Toxic Epidermal Necrolysis-like Subacute Cutaneous Lupus Erythematosus: A Case Report
Toxic epidermal necrolysis (TEN)-like lesions have been described in the setting of lupus erythematosus, and have been considered as a specific hyperacute variant of cutaneous lupus erythematosus, with features different from classical drugrelated toxic epidermal necrolysis. This is a report of a case of subacute cutaneous lupus erythematosus in a 62-year old Caucasian woman, which evolved into a TEN-like presentation over the course of 4 weeks. The patient responded rapidly to treatment with high doses of prednisone
Introduction
Cutaneous lupus erythematosus (LE) includes a wide spectrum of dermatologic manifestations [1]. A bullous eruption in the setting of lupus erythematosus can be a diagnostic challenge. The toxic epidermal necrolysis (TEN)- like presentations of acute or subacute cutaneous lupus erythematosus (TEN-like ACLE/SCLE) may closely mimic TEN [2, 3]. Although the clinical and histological features of these rare conditions are very similar, several subtle differences can help in differentiation between them. In contrast to classic TEN, whose occurrence is usually associated with drug ingestion, TEN-like ACLE/SCLE are often triggered by extensive ultraviolet (UV) exposure and the blistering eruption typically starts on UV-exposed areas [4]. A previous history of LE and lupus-specific response in histopathological finding could be additional clues for diagnosis of TEN-like LE. Also, the course of TEN-like LE is usually subacute, systemic symptoms (seen in TEN) are absent and mucous membranes are spared or mildly affected [5]. However, in some cases it can be difficult to distinguish these unusual, vesiculobullous forms of LE from classical TEN both clinically and histopathologically.
This is a report of a case of SCLE in a 62-year old Caucasian female, which gradually evolved into a TEN-like expression over the course of 4 weeks after prolonged sun exposure and irregular medication intake (chloroquine and prednisone). There was no history of recent infection or drug intake. The patient had a 3 months history of SCLE characterized by photo distributed annular and polycyclic erythematous plaques. The diagnosis was confirmed by histopathological examination and direct immunofluorescence of skin lesions that were consistent with LE. Lupus band test on sun-protected non-lesional skin was negative. Antinuclear antibodies (ANA) and anti-Ro (SS-A) antibodies were elevated (1: 160 and 73.4 RU/ml, respectively). No other laboratory abnormalities were detected. She was treated with chloroquine and low/ mid dose systemic steroids (prednisone, 0.3-0.4 mg/kg/daily).
On physical examination the patient had symmetrically distributed, mostly dusky erythematous plaques and areas on the face, neck, trunk and extremities, with erosions and skin shedding (Figures 1a-c) and targetoid lesions, mostly on lower extremities (Figure 1d). All visible mucous membranes were unaffected. Nikolsky’s sign was mildly positive, mostly on her upper trunk and proximal aspect of extremities. The patient was in good general health.
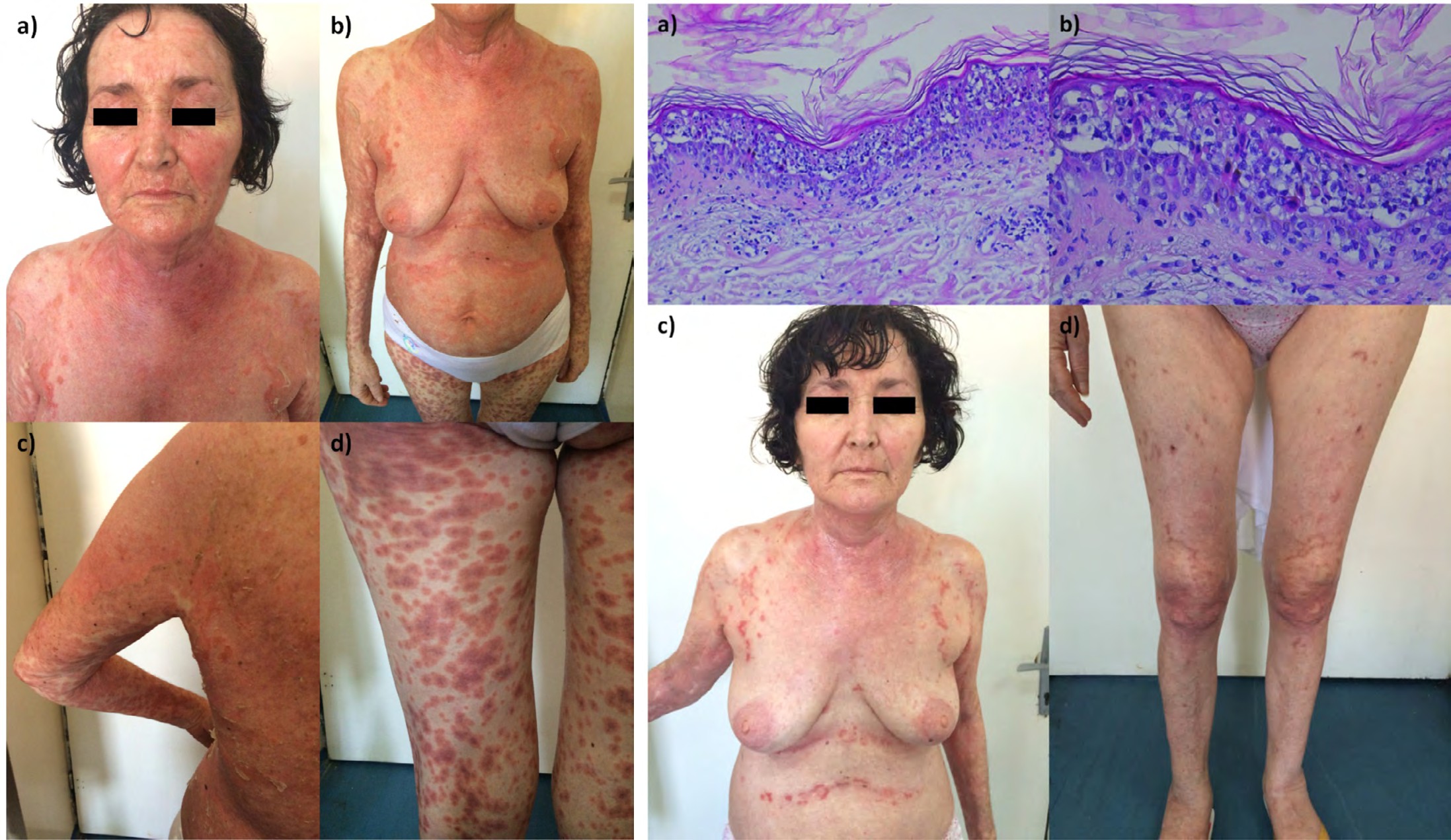
Figure 1*: a, b and c) symmetrically distributed, mostly dusky erythematous plaques and areas on the face, neck, trunk and extremities, with erosions and skin shedding; d) targetoid lesions on lower extremities. *Photos taken 5 days upon admission.
Direct immunofluorescent test of the skin lesion was negative (probably due to prior treatment with systemic steroids). Laboratory investigations demonstrated normal complete blood cell count, serum chemistry, renal function tests and urinalysis.
Histopathology showed numerous necrotic keratinocytes as well as extensive epidermal necrosis. Also, there was a superficial scarce perivascular and periadnexal infiltrate of lymphocytes (Figure 2a and b).
The diagnosis of TEN-like presentation of SCLE was made based on reported history, clinical presentation and histopathological findings.
The treatment with oral prednisone 1.0 mg/kg tapered quickly within next 3 weeks to 0.6 mg/kg then slowly over 2 months and chloroquine 250 mg daily, combined with potent topical steroid therapy, led to rapid improvement over the following week, with complete resolution of skin lesions within 3 weeks (Figures 2c & d).
In the follow-up period of 4 years, she experienced several minor flares of SCLE. Lesions presented as few anular erythematous plaques, localized on shoulders and chest area mainly, resolving on potent steroid ointments ant topical calcineurin inhibitors. At present, she is treated with chloroquine, 250 mg daily, with 3 month-breaks per year.
Discussion
Vesiculobullous skin lesions in the setting of SCLE as well as ACLE, either during the course of the disease or as a part of an initial clinical presentation, are considered as lupus- specific skin eruption as they exhibit typical histopathological features of LE [1, 6]. Sontheimer, et al. pointed that lesions are the result of aggressive inflammatory epidermal basal layer damage, occurring as a dramatic extension of the interface dermatitis [1]. Differentiating a bullous eruption in the context of preexisting lupus remains difficult. There are distinguishing features although the differences can be subtle [5].
TEN-like lesions occurring in the context of ACLE/SCLE can create considerable diagnostic difficulties, particularly in the patients without preceding diagnosis of either ACLE or SCLE [3, 6, 7]. Ting, et al. proposed the term. Acute Syndrome of Apoptotic Pan-Epidermolysis“(ASAP) as a unifying designation for clinical entities characterized with acute and massive cleavage resulting from hyperacute apoptotic injury of the epidermis [4]. All those entities may simulate TEN, definitive diagnosis may sometimes be impossible since histopathological findings, serology may be identical [7], but they differ widely in term of etiopathogenesis [8]. Although mucosal membrane involvement has been noticed, in TEN- like LE, oral mucosa being most commonly involved, other membranes are not affected [4, 9]. The standard treatment of TEN-like ACLE/ SCLE remains controversial; corticosteroids have been shown to have beneficial effects [10].
Histopatological findings of TEN- like ACLE/SCLE demonstrate a full-thickness epidermal necrosis in up to 88% of cases [2]. Features used to differentiate full-thickness epidermal necrosis in the setting of SCLE according to Rayan, et al. are listed in Table 1 [5]. As patients with TEN-like ACLE/SCLE demonstrate full-thickness epidermal necrosis, Nikolsky’s sign is expected to be positive. However, Nikolsky’s sign may be absent, probably depending on the extent of skin lesions [3, 5].
| TEN | TEN-like SCLE | SCLE with blisters | |
|---|---|---|---|
| Clinical | Flu-like prodrome Dusky macules that coalesce Rapid progression Bullae and sloughing of epidermis | May have preceding diagnosis of lupus Subacute onset and slow progression Bullae and sloughing of epidermis | Annular plaques with vesicles/bullae at border Crusting |
| Nikolsky sign | positive | Positive or negative | negative |
| Mucosa membrane involvement | severe | Less severe and predominantly oral mucosa | absent |
| Serology | Negative | ANA positive | ANA positive Anti SSA/SSB positive in most cases |
| Histopathology | Full thickness epidermal necrosis with sparse superficial lymphocytic inflammatory infiltrate | Full thickness epidermal necrosis with sparse superficial lymphocytic inflammatory infiltrate Features of interface dermatitis | Basal vacuolar change, epidermal atrophy, dermal oedema and superficial mucin Intense vacuolar degeneration resulting in separation of dermis from epidermis |
| DIF | negative | May show lupus band | Most cases are positive |
| Drug etiology | Most cases | No | Reported |
| Course | Evolves over 3–5 days and heals over 3–4 weeks Scarring may occur Mortality up to 30–40%. | Subacute course with rapid improvement following treatment | May be chronic or with intermittent exacerbations |
Table 1: Features used to differentiate full-thickness epidermal necrosis in the setting of subacute cutaneous lupus erythematosu
Table 1: Features used to differentiate full-thickness epidermal necrosis in the setting of subacute cutaneous lupus erythematosus (according to Rayan, et al.). TEN, Toxic epidermal necrolysis; SCLE, Subacute cutaneous lupus erythematosus; DIF, direct immunofluorescence; ANA, Antinuclear antibodies; SSA/SSB, Sjögren’s-syndrome-related autoantibodies.
Our patient demonstrated a classical clinical pattern of SCLE that evolved to TEN over the course of 4 weeks. Although she had extensive skin lesions and positive Nikolsky’s sign, she remained systemically well. The course was prolonged and her response to higher dose of prednisone was remarkably fast, which is atypical of classic TEN. Sun- exposed areas were the initial areas of involvement in our patient, suggesting UV exposure to be an important trigger or aggravating factor. Cases of TEN-like ACLE following UV exposure with or without sparing of covered lesions have been reported in up to 85% of patients [2, 4]. Romero, et al. described initial TEN- like on preexisting LE lesions [2]. The diagnosis of TEN-like expression of SCLE in our patient and differentiation from classic TEN was made taking in consideration the preexisting SCLE, the subacute progression, photodistribution, positive autoimmune serology, absence of mucosal involvement and systemic symptoms as well as prompt response to systemic steroids. Lack of evidence of high risk drug intake also favor a diagnosis of TEN-like ACLE/SCLE. Our patient met the features highlighted by Rayan, et al. (Table 1) [5].
Conclusion
TEN-like bullous eruptions in patients with SCLE can mimic TEN, which is usually associated with medication use. This case represents a rare and unusual expression of SCLE and also highlights the difficulties in differentiating between classic drug-induced TEN and TEN-like SCLE. Clinicians rely on corroborative history, positive serology and clinical course with supportive histopathology to make a diagnosis.
References
-
Sontheimer RD (1997) The lexicon of cutaneous lupus ery¬thematosus - a review and personal perspective on the nomenclature and classification of the cutaneous manifestations of lupus erythematosus. Lupus 6(2): 84- 95.
-
Romero LS, Bari O, Forbess Smith CJ, Schneider JA, Cohen PR (2018) Toxic epidermal necrolysis-like acute cutaneous lupus erythematosus: report of a case and review of the literature. Dermatol Online J 24(5): 13030.
-
Paradela S, Martínez Gómez W, Fernández Jorge B, Castiñeiras I, Yebra Pimentel T, et al. (2007) Toxic epidermal necrolysis-like acute cutaneous lupus ery¬thematosus. Lupus 16(9): 741-745.
-
Ting W, Stone MS, Racila D, Scofield RH, Sontheimer RD (2004) Toxic epidermal necrolysis-like acute cutaneous lupus erythematosus and the spectrum of the acute syndrome of apoptotic pan-epidermolysis (ASAP): a case report, concept review and proposal for new classification of lupus erythematosus vesiculobullous skin lesions. Lupus 13(12): 941-950.
-
Rayan E, Marshman G, Astill D (2012) Toxic epidermal necrol¬ysis-like subacute cutaneous lupus erythematosus. Australas J Dermatol 53(4): 303-306.
-
Lee AL, Werth PV (2017) Lupus erythematosus. 4th (Edn.), In: Bolognia JL, Schaffer JV, Cerroni L (Eds.), Dermatology. Philadelphia, PA: Mosby Elsevier, pp: 662- 680.
-
Lee HY, Tey HY, Pang SM, Thirumoorthy T (2011) Systemic lupus erythematosus presenting as Stevens– Johnson syndrome and toxic epidermal necrolysis: a report of three cases. Lupus 20: 647-652.
-
Monga B, Ghosh S, Jain V (2014) Toxic epidermal necrolysis-like rash of lupus: a dermatologist’s dilemma. Indian J Dermatol 59(4): 401-402.
-
Merklen Djafri C, Bessis D, Frances C, Poulalhon N, Debarbieux S, et al. (2015) Blisters and loss of epidermis in patients with Lupus Erythematosus. A clinicopathological study of 22 patients. Medicine 94(46): e2102.
-
Boontaveeyuwat E, Silpa archa N, Kulthanan K (2012) Toxic epidermal necrolysis-like acute cutaneous lupus ery-thematosus (TEN-like ACLE) in SLE patients: a report of two cases. Asian Pac J Allergy Immunol 30(1): 83-87.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling