Recalcitrant Curvularia Onychomycosis Favourable Treatment Response to Q Switch Nd YAG Laser
We report the case of an immunocompetent 51 year old female with fingernail onychomycosis for 15 years. There was no response to multiple courses of anti fungals (terbinafine, itraconazole, griseofulvin) over the years. Upon SDA culture, causative agent was found to be Curvularia lunata. Patient was started on Itraconazole monthly pulse with daily Terbinafine. After 2 months of no improvement, biweekly sittings of 1064nm Q-switched Nd:YAG (fluence 350 mJ/cm2 over a 2-mm spot at a 5-Hz frequency with two applications in squared form across nail plate). After 8 such sittings, patient showed marked improvement. Q-switched Nd:YAG laser is a promising treatment for recalcitrant onychomycosis as evidenced by our case report. It acts by selective photothermal and photomechanical effect targeting melanin in fungal cell wall. Further studies are needed towards the establishment of standard treatment schedules, as well as the optimum fluency, length and format
Introduction
Curvularia is a dematiacious fungus known to cause non dermatophytic onychomycosis [1]. Due to its presence in vegetation and soil, coupled with an increased use of azole fungicides, there is evidence of resistance to anti fungal treatment [2]. We report a case of an immunocompetent female with fingernail onychomycosis caused by curvularia of 15 year duration, which did not show response to multiple anti fungals over the years and showed favourable response to Q switched Nd:Yag Laser.
Case Report
A 51 year old female presented with discolouration and dystrophy of all fingernails for past 15 years, which was first observed in left thumbnail and gradually spread to involve all other finger nails. The patient had history of consumption of long courses of multiple anti fungals (terbinafine, itraconazole, griseofulvin) over the years, but found no relief. On local examination, all finger nails showed onychodystrophy, leukonychia and melanonychia.
Upon Culture (Sabouraud’s dextrose agar and Lacto phenol cotton blue mount) the organism was identified as Curvularia lunata. Susceptibility testing showed MIC (minimum inhibitory concentration) of terbinafine as 0.25 mg/L, Itraconazole 0.5mg/L, Fluconazole 32 mg/L, Griseofulvin 2mg/L. Due to lack of sensitivity guidelines for Curvularia, in accordance with breakpoints for other non dermatophytic fungi, we found it to be sensitive to all the above drugs [Figure 1].
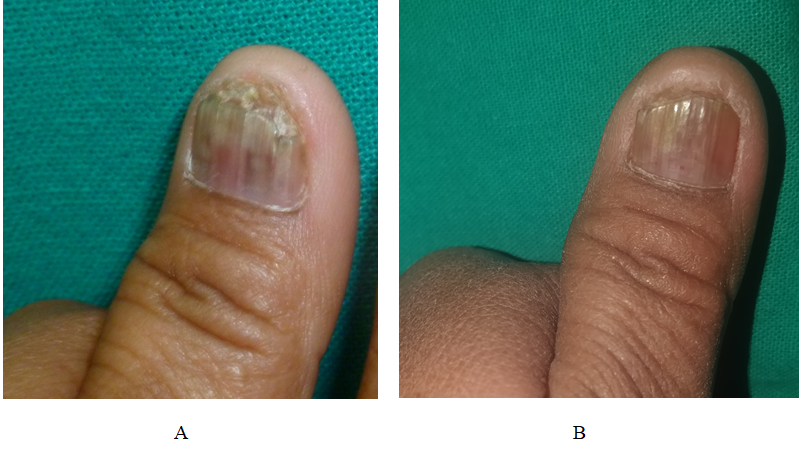
Patient was started on Itraconazole 200mg BD for 1 week monthly pulse with daily Terbinafine 250mg OD. After 2 months of no improvement, biweekly sittings of 1064nm Q-switched Nd:YAG laser (Dermaindia, Tamil Nadu, India) were started. The laser’s settings were adjusted to yield a fluence of 350 mJ/cm2 over a 2-mm spot at a 5-Hz frequency in a single session. Two applications were performed in a squared form across the entire nail plate. Immediate changes after laser light application were observed in form of lightening of pigment. Pre procedure photos were taken before every sitting. After 8 such sittings, patient showed marked improvement in clinical appearance. No recurrence was noted in a follow up period of 6 months (Figure 2).

Discussion
In vitro studies of the q-switched Nd:YAG laser system have yielded conflicting results, whereas clinical studies have shown good results. Due to its minimally invasive nature and less adverse effects, it appears to be a promising treatment for recalcitrant onychomycosis especially when combined with topical and oral antifungals.
Other lasers effective for onychomycosis include the carbon dioxide, near infrared diode laser (870/930-nm), and femtosecond infrared 800 nm lasers aside from other modalities like photodynamic and ultraviolet light therapy [3]. They work via both photothermal and photochemical effects.
Photothermal effects can be selective as well as non- selective. Since selective heating of dermatophytes is quite difficult, most laser systems target dermatophytes through nonspecific bulk heating of the tissue, but has a greater risk of tissue damage and side effects. Thus selective lasers are preferred [4].
Q-switched Nd-YAG laser provides a selective effect, both photothermal and photomechanical, on the fungus. The 1064 nm setting is beyond the absorption spectrum of xanthomegnin (a fungal metabolite), but its effectiveness is due to another chromophore- melanin, a component of the fungal cell wall. The laser penetrates the tissue deeply and efficiently targets fungal growth in the nail bed [3]. The exact mechanism is under evaluation, but it may combine direct fungicidal effects of the laser with induced modifications in the immune system or changes in the local microenvironment.
Laser treatment for onychomycosis is still incipient, and thus, further efforts toward the establishment of standard treatment schedules, as well as the best pulse characteristics with regards to fluency, length and format, are still required.
References
-
Wilhelmus KR, Jones DB (2001) Curvularia keratitis. Trans Am Ophthalmol Soc 99: 111-132.
-
Bengyella L, Yekwa LE, Waikhom SD, Nawaz K, Iftikhar S, et al. (2017) Upsurge in Curvularia infections and global emerging antifungal drug resistance. Asian Journal of Scientific Research 10(4): 299-307.
-
Ledon JA, Savas J, Franca K, Chacon A, Nouri K (2014) Laser and light therapy for onychomycosis: a systematic review. Lasers Med Sci 29(2): 823-829.
-
Ortiz AE, Avram MM, Wanner MA (2014) A review of lasers and light for the treatment of onychomycosis. Lasers in surgery and medicine. 46(2): 117-124.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling