Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
Testicular Adrenal Rest Tumors (TARTs) are intratesticular masses linked to congenital adrenal hyperplasia (CAH) and the over secretion of adrenocorticotropic hormone. We present a case of a 17-year-old male patient with CAH who exhibited unique findings on ultrasonography. This case illustrates the changes in ultrasound imaging features over the years. The patient had bilaterally observed TARTs and later developed diffuse microlithiasis on follow-up images. The TARTs displayed minimal disruption to the underlying testicular structures, preserving the testicular contour, and showed hypervascularity. This report adds to the limited literature on TARTs in CAH patients and underscores the significance of identifying these unique presentations to aid in diagnosis and management, thereby avoiding unnecessary biopsies and interventions..
Abbreviations
TARTs: Testicular Adrenal Rest Tumors; CAH: congenital adrenal hyperplasia; ACTH: adrenocorticotropic hormone.
Introduction
Testicular adrenal rest tumors (TARTs) are intratesticular masses prevalent in males with congenital adrenal hyperplasia (CAH) caused by a deficiency of enzyme 21-hydroxylase in the adrenal cortex [1, 2]. This deficiency reduces the production of cortisol and aldosterone, and due to the negative feedback mechanism controlling the hypothalamic-pituitary-adrenal axis, increases the accumulation of 17-hydroxyprogesterone and adrenal androgens [1]. The cortisol deficiency leads to oversecretion of adrenocorticotropic hormone (ACTH), resulting in adrenal hyperplasia [1, 2].
Ultrasonography is the preferred radiological modality for the diagnosis of testicular pathologies because it is readily available and easily accessible. Additionally, it is low-cost, quick, and does not expose the patient to radiation [1, 2]. Gray-scale scrotal ultrasonography may reveal lesions in CAH ranging from hypoechoic areas near the testicular mediastinum to scattered testicular hyper-echogenicities [2]. Most lesions are lobulated and hypoechoic, with possible hyperechoic areas secondary to fibrosis. The lesions may be homogeneous or heterogeneous and hypovascular or hypervascular. The lesions may also demonstrate testicular microlithiasis, which is characterized by calcification within the seminiferous tubules, presenting on ultrasound imaging as multiple or uniform echogenic 0.1 - 0.3 cm foci scattered throughout the testicular parenchyma [2].
Doppler ultrasound may reveal a spoke wheel pattern of converging vessels or a normal testicular vasculature with unchanged vessel caliber, which is specific for this pathology [3]. TARTs are typically bilateral and do minimal disruption to underlying testicular structures, thus do not distort the testicular contour [2].
Case Presentation
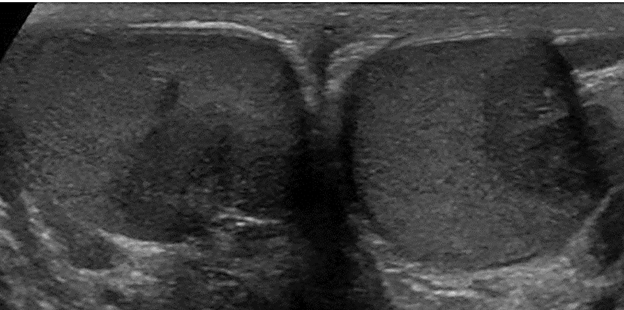
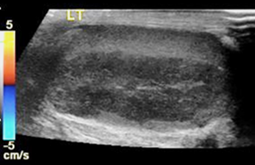
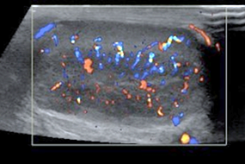
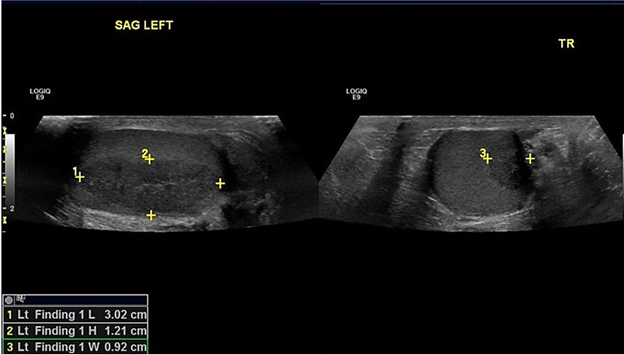
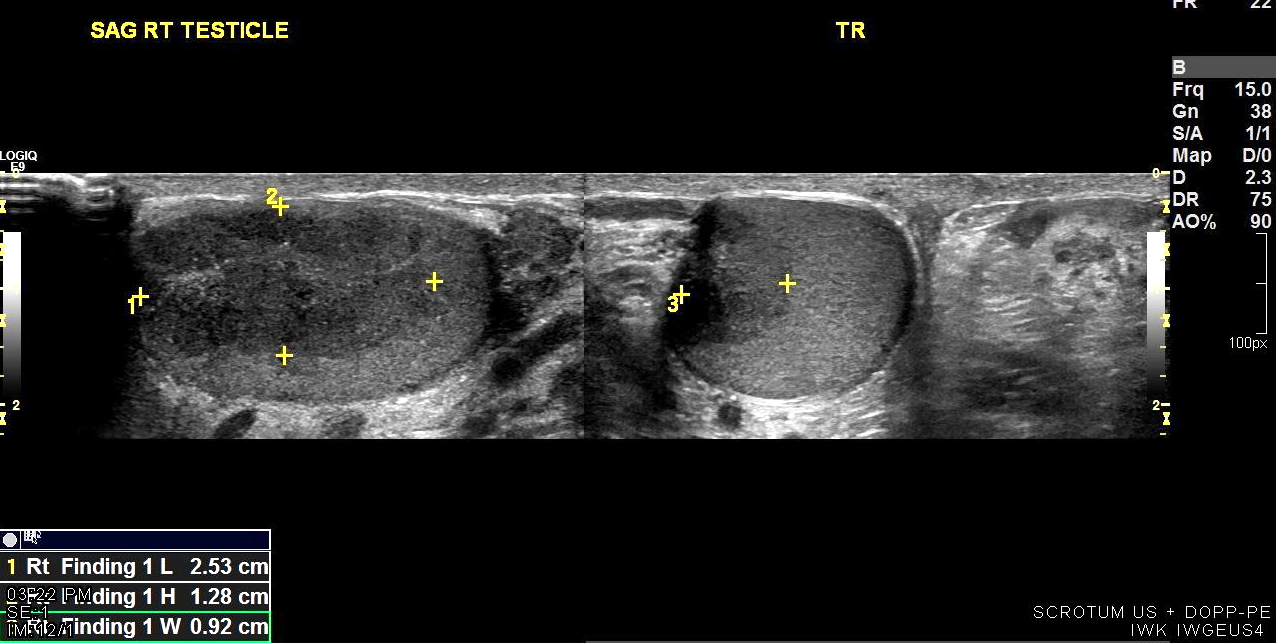
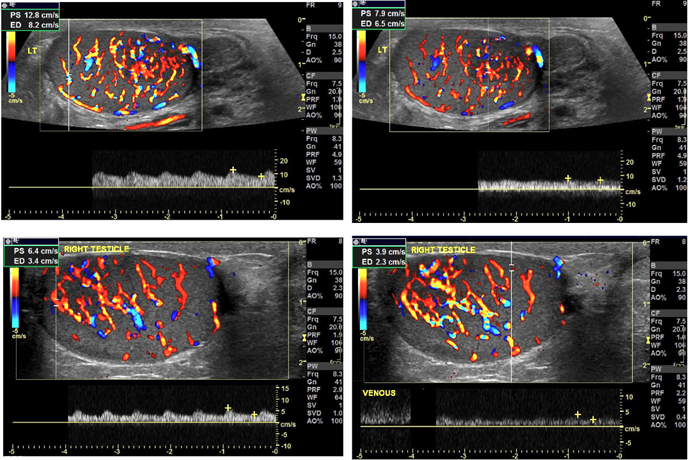
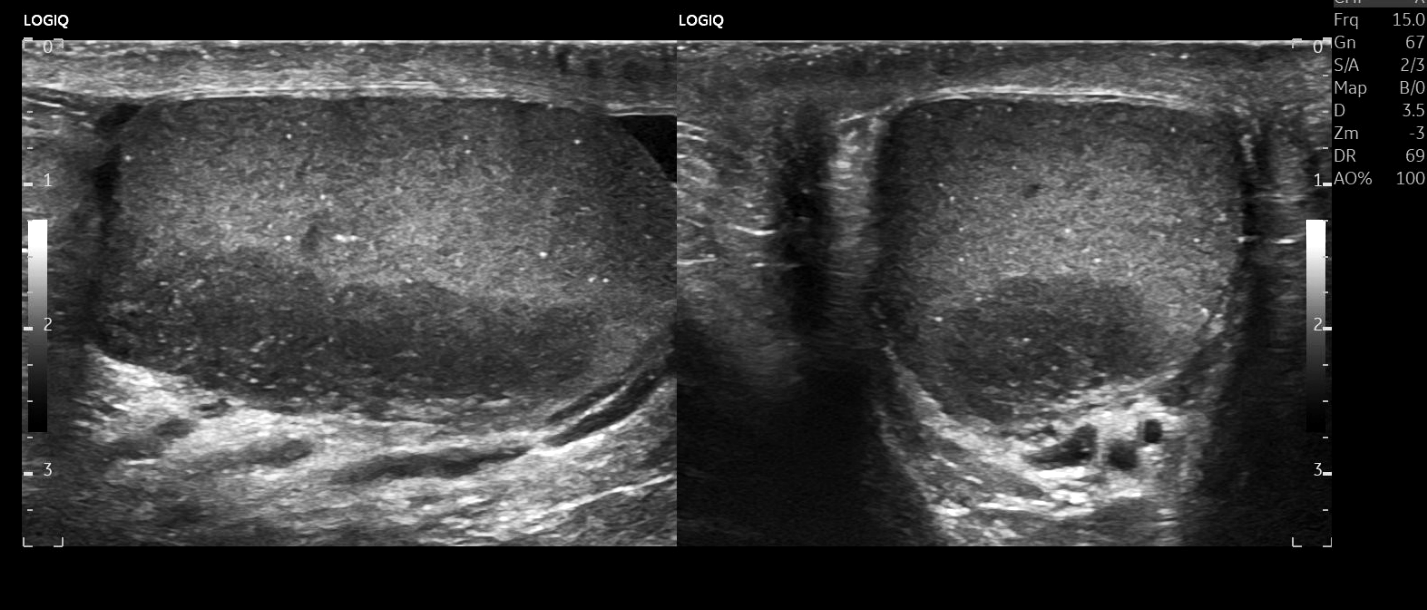
A 17-year-old male presented with a salt-wasting type of CAH secondary to a severe deficiency of enzyme 21-hydroxylase, culminating in reduced aldosterone production and lack of sodium and water reabsorption by the distal renal tubules. Ultrasonography performed in 2019, revealed hypoechoic areas in bilateral testes adjacent to the testicular hilum, consistent with TARTs (Figures 1 & 2). The left testicular hypoechoic lesion measures 3.0 × 0.9 × 1.2 cm (Figure 3), and the right one measures 2.5 × 0.9 × 1.3 cm (Figure 4). The bilateral testicles maintain normal vascularity (Figure 5). Subsequent imaging performed in 2023, identified newly scattered microlithiasis compared to prior scans (Figures 6 & 7). Notably, the TARTs were within the mediastinum testes and did not disrupt the underlying testicular structures, preserving the testicular contour, aligning with findings from existing case reports [3, 4]. Imaging over time also showed minimal fluctuation in the size of the lesion since diagnosis, supporting a benign pathology. It is worth mentioning that bilateral TARTs are more common than unilateral ones, which occur in only 25% of the cases [2]. Testicular microlithiasis is a common finding in testicular germ cell tumors but is also prevalent in patients with benign lesions [1, 2].

Discussion
TARTs are ectopic adrenal tissue present inside the testes due to persistent stimulation by high circulating levels of ACTH [1]. TARTs are formed due to the trophic effects of persistently elevated ACTH found in CAH, as in the above case, or rarely due to Cushing’s syndrome [1]. CAH is a group of autosomal recessive enzyme defects, with the majority of cases linked to a deficiency of 21-hydroxylase in the adrenal cortex. It leads to high 17-hydroxyprogesterone levels and reduced cortisol and aldosterone levels which reduces the negative feedback to the hypothalamic-pituitary-adrenal axis. This, in turn, causes the overproduction of ACTH with subsequent adrenal hyperplasia and the formation of ectopic adrenal cell rests [1].
Most cases of TARTs are asymptomatic, with a minority presenting with features of a testicular mass. Common symptoms may include testicular heaviness, dull-aching pain in the groin, and swelling in the groin region, usually in adolescence and early adulthood [1].
The sonographic findings in our case demonstrated slow- growing bilateral testicular hypoechoic masses with normal blood flow and testicular microlithiasis. Akbarzadeh Pasha A et al. similarly reported a 2.6 × 2.1 × 2.6 cm hypoechoic mass with echogenic foci suggesting calcifications in the left testicle and two distinct hypoechoic foci on the right side with preserved vascular supply. A pre-operative abdominopelvic ultrasound revealed bilateral adrenal hyperplasia, clinching the diagnosis of TARTs [3]. However, Mansoor NM, et al. showed the existence of multiple coalescing hypo and hyperechoic lesions with ‘curvilinear’ areas of ‘focal’ calcification versus the diffuse testicular microlithiasis in our study. They also illustrated an increase in the vascularity surrounding the lesions and reduced Doppler flow within the lesions [4]. This is in contrast to our study, which shows slightly increased vascularity of the lesion with preserved flow in the surrounding testicle.
Yu L, et al. studied bilateral giant TARTs in a patient with 3 beta-hydroxysteroid dehydrogenase-2 deficiency, a rare form of CAH. They demonstrated a tumor size of 8.3 × 4.6 ×4.4 cm and 7.4 × 4.9 × 3.1 cm [5]. Our study also showed sufficiently large tumors measuring 3.0 × 0.9 × 1.2 cm on the left side and 2.5 × 0.9 × 1.3 cm on the right. However, the usual case presentation is the small size of tumors signifying asymptomatic cell rests. This is likely linked to TARTs beginning as small, distinct lesions that could evolve to form one large, coalescing lesion [6].
Jacobson A, et al. reported TARTs in a 49-year-old male (the usual age of presentation is teens and early adulthood [6]). Imaging revealed multiple bilateral mixed hyper and hypoechoic masses in the testicular mediastinum ranging from 0.3 to 0.6 cm with a normal testicular size versus a testicular mass in our study [7].
The differential diagnoses include other causes presenting as testicular masses, such as testicular carcinoma, testicular infections or abscesses. The imaging features favoring a benign diagnosis include bilateral, well- defined, homogeneously hypoechoic lesions, with or without microlithiasis, with intact vascularity, distinct localization with preservation of normal testicular parenchyma and absence of internal echodensities [6]. However, malignant lesions commonly demonstrate a unilateral, heterogeneous mass with solid and cystic areas, high internal vascularity, and destruction of normal parenchyma with infiltration into the surrounding tissues [6]. Therefore, it mandates prompt identification and characterization of the masses to direct accurate and adequate management strategies and avoid unnecessary surgery and mistreatment. The extreme complication of TARTs is infertility which is attributed to the mechanical obstruction to seminiferous tubules and the direct toxic effects of hormone precursors in CAH [6].
The usual management of testicular adrenal cell rests blends a myriad of medical and surgical therapies, such as exogenous glucocorticoids to suppress the ectopic adrenal tissue or surgical removal of the testicular masses. The former is exceptional as it helps in the stabilization or recession of these cell rests in most cases [6].
Conclusion
This case report highlights the importance of recognizing testicular adrenal rest tumors (TARTs) in adolescent males with congenital adrenal hyperplasia (CAH). The presented case of a 17-year-old male with CAH and bilaterally observed TARTs, which exhibited unique ultrasonographic features, contributes valuable insights into the diagnosis and management of TARTs. The findings of hypervascularity and minimal disruption to testicular structures, along with the development of testicular microlithiasis, underscore the significance of detailed ultrasound monitoring. These observations support the benign nature of TARTs and suggest that invasive procedures such as biopsies can often be avoided. Continuous follow-up and appropriate medical management remain crucial in mitigating complications, including infertility, associated with TARTs in CAH patients. The case further emphasizes the utility of ultrasonography in differentiating TARTs from other testicular masses, aiding in accurate and non-invasive diagnosis. This report, therefore, adds to the limited literature on TARTs, providing a foundation for future studies and enhancing clinical understanding and management strategies for CAH patients with testicular involvement.
Conflict of Interest & Competing Interests: None to declare.
References
-
Engels M, Span PN, van Herwaarden AE, Sweep FCGJ, Stikkelbroeck NMML, et al. (2019) Testicular adrenal rest tumors: Current insights on prevalence, characteristics, origin, and treatment. Endocr Rev 40(4): 973-987.
-
Vanzulli A, DelMaschio A, Paesano P, Braggion F, Livieri C, et al. (1992) Testicular masses in association with adrenogenital syndrome: US findings. Radiology 183(2): 425-429.
-
Akbarzadeh Pasha A, Shafi H, Teimorian M, Rostami G, Moudi E, et al. (2021) Congenital adrenal hyperplasia presented with bilateral testicular tumor: A case report. Caspian J Intern Med 12(Suppl 2): S431-S434.
-
Mansoor NM, Huang DY, Sidhu PS (2022) Multiparametric ultrasound imaging characteristics of multiple testicular adrenal rest tumours in congenital adrenal hyperplasia. Ultrasound 30(1): 80-84.
-
Yu L, Chen P, Zhu W, Sun J, Li S (2021) Case report: Clinical experience of bilateral giant pediatric testicular adrenal rest tumors with 3 beta-hydroxysteroid dehydrogenase-2 family history. BMC Pediatr 21(1): 405.
-
Wang Z, Yang Z, Wang W, Chen L, Huang Y, et al. (2015) Diagnosis of testicular adrenal rest tumors on ultrasound: A retrospective study of 15 cases report. Medicine 94(36): e1471.
-
Jacobson A, Koberlein E, Thomay A, Lombard CB, Adelanwa A, et al. (2022) Congenital adrenal hyperplasia with associated giant adrenal myelolipoma, testicular adrenal rest tumors and primary pigmented nodular adrenocortical disease: A case report and brief review of the literature. Radiol Case Rep 17(3): 710-716.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage
- Effect of Contrast Agents on Pregnant Women