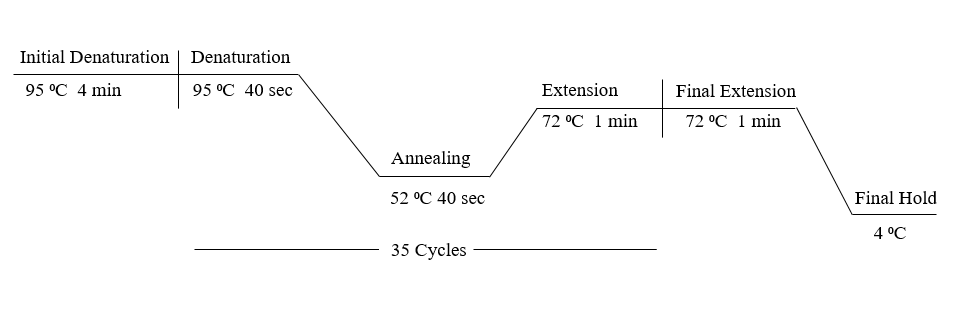
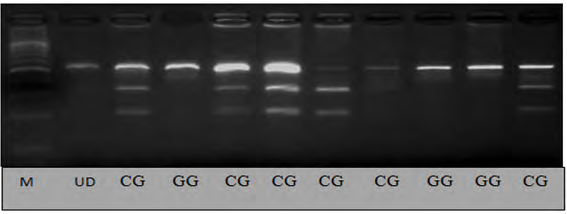
The region of resistin gene containing -420 C>G polymorphism (rs1862513) was amplified by polymerase chain reaction using the following primer F: 5’TGTCATTCTCACCCAGAGAC 3’ R: 5’TGGGCTCAGCTAACCAAATC 3’ Polymerase chain reaction (PCR) was performed in 0.2mL PCR tubes (Axygen USA) containing 25μL reaction mixture. The each reaction was consisting of 2.5μL of Taq Buffer, 0.5μL dNTP,s 2μL MgCl2, F-primer 1.25μL, R-primer 1.25μL, Taq DNA Polymerase 0.25, Genomic DNA 3μL and PCR water 14.25μL. PCR assays was performed in thermal cycler Applied Biosystems Gene Amp® PCR system 9700 (Life Technologies, USA).The cycling condition applied was as follows: the initial denaturation was at 95°C for 4 min, then 35 cycles of denaturation at 95°C for 40 s, annealing at 52°C for 40 s, elongation at 72°C for 1 min and the final elongation at 72°C for 1 min and hold at 25°C for 15 min. Amplified PCR products of DNA samples were analyzed on two percent (2%) agarose gel electrophoresis shown in figure 1.
Design for Restriction Fragment Length Polymorphism (RFLP) Analysis
The sequence of targeted (Resistin at position -420 C>G) 533 bp amplicon was retrieved from the NCBI databank. An online software NEBcutter version 2.0 (http://tools.neb. com/NEBcutter) was used to select the suitable restriction endonucleases specific for the PCR amplicon in order to confirm distinctive RFLP patterns for individual target.
Enzymatic Digestion and RFLP Analysis of PCR Products (Restriction Fragment Length Polymorphism)
The PCR product (533bp) was digested with restriction endonuclease BphiI enzyme. The total reaction volume of each digestion was 20μL consisting of 4.5μL of PCR product, 1× digestion buffer was 3.5μL and 12μL BphiI enzyme, and an adjusted amount of sterilized water. After gentle mixing, the reaction mixtures were spun down and incubated at 37°C for 16 hrs. 3% agarose gel was used to analyze the digested PCR fragments.
Statistical Analysis
Student t test was applied to compare the mean value ± standard deviation between control and patients. The data was articulated in numeral values and percentages. Fisher exact test and Chi square test were used to evaluate the genotype and alleles frequencies between control and female acne patients. Statistical significance was recognized at P < 0.05. Odd ratio (OR) was used to calculated the strength association and risk of acne. For 2×2 contingency table 95% CI (Confidence interval) was obtained. Graph Pad Prism was used for statistical tests.
Results
For genetic analysis the study population comprised of 76 female acne patients from Benazir Bhutto Hospital Rawalpindi and 58 healthy females from Qauid-e-Azam
University. PCR–RFLP technique was used for genotyping. The PCR amplified product (533 bps) figure (6) was digested with enzyme endonuclease BpiI to detect C>G polymorphism at -40C>G promoter site. This study proved that acne vulgaris shows potential association with diseases severity related to skin types of different age groups and RETN gene polymorphisms -420 C /G.
Baseline and Clinical Characteristics of Patients and Controls
Age of study population ranged from 16 years to 35 years (Table 1). The patient group contained 36 (47%) female aged 16- 20 years and 40 (53%) female aged 21-35 years while control group contained 08 (10%) females aged 16-20 years and 68 (90%) females aged 21-35 years. P value obtained was significant (P< 0.05; 95% CI =0.06-0.37; OR= 0.15) Table 1. Mean value and standard deviation were calculated for analyses of age. Student’s t-test (un-paired) was used to compare the mean age of controls and patients. The results interpreted that mean age of patients (22.59±4.34) as compared to controls (21.78±2.10) was statistically non significant (P > 0.05, t value = 1.30) (Table 2).
| Control n (%) | Patient's n (%) | OR (95% CI) | P value | |
|---|---|---|---|---|
| 58 (100) | 76 (100) | |||
| 16-20 years | 07 (10) | 36 (47) | 0.15 (0.06-0.37) | <0.0001 |
| 21-35 years | 52 (90) | 40 (53) | 0.15 (0.06-0.37) | <0.0001 |
Table 1: Baseline characteristics of female control subjects and female acne patients. Fischer exact-test was applied for calcula
| Control(n=58 ) Mean ± SD | Patients (n=76) Mean ± SD | t value | P value | |
|---|---|---|---|---|
| Age (years) | 21.78 ± 2.10 | 22.59 ± 4.34 | 1.3 | 0.1929 |
Table 2: Clinical characteristics of controls and acne patients. Values are represented as mean ± SD Student t test was applied f
Correlation of Various Clinical Variant Groups in Acne Vulgaris Patients
The clinical variables of acne vulgaris patients were represented (figure 2).
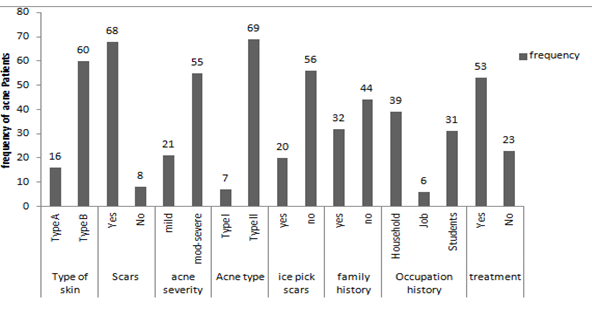
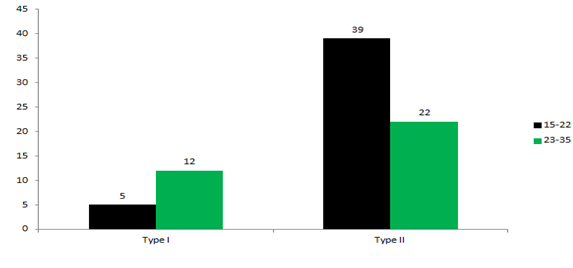
Figure 2: Frequency of acne Patients vs. Clinical variants of acne. Type of skin; Type A= Normal or dry, Type B= Oily or combination From 76 acne patients 16 (21%) patients had Type A (normal or dry) skin type and 60 (79%) patients had Type B (oily combination or sensitive) skin type. 68 (89%) patients had scars on their skin while rest of patients had no skin scars. On the basis of acne severity 21 (28%) patients had mild level of acne while 55 (72%) patients had moderate to severe level of acne. In 76 acne patients 20 (26%) patients had ice pick scars on their skin while rest of patients had skin without ice pick scars. In 76 acne patients, 32 (42%) reported a positive family history (i.e. either parents or siblings having acne), while 39 cases reported a negative family history of acne. It was stated that during treatment about 38(50%) patient had facial acne and 32(42%) cases reported had acne breakout on other parts of body (i.e. back shoulder, arms, neck, chest and leg) and 6(8%) cases reported had acne throughout their body. Non-significant P-value was obtained by comparison of family history in different severity groups mild, moderate-severe (P>0.05, OR=1.47, 95%CI=0.53-4.06) while significant P value was obtained by comparison of severity groups in different skin types (P<0.05, OR=3.67, 95% CI=1.24-10.85) and also association is found between acne types and different age groups (P< 0.05, OR=0.2, 95%CI= 0.07-0.74). Drug response was no significant associated with duration of disease (P>0.05, OR=1.43, 95%CI=0.48-4.25) result shown in table 3.
| Clinical Variables | Family history | Odd ratio | OR (95% CI) | P –value | |
|---|---|---|---|---|---|
| Disease severity | Positive 21 (100%) | Negative 55 (100%) | 1.47 | (0.53- 4.06) | 0.602 |
| Mild | 10 (48%) | 21 (38%) | |||
| Moderate-Severe | 11 (52%) | 34 (62%) | |||
| Disease severity | Skin types | ||||
| Type A 22 (100%) | Type B 54 (100%) | ||||
| Mild | 10 (45.5%) | 10 (18.5%) | 3.67 | (1.24-10.85) | 0.022 |
| Moderate-severe | 12 (54.5%) | 44 (81.5%) | |||
| Age groups | Acne types | ||||
| Type I 17 (100) | Type II 61 (100) | ||||
| 15-22 | 5(29.42%) | 39(63.94%) | 0.23 | (0.07-0.74) | 0.01 |
| 23-25 | 12 (70.58%) | 22(36.06%) | |||
| Duration of disease (Years) | Drug response | ||||
| Yes 30 (100) | No 23 (100) | ||||
| 0.5-3 | 17 (57%) | 11 (48%) | 1.43 | (0.48-4.25) | 0.59 |
| 04-13 | 13 (43%) | 12 (52%) |
Table 3: Comparison of Clinical variant groups in Acne vulgaris Patients. Skin type A= Normal or Dry, Skin type B=Oily, Combinati
Table 3: Comparison of Clinical variant groups in Acne vulgaris Patients. Skin type A= Normal or Dry, Skin type B=Oily, Combination or Sensitive. Acne Type I= Comedonica (non-inflammatory lesions), Acne Type II= Nodulocystic-Papulopustular (inflammatory lesions). Fischer exact test and chi square test was applied for calculation of P value. P<0.005 statistically significant = Skin type vs. Disease severity, Acne type vs. Age groups.
Association of RETN Polymorphism in Various Clinical Variant Groups of Acne Vulgaris Patients
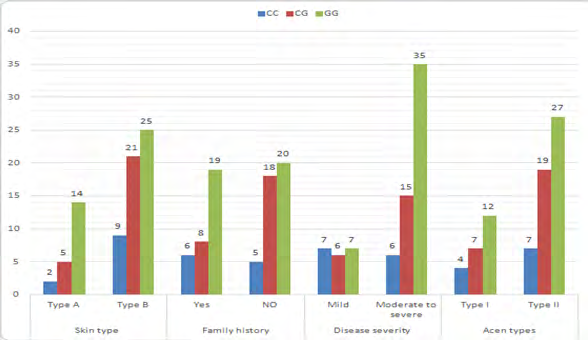
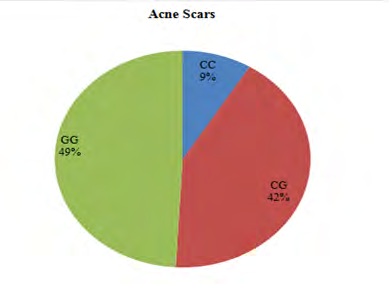
To illuminate the association of RETN -420C>G single nucleotide polymorphism (SNP) with the pathogenesis of acne, genotype frequencies were compared with variables like severity of acne, skin type, family history, scars and acne types figure.4, figure.5. The results of significance tests interpreted that the severity of acne was associated with resistin (RETN) genotypes (P<0.05; χ2=7.15). There has been non-significant association of RETN polymorphism in the distribution of different acne types and skin types (P>0.05, χ 2=0.34; P>0.05, χ 2 =2.29). The genotype frequencies in the patients having a positive family history was not significantly different as compared with patients having a negative family history (P>0.05, χ2=2.69). The results showing the relationship between RETN polymorphism and acne scars was significance (P< 0.05, χ2= 9.48). Association of RETN polymorphism in different variables and test statistics is shown in Table 4.
- Variables
- Total
- Genotypes CC CG GG χ2
- P value
- Disease severity
- 6.33
- 0.04
- Mild
- 20 (100)
- 7 (35%)
- 6 (30%)
- 7 (35%)
- Mild-severe
- 56 (100)
- 6 (11%)
- 15 (27%)
- 32 (62%)
- Skin types
- 2.74
- 0.14 (NS)
- Type A
- 21 (100)
- 2 (9%)
- 5 (24%)
- 14 (67%)
- Type B
- 55 (100)
- 9 (16.5%)
- 21 (38%)
- 25 (45.5%)
- Scars
- 9.48
- 0.008
- Presence
- 57 (100)
- 5 (9%)
- 24 (42%)
- 28 (49%)
- Absence
- 19 (100)
- 6 (32%)
- 2 (10%)
- 11 (58%)
- Family History
- 2.69
- 0.26 (NS)
- Positive
- 33 (100)
- 6 (18%)
- 8 (24%)
- 19 (28%)
- Negative
- 43 (100)
- 5 (12%)
- 18 (42%)
- 20 (46%)
- Acne types
- 0.34
- 0.84 (NS)
- Type I
- 23 (100)
- 4 (17.4)
- 7 (30.4%)
- 12 (52.2%)
- Type II
- 53 (100)
- 7 (13%)
- 19 (36%)
- 27 (51%)
Table 4: Comparison of genotype frequencies of RETN C>G-420 among Clinical variant groups of acne patients.
RETN Polymorphism: Genotype and Alleles Distribution among Study Population
Susceptibly of disease was analyzed to associate the genotype pattern of acne patients with SNP of -420 resistin gene. Genotyping was carried out by PCR-RFLP method using BpiI restriction enzyme. BpiI recognized 5’…GAAGAC(N2)↓… 3’ sequence, and digested 533bp amplified PCR product into different bands depending upon genotype of sample. Band sizes were CC (326, 207 bp), CG (533,326, 207bp), GG (533bp) respectively (Figure 6). Association of RETN polymorphism among study population has been represented in Table 5.
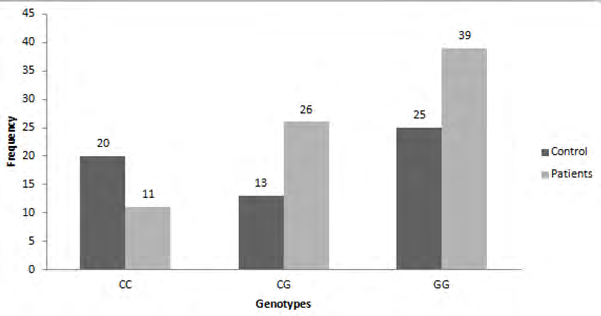
A significant P value was obtained when genotypes (CC, CG and GG) of between patient and control groups were compared (P< 0.05; χ2 = 4.04). The genotype distribution in patients and controls was following CC = 11 (15%), CG = 26 (34%) and GG = 39 (51%); CC = 20 (35%), CG = 13 (22%) and GG = 25 (43%) respectively (figure 7). Comparison of wild type CC and dominant model (CG+GG) for resistin -420 C>G polymorphism showed that variant genotype was more common in patients (85%) as compared to the control group (63%) (P<0.05; OR = 4.98; 95% CI = 2.18-11.35: table 5). Similarly, allele frequencies were compared between the two groups and a significant P value was obtained (P<0.05; OR =1.82; 95% CI = 1.10-3.00) and frequency of G allele is high in acne patients as compare to control subjects.
| Total(134) | Control (58) | Patient (76) | χ2 | OR (95% CI) | P-value | |
|---|---|---|---|---|---|---|
| CC | 31 (23%) | 20 (35%) | 11 (15%) | 4.04 | - | 0.02 |
| CG | 39 (29%) | 13 (22%) | 26 (34%) | 4.04 | - | 0.02 |
| GG | 64 (48%) | 25 (43%) | 39 (51%) | 4.04 | - | 0.02 |
| CC | 31 (23%) | 20 (35%) | 11 (15%) | 3.11 | (1.30-6.90) | 0.007 |
| CG+GG | 103 (77%) | 38 (65%) | 65 (85%) | 3.11 | (1.30-6.90) | 0.007 |
| Alleles | Total (268) | Controls (116) | Patients (152) | 1.82 | (1.12-3.00) | 0.022 |
| C | 101 (38%) | 53 (46%) | 48 (32%) | 1.82 | (1.12-3.00) | 0.022 |
| G | 167 (62%) | 63 (54%) | 104 (68%) | 1.82 | (1.12-3.00) | 0.022 |
Table 5: Comparison of resistin SNP genotypes and allele’s frequencies of studied polymorphism in control and patients. For P val
Table 5: Comparison of resistin SNP genotypes and allele’s frequencies of studied polymorphism in control and patients. For P value Chi square test and Fischer exact test was applied OR= Odd Ratio, CI= confidence interval. Statistically significant P<0.005 Acne vulgaris is a chronic inflammatory disorder of pilosebaceous units. As compared to other diseases the incidence ratio of acne vulgaris is high [26]. Prevalence of acne is high in adolescence and in young adults. Acne vulgaris have complex etiology and pathophysiology. Hormonal factors such as androgens and immunogenic cytokines increases the production of sebum, favors the conversion from comedones to inflammatory lesions [16].
It was concluded from different studies that main risk factors of acne vulgaris are deficiency in sleep, stress, family history, socioeconomic impact and use of low quality cosmetics and skin type [13]. Studies show that proinflammatory cytokines are present in pilosebaceous units which mediate the formation of acne. Resistin is a proinflammatory cytokine [27]. Officially Steppan and his co-workers first discovered resistin in 2001 [3]. One study reported that resistin mediates the expression of adhesion molecules through monocytes; results in the up- regulation of ICAM-I, VCAM-I and MCP-1 expression by p38 MAPK dependent pathway cause atherosclerosis which is inflammatory process [20, 28]. Monocytes are main source of resistin hormone which is mainly concerned with up- regulation of inflammatory response [29]. The current case control study was designed to investigate the association of resistin RETN -420C>G polymorphism with acne in female patients of a Pakistani population. The results showed that there is a significant association between the RETN -420C>G polymorphism and the studied female acne patients. These findings are similar to those described in previous studies showing an association of the -420C>G polymorphism in chronic and inflammatory diseases such as cardiovascular diseases, atherosclerosis and obesity [30, 31, 32]. In the present study there is significant association of the RETN -420C>G with diseases severity and acne scars while no relationship was found with family history and skin type. This study did not found any significant association among duration of disease, family history of acne in female acne patients while Bataille and coworkers in 2002 demonstrated a significant association between high risk of acne development and family history of acne [33]. This study shows a significant association between acne types in different age groups and with skin types among acne patients. These results are agree with previous studies demonstrating women with comedonal acne were older than women with inflammatory lesions and age matched peers had high incidence of acne as compared to postmenopausal women [34]; Wei and coworkers suggested that the oil skin may be main risk factor of acne [35, 36, 37, 38, 39, 40, 41, 42].
In conclusion the pathophysiology of acne vulgaris is multifactorial and complex that may be due to a number of gene. The study should be replicated in other to determine the role of said SNP in acne and its functional aspect.
References
-
Williams HC, Dellavalle RP, Garner S (2012) Acne vulgaris. The Lancet 379(9813): 361-372.
-
Hsieh MF, Chen CH (2011) Delivery of pharmaceutical agents to treat acne vulgaris: current status and perspectives. J Med Biol Eng 32(4): 215-224.
-
Steppan CM, Bailey ST, Bhat S, Brown EJ, Banerjee RR, et al. (2001) The hormone resistin links obesity to diabetes. Nature 409(6818): 307-312.
-
Schwartz DR, Lazar MA (2011) Human resistin: found in translation from mouse to man. Trends in Endocrinology & Metabolism 22(7): 259-265.
-
Wang H, Chen DY, Cao J, He ZY, Zhu BP, et al. (2009) High serum resistin level may be an indicator of the severity of coronary disease in acute coronary syndrome. Chinese medical sciences journal 24(3): 161-166.
-
Bokarewa M, Nagaev I, Dahlberg L, Smith U, Tarkowski A (2005) Resistin, an adipokine with potent proinflammatory properties. The Journal of Immunology 174(9): 5789-5795.
-
Adrych K, Smoczynski M, Sledzinski T, Dettlaff Pokora A, Goyke E, et al. (2009) Increased serum resistin concentration in patients with chronic pancreatitis: possible cause of pancreatic fibrosis. Journal of clinical gastroenterology 43(1): 63-68.
-
Basak SA, Zaenglein AL (2013) Acne and its management. Pediatrics in review 34(11): 479-497.
-
Eichenfield L, Leyden J (1991) Acne: current concepts of pathogenesis and approach to rational treatment. Pediatrician 18(3): 218-223.
-
Younis S, Blumenberg M, Javed Q (2016) Resistin gene polymorphisms are associated with acne and serum lipid levels, providing a potential nexus between lipid metabolism and inflammation. Arch Dermatol Res 308(4): 229-237.
-
Konrad A, Lehrke M, Schachinger V, Seibold F, Stark R, et al. (2007) Resistin is an inflammatory marker of inflammatory bowel disease in humans. European journal of gastroenterology & hepatology 19(12): 1070- 1074.
-
Takeda K, Kaisho T, Akira S (2003) Toll-like receptors. Annual Review of Immunology 21(1): 335-376.
-
Haider A, Mamdani M, Shaw JC, Alter DA, Shear NH (2006) Socioeconomic status influences care of patients with acne in Ontario, Canada. Journal of the American Academy of Dermatology 54(2): 331-335.
-
Freedberg IM, Tomic Canic M, Komine M, Blumenberg M (2001) Keratins and the keratinocyte activation cycle. Journal of Investigative Dermatology 116(5): 633-640.
-
Makrantonaki E, Ganceviciene R, Zouboulis C (2011) An update on the role of the sebaceous gland in the pathogenesis of acne. Dermato-endocrinology 3(1): 41- 49.
-
Ghodsi SZ, Orawa H, Zouboulis CC (2009) Prevalence, severity, and severity risk factors of acne in high school pupils: a community-based study. Journal of Investigative Dermatology 129(9): 2136-2141.
-
Kilkenny M, Merlin K, Young R, Marks R (1998) The prevalence of common skin conditions in Australian school students: 1. Common, plane and plantar viral warts. The British journal of dermatology 138(5): 840- 845.
-
Collier CN, Harper JC, Cantrell WC, Wang W, Foster KW, et al. (2008) The prevalence of acne in adults 20 years and older. Journal of the American Academy of Dermatology 58(1): 56-59.
-
Kapadia N, Talib A (2004) Acne treated successfully with azithromycin. International journal of dermatology 43(10): 766-767.
-
Hsu WY, Chao YW, Tsai YL, Lien CC, Chang CF, et al. (2011) Resistin induces monocyte–endothelial cell adhesion by increasing ICAM‐1 and VCAM‐1 expression in endothelial cells via p38MAPK‐dependent pathway. Journal of cellular physiology 226(8): 2181-2188.
-
Kawanami D, Maemura K, Takeda N, Harada T, Nojiri T, et al. (2004) Direct reciprocal effects of resistin and adiponectin on vascular endothelial cells: a new insight into adipocytokine–endothelial cell interactions. Biochemical and biophysical research communications 314(2): 415-419.
-
Smith SR, Bai F, Charbonneau C, Janderová L, Argyropoulos G (2003) A promoter genotype and oxidative stress potentially link resistin to human insulin resistance. Diabetes 52(7): 1611-1618.
-
Chung S, Choi H, Kim K, Cho Y, Lee H, et al. (2005) Regulation of human resistin gene expression in cell systems: an important role of stimulatory protein 1 interaction with a common promoter polymorphic site. Diabetologia 48(6): 1150-1158.
-
Wang B, Yang W, Wen W, Sun J, Su B, et al. (2010) γ-secretase gene mutations in familial acne inversa. Science 330(6007): 1065-1065.
-
Sambrook J, Fritsch EF, Maniatis T (1989) Molecular cloning: Cold spring harbor laboratory press New York.
-
Rzany B, Kahl C (2006) Epidemiology of acne vulgaris. JDDG: Journal der Deutschen Dermatologischen Gesellschaft 4(1): 8-9.
-
Wahab HMA, Ragaie MH, Gaber SS, Younis RH (2019) Resistin gene polymorphisms and serum lipid levels in acne vulgaris: a case–control study in Egyptian patients. Journal of the Egyptian Women’s Dermatologic Society 16(1): 43-50.
-
Verma S, Li SH, Wang CH, Fedak PW, Li RK, et al. (2003) Resistin promotes endothelial cell activation further evidence of adipokine-endothelial interaction. Circulation 108(6): 736-740.
-
Vassiliadi DA, Tzanela M, Kotanidou A, Orfanos SE, Nikitas N, et al. (2012) Serial changes in adiponectin and resistin in critically ill patients with sepsis: Associations with sepsis phase, severity, and circulating cytokine levels. Journal of critical care 27(4): 400-409.
-
Azuma K, Oguchi S, Matsubara Y, Mamizuka T, Murata M, et al. (2004) Novel resistin promoter polymorphisms: association with serum resistin level in Japanese obese individuals. Hormone and metabolic research 36(08): 564-570.
-
Kaser S, Kaser A, Sandhofer A, Ebenbichler C, Tilg H, Patsch J (2003) Resistin messenger-RNA expression is increased by proinflammatory cytokines in vitro. Biochemical and biophysical research communications 309(2): 286-290.
-
Tan JK, Vasey K, Fung KY (2001) Beliefs and perceptions of patients with acne. Journal of the American Academy of Dermatology 44(3): 439-445.
-
Bataille V, Snieder H, MacGregor A, Sasieni P, Spector T (2002) The influence of genetics and environmental factors in the pathogenesis of acne: a twin study of acne in women. Journal of investigative dermatology 119(6): 1317-1322.
-
Perkins AC, Maglione J, Hillebrand GG, Miyamoto K, Kimball AB (2012) Acne vulgaris in women: prevalence across the life span. Journal of Women’s Health 21(2): 223-230.
-
Wei B, Pang Y, Zhu H, Qu L, Xiao T, et al. (2010) The epidemiology of adolescent acne in North East China. Journal of the European Academy of Dermatology and Venereology 24(8): 953-957.
-
Ahmed S, Ahmed I (2007) Frequency and magnitude of anxiety and depression among acne patients: A study of 100 cases. JLUMHS 6(1): 25-29.
-
Bhate K, Williams H (2013) Epidemiology of acne vulgaris. British Journal of Dermatology 168(3): 474- 485.
-
Davis EC, Callender VD (2010) A review of acne in ethnic skin: pathogenesis, clinical manifestations, and management strategies. The Journal of clinical and aesthetic dermatology 3(4): 24.
-
Rutter P (2005) Symptoms, Diagnosis and Treatment: A Guide for Pharmacists and Nurses. Elsevier Health Sciences.
-
Tahir CM (2010) Pathogenesis of acne vulgaris: simplified. Journal of Pakistan Association of Dermatologists 20(2): 93-97.
-
Truter I (2009a) Evidence-based pharmacy practice (EBPP): acne vulgaris. SA Pharmaceutical Journal 76(3): 12-19.
-
Truter I (2009b) Evidence-based pharmacy practice (EBPP): acne vulgaris: review. SA Pharmaceutical Journal 76(3): 12-19.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling