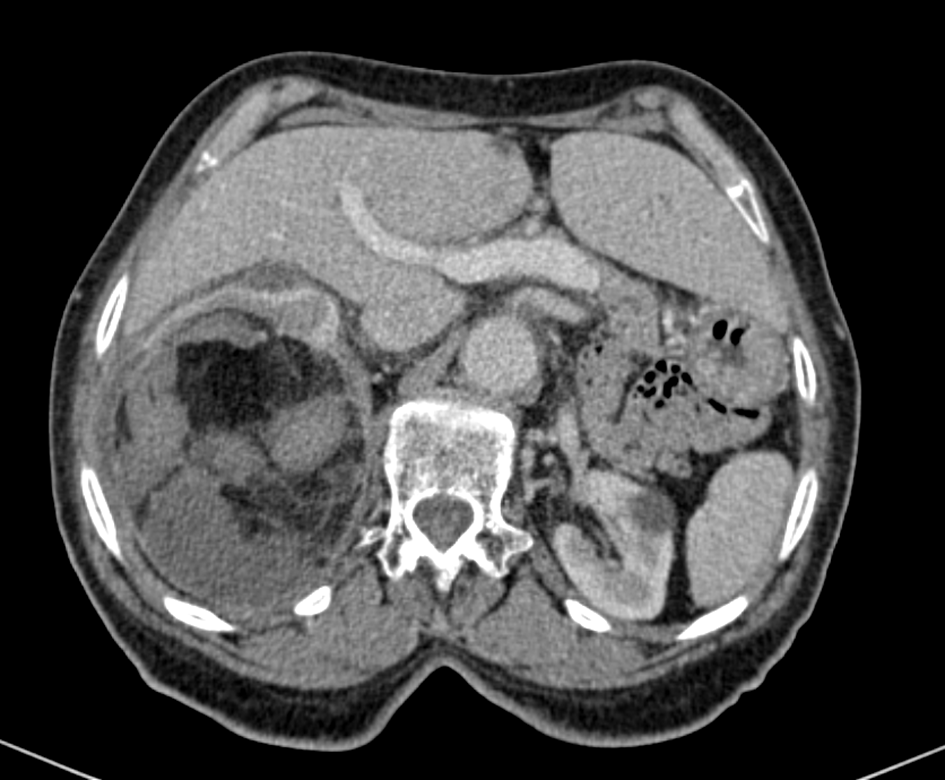
Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage
A 55 years old female patient with no specific medical history consulted in our unity for isolated severe right lumbar pain. An emergency abdomino-pelvic CT-Scan was performed: Revealing a well limited, heterogeneous right renal angiomyolipoma, with triple component, predominantly fatty, complicated by hemorrhage.
Abbreviations
CT: Computed Tomography; RMA: Renal Angiomyolipoma; PDC: Phosphatidyl Choline.
Image Article
Image Article
A 55 years old female patient with no specific medical history consulted in our unity for isolated severe right lumbar pain.
An emergency abdomino-pelvic CT-Scan was performed: Revealing a well limited, heterogeneous right renal angiomyolipoma, with triple component, predominantly fatty, complicated by hemorrhage (Figures 1 & 2).

Renal angiomyolipoma (RMA) is a rare benign tumor (0.3 to 3%) which comprises, in varying proportions, a fatty contingent (often the most abundant), a contingent formed by smooth muscle cells and a vascular contingent [1].
There are two clinical forms of renal RMA. The first is sporadic RMA, which most often occurs in the fifth decade of life and is predominantly seen in female gender. The second form, RMA associated with tuberous sclerosis of Bourneville, is classified as a phacomatosis and affects younger subjects, with no gender predominance.
Clinical symptom atology is polymorphic, dominated by lumbar pain, which his related to the size of the renal angiomyolipoma and intra tumor alhemorrhage [1, 2, 3].
The CT-scan is the key examination.
The classic treatment for renal angiomyolipoma larger than 4 cm is total or partial surgical nephrectomy, although arterial embolization maybe an effective therapeutic alternative that preserves the renal unit [1].
The growth of renal angiomyolipoma is responsible for complication such as hemorrhagic rupture following minimal and spontaneous trauma, giving it a noisy clinical mode of entry in the form of lumbar pain, arterial hypertension, hematuria or even shock in connection with massive intra, peri or extra-renal bleeding [4].
This rupture can threaten the patient’s vital prognosis, which hence the need to be aware of this entity and not delay its management.
References
-
Moudouni SM, En-Nia I, Patard JJ, Lobel B, Guille F (2001) L’emboliswation artérielle dans les angiomyolipomes rénaux hémorragiques. Progress in Urology 11: 235-238.
-
Osterling JE, Fishman EK, Goldman SM, Marshall FF (1986) The management of renal angiomyolipoma. The journal of urology 135(6) : 1121-1124.
-
Unlu C, Lamme B, Nass P, Bolhuis HW (2006) Retroperitoneal hemorrhage caused by a renal angiomyolipome. Emerg Med J 23(6): 464-465.
-
Yigit T, Yigitler C, Gulec B, Ozcan A, Kozak O, Pekcan M (2004) Acute abdomen due to spontaneous renal angiomyolipoma rupture. Prog Urol 14(2): 207-209.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Effect of Contrast Agents on Pregnant Women