Water-exacerbated Pruritus and a Flagellate Eruption: Adult-onset Still’s Disease Occurring in Association with Influenza A Virus Infection
Adult-onset Still’s disease (AOSD) presents with fever, systemic symptoms and rash. Atypical presentations are increasingly described. Uncommonly, viral-associated AOSD occurs. We report AOSD presenting in a 30-year-old male with waterexacerbated pruritus, a subsequent flagellate eruption, and associated influenza A virus infection.
Introduction
Adult-onset Still’s disease (AOSD) presents with fever, systemic symptoms and rash. Atypical presentations are increasingly described [1]. Uncommonly, viral-associated AOSD occurs [2]. We report AOSD presenting with water- exacerbated pruritus, a flagellate eruption, and associated influenza A virus infection.
Case Synopsis
A 30-year-old Jamaican male with no chronic diseases presented with a two-week history of cough, pleuritic chest pain, nocturnal fever, sore throat, myalgia and arthralgias of the knees and ankles. In hospital, he had recurrent fevers above 39°C, despite multiple courses of intravenous antibiotics. During hospitalization, he developed pruritus, markedly worse after water contact (primarily sweating or showering) and subsequently, a rash. Dermatology was consulted. Examination revealed flagellate, hyperpigmented plaques on the back and brown papules involving the anterior trunk and buttocks (Figure 1A-B). No wheals or dermatographism were seen. Tonsils were enlarged. No lymphadenopathy or hepatosplenomegaly were palpated. Blood work revealed an elevated white blood cell count (19x109/L) with neutrophilia (absolute neutrophil count 14770/mm3), transaminitis, anemia, elevated c-reactive protein and erythrocyte sedimentation rate and elevated lactate dehydrogenase. Blood/sputum/urine cultures were sterile. Serology for rheumatoid factor and antinuclear antibodies were negative. Viral studies including HIV, dengue and hepatitis B/C were negative. Influenza A/B RT-PCR was pending at the time of consultation. Echocardiogram revealed no cardiac vegetations and chest x-ray and abdominal ultrasound were unremarkable.
Punch biopsies from the upper back and left shoulder revealed hyperkeratosis, epidermal hyperplasia, apoptotic keratinocytes at all levels of the epidermis, and a superficial perivascular and interstitial neutrophilic infiltrate with scattered eosinophils (Figure 1C-D). A ferritin level was requested revealing significant elevation at 15,679 ng/ml (10-330). Interestingly, reverse transcription-polymerase chain reaction (RT-PCR) for influenza A virus (IAV) was positive. Based on the clinical features and characteristic histology, a diagnosis of AOSD with flagellate eruption, aquagenic exacerbation occurring in the setting of IAV infection was rendered. Prednisone 40mg once daily and 0.05% clobetasol propionate ointment twice daily were prescribed, with defervescence and cessation of pruritus within 48 hours. Weekly oral methotrexate was added, and the patient referred to rheumatology for continued management.
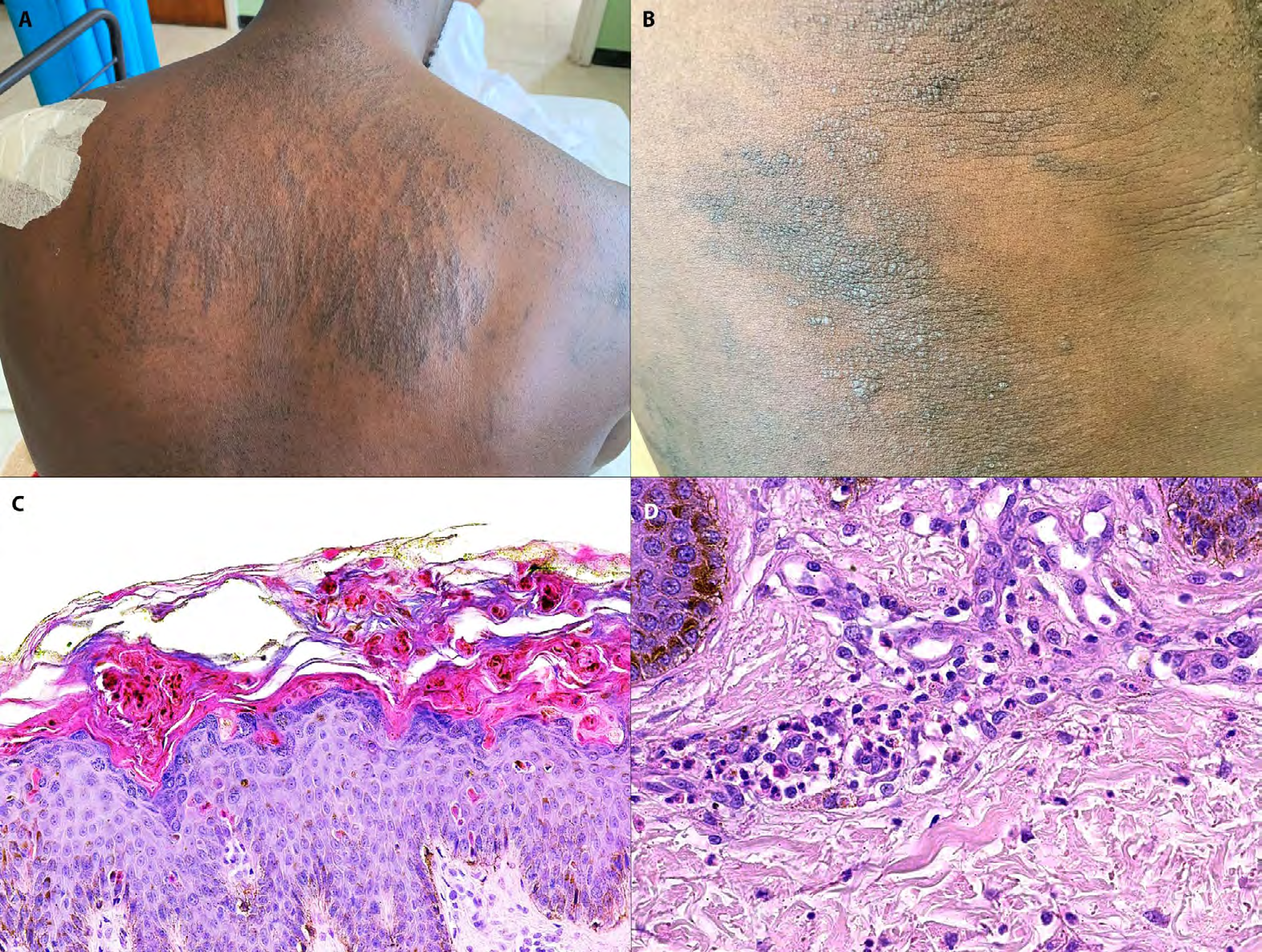
Figure 1: Adult onset Still’s disease. Note Flagellate hyperpigmented plaques on the upper back (A) and brown hyperkeratotic papules on the abdomen (B). Histopathology reveals hyperkeratosis, apoptotic keratinocytes high in the epidermis (C) and an associated neutrophilic infiltrate (D), characteristic of the persistent lesions in adult onset Still’s disease. C-D: Hematoxylin and eosin X200 (C), X400 (D)
Case Discussion
AOSD is an autoinflammatory disease presenting with fever, sore throat, arthralgias, neutrophilia and a rash. Multiorgan involvement may occur [3]. While the classical rash of AOSD is evanescent and urticarial, persistent lesions flagellate eruptions, have recently been described [1]. Our case, while exhibiting typical systemic findings and the increasingly recognized flagellate eruption, is notable for two features: marked water-exacerbated itch and concurrent IAV infection. Though the pathophysiology of water-induced itch is poorly understood, it is well described in systemic diseases, classically polycythemia vera [4]. To our knowledge, it has not been reported in AOSD.
Virus-associated AOSD has been described. Implicated microorganisms include rubella, parainfluenza, Epstein Barr virus, Coxsackie virus, mumps virus and cytomegalovirus [2, 5]. More recently reported, is AOSD after influenza vaccination [6]. Our patient’s RT-PCR was positive for IAV, further supporting a potential role for IAV-associated disease. While the precise relationship of IAV to AOSD onset is unclear, advances in the understanding of autoinflammation in Still’s disease are instructive. Specifically, NLR containing a pyrin domain (NLRP3) inflammasome dysregulation with increased signalling has been described in AOSD [7]. Fascinatingly, NLRP3 inflammasome signalling also appears crucial for antiviral response in IAV infection [8]. Unfortunately, inflammasome dysregulation/over-activation in IAV infection induces a hyperinflammatory state with severe pulmonary disease [8, 9, 10]. Perhaps IAV/pathogen- associated AOSD is another manifestation of overshooting this innate immune response.
Conclusion
To summarize, we report AOSD presenting with water- exacerbated pruritus, a flagellate eruption, and concomitant IAV infection. A high index of suspicion is required to diagnose this entity with its increasing clinical manifestations. Concurrent viral infections should be excluded.
References
-
Sun NZ, Brezinski EA, Berliner J, Haemel A, Connolly MK, et al. (2015) Updates in adult-onset Still disease: Atypical cutaneous manifestations and associations with delayed malignancy. J Am Acad Dermatol. 73(2): 294-303.
-
Wouters JM, van der Veen J, van de Putte LB, de Rooij DJ (1988) Adult onset Still›s disease and viral infections. Ann Rheum Dis 47(9): 764-767.
-
Pouchot J, Sampalis JS, Beaudet F, Carette S, Décary F, et al. (1991) Adult Still›s disease: manifestations, disease course, and outcome in 62 patients. Medicine (Baltimore) 70(2): 118-136.
-
Lelonek E, Matusiak Ł, Wróbel T, Szepietowski JC (2018) Aquagenic Pruritus in Polycythemia Vera: Clinical Characteristics. Acta Derm Venereol 98(5): 496-500.
-
Jia J, Shi H, Liu M, Liu T, Gu J, et al. (2019) Cytomegalovirus Infection May Trigger Adult-Onset Still’s Disease Onset or Relapses. Front Immunol 10: 898.
-
Yoo WH (2010) Adult onset Still’s disease following influenza vaccination. Joint Bone Spine 77(4): 373-374.
-
Hsieh CW, Chen YM, Lin CC, Tang KT, Chen HH, et al. (2017) Elevated Expression of the NLRP3 Inflammasome and Its Correlation with Disease Activity in Adult-onset Still Disease. J Rheumatol 44(8): 1142-1150.
-
Tate MD, Mansell A (2018) An update on the NLRP3 inflammasome and influenza: the road to redemption or perdition?. Curr Opin Immunol 54: 80-85.
-
McAuley JL, Tate MD, MacKenzie-Kludas CJ, Pinar A, Zeng W, et al. (2013) Activation of the NLRP3 inflammasome by IAV virulence protein PB1-F2 contributes to severe pathophysiology and disease. PLoS Pathog 9(5): e1003392.
-
Ong JD, Mansell A, Tate MD (2017) Hero turned villain: NLRP3 inflammasome-induced inflammation during influenza A virus infection. J Leukoc Biol 101(4): 863- 874.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling