Giant Intrathoracic Lipoma: A Rare Presentation
Intrathoracic lipoma is exceptionally uncommon occurence. This report describes a case of 52-year-old male who presented with shortness of breath with chest pain, fatigue, and exertional dyspnea. A routine chest X-ray revealed a large homogenous mass in bilateral lung fields which on CT scan of the chest revealed a mass of fat attenuation in right thoracic cavity herniating retrosternally and involving left thoracic cavity with mediastinal shift to the left. Fine needle aspiration cytology confirmed it be a lipoma.
Abbreviations
CT: Computed Tomography; FNAC: Fine-Needle Aspiration Cytology; CECT: Contrast-Enhanced Computed Tomography; MRI: Magnetic Resonance Imaging.
Introduction
Lipomas are non-cancerous tumors derived from mature fat cells. While lipomas are commonly encountered, intrathoracic lipomas are relatively rare. The occurrence of a giant intrathoracic lipoma is even more exceptional [1]. Prior reports have indicated that intrathoracic lipomas can originate from various sources within the thoracic region, including the mediastinum, diaphragm, bronchus, lung, or thoracic wall [2]. We report a case of massive intrathoracic lipoma in a 52 year old male who presented with shortness of breath.
Case Report
A 52-year-old male presented at our hospital’s outpatient clinic, reporting shortness of breath accompanied by chest pain, fatigue, and exertional dyspnea. He did not experience cough, hemoptysis, weight loss, and did not have any significant past medical history. During the physical examination, the patient displayed the absence of breath sounds and dullness upon percussion in the right chest area. The routine blood workup results were within the normal range.
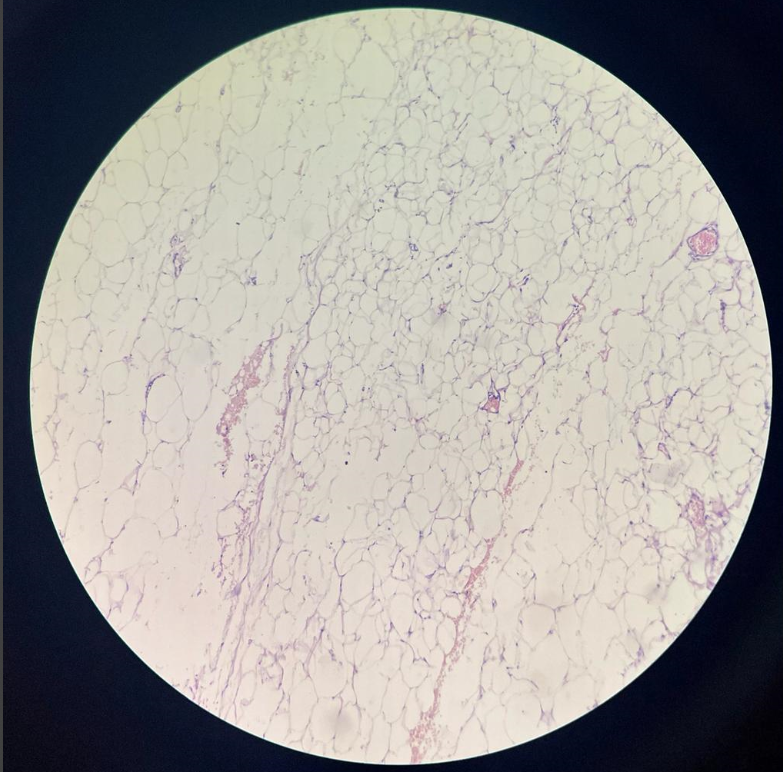
A routine chest X-ray was performed, which showed a large homogenous mass occupying most of right chest and extending towards left side. CECT chest revealed large, homogenous, fat density mass in right thoracic cavity sparing the apical region, herniating retrosternally and involving left thoracic cavity with mediastinal shift to the left. The remaining left lung appeared normal. A CT-guided fine-needle aspiration cytology (FNAC) was performed, which confirmed it to be lipoma and showed mature adipocytes without evidence of any sarcomatous changes (Figures 1-3).
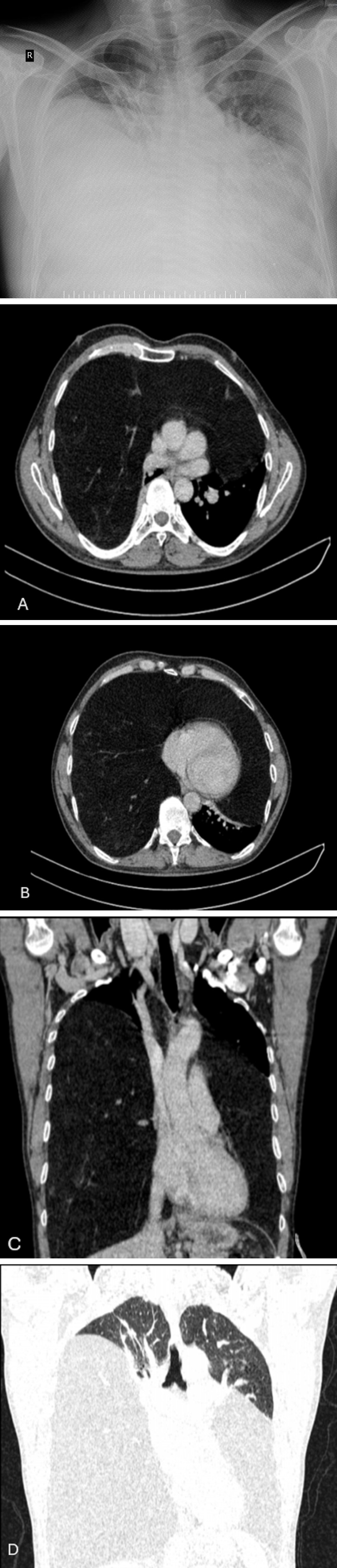
Figure 2(A-D): CECT chest shows a large, homogenous, fat density mass in right thoracic cavity herniating retrosternally and involving left thoracic cavity with mediastinal shift to the left.
Discussion
Lipomas are benign tumors composed of mature fat cells and can develop in various regions of the body. They are typically categorized into two types based on their location: superficial or subcutaneous and deep-seated lipomas. The subcutaneous or superficial variety is the most frequently encountered type [2]. While intrathoracic lipomas are indeed uncommon, they can be found in different locations within the thoracic region, including the mediastinal, diaphragmatic, bronchial, and pulmonary levels [3]. They can extend into various spaces within the thoracic cavity, including the pleural, subpleural, or extrapleural areas [2, 4]. Fothergill reported the first case of intrathoracic lipoma in 1783 [2, 5].
George Huer’s classification of intrathoracic lipomas divides them into three distinct groups: A. Dumbbell tumors: These lipomas have both intrathoracic and extrathoracic portions connected by an isthmus. B. Anterior superior mediastinal lipoma: These lipomas are situated at the roof of the neck within the anterior superior mediastinal region. C. Tumors entirely within the thoracic cavity: This category includes lipomas that lie entirely within the thoracic cavity without extending into extrathoracic areas [6].
In accordance with this classification, our case falls into the category that remains entirely within the thoracic cavity.
According to study done by Tateishi U, et al., it was found that obesity might be one of the causative factors of intrathoracic lipoma [7]. In a case series by Sukurai H, et al., it was demonstrated that three out of ten patients had a BMI greater than 25 kg/m2, indicating that obesity may be a factor in some cases of lipomas [2].
Lipomas typically exhibit very slow growth and are often detected at a later stage of life due to their gradual development [3, 8]. While most patients with intrathoracic lipomas remain asymptomatic, it’s important to note that, as these lipomas can grow to substantial sizes, they have the potential to exert pressure on surrounding structures. The symptoms experienced, such as dyspnea (difficulty breathing) and dysphagia (difficulty swallowing), can be attributed to the local compression of adjacent structures, such as the trachea or esophagus [3]. Intrathoracic lipomas have the potential to compress various internal structures, including the heart, which can have severe consequences, such as heart failure, depending on the degree and location of the compression [9]. They can also lead to various complications, including intratumoral hemorrhage and invasion of intercostal spaces potentially leading to rib lysis (breakdown of ribs), which can further contribute to pain and structural issues within the thoracic cavity [10].
Akar E, et al. conducted a retrospective study analyzing the clinicopathological records of seven patients who underwent surgery for intrathoracic lipomas between 2005 and 2017. Out of these patients, four were asymptomatic, whereas the other three experienced symptoms such as chest pain and exertional dyspnea [11].
While the tumor is typically discovered incidentally in chest X-rays, CT scans and magnetic resonance imaging (MRI) scans are the most valuable imaging techniques for diagnosing intrathoracic lipomas. [8, 10]. A definitive diagnosis can be made through chest CT when it reveals a mass with homogeneous fat attenuation (measuring between -50 to -150 Hounsfield Units) that typically forms obtuse angles with the chest wall, displacing nearby pulmonary parenchyma and vessels [10]. The density might not be entirely uniform due to the presence of fibrous stroma and areas of dystrophic ring-type calcifications within scattered dense soft tissue components, which are common features of lipomas [12]. On MRI, intrathoracic lipomas typically exhibit high signal intensities on both T1 and T2-weighted images [13].
Intrathoracic lipomas are predominantly benign tumors, and the definitive treatment option to prevent future recurrences involves complete en-bloc resection whenever possible. This can be achieved through various surgical approaches, including muscle-sparing techniques, standard open thoracotomy, and mini-thoracotomy. In recent years, thoracoscopic surgery has become less invasive, with procedures such as uniportal video-assisted thoracoscopic surgery and needlescopic surgery now widely performed. These less invasive techniques allow for earlier, safer, and more reliable diagnosis and treatment, improving patient outcomes and reducing recovery times [14].
The prognosis following the resection of lipomas is typically favorable. After removal, local recurrence of intrathoracic or mediastinal lipomas is rare.
Conclusion
Intrathoracic lipomas are uncommon, benign tumors in contrast to the highly prevalent subcutaneous lipomas. They tend to exhibit slow, asymptomatic growth over several years and are typically discovered incidentally during routine investigations once they attain significant size. Diagnosis is usually confirmed through CT and MRI scans. When an incidentally identified large mass is encountered within the thoracic cavity, it is important to consider intrathoracic lipoma as a potential differential diagnosis. While pleural lipomas do not progress to liposarcoma, thorough surgical resection is still imperative to prevent any potential recurrence.
References
-
(2002) Pathology and genetics of tumours of soft tissue and bone. In: Fletcher CD, Unni KK, Mertens F (Eds.), WHO Classification of Tumours. 3rd Edition (Edn.), IARC, pp: 415.
-
Sakurai H, Kaji M, Yamazaki K, Suemasu K (2008) Intrathoracic lipomas: their clinicopathological behaviors are not as straightforward as expected. Ann Thorac Surg 86(1): 261-265.
-
Chen M, Yang J, Zhu L, Zhao H (2013) Intrathoracic giant pleural lipoma: case report and review of the literature. J Cardiothorac Surg 8(1): 1-4.
-
Tesfaye S, Abera B, Bezabeh A, Bezabih YS, Tesfaye W (2022) A rare case of huge intrathoracic lipomatosis filling the right pleural cavity removed by open thoracic surgery: A case report. Int J Surg Case Rep 98: 107565.
-
Sulzer MA, Goei R, Bollen EC, Theunissen PH, Maesen FP (1994) Lipoma of the external thoracic wall. Eur Respir J 7(1): 207-209.
-
Heuer GJ (1933) The thoracic lipomas. Ann Surg 98(5): 801-819.
-
Tateishi U, Gladish GW, Kusumoto M, Hasegawa T, Yokoyama R, et al. (2003) Chest wall tumors: radiologic findings and pathologic correlation: part 2: Malignant tumors. Radiographics 23(6):1491-1508.
-
Yang J, Li S, Kang A, Chen X, Su B, et al. (2012) A giant intrathoracic osteolipoma: a case report and review of the literature. Int J Surg Case Rep 3(7): 290-292.
-
Jack AI, Blohm ME, Lye M (1995) An intrathoracic lipoma impairing left ventricular function. Br Heart J 74(1): 95.
-
Buxton RC, Tan CS, Khine NM, Cuasay NS, Shor MJ, et al. (1988) Atypical transmural thoracic lipoma: CT diagnosis. J Comput Assist Tomogr 12(2): 196-198.
-
Akar E, Haberal MA, Dikis OS (2020) Diagnostic and therapeutic treatment methods for intrathoracic extrapulmonary lipomas. Niger J Clin Pract 23(5): 626- 630.
-
Narbon BS, Paris OS, Sprekelsen JCB, Gil FP, Vilanova AG, et al. (1997) Hourglass thoracic lipoma of infancy: case report and review of the literature. J Pediatr Surg 32(5): 785-786.
-
(2007) Benign lipomatous tumors. In: Weiss SW, Goldblum JR, Folpe AL (Eds.), Enzinger and Weiss’s soft tissue tumors. 7th Edition (Edn.), Elsevier, pp: 1304.
-
Hirai Y, Mikasa Y, Iguchi H, Fusamoto A, Yata Y, et al. (2022) Intrathoracic lipoma of the chest wall that appeared relatively rapidly and could be resected and diagnosed by minimally invasive thoracoscopic surgery: A case report. Respirol Case Rep 10(5): e0946.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage
- Effect of Contrast Agents on Pregnant Women